
Anti-Demineralization Effects of Dental Adhesive-Composites on Enamel–Root Dentin Junction

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
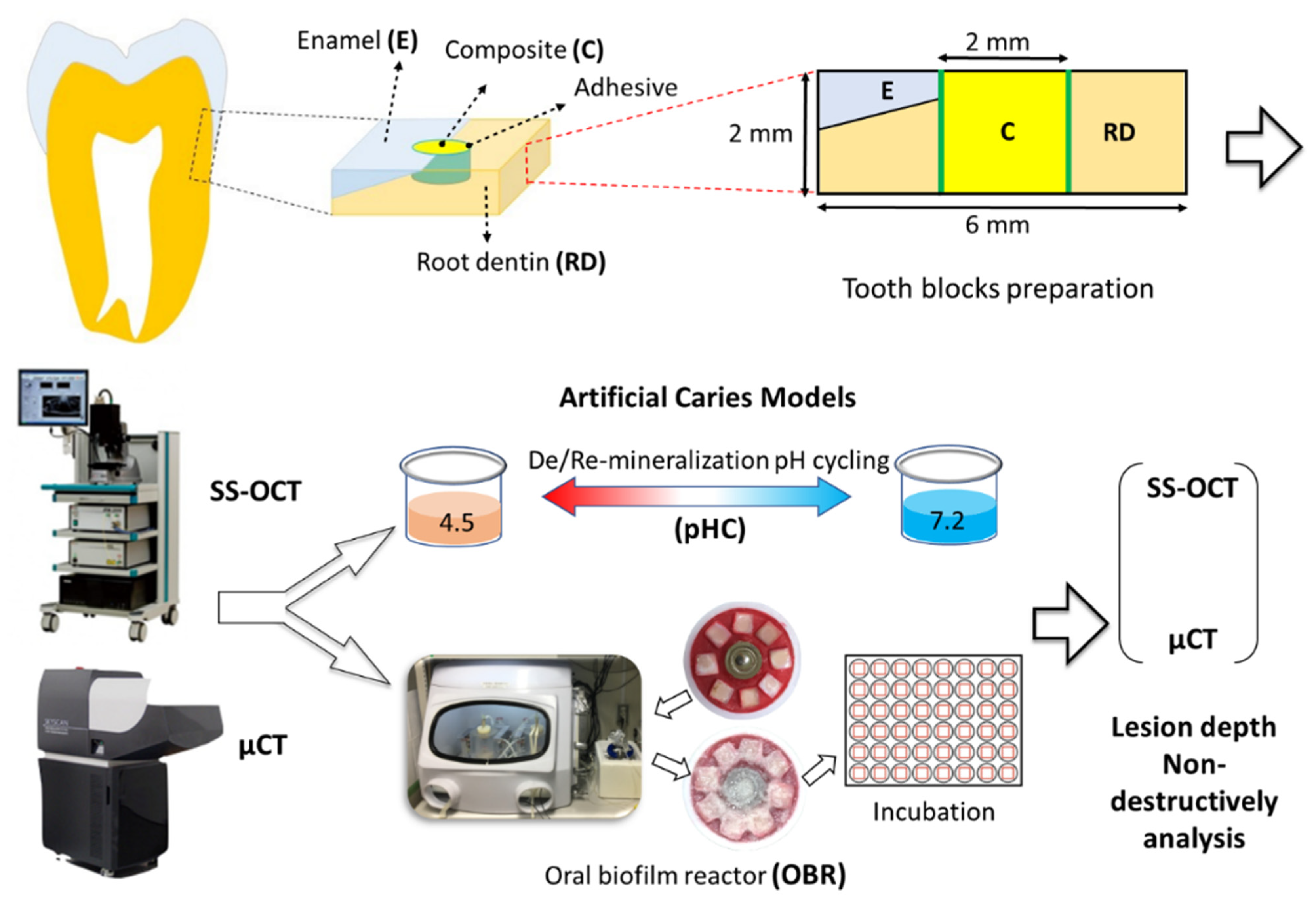
2.1. Specimen Preparation
2.2. Establishment of the Artificial Caries Models
2.3. pH Cycling (pHC) Model
2.4. Oral Biofilm Reactor (OBR) Model
2.5. Swept-Source Optical Coherence Tomography (SS-OCT)
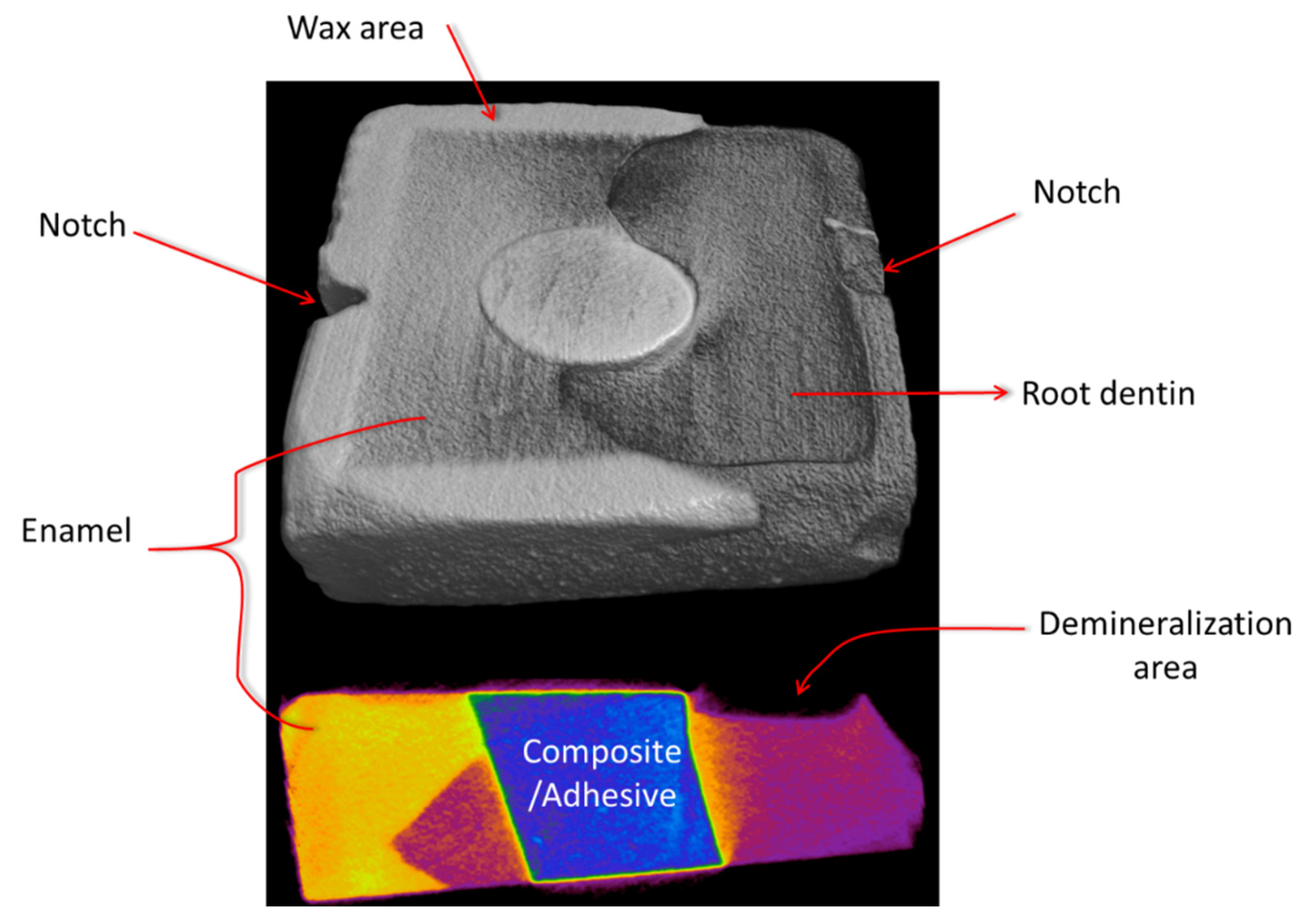
2.6. Micro Computed Tomography (ΜCT) Imaging Analysis
2.7. Statistical Analysis
3. Results
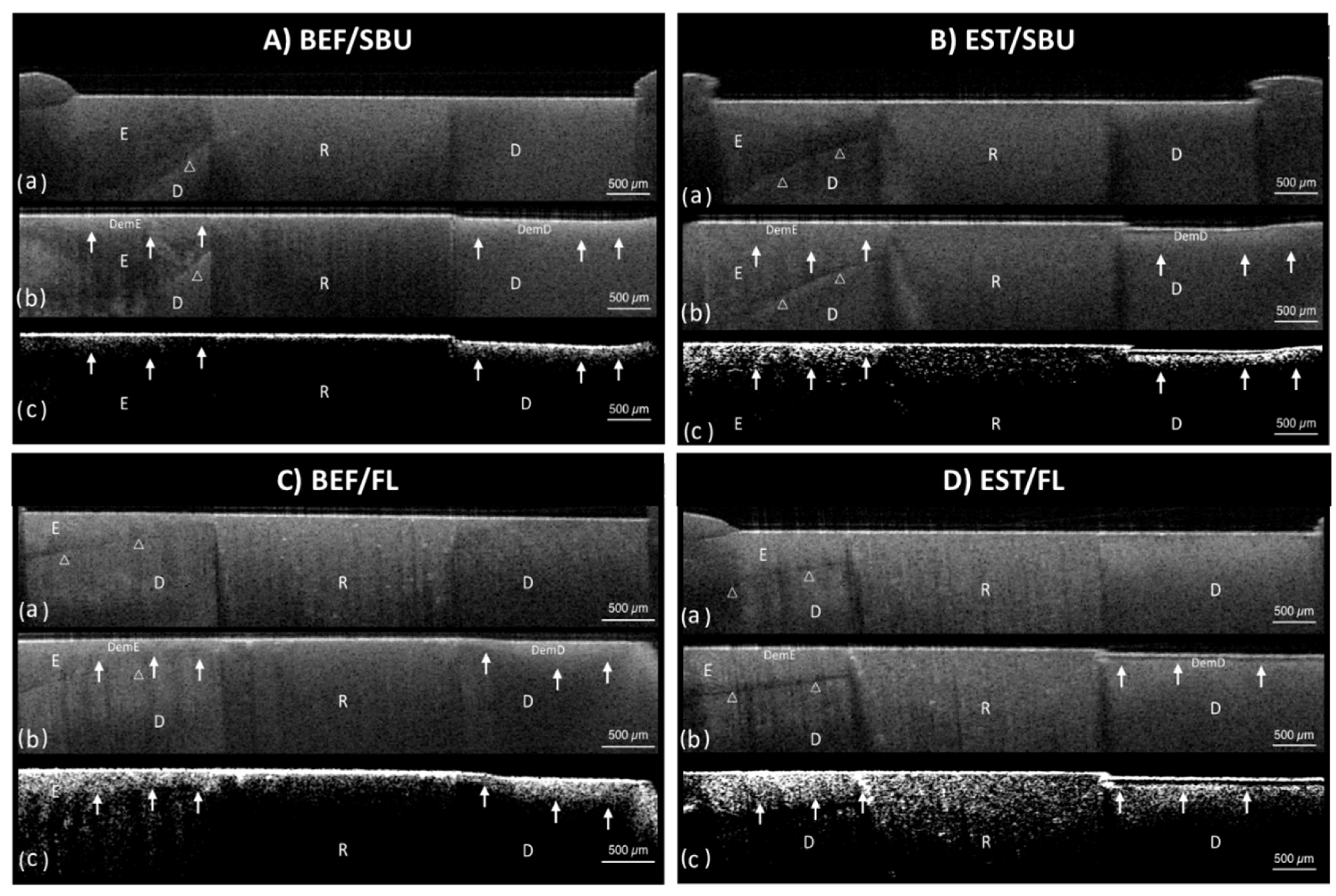
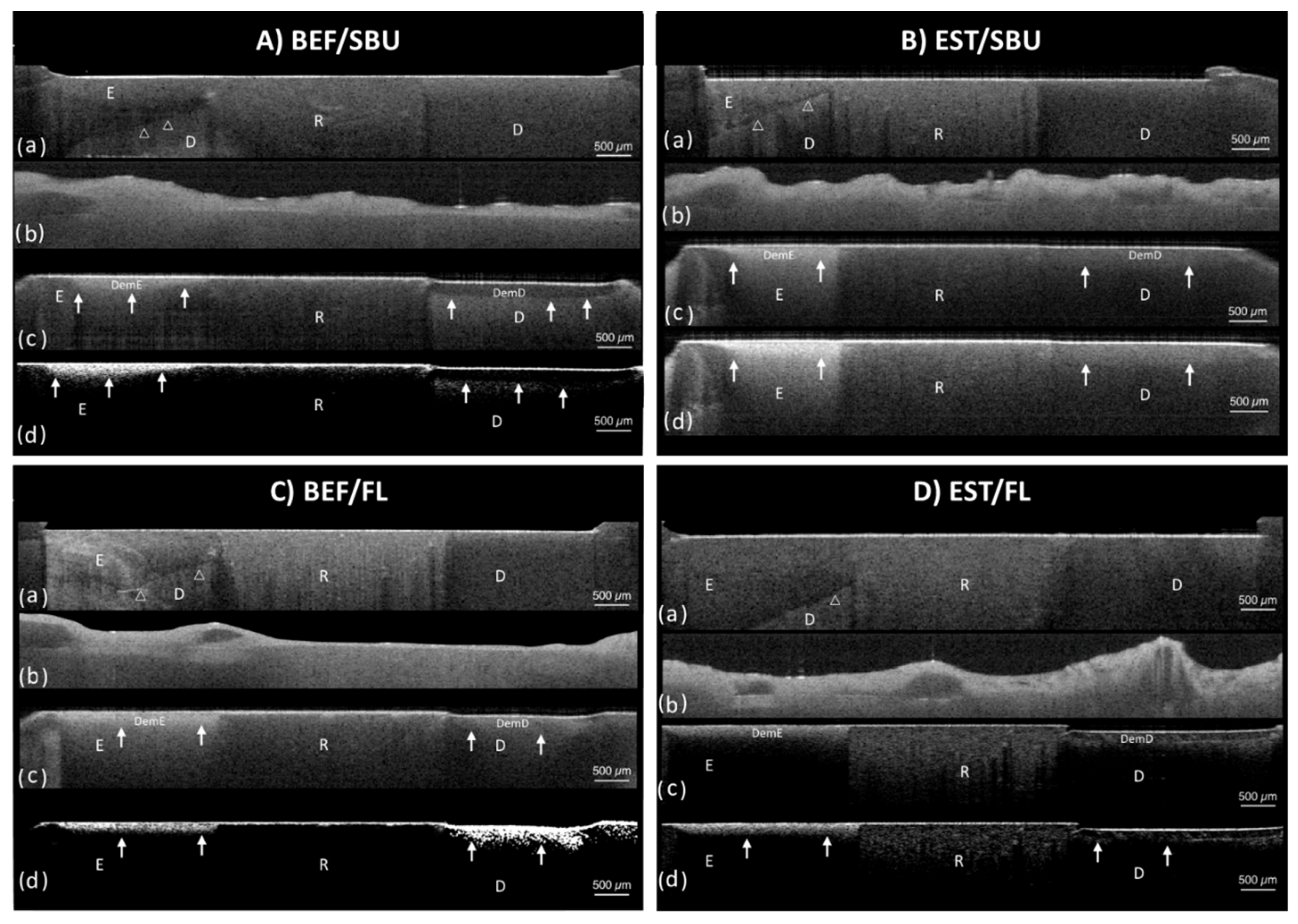
3.1. Artificial Caries Pattern Assessment
- (1)
- Type A: The lesion was generally shallow but became deeper away from the restoration. The bonding interface was intact and showed no attachment loss.
- (2)
- Type B: Type B was similar to the Type A pattern except the lesion depth had a steeper drop near the restoration. The interface was still intact and showed no attachment loss.
- (3)
- Type C: The depth of lesion was consistent whether near or away from the restoration. The interface presented significant attachment loss.
- (4)
- Type D: The lesion depth was similar to Type C, however, the interface presented severe breakdown at the interface compared to Type C.
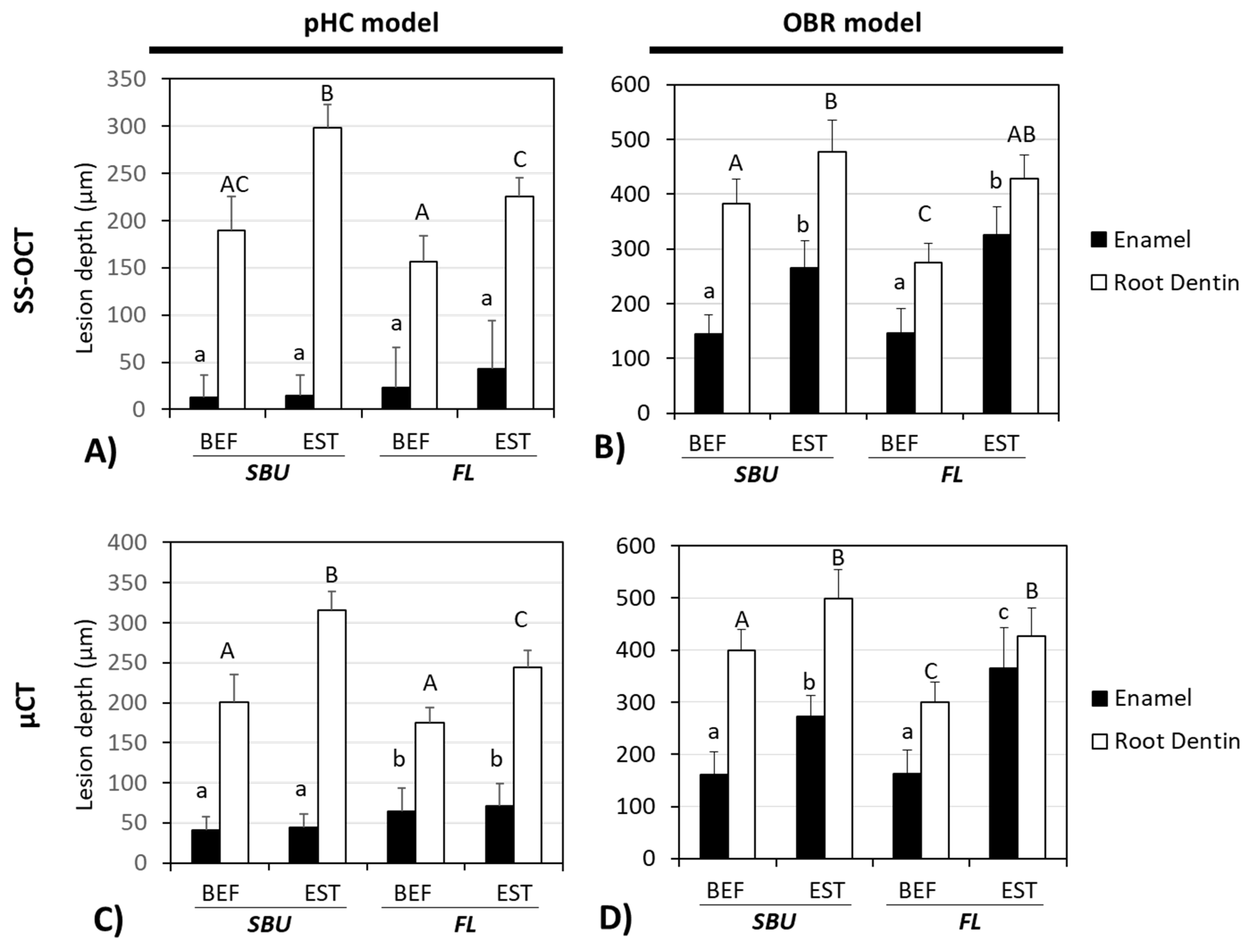
3.2. Lesion Depths Assessment by SS-OCT and μCT
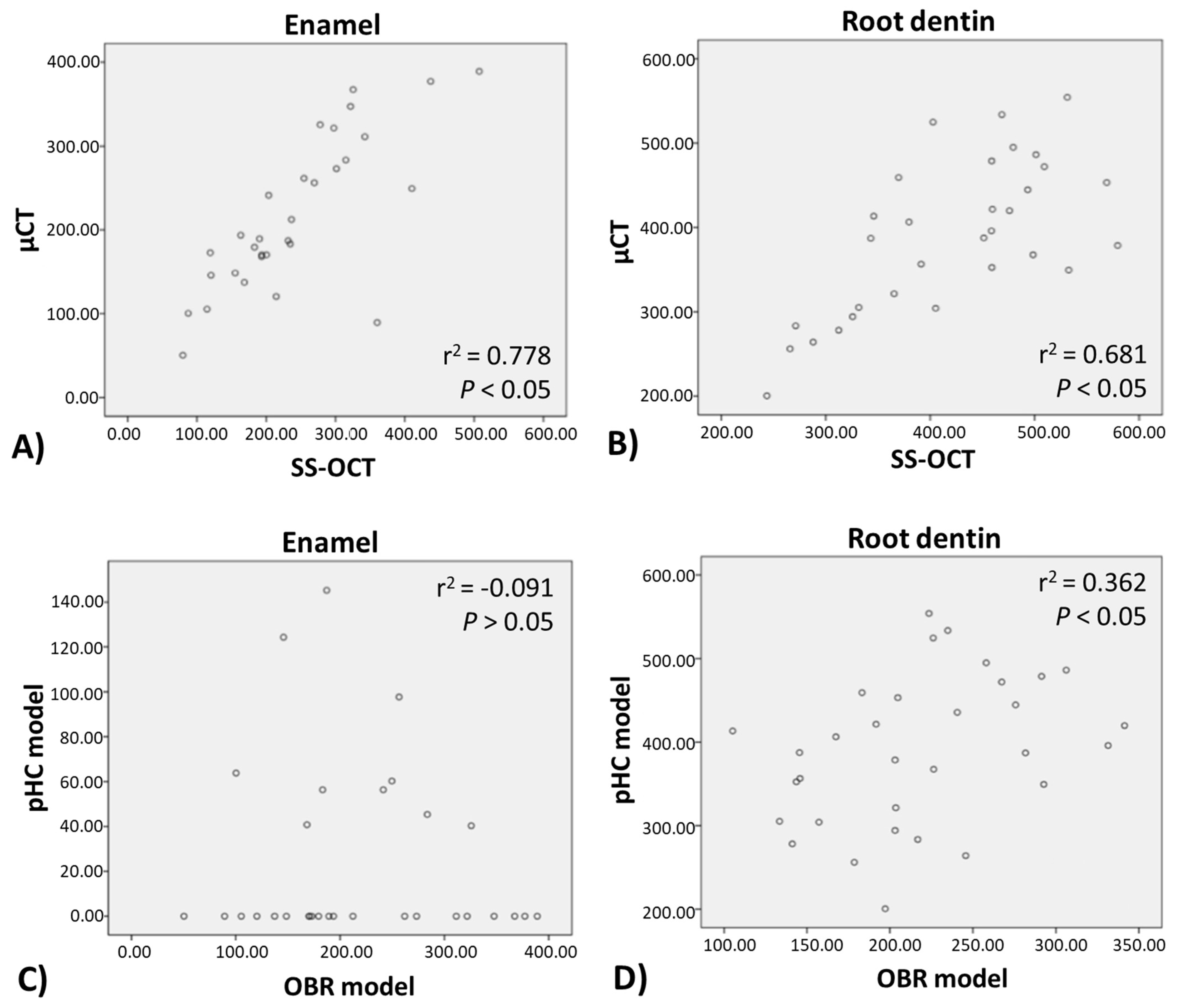
3.3. Correlation Analysis of pHC and OBR Model, SS-OCT, and μCT
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Abt, E. The risk of failure is higher for composites than for amalgam restorations. J. Evid. Based Dent. Pract. 2008, 8, 83–84. [Google Scholar] [CrossRef] [PubMed]
- Bernardo, M.; Luis, H.; Martin, M.D.; Leroux, B.G.; Rue, T.; Leitão, J.; DeRouen, T.A. Survival and reasons for failure of amalgam versus composite posterior restorations placed in a randomized clinical trial. J. Am. Dent. Assoc. 2007, 138, 775–783. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- AlQranei, M.S.; Balhaddad, A.A.; Melo, M.A.S. The burden of root caries: Updated perspectives and advances on management strategies. Gerodontology 2021, 38, 136–153. [Google Scholar] [CrossRef] [PubMed]
- López, R.; Smith, P.C.; Göstemeyer, G.; Schwendicke, F. Ageing, dental caries and periodontal diseases. Clin. Periodontol. 2017, 44, S145–S152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miki, S.; Kitagawa, H.; Kitagawa, R.; Kiba, W.; Hayashi, M.; Imazato, S. Antibacterial activity of resin composites containing surface pre-reacted glass-ionomer (S-PRG) filler. Dent. Mater. 2016, 32, 1095–1102. [Google Scholar] [CrossRef]
- Fujimoto, Y.; Iwasa, M.; Murayama, R.; Miyazaki, M.; Nagafuji, A.; Nakatsuka, T. Detection of ions released from S-PRG fillers and their modulation effect. Dent. Mater. J. 2010, 29, 392–397. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Imazato, S.; Ma, S.; Chen, J.H.; Xu, H.H. Therapeutic polymers for dental adhesives: Loading resins with bio-active components. Dent. Mater. 2014, 30, 97–104. [Google Scholar] [CrossRef] [Green Version]
- Ito, S.; Iijima, M.; Hashimoto, M.; Tsukamoto, N.; Mizoguchi, I.; Saito, T. Effects of surface pre-reacted glass-ionomer fillers on mineral induction by phosphoprotein. J. Dent. 2011, 39, 72–79. [Google Scholar] [CrossRef]
- Lee, M.J.; Kwon, J.S.; Kim, J.Y.; Ryu, J.H.; Seo, J.Y.; Jang, S.; Kim, K.M.; Hwang, C.J.; Choi, S.H. Bioactive resin-based composite with surface pre-reacted glass-ionomer filler and zwitterionic material to prevent the formation of multi-species biofilm. Dent. Mater. 2019, 35, 1331–1341. [Google Scholar] [CrossRef]
- Van Meerbeek, B.; De Munck, J.; Yoshida, Y.; Inoue, S.; Vargas, M.; Vijay, P.; Van Landuyt, K.; Lambrechts, P.; Vanherle, G. Buonocore memorial lecture. Adhesion to enamel and dentin: Current status and future challenges. Oper. Dent. 2003, 28, 215–235. [Google Scholar]
- Stewart, C.A.; Hong, J.H.; Hatton, B.D.; Finer, Y. Antimicrobial antidegradative dental adhesive preserves restoration-tooth bond. Dent. Mater. 2020, 36, 1666–1679. [Google Scholar] [CrossRef] [PubMed]
- Gou, Y.P.; Li, J.Y.; Meghil, M.M.; Cutler, C.W.; Xu, H.H.K.; Tay, F.R.; Niu, L.N. Quaternary ammonium silane-based antibacterial and anti-proteolytic cavity cleanser. Dent. Mater. 2018, 34, 1814–1827. [Google Scholar] [CrossRef]
- Kermanshahi, S.; Santerre, J.P.; Cvitkovitch, D.G.; Finer, Y. Biodegradation of resin-dentin interfaces increases bacterial microleakage. J. Dent. Res. 2010, 89, 996–1001. [Google Scholar] [CrossRef] [PubMed]
- Piemjai, M.; Chantarawej, P.; Nakabayashi, N. Evaluation of Caries-Free Restorations Bonded with Various Adhesive Systems: In Vitro Study. Int. J. Dent. 2020, 2020, 5859835. [Google Scholar] [CrossRef]
- Bitter, K.; Paris, S.; Martus, P.; Schartner, R.; Kielbassa, A.M. A Confocal Laser Scanning Microscope investigation of different dental adhesives bonded to root canal dentine. Int. Endod. J. 2004, 37, 840–848. [Google Scholar] [CrossRef]
- Chiang, Y.C.; Rosch, P.; Dabanoglu, A.; Lin, C.P.; Hickel, R.; Kunzelmann, K.H. Polymerization composite shrinkage evaluation with 3D deformation analysis from microCT images. Dent. Mater. 2010, 26, 223–231. [Google Scholar] [CrossRef]
- Zhou, Y.; Matin, K.; Shimada, Y.; Wang, G.; Sadr, A.; Tagami, J. Detection and analysis of early degradation at resin-dentin interface by optical coherence tomography (OCT) and confocal laser scanning microscope (CLSM). J. Dent. 2021, 106, 103583. [Google Scholar] [CrossRef]
- Jacker-Guhr, S.; Ibarra, G.; Oppermann, L.S.; Luhrs, A.K.; Rahman, A.; Geurtsen, W. Evaluation of microleakage in class V composite restorations using dye penetration and micro-CT. Clin. Oral. Investig. 2016, 20, 1709–1718. [Google Scholar] [CrossRef]
- Yamamoto, S.; Sayed, M.; Takahashi, M.; Matin, K.; Hiraishi, N.; Nikaido, T.; Burrow, M.F.; Tagami, J. Effects of a surface prereacted glass-ionomer filler coating material on biofilm formation and inhibition of dentin demineralization. Clin. Oral Investig. 2021, 25, 683–690. [Google Scholar] [CrossRef] [PubMed]
- Featherstone, J.D.B.; OReilly, M.M.; Shariati, M.; Brugler, S. Enhancement of remineralization in vitro and in vivo. In Factors Affecting De-and Remineralization of the Teeth, 1st ed.; Leach, S.A., Ed.; IRL Press: Oxford, UK, 1986; pp. 23–34. [Google Scholar]
- Argenta, R.M.O.; Tabchoury, C.P.M.; Cury, J.A. A modified pH-cycling model to evaluate fluoride effect on enamel demineralization. Pesqui. Odontol. Bras. 2003, 17, 241–246. [Google Scholar] [CrossRef]
- Hayati, F.; Okada, A.; Kitasako, Y.; Tagami, J.; Matin, K. An artificial biofilm induced secondary caries model for in vitro studies. Aust. Dent. J. 2011, 56, 40–47. [Google Scholar] [CrossRef]
- Daneshmehr, L.; Matin, K.; Nikaido, T.; Tagami, J. Effects of root dentin surface coating with all-in-one adhesive materials on biofilm adherence. J. Dent. 2008, 36, 33–41. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Shimada, Y.; Matin, K.; Sadr, A.; Sumi, Y.; Tagami, J. Assessment of bacterial demineralization around composite restorations using swept-source optical coherence tomography (SS-OCT). Dent. Mater. 2016, 32, 1177–1188. [Google Scholar] [CrossRef]
- Gyo, M.; Nikaido, T.; Okada, K.; Yamauchi, J.; Tagami, J.; Matin, K. Surface response of fluorine polymer-incorporated resin composites to cariogenic biofilm adherence. Appl. Environ. Microbiol. 2008, 74, 1428–1435. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kiatsirirotea, K.; Sitthisettaponga, T.; Phantumvanit, P.; Chan, D.C.N. Fluoride-Releasing Effect of a Modified Resin Denture Containing S-PRG Fillers on Salivary Fluoride Retention: A Randomized Clinical Study. Caries Res. 2019, 53, 137–144. [Google Scholar] [CrossRef] [PubMed]
- Zafar, M.S. Effects of surface pre-reacted glass particles on fluoride release of dental restorative materials. World Appl. Sci. J. 2013, 28, 457–462. [Google Scholar]
- Svanberg, M.; Mjör, I.; Ørstavik, D. Mutans streptococci in plaque from margins of amalgam, composite, and glass-ionomer restorations. J. Dent. Res. 1990, 69, 861–864. [Google Scholar] [CrossRef]
- He, J.; Söderling, E.; Österblad, M.; Vallittu, P.K.; Lassila, L.V. Synthesis of methacrylate monomers with antibacterial effects against S. mutans. Molecules 2011, 16, 9755–9763. [Google Scholar] [CrossRef] [Green Version]
- Feuerstein, O.; Matalon, S.; Slutzky, H.; Weiss, E.I. Antibacterial properties of self-etching dental adhesive systems. J. Am. Dent. Assoc. 2007, 138, 349–354. [Google Scholar] [CrossRef] [Green Version]
- Da Rosa, W.L.d.O.; Piva, E.; da Silva, A.F. Bond strength of universal adhesives: A systematic review and meta-analysis, review and meta-analysis. J. Dent. 2015, 43, 765–776. [Google Scholar] [CrossRef]
- Carrilho, E.; Cardoso, M.; Marques Ferreira, M.; Marto, C.M.; Paula, A.; Coelho, A.S. 10-MDP Based Dental Adhesives: Adhesive Interface Characterization and Adhesive Stability-A Systematic Review. Materials 2019, 12, 790. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shimada, Y.; Sadr, A.; Burrow, M.F.; Tagami, J.; Ozawa, N.; Sumi, Y. Validation of swept-source optical coherence tomography (SS-OCT) for the diagnosis of occlusal caries. J. Dent. 2010, 38, 655–665. [Google Scholar] [CrossRef] [PubMed]
- Natsume, Y.; Nakashima, S.; Shimada, Y.; Sadr, A.; Tagami, J.; Sumi, Y. Estimation of lesion progress in artificial root caries by swept source optical coherence tomography in comparison to transverse microradiography. J. Biomed. Opt. 2011, 16, 071408. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Materials (Abbreviation) | Composition | Application Instructions | |
|---|---|---|---|
| Adhesive | Single Bond Universal® (SBU) 3M Espe, USA; Lot. 620316 | 10-MDP phosphate monomer, Vitrebond™ copolymer, HEMA, Bis-GMA, dimethacrylate resins, filler, silane, initiators, ethanol, water. | Apply the adhesive and rub it in for 20 s. Gently air dry for approximately 5 s. Light cure for 10 s |
| FL Bond II® (FL) Shofu, Kyoto, Japan; Lot. 101770 (primer) Lot. 101704 (bonding) | Primer: Water, ethanol, carboxylic acid monomer, phosphoric acid monomer and initiator. Adhesive: SPRG based on fluoroboro-aluminosilicate glass, UDMA, TEGDMA, 2-HEMA, initiator. | Apply primer, leave undisturbed for 10 s, air dry. Apply bonding agent, do not air dry. Polymerize for 5 s with LED. | |
| Composite | Beautifil II® (BEF) Shofu, Kyoto, Japan; Lot. 081695 | S-PRG fillers 68.6% w/v 83.3% w/w Bis-GMA, TEGDMA | Dispense in layers up to 2 mm in thickness. Light cure for 20 s. |
| Estelite® (EST) Tokuyama, Tokyo, Japan; Lot. E054 | Bis-GMA, TEGDMA Fillers: 82% wt, zirconia/silica particles | Dispense in layers up to 2 mm in thickness. Light cure for 20 s. | |
| Classification | Demineralization Pattern | Description | Attachment |
|---|---|---|---|
| Type A |  | The lesion is shallower near the restorations and deeper away from the restoration. | No Attachment loss |
| Type B |  | Type B is similar to Type A, but the lesion had a steeper drop near the restoration. | |
| Type C |  | The lesion is of similar depth regardless of distance from the restoration. | Attachment loss |
| Type D |  | The lesion is inverted: Narrow and deep along the restoration. |
| Test Groups | Type A | Type B | Type C | Type D |
|---|---|---|---|---|
| pHC Groups | ||||
| BEF/SBU | – | 100% | – | – |
| EST/SBU | – | – | – | 100% |
| BEF/FL | 37.5% | 62.5% | – | – |
| EST/FL | – | – | 75% | 25% |
| OBR Groups | ||||
| BEF/SBU | 37.5% | 37.5% | 25% | – |
| EST/SBU | – | – | 25% | 75% |
| BEF/FL | 75% | 25% | – | – |
| EST/FL | – | – | 63.5% | 37.5% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lai, Y.-J.; Takahashi, R.; Lin, P.-Y.; Kuo, L.; Zhou, Y.; Matin, K.; Chiang, Y.-C.; Shimada, Y.; Tagami, J. Anti-Demineralization Effects of Dental Adhesive-Composites on Enamel–Root Dentin Junction. Polymers 2021, 13, 3327. https://doi.org/10.3390/polym13193327
Lai Y-J, Takahashi R, Lin P-Y, Kuo L, Zhou Y, Matin K, Chiang Y-C, Shimada Y, Tagami J. Anti-Demineralization Effects of Dental Adhesive-Composites on Enamel–Root Dentin Junction. Polymers. 2021; 13(19):3327. https://doi.org/10.3390/polym13193327
Chicago/Turabian StyleLai, Yu-Jung, Rena Takahashi, Po-Yen Lin, Ling Kuo, Yuan Zhou, Khairul Matin, Yu-Chih Chiang, Yasushi Shimada, and Junji Tagami. 2021. "Anti-Demineralization Effects of Dental Adhesive-Composites on Enamel–Root Dentin Junction" Polymers 13, no. 19: 3327. https://doi.org/10.3390/polym13193327