Dose Limits and Countermeasures for Mitigating Radiation Risk in Moon and Mars Exploration



1
Biophysics Department, GSI Helmholtzzentrum für Schwerionenforschung, 64291 Darmstadt, Germany
2
Institute for Condensed Matter Physics, Technische Universität Darmstadt, 64289 Darmstadt, Germany
*
Author to whom correspondence should be addressed.
Physics 2022, 4(1), 172-184; https://doi.org/10.3390/physics4010013
Submission received: 29 November 2021
/
Revised: 18 January 2022
/
Accepted: 26 January 2022
/
Published: 9 February 2022
(This article belongs to the Special Issue Selected Papers from Applied Nuclear Physics Conference 2021)
Abstract
:After decades of research on low-Earth orbit, national space agencies and private entrepreneurs are investing in exploration of the Solar system. The main health risk for human space exploration is late toxicity caused by exposure to cosmic rays. On Earth, the exposure of radiation workers is regulated by dose limits and mitigated by shielding and reducing exposure times. For space travel, different international space agencies adopt different limits, recently modified as reviewed in this paper. Shielding and reduced transit time are currently the only practical solutions to maintain acceptable risks in deep space missions.
1. Introduction
Exposure to ionizing radiation is notoriously associated with early and late morbidity. Deterministic (nonstochastic) effects, such as skin burns and cataracts, are observed only at doses higher than a threshold, and their severity increases with the dose. Acute radiation burden in space can be a concern in the case of large solar storms, when doses could even be life threatening for an inadequately shielded crew. Stochastic effects do not seem to have a threshold, and their severity is independent of the dose. In radiation protection, the main concern for late stochastic effects is cancer induction, which can occur after a latency time of many years from exposure. As uncertainties in space radiation risk estimates are still substantially high, and effective countermeasures have not been developed, it is now generally acknowledged that space radiation is the main health risk for human space exploration [1], followed by the physiological effects of microgravity and the psychosocial effects of long confinement. The space radiation threat has substantially boosted research in space radiation risk. In the USA, National Aeronautics and Space Administration (NASA) is supporting the Space Radiation Health Program based at NASA Space Radiation Laboratory (NSRL) in the Brookhaven National Laboratory (BNL) [2], while in Europe, European Space Agency (ESA) is supporting experimental studies on space radiation shielding (ROSSINI) [3] and radiobiology (IBER) [4].
Considering their unavoidable exposure to space radiation during missions, astronauts are classified as radiation workers. The protection of radiation workers on Earth is far advanced and based on solid scientific evidence of epidemiological investigations [5]. The scientific evidence is used to estimate the risk of mortality and morbidity caused by radiation exposure. Ethical choices on acceptable risk have led to the establishment of exposure limits for both the general population and radiation workers. The current recommendations for radiation limits on Earth are based on the latest International Commission on Radiological Protection (ICRP) report [6]. The main source of these recommendations is still the follow-up of the survivors of the atomic bombs dropped in Hiroshima and Nagasaki in 1945 [7]. However, A-bomb survivors were essentially exposed to acute doses of sparsely ionizing radiation (γ-rays with a small neutron contribution). The situation in space is different: The space radiation environment is mainly composed of energetically charged particles, from H to U, with energies of a few hundred MeV/n in Low-Earth Orbit (LEO), but exceeding the TeV/n in deep space, Beyond LEO (BLEO) [8]. The contribution of high-LET (linear energy transfer) heavy ions to the total equivalent dose in space is substantial [9], whereas exposure in Hiroshima and Nagasaki was mostly due to low-LET radiation. Cosmic radiation dose rates have been carefully measured on the International Space Station (ISS) [10], in deep space [11], and on the Mars surface [12], and are in the range of 0.5–2.0 mSv/day. Clearly, the dose rate in space is much higher than the terrestrial dose rate, but still belongs to the low-dose rate region where the sparing effect applies [13]. Uncertainties in space radiation risk are very large as most epidemiological data are confined to high dose rates and low-LET radiation (such as in the A-bomb survivors), whereas space radiation exposure is characterized by low dose rates and high-LET radiation. How to extrapolate from one environment to the other is still poorly understood, in spite of considerable experimental work that has been carried out in the past few decades [14].
Epidemiological studies on astronauts’ mortality do not contribute to our knowledge of space radiation risk. In fact, the population of astronauts is relatively small, and most of them were involved in short-term LEO missions resulting in very low doses. Moreover, astronauts live longer than the general population, as expected from the healthy worker effect [15].
Space radiation experiments can fill these gaps, but spaceflight experiments on space radiation biological effects are difficult to repeat and generally limited to in vitro cells. It can be stated that almost everything we know on space radiation effects has been measured in ground experiments with high-energy accelerators [16]. This implies that the extrapolation to human risk is particularly complex, because we have to translate in vitro or animal data into human risk. This is not uncommon in radioprotection. For instance, the quality factors , for a specific radiation type and energy R, used to weight the physical dose (in Gy) in the calculation of the equivalent dose (in Sv) in a tissue T are essentially based on experiments in cells and animals [6]. However, for space radiation risk assessment, there are many sources of uncertainty, eventually leading to very large confidence intervals on risk estimates for different mission scenarios [9]. For this very reason, dose limits should not only consider the acceptable risk but also the uncertainty of the estimated risk,
2. Dose Limits
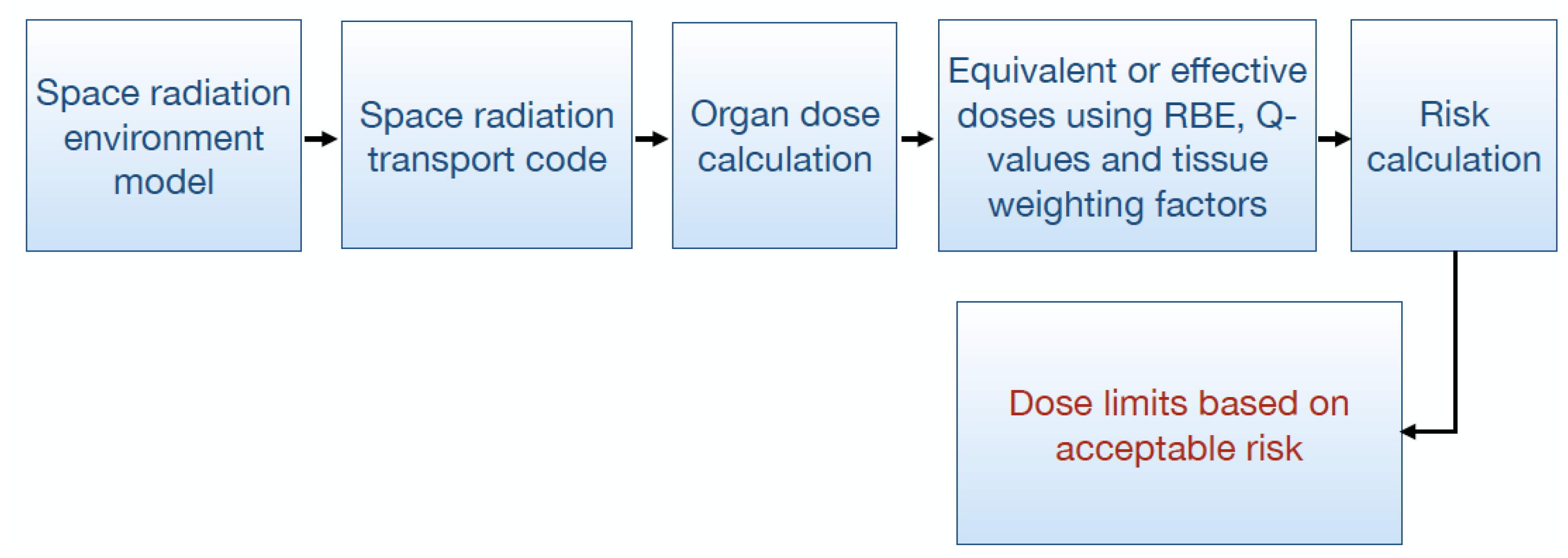
Dose limits are based on acceptable risk. The acceptable risk can depend on the circumstances. For instance, ICRP [6] recommends a limit of 1 mSv/year for the general population, but up to 20 mSv/year for radiation workers. In the case of nuclear accidents, exceptional exposures up to 100 mSv are acceptable for the liquidators involved and committed to containing the accident. The limits are based on the assumption that radiation exposure causes an excess lifetime detriment risk of 5% Sv−1. In principle, different effects are evaluated in the calculation of detriment, including hereditary effects, but the life detriment is largely dominated by cancer mortality, whose data are well established from the A-bomb survivor database [17,18]. Ethical considerations support the concept that dose limits should be based on acceptable risk for astronauts, too. The attempts to dismiss all the limits and to resort to e.g., informed consent has been generally dismissed due to the ALARA principle [19,20]. Taking all these factors into account, the path for the calculation of the dose limits is given in Figure 1. The first step is essentially the calculation of the dose for a given mission scenario. This step requires dosimetry and radiation transport calculations. Different agencies use different radiation transport models, some based on deterministic codes and others on Monte Carlo codes. The codes are affected by substantial uncertainties, generally linked to the limited knowledge of specific cross-sections [21]. The main uncertainty is related to the relative biological effectiveness (RBE) of space radiation [9], given the lack of epidemiological data. Some information can, however, be extracted from charged particle therapy in oncology, even if the dose and dose-rate regimes are substantially different [22].
The following steps are more related to biology and epidemiology, they have higher uncertainties, and different approaches can be used for the calculations. We will review the different approaches used by the agencies in the next sections.
2.1. NASA
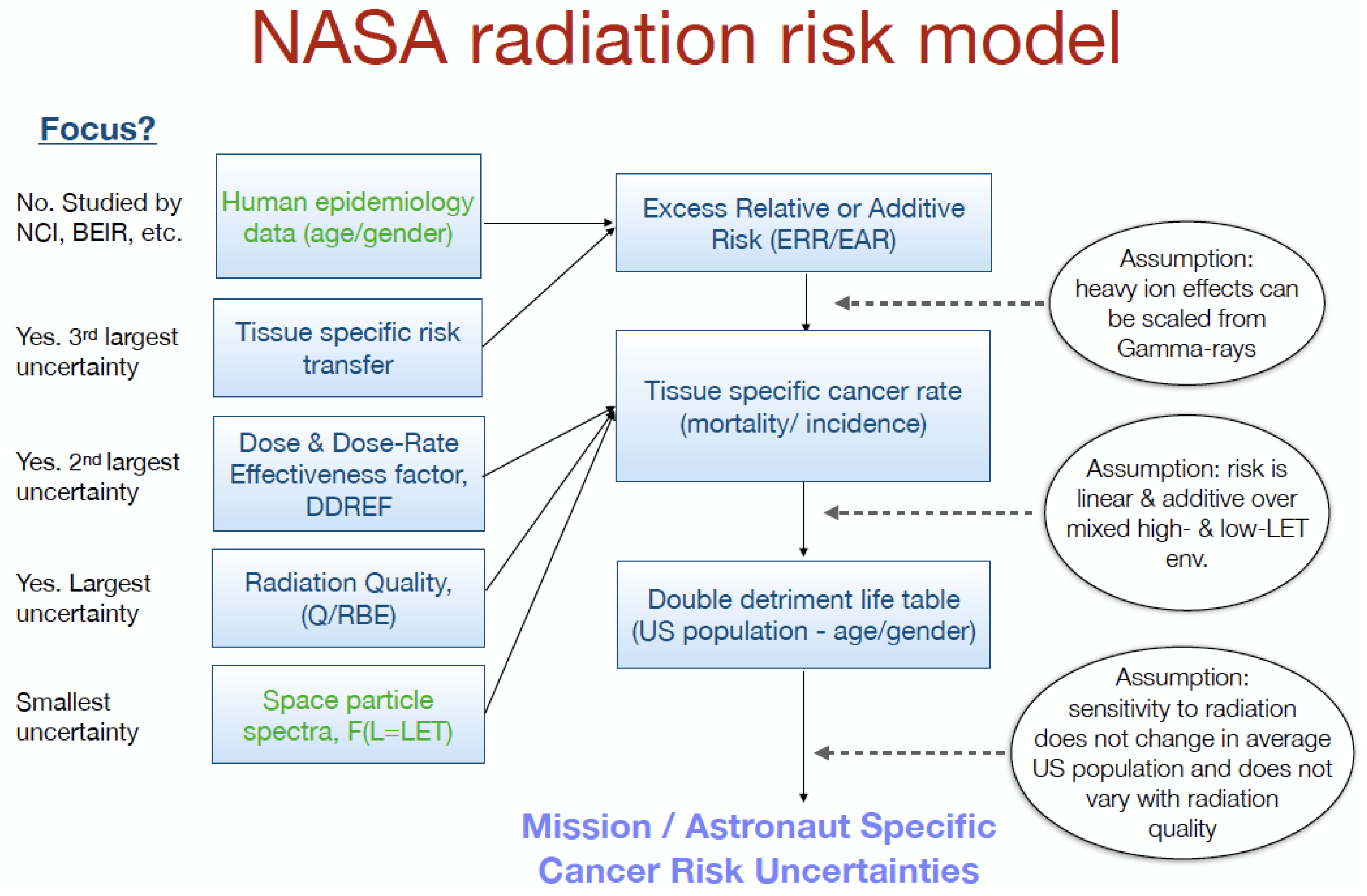
Until 2020, NASA was using the NASA Space Cancer Risk (NSCR) model NSCR-2012 [23] for estimating dose limits in LEO (Figure 2).
Recommendations by the US National Council on Radiation Protection and Measurements (NCRP) have guided NASA in the development of a risk-based system for radiation protection that limits individual occupational radiation exposures to a lifetime 3% excess risk of cancer death [24]. NCRP has noted that the large uncertainties in estimating the health risks for heavy ions preclude the assignment of exposure limits for long-term deep-space missions until further information is obtained [24,25]. Mission safety can only be predicted within a defined confidence level corresponding to the statistical nature of such a calculation. Large uncertainties limit the value of a median projection or so-called central estimate. The limited understanding of HZE (high-Z and energy) particle radiobiology contributes to the large uncertainty for predicting space radiation effects, which is the major difference between space- and ground-based radiation exposures. Permissible exposure limits for exploration missions have been implemented at NASA based on the NCRP recommendations for organ dose methodologies and point estimates for cancer risks; however, NASA applies these with an ancillary requirement to protect against the upper-bound of the 95% confidence level of risk projection. The NSCR-2012 model therefore calculates the risk of exposure-induced death (REID) as:
where hc (a|e, D) is the excess mortality rate at age a due to cause c attributable to radiation exposure with dose D at age e. The excess risk at age a is expressed as
since the survival function with radiation exposure S*(a|e, D) is applied to both exposed and non-exposed persons.
hc (a|e, D) S*(a|e, D) = μc*(a|e, D) S*(a|e, D) − μc (a) S*(a|e, D)
NASA therefore adopted sex- and age-specific career limits based on 3% REID within 95% confidence interval (CI), resulting in the doses in Table 1 for a 1-year mission.
However, NASA has considered revising the dose limits for several reasons. First, the current limits only apply to LEO; second, the gender difference may create an unequal work environment; and, third, NASA limits are substantially lower than those of other agencies (see below), leading to hindrances in planning international missions. In July 2021, the National Academy of Sciences [27] has supported the view that NASA should use a maximum allowable effective dose determined by applying the cancer risk model NSCR 2012 to the most susceptible case: a 35-year-old female. This corresponds to a 600-mSv gender- and age-independent limit. NASA is now implementing this new dose limit, even if the scientific community is concerned by the new limit, especially because it does not consider the uncertainty [28].
2.2. RSA
The Russian space agency (RSA) model started to be developed already in the 1960s and is a risk model that includes noncancer effects in the risk calculation, and even the impact of the space environment (microgravity) on the radiation effect [29,30,31]. The 1 Sv limit, agreed with the ISS partner in the Medical Operation Board, was actually chosen in an attempt to harmonize the limits with ESA, but it actually corresponds to an excess fatality risk (cancer + noncancer) around 7%, i.e., higher than the 3% recommended by NCRP to NASA.
Parameters in the RSA model are dose, radiation risk, and lifetime reduction when qualitatively estimating the effects induced by radiation. In addition, radiobiological effects of in-flight and later effects on organs have been considered. Acute exposure from γ-rays is well documented and studied, including its dose–time relations. From those data, the probability of in-flight and late effects from the radiation exposure and their damaging effects have been established. Irradiation in space is considered here to be irregular in dose distribution and time. Therefore, the expression for the risk should include a parameter as a function of time.
The generalized dose H (a Russian analogue of the ICRP effective dose [32]) in the standard irradiation on Earth is calculated as
where i indicates the i-th source of radiation hazard; H is the generalized dose in Sv; is the mean tissue absorbed dose; QF is the quality factor of radiation; TF is a temporal non-uniformity coefficient of irradiation, accounting for the dose rate and converting the effects that are induced by fractionated and chronic irradiation into a single acute exposure; SF is the coefficient of spatial non-uniformity of irradiation, to convert the nonuniform irradiation effects to a uniform exposure; and MF is a modification coefficient for non-radiation factors of space flight, such as hypergravity, microgravity, hypobaric hypoxia, and psychological stress.
Following the original definition of the generalized dose in Equation (4) and the calculation of the coefficients based on animal and/or spaceflight experiments, the total radiation risk is finally defined as
where noncancer effects are directly included in the risk calculation.
Mice, rat, and dog ground-based experiments were used to obtain experimental data for calculating the total radiation risk as a function of the mean and generalized dose, from Equation (4), as presented in Table 2. For the generalized dose, the GCR contribution was 30% of the total dose, and preflight medical procedure contributions were taken to be 25 cSv. This means that the data in Table 2 really apply to LEO only. The career limit in LEO was set at a total risk of 7%, corresponding to an equivalent dose of 1 Sv independent of age and gender.
The total radiation risk and the consequent mean lifetime reduction are therefore used as the criteria for the dose limits. This model implies that the total radiation risk in Table 2 does not depend on the age of the cosmonaut. The radiation cancer risk is age dependent but is smaller than the total radiation risk and is therefore not sufficient to alone estimate later effects according to this model.
Russian standards have been reviewed in 2021 [33], with several changes to the tissue dose limits for the deterministic effect, but the maximum career effective dose remained at 1 Sv. The new recommendations apply again to LEO only.
2.3. ESA
The ESA has not yet developed a radiation risk assessment model, nor has it decided to follow the model of US or Russia. The dose limits are based on the recommendations of ICRP 60 issued in 1991 [34]. The astronaut career limit recommendations of ICRP were essentially based on the maximum exposure limit of 50 mSv/y for radiation workers, assuming a maximum astronaut career of 20 years. This results in a career limit of 1 Sv, age- and gender-independent. The choice of this limit was originally accepted by the International Medical Operation Board as temporary and subject to revision [10]. However, it has remained unchanged over the past 20 years, even though ICRP has since reduced the maximum annual dose for terrestrial workers to 20 mSv/y [6]. It was originally the task of the ICRP to produce specific recommendations for spaceflight, but even though Publication 123 [35] provided sophisticated tools for the calculation of organ-equivalent doses, it did not find agreement for a dose-limit recommendation.
At the time of Publication 123, NASA had already developed its scientifically advanced risk model described in Section 2.1, Russia was using their own model described in Section 2.2, and any attempt to find a common standard was hampered by the acknowledged uncertainties in risk estimates, mostly due to space radiation quality [36]. Meanwhile, the ESA Topical Team on Space Radiation [4] recommended developing a European risk model based on European expertise in the different boxes shown in Figure 1. In fact, Europe has specific expertise in Monte Carlo [37] and deterministic [38] transport particle radiation transport codes; RBE models based on amorphous track structure [39] or microdosimetry [40]; and epidemiological analysis leading to a reduction in the uncertainties of cancer risk derived from the A-bomb and other cohorts [41].
Following the Topical Team recommendations, European scientists have recently proposed a space radiation risk model based on a different metric [42], the radiation-attributed decrease of survival (RADS), defined as:
where S (a|e) is the conditional survival at age a for those who have already survived up to age e while the survival function with radiation exposure S*(a|e, D) and the hazard function are expressed as:
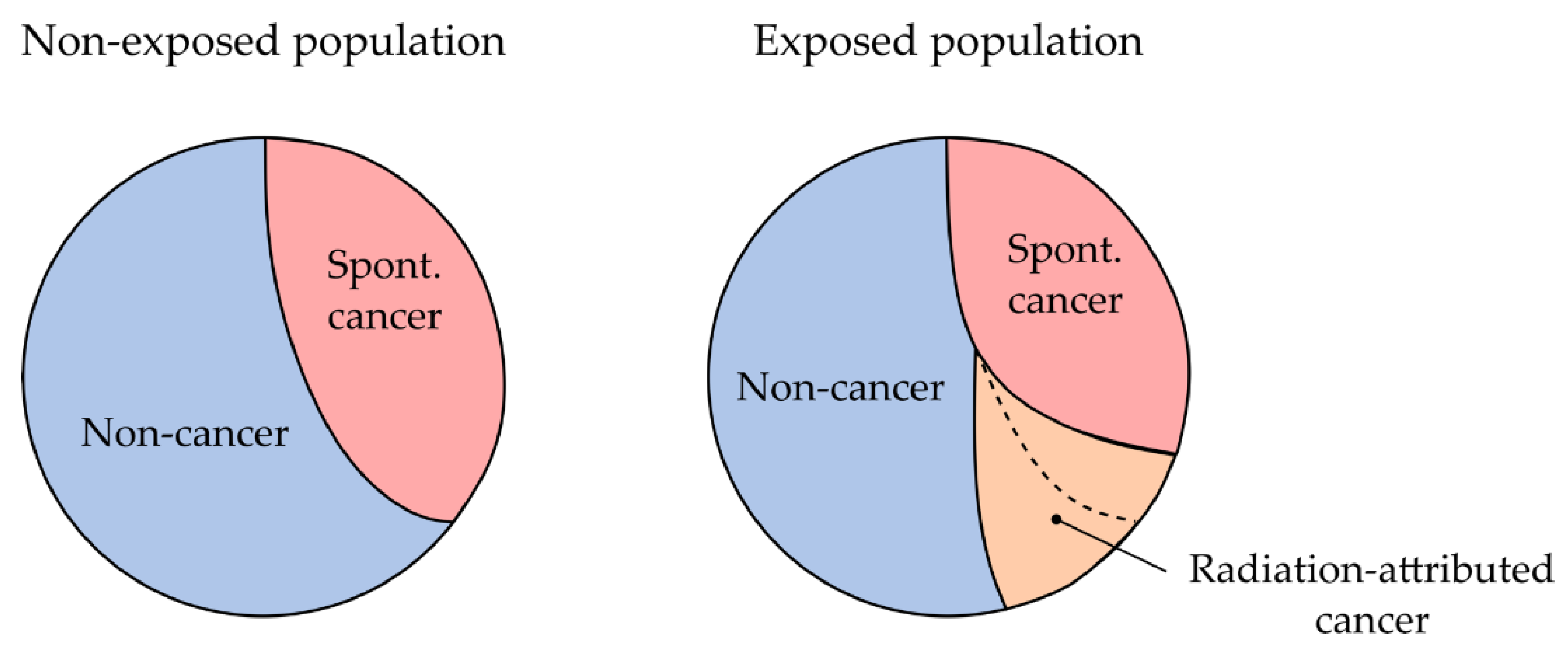
RADS is historically known as the cumulative risk. Unlike other risk metrics, RADS is independent of survival function. It is interpreted as the relative reduction in survival probability at a certain age due to radiation exposure. In REID, the baseline rates are the same for exposed and unexposed populations, and this creates a bias at high doses (Figure 3), relevant for exploration missions [43]. This bias is removed in RADS.
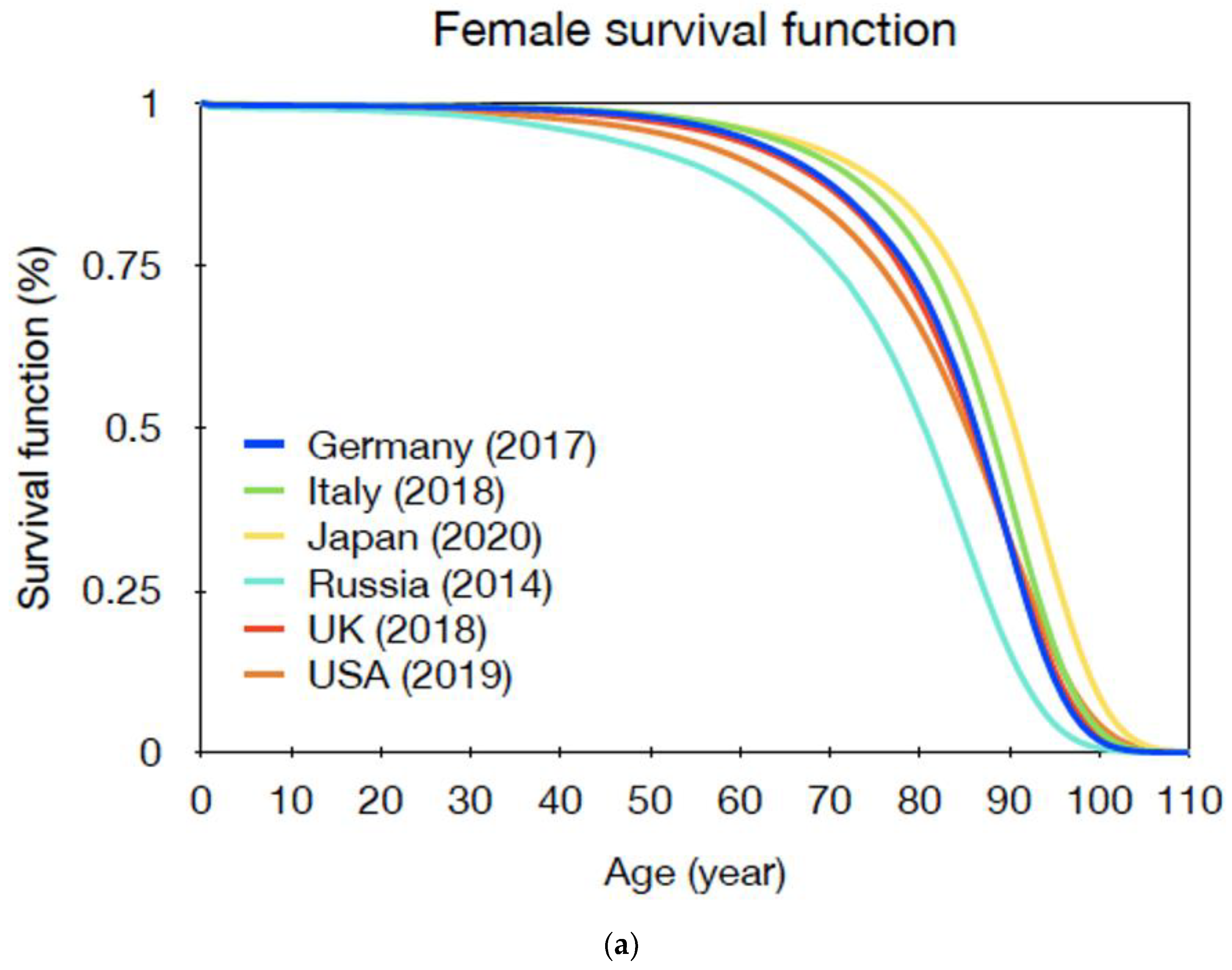
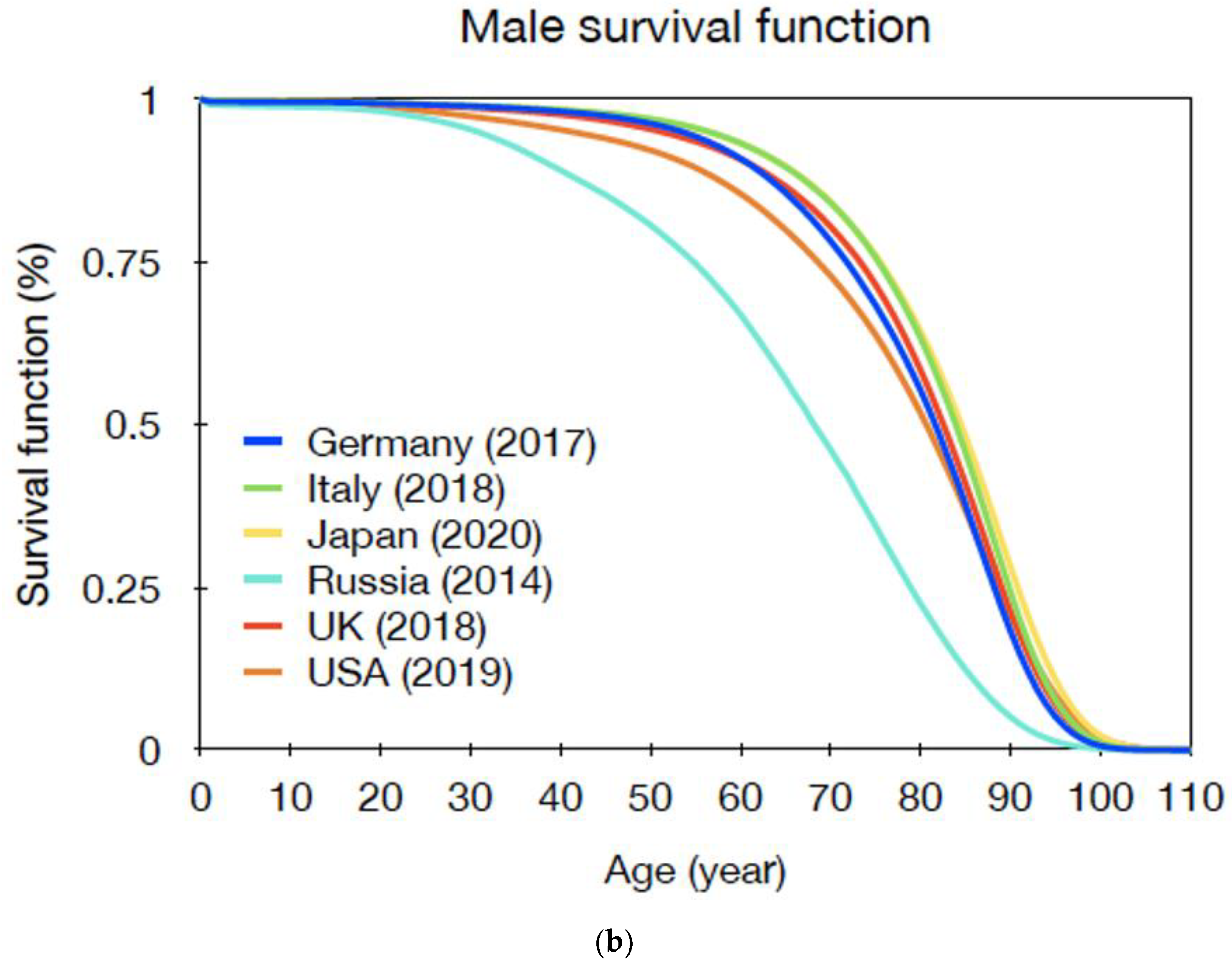
However, the independence of RADS from survival function does not mean it is free from demographic health statistics, which can be very variable (Figure 4) [44]. Information about baseline cancer risk is required when a relative risk model is used to estimate the excess risk due to radiation exposure. Moreover, RADS does not take into account competing risks, which play a role in modifying the chance that the event of interest occurs. As a result, RADS continues to increase with age as long as the excess risk remains positive, and this feature makes it difficult to assess its significance based on a comparison with the baseline risk. Notwithstanding these limitations, RADS seems to have large potential as a risk metric for long-term exploratory missions.
2.4. JAXA
The Japanese space agency (JAXA) is following the NCRP recommendation [24] of adopting a dose limit based on a 3% excess cancer risk mortality. Lifetime cancer mortality (LCM) is the metric used for calculating risks of radiation to Japanese astronauts in JAXA:
Here, is the natural mortality at age for all death of Japanese in 2007, and is the cancer mortality at age attributed to radiation exposure of dose at age . Mean values of cancer mortalities from excess relative (ERR) and the absolute (EAR) risk model are used for calculating of solid cancer. On the other hand, cancer mortalities from the EAR model are used for calculating that of leukemia. ERR and EAR are extracted from the A-bomb survivor database.
The limits are close to those previously adopted by NASA (Table 1) and converge to ESA and RSA limits for male astronauts older than 45.
2.5. CSA
The Canadian Space Agency (CSA) decided to follow ESA in the determination of the dose limits. For this reason, the career limit is set at 1 Sv, with the justifications provided in Section 2.3. However, Canadian Nuclear Laboratories are examining an alternative health-risk metric termed Disability Adjusted Life Year (DALY) [46]. One DALY is equivalent to one year of healthy-life lost and is given as the sum of years of life lost (YLL) due to premature mortality and years lived with disability (YLD) due to morbidity (Table 4). The DALY is well established in population health studies to assess the global burden of diseases [47]. Similar metrics are also widely used by healthcare practitioners for decisions regarding medical treatment effectiveness.
The proposal deserves special attention because DALY is intuitive and easy to communicate, focuses on the quality of life rather than on a generic risk that can occur at any time in life, and places radiological risk in a context with other risks. DALY was already proposed as a metric of radiation health risk [48], and the authors suggested that it is superior to the concept of “detriment” used by ICRP [49]. Of course, DALY still requires the data used in REID, RADS, or LCM metrics.
3. ICRP
At the time of the issue of ICRP Publication 123 [35], ESA astronauts’ space missions were limited to ISS with a maximum duration of approximately 3 months. With these missions, the estimated doses are not even close not only to the ESA/RSA limits, but also to the restrictive NASA limits. The situation changed with the plans for the 1-year mission, where previous NASA limits could lead to the exclusion of some crewmembers, especially women with previous flight experience [50], whereas ESA limits would allow essentially any astronaut to participate. With the Mars Science Laboratory (MSL) measurements demonstrating that the mission to Mars would approach 1 Sv [11], the problem became even more clear because essentially no NASA astronauts would be allowed to join a Mars mission today, whereas the ESA and RSA astronauts would be close to the maximum dose [51]. Presently, no limits for BLEO are established by any Agency, so this extrapolation is formally incorrect, yet the advances in exploration plans for the Moon and Mars clearly also attracted attention from the media and the public to the problem of space radiation in Solar-system exploration and in particular on the lack of a consensus. Since space agencies acknowledge that a mission to Mars should be International [52], involving at least US, Russia, and Europe, the problem of the different dose standards has become a priority in the 21st century.
An additional problem is that, with the notable exception of RSA, all career dose limits described above are essentially based on cancer mortality. Normal tissue damage is only accounted for by short-term, deterministic limits (see Ref. [26] for a review of the deterministic limits used by different agencies) but late degenerative effects are not included in career limits. The risk of cardiovascular disease (CVD) is considered a major uncertainty in radiation protection on Earth [53] and in space [54], and space radiation seems to be exquisitely effective in inducing central nervous system (CNS) damage [55], while the brain is generally considered radioresistant. NASA is currently assuming a threshold of 500 mGy-Eq. for CVD and 100 mGy for z > 10 for CNS effects. These limits should be within the 600 mSv limit based on 3% cancer mortality, but the uncertainty of RBE of space radiation is even larger for normal tissue degenerative effects than for carcinogenesis. In addition, the individual radiosensitivity of the crewmembers is currently ignored [56]. Some information on this issue can be derived from radiation oncology, where they are also actively studied [22].
To try to harmonize the different approaches used internationally, the ICRP established a new task group (TG115) with the primary goal of developing a comprehensive framework for risk and dose assessment for the radiological protection of astronauts, which might also be of relevance for space tourism. TG115 will build on ICRP Publication 123 [35] but will provide an assessment of the use of risk as a radiological protection quantity and recommendations for a uniform approach to dose limits.
4. Countermeasures
Dose limits are designed to allow space exploration with an acceptable radiation risk. However, ALARA should also be considered in any mission design, regardless of the limits. This means that possible countermeasures should always be explored, and their design should at least maintain the dose—and risk—within the limits. Biological countermeasures (radioprotective drugs) are currently under investigation, but none have been approved for use in astronauts [57]. On the other hand, the simplest physical countermeasure available is shielding, but it is notoriously problematic in space, due to the high energy of the galactic cosmic rays and the severe weight limitations in spaceflight [58]. Shielding, is, however, an effective countermeasure for solar particle events [59]. Assuming a 1 Sv dose limit, it has been recently estimated that a mission to Mars in the solar maximum with 30 g/cm2 Al-shielding can have a maximum duration of 4 years, while the new NASA limit of 600 mSv would be reached in approximately 2 years [60]. The results are interesting, but show the risk of using the maximum dose limit, and not ALARA, for the mission design. ICRP has repeatedly stated that limits are useful practical quantities but they should not be used for design, where ALARA consideration should prevail. As noted above, the limit of 1 Sv is not based on solid scientific grounds and is associated with a substantial risk uncertainty, which makes uncertainty-independent estimates quite risky for long-term BLEO missions [28]. Shielding optimization can be largely improved using different materials, particularly light, highly hydrogenated materials that can be tested at ground-based accelerators [3,61,62,63]. Ground-based measurements are also very useful in benchmarking Monte Carlo transport codes that are eventually used for predicting the doses in different mission scenarios [21].
Shielding using in situ planetary resources has large potential considering that the weight limits do not apply and that, in principle, humans can establish bases in deep pits, caves, or lava tubes [64]. This implies that the most effective countermeasure will be reducing the transit time i.e., innovative propulsion [65]. There is a general agreement that a mission to Mars cannot rely on chemical propulsion, and innovative strategies should be pursued, namely:
- -
- nuclear propulsion,
- -
- plasma,
- -
- ionic thrusters.
A recent review of nuclear propulsion technology (both thermal and electric) technologies concluded that nuclear-powdered spacecrafts offer great potential, but still require substantial ground-based R&D (Research and Development) [66]. NASA has recently invested over 10 M$ in this research. Potentially, nuclear thermal energy may reduce the transit time to Mars to only 3 months, and the effective dose in the solar maximum with a conventional 20 g/cm2 shielding would drop below 100 mSv [67].
Plasma thrusters are electrical engines based on the acceleration of ionized gas in an electromagnetic field. They are already used for satellite maneuvers in space, but they are less powerful than chemical thrusters. However, it is theoretically possible to produce plasma thrusters with an exhaust velocity 10× the current ones, exploiting a toroidal magnetic field similar to those used at tokamak for nuclear fusion [68]. The exhaust velocity of plasmoids can be increased or decreased by changing the strength of the magnetic fields rather than a conventional electric field increase that only produces low specific impulses.
Ion thrusters, based on ion acceleration, can be as fast as chemical propulsion, but much more efficient [69]. They are also currently used by satellites in space. While most Hall thrusters in space operations are based on xenon gas, it has recently been shown that it can be replaced with iodine, which is cheaper and can be stored in solids [70].
Unfortunately, a drastic reduction of travel time seems to be unlikely with the current technologies, including ion and nuclear thrusters. R&D in this field is highly needed, as reducing the time is also the best countermeasure against morbidity caused by radiation, microgravity, and isolation.
5. Conclusions
While space radiation is generally acknowledged as the main health risk in human space exploration, there is no international agreement on the dose limits for the crewmembers of exploratory-class missions. We do not have a common international astronauts’ career dose limit in Low-Earth Orbit (LEO), emerging private players are currently not subject to the space agencies’ limits, limits are not well defined in Beyond LEO (BLEO), and hardly any consideration of noncancer risks is included. International Commission on Radiological Protection task group (ICRP TG115) is currently reviewing the different strategies to issue recommendations toward a uniform approach. Limits are necessary to design appropriate countermeasures, such as shielding or reduced travel time, but considering the large uncertainties in space radiation risk, they should be regarded as extreme cases and not as design parameters. Ground-based research in space radiobiology, shielding material development and testing, and rocket propulsion is urgently needed to follow the short-term ambitious exploration plans.
Author Contributions
Search for literature, M.D. and D.B.; writing—original draft preparation, M.D.; writing—review and editing, M.D. and D.B. All authors have read and agreed to the published version of the manuscript.
Funding
This work was funded by ESA under the ERFNet contract.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Chancellor, J.; Scott, G.; Sutton, J. Space Radiation: The number one risk to astronaut health beyond low Earth orbit. Life 2014, 4, 491–510. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- La Tessa, C.; Sivertz, M.; Chiang, I.H.; Lowenstein, D.; Rusek, A. Overview of the NASA space radiation laboratory. Life Sci. Space Res. 2016, 11, 18–23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giraudo, M.; Schuy, C.; Weber, U.; Rovituso, M.; Santin, G.; Norbury, J.W.; Tracino, E.; Menicucci, A.; Bocchini, L.; Lobascio, C.; et al. Accelerator-based tests of shielding effectiveness of different materials and multilayers using high-energy light and heavy ions. Radiat. Res. 2018, 190, 526–537. [Google Scholar] [CrossRef] [PubMed]
- Walsh, L.; Schneider, U.; Fogtman, A.; Kausch, C.; McKenna-Lawlor, S.; Narici, L.; Ngo-Anh, J.; Reitz, G.; Sabatier, L.; Santin, G.; et al. Research plans in Europe for radiation health hazard assessment in exploratory space missions. Life Sci. Space Res. 2019, 21, 73–82. [Google Scholar] [CrossRef]
- Mullenders, L.; Atkinson, M.; Paretzke, H.; Sabatier, L.; Bouffler, S. Assessing cancer risks of low-dose radiation. Nat. Rev. Cancer 2009, 9, 596–604. [Google Scholar] [CrossRef] [PubMed]
- ICRP. The 2007 Recommendations of the International Commission on Radiological Protection. Publication 103. Ann. ICRP 2007, 37, 1–332. Available online: https://www.sciencedirect.com/journal/annals-of-the-icrp/vol/37/issue/2 (accessed on 25 January 2022).
- Preston, D.L.; Shimizu, Y.; Pierce, D.A.; Mabuchi, K. Studies of mortality of atomic bomb survivors. Report 13: Solid cancer and noncancer disease mortality: 1950–1997. Radiat. Res. 2003, 407, 381–407. [Google Scholar] [CrossRef]
- Durante, M.; Cucinotta, F.A. Physical basis of radiation protection in space travel. Rev. Mod. Phys. 2011, 83, 1245–1281. [Google Scholar] [CrossRef]
- Durante, M.; Cucinotta, F.A. Heavy ion carcinogenesis and human space exploration. Nat. Rev. Cancer 2008, 8, 465–472. [Google Scholar] [CrossRef]
- Straube, U.; Berger, T.; Reitz, G.; Facius, R.; Fuglesang, C.; Reiter, T.; Damann, V.; Tognini, M. Operational radiation protection for astronauts and cosmonauts and correlated activities of ESA medical operations. Acta Astronaut. 2010, 66, 963–973. [Google Scholar] [CrossRef]
- Zeitlin, C.; Hassler, D.M.; Cucinotta, F.A.; Ehresmann, B.; Wimmer-Schweingruber, R.F.; Brinza, D.E.; Kang, S.; Weigle, G.; Bottcher, S.; Bohm, E.; et al. Measurements of energetic particle radiation in transit to Mars on the Mars Science Laboratory. Science 2013, 340, 1080–1084. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hassler, D.M.; Zeitlin, C.; Wimmer-Schweingruber, R.F.; Ehresmann, B.; Rafkin, S.; Eigenbrode, J.L.; Brinza, D.E.; Weigle, G.; Bottcher, S.; Bohm, E.; et al. Mars’ surface radiation environment measured with the Mars Science Laboratory’s Curiosity rover. Science 2014, 343, 1244797. [Google Scholar] [CrossRef] [Green Version]
- Rühm, W.; Woloschak, G.E.; Shore, R.E.; Azizova, T.V.; Grosche, B.; Niwa, O.; Akiba, S.; Ono, T.; Suzuki, K.; Iwasaki, T.; et al. Dose and dose-rate effects of ionizing radiation: A discussion in the light of radiological protection. Radiat. Environ. Biophys. 2015, 54, 379–401. [Google Scholar] [CrossRef]
- Durante, M. Space radiation protection: Destination Mars. Life Sci. Space Res. 2014, 1, 2–9. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, R.; Little, M.P.; Day, S.; Charvat, J.; Blattnig, S.; Huff, J.; Patel, Z.S. Cancer incidence and mortality in the USA Astronaut Corps, 1959–2017. Occup. Environ. Med. 2021, 78, 869–875. [Google Scholar] [CrossRef] [PubMed]
- Durante, M.; Kronenberg, A. Ground-based research with heavy ions for space radiation protection. Adv. Space Res. 2005, 35, 180–184. [Google Scholar] [CrossRef]
- Ozasa, K.; Shimizu, Y.; Suyama, A.; Kasagi, F.; Soda, M.; Grant, E.J. Studies of the mortality of atomic bomb survivors, Report 14, 1950–2003: An overview of cancer and noncancer diseases. Radiat. Res. 2012, 243, 229–243. [Google Scholar] [CrossRef] [Green Version]
- Grant, E.J.; Brenner, A.; Sugiyama, H.; Sakata, R.; Sadakane, A.; Utada, M.; Cahoon, E.K.; Milder, C.M.; Soda, M.; Cullings, H.M.; et al. Solid cancer incidence among the life span study of atomic bomb survivors: 1958–2009. Radiat. Res. 2017, 187, 513–537. [Google Scholar] [CrossRef] [Green Version]
- Shuchman, M. Striving for Mars: What are acceptable risks? CMAJ 2014, 186, E7–E8. [Google Scholar] [CrossRef] [Green Version]
- Kahn, J.; Liverman, C.T.; Mccoy, M.A. Health Standards for Long Duration and Exploration Spaceflight; National Academies Press: Washington, DC, USA, 2014. Available online: https://www.ncbi.nlm.nih.gov/books/NBK222144/ (accessed on 25 January 2022).
- Luoni, F.; Horst, F.; Reidel, C.A.; Quarz, A.; Bagnale, L.; Sihver, L.; Weber, U.; Norman, R.B.; de Wet, W.; Giraudo, M.; et al. Total nuclear reaction cross-section database for radiation protection in space and heavy-ion therapy applications. New J. Phys. 2021, 23, 101201. [Google Scholar] [CrossRef]
- Tinganelli, W.; Luoni, F.; Durante, M. What can space radiation protection learn from radiation oncology? Life Sci. Space Res. 2021, 30, 82–95. [Google Scholar] [CrossRef] [PubMed]
- Cucinotta, F.A.; Kim, M.H.Y.; Chappell, L.J. Space Radiation Cancer Risk Projections and Uncertainties—2012. Report NASA/TP-2013-217375; The NASA STI Program Office: Hanover, MD, USA, 2013. Available online: https://three.jsc.nasa.gov/articles/TP_2013_CancerRisk.pdf (accessed on 25 January 2022).
- NCRP. Radiation Protection Guidance for Activities in Low-Earth Orbit (2000); NCRP Report No. 132; NCRP: Bethesda, MD, USA, 2000; Available online: https://ncrponline.org/shop/reports/report-no-132 (accessed on 25 January 2022).
- NCRP. Information Needed to Make Radiation Protection Recommendations for Space Missions Beyond Low-Earth Orbit (2006); NCRP Report No. 153; NCRP: Bethesda, MD, USA, 2006; Available online: https://ncrponline.org/shop/reports/report-no-153 (accessed on 25 January 2022).
- McKenna-Lawlor, S.; Bhardwaj, A.; Ferrari, F.; Kuznetsov, N.; Lal, A.K.; Li, Y.; Nagamatsu, A.; Nymmik, R.; Panasyuk, M.; Petrov, V.; et al. Feasibility study of astronaut standardized career dose limits in LEO and the outlook for BLEO. Acta Astronaut. 2014, 104, 565–573. [Google Scholar] [CrossRef]
- National Academy of Sciences. Space Radiation and Astronaut Health; The National Academies Press: Washington, DC, USA, 2021. [CrossRef]
- Cucinotta, F.A.; Schimmerling, W.; Blakely, E.A.; Hei, T.K. A proposed change to astronaut exposures limits is a giant leap backwards for radiation protection. Life Sci. Space Res. 2021, 31, 59–70. [Google Scholar] [CrossRef]
- Petrov, V.M.; Kovalev, E.E.; Sakovich, V.A. Radiation: Risk and protection in manned space flight. Acta Astronaut. 1981, 8, 1091–1097. [Google Scholar] [CrossRef]
- Shafirkin, A.V.; Petrov, V.M.; Kolomensky, A.V.; Shurshakov, V.A. Lifetime total radiation risk of cosmonauts for orbotal and interplanetary flights. Adv. Space Res. 2002, 30, 999–1003. [Google Scholar] [CrossRef]
- Petrov, V.M. Radiation risk during long-term spaceflight. Adv. Space Res. 2002, 30, 989–994. [Google Scholar] [CrossRef]
- Menzel, H.-G.; Harrison, J. Effective dose: A radiation protection quantity. Ann. ICRP 2012, 41, 117–123. [Google Scholar] [CrossRef]
- ROSCOSMOS. Limitation of Cosmonaut Exposure during Near-Earth Space Flights; ROSCOSMOS: Moscow, Russia, 2021. [Google Scholar]
- ICRP. Recommendations of the International Commission on Radiological Protection. Publication 60. Ann. ICRP 1991, 21, 1–201. Available online: https://www.sciencedirect.com/journal/annals-of-the-icrp/vol/21/issue/1 (accessed on 25 January 2022).
- Dietze, G.; Bartlett, D.T.; Cool, D.A.; Cucinotta, F.A.; Jia, X.; McAulay, I.R.; Pelliccioni, M.; Petrov, V.; Reitz, G.; Sato, T. ICRP Publication 123: Assessment of radiation exposure of astronauts in space. Ann. ICRP 2013, 42, 1–339. [Google Scholar] [CrossRef]
- Cucinotta, F.A.; Durante, M. Cancer risk from exposure to galactic cosmic rays: Implications for space exploration by human beings. Lancet Oncol. 2006, 7, 431–435. [Google Scholar] [CrossRef] [Green Version]
- Agostinelli, S.; Allison, J.; Amako, K.; Apostolakis, J.; Araujo, H.; Arce, P.; Asai, M.; Axen, D.; Banerjee, S.; Barrand, G.; et al. Geant4—A simulation toolkit. Nucl. Instrum. Methods Phys. Res. Sect. A Accel. Spectrometers Detect. Assoc. Equip. 2003, 506, 250–303. [Google Scholar] [CrossRef] [Green Version]
- Krämer, M.; Durante, M. Ion beam transport calculations and treatment plans in particle therapy. Eur. Phys. J. D 2010, 60, 195–202. [Google Scholar] [CrossRef]
- Friedrich, T.; Scholz, U.; Elsässer, T.; Durante, M.; Scholz, M. Calculation of the biological effects of ion beams based on the microscopic spatial damage distribution pattern. Int. J. Radiat. Biol. 2012, 88, 103–107. [Google Scholar] [CrossRef] [PubMed]
- Chauvie, S.; Francis, Z.; Guatelli, S.; Incerti, S.; Mascialino, B.; Moretto, P.; Nieminen, P.; Pia, M.G. Geant4 physics processes for microdosimetry simulation: Design foundation and implementation of the first set of models. IEEE Trans. Nucl. Sci. 2007, 54, 2619–2628. [Google Scholar] [CrossRef] [Green Version]
- Schneider, U.; Walsh, L. Risk of secondary cancers: Bridging epidemiology and modeling. Phys. Med. 2017, 42, 228–231. [Google Scholar] [CrossRef] [PubMed]
- Walsh, L.; Hafner, L.; Straube, U.; Ulanowski, A.; Fogtman, A.; Durante, M.; Weerts, G.; Schneider, U. A bespoke health risk assessment methodology for the radiation protection of astronauts. Radiat. Environ. Biophys. 2021, 60, 213–231. [Google Scholar] [CrossRef]
- Ulanowski, A.; Kaiser, J.C.; Schneider, U.; Walsh, L. Lifetime radiation risk of stochastic effects—Prospective evaluation for space flight or medicine. Ann. ICRP 2020, 49, 200–212. [Google Scholar] [CrossRef]
- Shkolnikov, V.; Barbieri, M.; Wilmoth, J. Human Mortality Databse. Available online: https://www.mortality.org (accessed on 25 January 2022).
- Komiyama, T. Practicalities of dose management for Japanese astronauts staying at the International Space Station. Ann. ICRP 2020, 49, 194–199. [Google Scholar] [CrossRef]
- Devleesschauwer, B.; Havelaar, A.H.; Maertens de Noordhout, C.; Haagsma, J.A.; Praet, N.; Dorny, P.; Duchateau, L.; Torgerson, P.R.; Van Oyen, H.; Speybroeck, N. Calculating disability-adjusted life years to quantify burden of disease. Int. J. Public Health 2014, 59, 565–569. [Google Scholar] [CrossRef]
- Murray, C.J.L.; Lopez, A.D. Measuring the Global burden of disease. N. Engl. J. Med. 2013, 369, 448–457. [Google Scholar] [CrossRef] [Green Version]
- Shimada, K.; Kai, M. Calculating disability-adjusted life years (DALY) as a measure of excess cancer risk following radiation exposure. J. Radiol. Prot. 2015, 35, 763–775. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Breckow, J. Do we really need the “detriment” for radiation protection? Radiat. Environ. Biophys. 2020, 59, 343–348. [Google Scholar] [CrossRef] [PubMed]
- Cucinotta, F.A. Space radiation risks for astronauts on multiple international space station missions. PLoS ONE 2014, 9, e96099. [Google Scholar] [CrossRef]
- Durante, M.; Cucinotta, F.A. Cosmic Rays: Hurdles on the Road to Mars. Nucl. Phys. News 2014, 24, 32–34. [Google Scholar] [CrossRef]
- ISECG. The Global Exploration Roadmap. January 2018; NASA: Washington, DC, USA, 2018. Available online: https://www.nasa.gov/sites/default/files/atoms/files/ger_2018_small_mobile.pdf (accessed on 25 January 2022).
- Little, M.P.; Azizova, T.V.; Hamada, N. Low- and moderate-dose non-cancer effects of ionizing radiation in directly exposed individuals, especially circulatory and ocular diseases: A review of the epidemiology. Int. J. Radiat. Biol. 2021, 97, 782–803. [Google Scholar] [CrossRef]
- Hughson, R.L.; Helm, A.; Durante, M. Heart in space: Effect of the extraterrestrial environment on the cardiovascular system. Nat. Rev. Cardiol. 2017, 15, 167–180. [Google Scholar] [CrossRef]
- NCRP. Potential for Central Nervous System Effects from Radiation Exposure During Space Activities Phase I: Overview (2016); NCRP Commentary No. 25; NCRP: Bethesda, MD, USA, 2016; Available online: https://ncrponline.org/shop/commentaries/potential-for-central-nervous-system-effects-from-radiation-exposure-during-space-activities-phase-i-overview-2016/ (accessed on 25 January).
- NCRP. Potential Impact of Individual Genetic Susceptibility and Previous Radiation Exposure on Radiation Risk for Astronauts (2010); NCRP Report No. 167; NCRP: Bethesda, MD, USA, 2010; Available online: https://ncrponline.org/shop/reports/report-no-167 (accessed on 25 January).
- Kennedy, A.R. Biological effects of space radiation and development of effective countermeasures. Life Sci. Space Res. 2014, 1, 10–43. [Google Scholar] [CrossRef] [Green Version]
- Spillantini, P.; Casolino, M.; Durante, M.; Mueller-Mellin, R.; Reitz, G.; Rossi, L.; Shurshakov, V.; Sorbi, M. Shielding from cosmic radiation for interplanetary missions: Active and passive methods. Radiat. Meas. 2007, 42, 14–23. [Google Scholar] [CrossRef]
- Wilson, J.W.; Cucinotta, F.; Shinn, J.; Simonsen, L.; Dubey, R.; Jordan, W.; Jones, T.; Chang, C.; Kim, M. Shielding from solar particle event exposures in deep space. Radiat. Meas. 1999, 30, 361–382. [Google Scholar] [CrossRef]
- Dobynde, M.I.; Shprits, Y.Y.; Drozdov, A.Y.; Hoffman, J.; Li, J. Beating 1 Sievert: Optimal radiation shielding of astronauts on a mission to Mars. Space Weather. 2021, 19, e2021SW002749. [Google Scholar] [CrossRef]
- Miller, J.; Zeitlin, C.; Cucinotta, F.A.; Heilbronn, L.; Stephens, D.; Wilson, J.W. Benchmark studies of the effectiveness of structural and internal materials as radiation shielding for the international space station. Radiat. Res. 2003, 159, 381–390. [Google Scholar] [CrossRef] [Green Version]
- Schuy, C.; La Tessa, C.; Horst, F.; Rovituso, M.; Durante, M.; Giraudo, M.; Bocchini, L.; Baricco, M.; Castellero, A.; Fioreh, G.; et al. Experimental assessment of Lithium hydride’s space radiation shielding performance and Monte Carlo benchmarking. Radiat. Res. 2018, 191, 154. [Google Scholar] [CrossRef] [PubMed]
- Zeitlin, C.; Guetersloh, S.; Heilbronn, L.; Miller, J.; Elkhayari, N.; Empl, A.; LeBourgeois, M.; Mayes, B.W.; Pinsky, L.; Christl, M.; et al. Shielding experiments with high-energy heavy ions for spaceflight applications. New J. Phys. 2008, 10, 075007. [Google Scholar] [CrossRef]
- Viúdez-Moreiras, D. The ultraviolet radiation environment and shielding in pit craters and cave skylights on Mars. Icarus 2021, 370, 114658. [Google Scholar] [CrossRef]
- Czysz, P.A.; Bruno, C.; Chudoba, B. Future Spacecraft Propulsion Systems and Integration; Springer: Berlin/Heidelberg, Germany, 2018. [Google Scholar] [CrossRef]
- National Academy of Sciences. Space Nuclear Propulsion for Human Mars Exploration; National Academies Press: Washington, DC, USA, 2021. [CrossRef]
- Durante, M.; Bruno, C. Impact of rocket propulsion technology on the radiation risk in missions to Mars. Eur. Phys. J. D 2010, 60, 215–218. [Google Scholar] [CrossRef]
- Ebrahimi, F. An Alfvenic reconnecting plasmoid thruster. J. Plasma Phys. 2020, 86, 905860614. [Google Scholar] [CrossRef]
- Mazouffre, S. Electric propulsion for satellites and spacecraft: Established technologies and novel approaches. Plasma Sources Sci. Technol. 2016, 25, 033002. [Google Scholar] [CrossRef]
- Rafalskyi, D.; Martínez, J.M.; Habl, L.; Zorzoli Rossi, E.; Proynov, P.; Boré, A.; Baret, T.; Poyet, A.; Lafleur, T.; Dudin, S.; et al. In-orbit demonstration of an iodine electric propulsion system. Nature 2021, 599, 411–415. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
A simplified flowchart of the steps necessary to build a radiation risk model in space. RBE stands for the relative biological effectiveness.
Figure 1.
A simplified flowchart of the steps necessary to build a radiation risk model in space. RBE stands for the relative biological effectiveness.

Figure 2.
Building blocks of the NASA radiation risk model. Adapted from [23].
Figure 2.
Building blocks of the NASA radiation risk model. Adapted from [23].

Figure 3.
An illustration of cumulative risks in non-exposed (left) and exposed (right) populations. Additional hazards due to the radiation exposure reduce the cumulative risks of spontaneous cancers and other—non-cancer-related—competing diseases or mortality causes. Adapted from Ref. [43].
Figure 3.
An illustration of cumulative risks in non-exposed (left) and exposed (right) populations. Additional hazards due to the radiation exposure reduce the cumulative risks of spontaneous cancers and other—non-cancer-related—competing diseases or mortality causes. Adapted from Ref. [43].

Figure 4.
Survival functions for the general populations in different countries: (a) female survival function and (b) male survival function. Data from the Human Mortality Database, 2021 [44].
Figure 4.
Survival functions for the general populations in different countries: (a) female survival function and (b) male survival function. Data from the Human Mortality Database, 2021 [44].



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
NASA Space Cancer Risk NSCR-2012 model career effective dose limits (in Sv) age and gender specific, for 1 year mission. Exposure to radiation during the career of each astronaut is required to not exceed a 3% risk of exposure-induced death (REID) from fatal cancers. Adapted from Ref. [26].
Table 1.
NASA Space Cancer Risk NSCR-2012 model career effective dose limits (in Sv) age and gender specific, for 1 year mission. Exposure to radiation during the career of each astronaut is required to not exceed a 3% risk of exposure-induced death (REID) from fatal cancers. Adapted from Ref. [26].
| Gender | Age at Exposure | |||
|---|---|---|---|---|
| 30 | 40 | 50 | 60 | |
| Female | 0.60 | 0.70 | 0.82 | 0.98 |
| Male | 0.78 | 0.88 | 1.00 | 1.17 |
Table 2.
Russian career effective dose limits and comparison between generalized dose and equivalent doses. Adapted from Refs. [31,33].
| Calculated Values | Age [y] | Mean Tissue Equivalent Dose [cSv] | ||
|---|---|---|---|---|
| 100 | 125 | 150 | ||
| Generalized dose [cSv] | - | 53.8 | 65.6 | 100 |
| Total radiation risk [%] | - | 7.00 | 8.53 | 12.0 |
| Radiation risk of cancer [%] | 30 | 3.60 | 4.50 | 5.40 |
| 40 | 2.36 | 2.95 | 3.54 | |
| 50 | 1.83 | 2.29 | 2.74 | |
| Mean lifetime reduction [y] | 30 | 2.42 | 2.95 | 3.49 |
| 40 | 2.16 | 2.63 | 3.10 | |
| 50 | 1.89 | 2.30 | 2.71 | |
Table 3.
Japanese astronauts’ career effective dose limits in Sv. Adapted from Ref. [45].
Table 3.
Japanese astronauts’ career effective dose limits in Sv. Adapted from Ref. [45].
| Age at the First Space Flight | Female | Male |
|---|---|---|
| 27–30 | 0.5 | 0.6 |
| 31–35 | 0.6 | 0.7 |
| 36–40 | 0.65 | 0.8 |
| 41–45 | 0.75 | 0.95 |
| >45 | 0.8 | 1.0 |
Table 4.
Definition of disability-adjusted-life years (DALY) proposed by the Canadian Nuclear Laboratory as metrics for space radiation risk. Variables represent the cause of the disability (c), gender (s), attained age (a), year (t), number of deaths (N), life expectancy (LE), number of incidence cases (I), disability weight (DW), averaged duration of disability until remission/death (LD).
Table 4.
Definition of disability-adjusted-life years (DALY) proposed by the Canadian Nuclear Laboratory as metrics for space radiation risk. Variables represent the cause of the disability (c), gender (s), attained age (a), year (t), number of deaths (N), life expectancy (LE), number of incidence cases (I), disability weight (DW), averaged duration of disability until remission/death (LD).
| DALY(c,s,a,t) = TLD(c,s,a,t) + YLL(c,s,a,t) |
| YLL(c,s,a,t) = N(c,s,a,t) × LE(s,a) |
| YLD(c,s,a,t) = I(c,s,a,t) × DW(c,s,a) × LD(c,s,a,t) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Boscolo, D.; Durante, M. Dose Limits and Countermeasures for Mitigating Radiation Risk in Moon and Mars Exploration. Physics 2022, 4, 172-184. https://doi.org/10.3390/physics4010013
AMA Style
Boscolo D, Durante M. Dose Limits and Countermeasures for Mitigating Radiation Risk in Moon and Mars Exploration. Physics. 2022; 4(1):172-184. https://doi.org/10.3390/physics4010013
Chicago/Turabian StyleBoscolo, Daria, and Marco Durante. 2022. "Dose Limits and Countermeasures for Mitigating Radiation Risk in Moon and Mars Exploration" Physics 4, no. 1: 172-184. https://doi.org/10.3390/physics4010013