
Therapeutic Efficacy of a Formulation Prepared with Linum usitatissimum L., Plantago ovata Forssk., and Honey on Uncomplicated Pelvic Inflammatory Disease Analyzed with Machine Learning Techniques
 ,
,  ,
,  ,
,  ,
,
Abstract
:1. Introduction
- The pessary of psyllium and linseed with honey is beneficial for PID but has not been validated to date.
- The pessary group was beneficial, safe, and cost-effective in curing uPID as they possess anti-inflammatory, antimicrobial, analgesic, and antioxidant activities as proven in in vitro and in vivo studies.
- The design of an automatic classification model based on the experimental analysis of the pessary and standard groups on uPID occurring in reproductive-age women.
- The design of a detection system based on medicine using a machine-learning classifier.
2. Materials and Methods
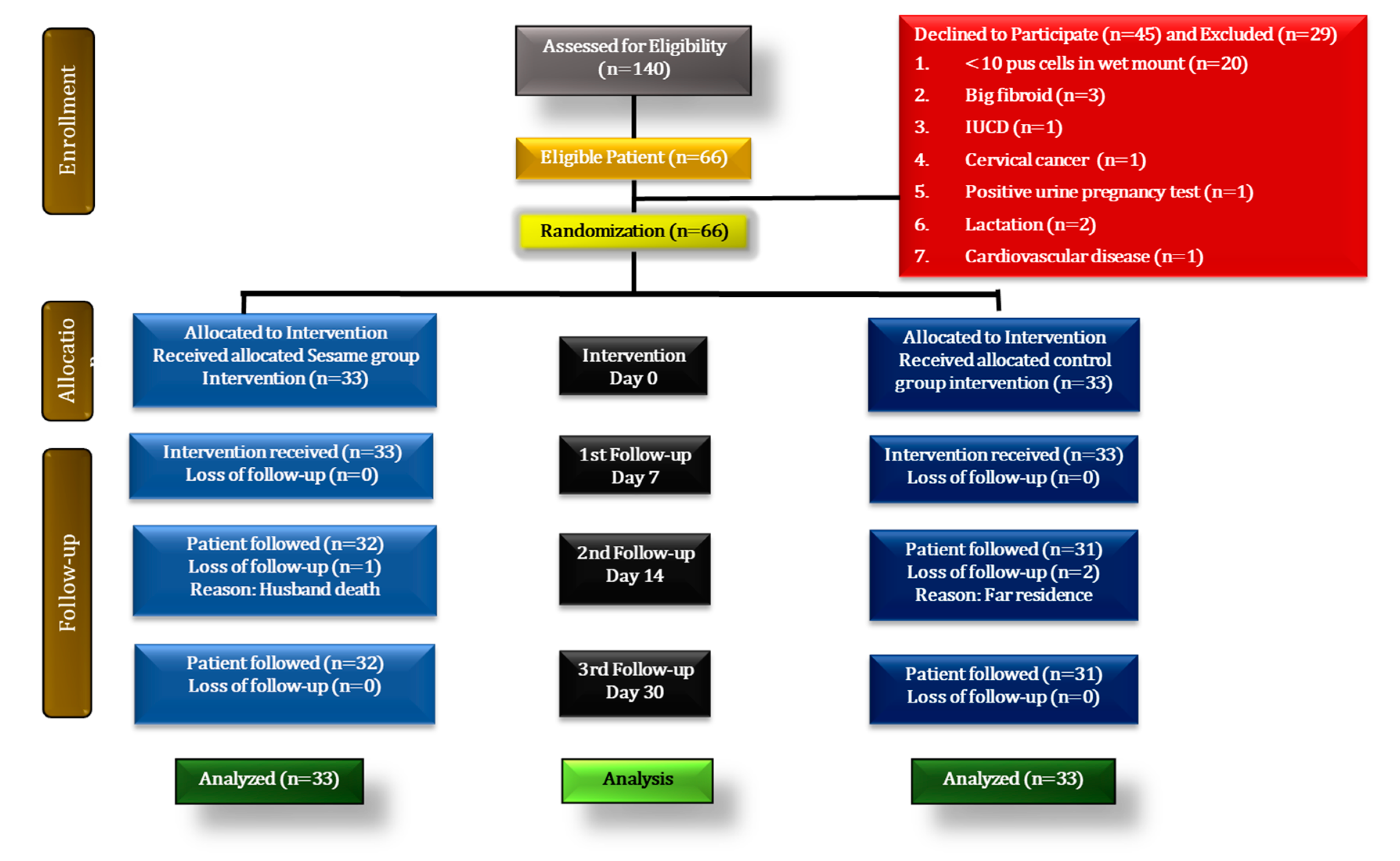
2.1. Study Design and Population
2.2. Data Collection and Assessment Tools
2.2.1. Data Collection
2.2.2. Assessment of Safety of Pessary and Standard Groups
2.2.3. Assessment of Haematological and Biochemical Markers
2.2.4. Follow-Up Assessment and Withdrawal Criteria
2.3. Intervention Used in Both Groups
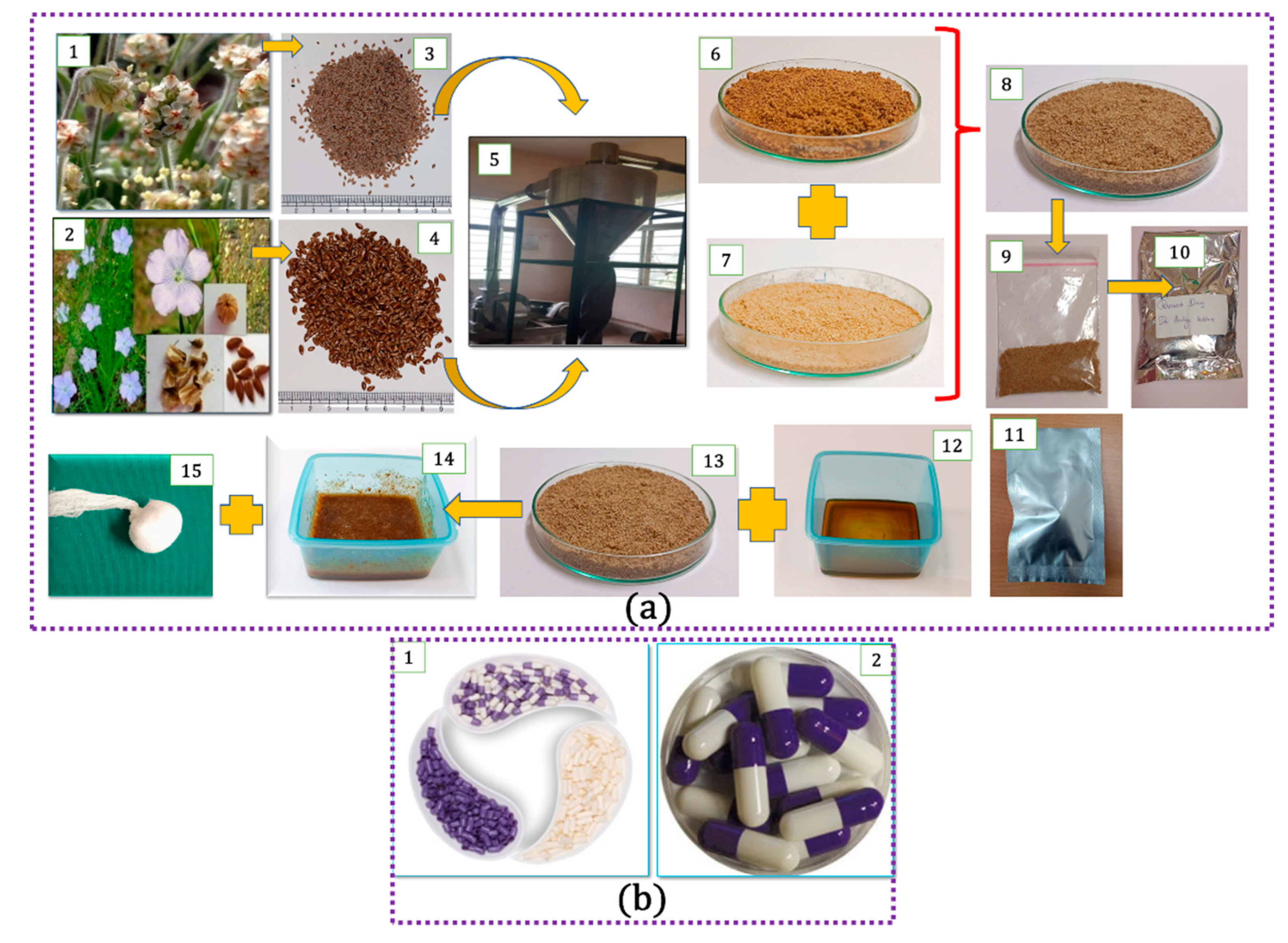
2.3.1. Selection and Identification
2.3.2. Method of Preparation, Dispensing, and Training of the Participants
2.3.3. Route of Administration and Dosage
2.3.4. Standard Controlled Group
2.4. Outcomes
2.5. Sample Size Estimation
2.6. Randomization, Allocation, Blinding, and Treatment Adherence
2.7. Statistical Methods
3. Results
3.1. Sociodemographic Characteristics
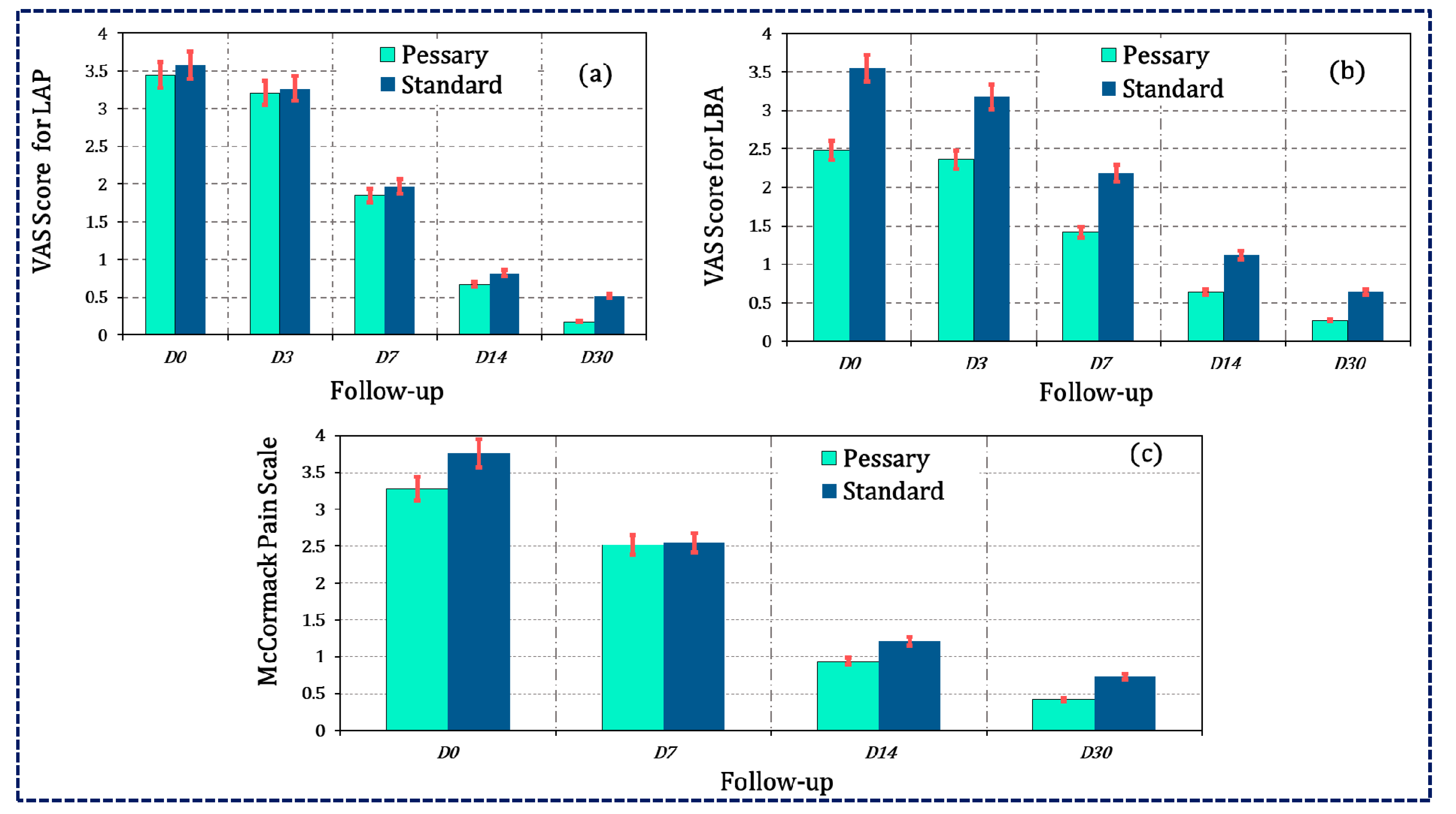
3.2. Primary Outcomes
3.3. Secondary Outcomes
3.3.1. WBC Count on Saline Microscopy of Vaginal Discharge
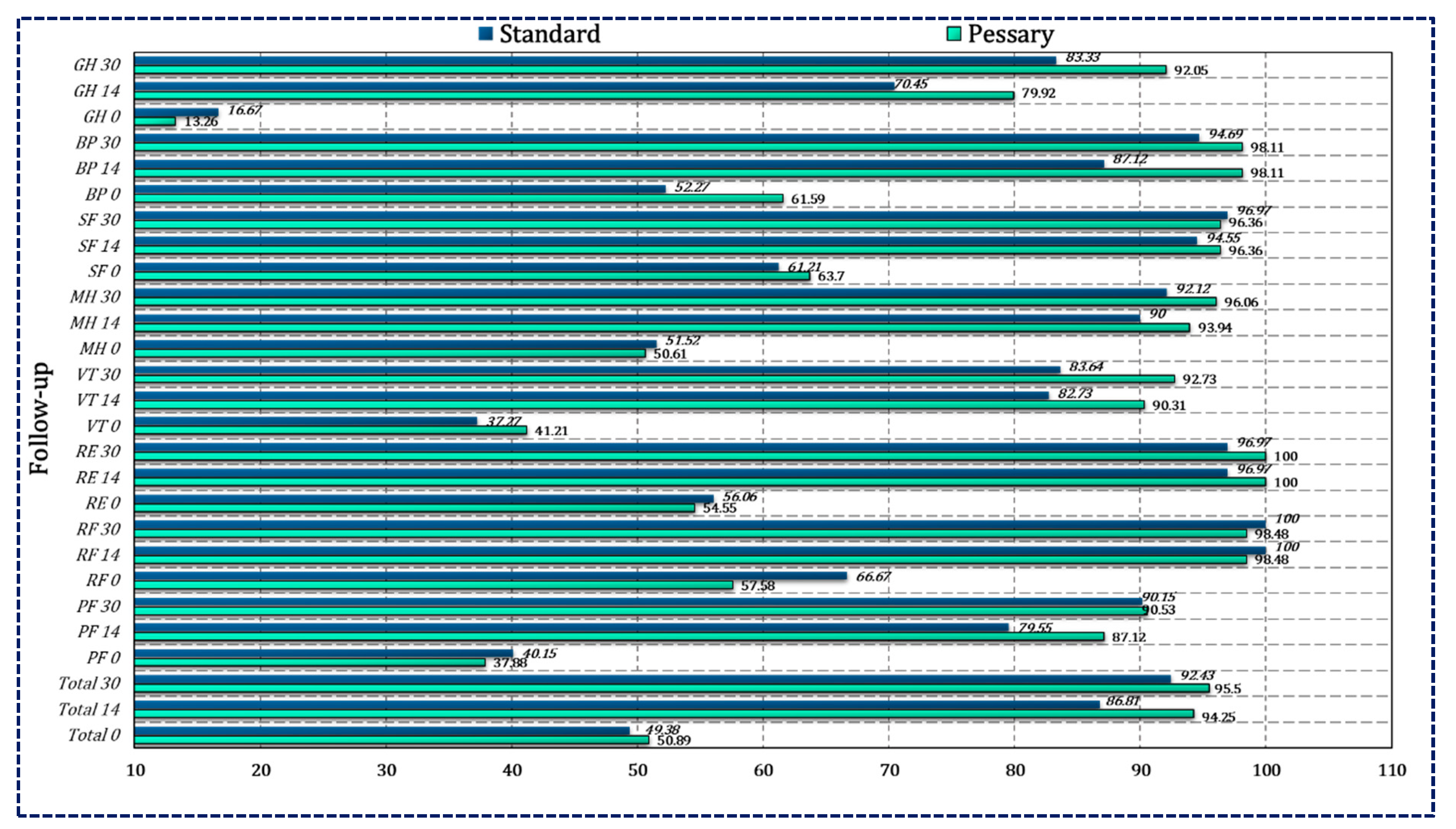
3.3.2. Heath-Related QoL Assessed by SF-12 Questionnaire
3.4. Haematological and Biochemical Markers for Safety Parameters
3.5. Classification of the Pessary and Standard Groups using Machine Learning Techniques
4. Discussion
4.1. Major Findings
4.2. Outcome Parameters
4.3. Overall Interpretation
4.4. Antimicrobial Activity of Bioactive Molecules of Linseeds, Psyllium, and Honey
4.5. Inflammatory Process in PID and Anti-Inflammatory and Antioxidant Activities of Linseeds, Psyllium, and Honey
4.6. Haematological and Biochemical Markers for Safety Parameters
4.7. Hepatoprotective and Nephroprotective Active of Psyllium and Linseeds
4.8. Strength, Limitations and Future Recommendations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Das, B.B.; Ronda, J.; Trent, M. Pelvic Inflammatory Disease: Improving Awareness, Prevention, and Treatment. Infect. Drug Resist. 2016, 9, 191–197. [Google Scholar] [CrossRef] [PubMed]
- Sultana, A.; Mehdi, S.; Rahman, K.; Fazmiya, M.J.A.; Heyat, M.B.B.; Akhtar, F.; Baig, A.A. Recent Advancements of Pelvic Inflammatory Disease: A Review on Evidence-Based Medicine. In Computational Intelligence in Healthcare Applications; Elsevier: Amsterdam, The Netherlands, 2022; pp. 101–120. ISBN 9780323990318. [Google Scholar]
- Dhasmana, D.; Hathorn, E.; McGrath, R.; Tariq, A.; Ross, J.D.C. The Effectiveness of Nonsteroidal Anti-Inflammatory Agents in the Treatment of Pelvic Inflammatory Disease: A Systematic Review. Syst. Rev. 2014, 3, 79. [Google Scholar] [CrossRef] [PubMed]
- Judlin, P.; Liao, Q.; Liu, Z.; Reimnitz, P.; Hampel, B.; Arvis, P. Efficacy and Safety of Moxifloxacin in Uncomplicated Pelvic Inflammatory Disease: The MONALISA Study. BJOG Int. J. Obstet. Gynaecol. 2010, 117, 1475–1484. [Google Scholar] [CrossRef]
- Kotecha, P.V.; Patel, S.V.; Baxi, R.K.; Shah, S.; Mehta, K.G.; Diwanji, M. Treatment Seeking Pathway of Pid (Pelvic Inflammatory Disease) Patients Attending Government Hospital Vadodara, India. Natl. J. Community Med. 2011, 2, 186–190. [Google Scholar]
- Dayal, S.; Singh, A.; Chaturvedi, V.; Krishna, M.; Gupta, V. Pattern of Pelvic Inflammatory Disease in Women Who Attended the Tertiary Care Hospital among the Rural Population of North India. Muller J. Med. Sci. Res. 2016, 7, 100–104. [Google Scholar] [CrossRef]
- Khan, A. Iksir-i-A‘Zame; Idarae Kitabus Shifa: New Delhi, India, 2011. [Google Scholar]
- Savaris, R.F.; Fuhrich, D.G.; Maissiat, J.; Duarte, R.V.; Ross, J. Antibiotic Therapy for Pelvic Inflammatory Disease. Cochrane Database Syst. Rev. 2020, 2020, CD010285. [Google Scholar] [CrossRef] [PubMed]
- Vishwesh, B.N.; Bhat, S.K. A Clinical Study to Evaluate the Role of Shivagutika in Pelvic Inflammatory Disease. J. Ayurveda Holist. Med. 2014, 2, 27–32. [Google Scholar]
- Bodhankar, M.; Pachori, R.R.; Kulkarni, N.S. Medicinal Plants as an Alternative for Treating Pelvic Inflammatory Disease. Int. J. Biochem. Mol. Biol. 2015, 3, 23–32. [Google Scholar]
- Kabir al-Din, M. Makhzan Al-Mufradat; Idarae Kitabus Shifa: New Delhi, India, 2007. [Google Scholar]
- Arzani, M.A. Qarabadeen Qadri; I’jaz Publishing House: New Delhi, India, 2009. [Google Scholar]
- Psyllium. In Standardisation of Single Drugs of Unani Medicine. Part-II, 1st ed.; Central Council for Research in Unani Medicine (CCRUM): New Delhi, India, 1992.
- Khare, C.P. Indian Medicinal Plants: An Illustrated Dictionary (Google EBook); Springer: Berlin/Heidelberg, Germany, 2007; 900p. [Google Scholar]
- Prajapati, N.D. Agro’s Dictionary of Medicinal Plants; Agrobios: Jodhpur, India, 2003. [Google Scholar]
- Deokar, G.; Kshirsagar, S.; Deore, P.; Kakulte, H. Pharmaceutical Benefits of Plantago ovate (Isabgol Seed): A Review. Pharm. Biol. Eval. 2016, 3, 32–41. [Google Scholar]
- Bagheri, S.M.; Zare-Mohazabieh, F.; Momeni-Asl, H.; Yadegari, M.; Mirjalili, A.; Anvari, M. Antiulcer and Hepatoprotective Effects of Aqueous Extract of Plantago ovata Seed on Indomethacin-Ulcerated Rats. Biomed. J. 2018, 41, 41–45. [Google Scholar] [CrossRef] [PubMed]
- Motamedi, H.; Darabpour, E.; Gholipour, M.; Seyyed Nejad, S.M. Antibacterial Effect of Ethanolic and Methanolic Extracts of Plantago ovata and Oliveria decumbens Endemic in Iran against Some Pathogenic Bacteria. Int. J. Pharmacol. 2010, 6, 117–122. [Google Scholar] [CrossRef]
- Bokaeian, M.; Fakheri, B.A.; Mohasseli, T.; Saeidi, S. Antibacterial Activity of Silver Nanoparticles Produced by Plantago ovata Seed Extract against Antibiotic Resistant Staphylococcus aureus. Int. J. Infect. 2015, 2, 176–178. [Google Scholar] [CrossRef]
- Sagar, S.; Goudar, G.; Sreedhar, M.; Panghal, A.; Sharma, P. Characterization of Nutritional Content and in Vitro—Antioxidant Properties of Plantago ovata Seeds. Int. J. Food Nutr. Sci. 2020, 9, 27. [Google Scholar] [CrossRef]
- Khedher, A.; Dhibi, S.; Bouzenna, H.; Akermi, S.; El Feki, A.; Teles, P.H.V.; Almeida, J.R.G.S.; Hfaiedh, N. Antiulcerogenic and Antioxidant Activities of Plantago ovata Ethanolic Extract in Rats. Brazilian J. Biol. 2022, 84, e255120. [Google Scholar] [CrossRef] [PubMed]
- Al-Jumaily, E.F.; AL-Azawi, A.H. Antioxidant and Hepatoprotective Activity of Purelignan from Flaxseed (Linum usitatissimum L.) Onacetaminophen Induced Toxicity in Male Rabbit. Int. J. Res. Stud. Biosci. 2015, 3, 8–16. [Google Scholar]
- Ravn, H.; Brimer, L. Structure and Antibacterial Activity of Plantamajoside, a Caffeic Acid Sugar Ester from Plantago Major Subs Major. Phytochemistry 1988, 27, 3433–3437. [Google Scholar] [CrossRef]
- Linseeds. In Standardisation of Single Drugs of Unani Medicine. Part-II.; Central Council for Research in Unani Medicine: Delhi, India, 1992; pp. 276–281.
- Bernacchia, R.; Preti, R.; Vinci, G. Chemical Composition and Health Benefits of Flaxseed. Austin J. Nutr. Food Sci. 2014, 2, 1–9. [Google Scholar]
- Heena Umer, K.; Zeenat, F.; Ahmad, W.; Ahmad Hakim Syed Ziaul Hasan Govt, I.; Vakil Khan, A.; Fahmeeda Zeenat, C.; Ahmad, I. Therapeutics, Phytochemistry and Pharmacology of Alsi (Linum usitatissimum Linn.): An Important Unani Drug. J. Pharmacogn. Phytochem. 2017, 6, 377–383. [Google Scholar]
- Mohamed El-Feky, F.; El-Sherbiny, I.M.; El-Fedawy, M.G.; Abdel-Mogib, M. Phytochemical Studies on Linum usitatissimum Seeds and the Nanoformulation of the Bioactive Butanol Extract. Int. J. Sci. Eng. Appl. 2016, 5, 76–91. [Google Scholar] [CrossRef]
- Azamat Kizi, K.S. Antibacterial Activity of Linum usitatissimum L. Seeds and Active Compound Detection. Eur. Int. J. Multidiscip. Res. Manag. Stud. 2022, 2, 263–266. [Google Scholar] [CrossRef]
- Tavarini, S.; Castagna, A.; Conte, G.; Foschi, L.; Sanmartin, C.; Incrocci, L.; Ranieri, A.; Serra, A.; Angelini, L.G. Evaluation of Chemical Composition of Two Linseed Varieties as Sources of Health-Beneficial Substances. Molecules 2019, 24, 3729. [Google Scholar] [CrossRef] [PubMed]
- Shim, Y.Y.; Gui, B.; Arnison, P.G.; Wang, Y.; Reaney, M.J.T. Flaxseed (Linum usitatissimum L.) Bioactive Compounds and Peptide Nomenclature: Areview. Trends Food Sci. Technol. 2014, 38, 5–20. [Google Scholar] [CrossRef]
- Goyal, A.; Sharma, V.; Upadhyay, N.; Gill, S.; Sihag, M. Flax and Flaxseed Oil: An Ancient Medicine & Modern Functional Food. J. Food Sci. Technol. 2014, 51, 1633–1653. [Google Scholar] [CrossRef] [PubMed]
- Zuk, M.; Dorotkiewicz-Jach, A.; Drulis-Kawa, Z.; Arendt, M.; Kulma, A.; Szopa, J. Bactericidal Activities of GM Flax Seedcake Extract on Pathogenic Bacteria Clinical Strains. BMC Biotechnol. 2014, 14, 70. [Google Scholar] [CrossRef] [PubMed]
- Al-bayati, F.A. Antibacterial Activity of Linum usitatissimum L. Seeds and Active Compound Detection. Rafidain J. Sci. 2007, 18, 27–36. [Google Scholar]
- Son, H.J.; Song, K. Bin Antimicrobial Activity of Flaxseed Meal Extract against Escherichia coli O157:H7 and Staphylococcus aureus Inoculated on Red Mustard. J. Microbiol. Biotechnol. 2017, 27, 67–71. [Google Scholar] [CrossRef]
- Hassan, M.; Tehrani, H.; Batal, R.; Kamalinejad, M.; Mahbubi, A. Extraction and Purification of Flaxseed Proteins and Studying Their Antibacterial Activities. J. Plant Sci. 2014, 2, 70. [Google Scholar] [CrossRef]
- Kaithwas, G.; Mukherjee, A.; Chaurasia, A.K.; Majumdar, D.K. Antiinflammatory, Analgesic and Antipyretic Activities of Linum usitatissimum L. (Flaxseed/Linseed) Fixed Oil. Indian J. Exp. Biol. 2011, 49, 932–938. [Google Scholar]
- Cornara, L.; Biagi, M.; Xiao, J.; Burlando, B. Therapeutic Properties of Bioactive Compounds from Different Honeybee Products. Front. Pharmacol. 2017, 8, 412. [Google Scholar] [CrossRef] [Green Version]
- Combarros-Fuertes, P.; Estevinho, L.M.; Dias, L.G.; Castro, J.M.; Tomás-Barberán, F.A.; Tornadijo, M.E.; Fresno-Baro, J.M. Bioactive Components and Antioxidant and Antibacterial Activities of Different Varieties of Honey: A Screening Prior to Clinical Application. J. Agric. Food Chem. 2019, 67, 688–698. [Google Scholar] [CrossRef]
- Linum usitatissimum L. Taxonomic Serial No.: 29226. Integrated Taxonomic Information System (ITIS)—Report. Available online: https://www.itis.gov/servlet/SingleRpt/SingleRpt?search_topic=TSN&search_value=29226#null (accessed on 15 January 2023).
- Plantago ovata Forssk. Taxonomic Serial No.: 504438. Integrated Taxonomic Information System (ITIS)—Report. Available online: https://www.itis.gov/servlet/SingleRpt/SingleRpt?search_topic=TSN&search_value=504438#null (accessed on 15 January 2023).
- Greenberg, D. A Quantitative and Qualitative Evaluation of Official and Unofficial Species of Psyllium Seeds and Their Mucilages. J. Am. Pharm. Assoc. 1948, 37, 139–145. [Google Scholar] [CrossRef] [PubMed]
- El Abdali, Y.; Allali, A.; Agour, A.; Mikou, K.; Lahkimi, A.; Eloutassi, N.; Bouia, A. Phytochemical Screening, and in Vitro Antiradical and Immunostimulant Potential of Linum usitatissimum L. Pharmacologyonline 2021, 3, 602–614. [Google Scholar]
- Vijayakumar, K.T.; Neethu, T.; Bhat, N.S.; Nayimabanu, T.; Varsharani, H. Physico-Chemical Property of Different Floral Honeys of Bangalore Region, Karnataka. J. Entomol. Zool. Stud. 2020, 8, 846–854. [Google Scholar]
- Fazmiya, M.J.A.; Sultana, A.; Rahman, K.; Heyat, M.D.B.; Sumbul; Akhtar, F.; Khan, S.; Appiah, S.C.Y. Current Insights on Bioactive Molecules, Antioxidant, Anti-Inflammatory, and Other Pharmacological Activities of Cinnamomum camphora Linn. Oxid. Med. Cell. Longev. 2022, 2022, 9354555. [Google Scholar] [CrossRef] [PubMed]
- Samarghandian, S.; Farkhondeh, T.; Samini, F. Honey and Health: A Review of Recent Clinical Research. Pharmacogn. Res. 2017, 9, 121–127. [Google Scholar] [CrossRef]
- Viuda Martos, M.; Ruiz Navajas, Y.; Fernández López, J.; Pérez-Alvarez, J.A. Functional Properties of Honey, Propolis, and Royal Jelly. J. Food Sci. 2008, 73, R117–R124. [Google Scholar] [CrossRef]
- Parween, A.; Tabassum, K.; Begum, W. Effect of Arq Mako and Sharbat Kasni in Waram Al Rahim (Pelvic Inflammatory Disease): An Observational Clinical Trial. Int. J. Adv. Res. Dev. 2017, 2, 7–13. [Google Scholar]
- Sayed, A.; Shameem, I.; Mubeen, U.; Qabalat, I.; Niswan, A.; Medicine, U.; Qabalat, I.; Niswan, A.; Medicine, U.; Qabalat, I.; et al. Effect of Arq brinjasif in Mild Pelvic Inflammatory Disease—A Randomised Controlled Trial. Int. J. Med. Res. 2016, 1, 91–96. [Google Scholar]
- Teelhawod, B.N.; Akhtar, F.; Heyat, M.B.B.; Tripathi, P.; Mehrotra, R.; Asfaw, A.B.; Al Shorman, O.; Masadeh, M. Machine Learning in E-Health: A Comprehensive Survey of Anxiety. In Proceedings of the 2021 International Conference on Data Analytics for Business and Industry, ICDABI 2021, Sakheer, Bahrain, 25–26 October 2021; pp. 167–172. [Google Scholar]
- Sultana, A.; Begum, W.; Saeedi, R.; Rahman, K.; Heyat, M.B.B.; Akhtar, F.; Son, N.Y.; Ullah, H. Experimental and Computational Approaches for the Classification and Correlation of Temperament (Mizaj) and Uterine Dystemperament (Su’-I-Mizaj Al-Rahim) in Abnormal Vaginal Discharge (Sayalan Al-Rahim) Based on Clinical Analysis Using Support Vector Mach. Complexity 2022, 2022, 1–16. [Google Scholar] [CrossRef]
- Iqbal, M.S.; Abbasi, R.; Bin Heyat, M.B.; Akhtar, F.; Abdelgeliel, A.S.; Albogami, S.; Fayad, E.; Iqbal, M.A. Recognition of MRNA N4 Acetylcytidine (Ac4C) by Using Non-Deep vs. Deep Learning. Appl. Sci. 2022, 12, 1344. [Google Scholar] [CrossRef]
- Pal, R.; Adhikari, D.; Heyat, M.B.B.; Guragai, B.; Lipari, V.; Brito Ballester, J.; De la Torre Díez, I.; Abbas, Z.; Lai, D. A Novel Smart Belt for Anxiety Detection, Classification, and Reduction Using IIoMT on Students’ Cardiac Signal and MSY. Bioengineering 2022, 9, 793. [Google Scholar] [CrossRef]
- Bin Heyat, M.B.; Akhtar, F.; Sultana, A.; Tumrani, S.; Teelhawod, B.N.; Abbasi, R.; Kamal, M.A.; Muaad, A.Y.; Lai, D.; Wu, K. Role of Oxidative Stress and Inflammation in Insomnia Sleep Disorder and Cardiovascular Diseases: Herbal Antioxidants and Anti-Inflammatory Coupled with Insomnia Detection Using Machine Learning. Curr. Pharm. Des. 2022, 28, 3618–3636. [Google Scholar] [CrossRef] [PubMed]
- Akhtar, F.; Bin Heyat, M.B.; Li, J.P.; Patel, P.K.; Rishipal; Guragai, B. Role of Machine Learning in Human Stress: A Review. In Proceedings of the 2020 17th International Computer Conference on Wavelet Active Media Technology and Information Processing, ICCWAMTIP 2020, Chengdu, China, 18–20 December 2020; pp. 170–174. [Google Scholar]
- Bin Heyat, M.B.; Lai, D.; Khan, F.I.; Zhang, Y. Sleep Bruxism Detection Using Decision Tree Method by the Combination of C4-P4 and C4-A1 Channels of Scalp EEG. IEEE Access 2019, 7, 102542–102553. [Google Scholar] [CrossRef]
- Tripathi, P.; Ansari, M.A.; Gandhi, T.K.; Mehrotra, R.; Bin Heyat, M.B.; Akhtar, F.; Ukwuoma, C.C.; Muaad, A.Y.; Kadah, Y.M.; Al-Antari, M.A.; et al. Ensemble Computational Intelligent for Insomnia Sleep Stage Detection via the Sleep ECG Signal. IEEE Access 2022, 10, 108710–108721. [Google Scholar] [CrossRef]
- Lai, D.; Bin Heyat, M.B.; Khan, F.I.; Zhang, Y. Prognosis of Sleep Bruxism Using Power Spectral Density Approach Applied on EEG Signal of Both EMG1-EMG2 and ECG1-ECG2 Channels. IEEE Access 2019, 7, 82553–82562. [Google Scholar] [CrossRef]
- Bin Heyat, M.B.; Akhtar, F.; Abbas, S.J.; Al-Sarem, M.; Alqarafi, A.; Stalin, A.; Abbasi, R.; Muaad, A.Y.; Lai, D.; Wu, K. Wearable Flexible Electronics Based Cardiac Electrode for Researcher Mental Stress Detection System Using Machine Learning Models on Single Lead Electrocardiogram Signal. Biosensors 2022, 12, 427. [Google Scholar] [CrossRef]
- Chola, C.; Bin Heyat, M.B.; Akhtar, F.; Al Shorman, O.; Bibal Benifa, J.V.; Muaad, A.Y.M.; Masadeh, M.; Alkahatni, F. IoT Based Intelligent Computer-Aided Diagnosis and Decision Making System for Health Care. In Proceedings of the 2021 International Conference on Information Technology, ICIT 2021—Proceedings, Amman, Jordan, 14–15 July 2021; pp. 184–189. [Google Scholar]
- Sultana, A.; Heyat, M.B.B.; Rahman, K.; Kunnavil, R.; Fazmiya, M.J.A.; Akhtar, F.; Sumbul; Vidal Mazón, J.L.; Rodríguez, C.L.; De La Torre Díez, I. A Systematic Review and Meta-Analysis of Premenstrual Syndrome with Special Emphasis on Herbal Medicine and Nutritional Supplements. Pharmaceuticals 2022, 15, 1371. [Google Scholar] [CrossRef] [PubMed]
- Moghtadaei, P.; Sardari, F.; Esmaeilian, S. Comparison of Ceftriaxone Plus Weekly Azithromycin or Daily Ofloxacin for Outpatient Treatment of Pelvic Inflammatory Disease: A Randomized Clinical Trial. J. Fam. Reprod. Health 2008, 2, 87–93. [Google Scholar]
- Bhat, T.A.; Begum, W. Efficacy of Tamarindus indicus, Melia azadirach and Santalum album in syndromic management of abnormal vaginal discharge: A single-blind randomised controlled trial. J. Complement. Integr. Med. 2017, 15, 19. [Google Scholar] [CrossRef] [PubMed]
- Thomas, L. Clinical Laboratory Diagnostics, 1 st ed.; TH-Books Sgesellschaft: Frankfurt, Germany, 1998. [Google Scholar]
- Tietz, N.W.; Rinker, A.D.; Shaw, L.M. IFCC Reference Procedure for Measurement of Catalytic Concentration of Enzymes at 37 °C. Part 9. Reference Procedure for Measurement of Catalytic Concentration of Alkaline Phosphatase. Clin. Chem. Lab. Med. 2011, 49, 1439–1446. [Google Scholar]
- Burtis, C.A.; Ashwood, E.R.; Bruns, D.E. Tietz Textbook of Clinical Chemistry and Molecular Diagnostics, 4th ed.; Saunder’s Co.: Bloomington, MN, USA, 2005. [Google Scholar]
- Sharma, J.B.; Chanana, C.; Kumar, S.; Roy, K.; Malhotra, N. Comparison of Ofloxacin & Ornidazole with Probiotic versus Doxycycline & Metronidazole for the Outpatient Treatment of Pelvic Inflammatory Disease. JK Sci. 2007, 9, 66–69. [Google Scholar]
- Anjum, A.; Sultana, A. A Randomized Comparative Study of Herbal Decoction of Cassia fistula Linn Pod’s Pericarp and Myristica fragrans Houtt Arils vs. Mefenamic Acid in Spasmodic Dysmenorrhoea. J. Complement. Integr. Med. 2019, 16, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Lam, W.Y.; Fresco, P. Medication Adherence Measures: An Overview. Biomed. Res. Int. 2015, 2015, 217047. [Google Scholar] [CrossRef] [PubMed]
- Saeedi, R.; Sultana, A.; Rahman, K.; Belal Bin Heyat, M.; Kamal, M.A.; Ishawu, M. Efficacy of Acacia nilotica Linn. Pod’s Sitz Bath plus Vaginal Pessary in Syndromic Management of Abnormal Vaginal Discharge: A Randomized Controlled Trial. Evid.-Based Complement. Altern. Med. 2022, 2022, 5769555. [Google Scholar] [CrossRef]
- Said, R.R.; Heyat, M.B.B.; Song, K.; Tian, C.; Wu, Z. A Systematic Review of Virtual Reality and Robot Therapy as Recent Rehabilitation Technologies Using EEG-Brain–Computer Interface Based on Movement-Related Cortical Potentials. Biosensors 2022, 12, 1134. [Google Scholar] [CrossRef]
- Nawabi, A.K.; Sheng, J.; Abbasi, R.; Iqbal, M.S.; Heyat, M.B.B.; Akhtar, F.; Wu, K.; Twumasi, B.A. Segmentation of Drug-Treated Cell Image and Mitochondrial-Oxidative Stress Using Deep Convolutional Neural Network. Oxid. Med. Cell. Longev. 2022, 2022, 5641727. [Google Scholar] [CrossRef]
- Tripathi, P.; Ansari, M.; Akhtar, F.; Heyat, M.B.B.; Mehrotra, R.; Yatoo, A.H.; Teelhawod, B.N.; Asfaw, A.B.; Baig, A.A. Automatic Epileptic Seizure Detection Based on the Discrete Wavelet Transform Approach Using an Artificial Neural Network Classifier on the Scalp Electroencephalogram Signal. Comput. Intell. Healthc. Appl. 2022, 10, 157–173. [Google Scholar] [CrossRef]
- Ullah, H.; Heyat, M.B.B.; Akhtar, F.; Muaad, A.Y.; Ukwuoma, C.C.; Bilal, M.; Miraz, M.H.; Bhuiyan, M.A.S.; Wu, K.; Damaševičius, R.; et al. An Automatic Premature Ventricular Contraction Recognition System Based on Imbalanced Dataset and Pre-Trained Residual Network Using Transfer Learning on ECG Signal. Diagnostics 2022, 13, 87. [Google Scholar] [CrossRef]
- Ullah, H.; Bin Heyat, M.B.; Akhtar, F.; Sumbul; Muaad, A.Y.; Islam, M.S.; Abbas, Z.; Pan, T.; Gao, M.; Lai, D. An End-to-End Cardiac Arrhythmia Recognition Method with an Effective DenseNet Model on Imbalanced Datasets Using ECG Signal. Comput. Intell. Neurosci. 2022, 2022, 9475162. [Google Scholar] [CrossRef] [PubMed]
- Sultana, A.; Baig, K.; Rahman, K.; Mehdi, S.; Heyat, M.B.B.; Akhtar, F.; Baig, A.A. Contemporary Overview of Bacterial Vaginosis in Conventional and Complementary and Alternative Medicine. In Computational Intelligence in Healthcare Applications; Elsevier: Amsterdam, The Netherlands, 2022; pp. 33–53. ISBN 9780323990318. [Google Scholar]
- Saeedi, R.; Deoband, J.T.; Khan, M.A.; Farzana, M.U.Z.N. A Conceptual Literary Exploration of Sayalan Al-Rahim (Abnormal Vaginal Discharge) in Unani Medicine. SLJIM 2020, 5, 414–423. [Google Scholar]
- Qhuddsia, Q.N.; Sultana, A.; Jahan, I. Efficacy of Unani Formulations in Chronic Endocervicitis: A Randomized Comparative Study. Int. J. Pharm. Pharm. Sci. 2015, 7, 101–104. [Google Scholar]
- Moylan, S.; Berk, M.; Dean, O.M.; Samuni, Y.; Williams, L.J.; O’Neil, A.; Hayley, A.C.; Pasco, J.A.; Anderson, G.; Jacka, F.N.; et al. Oxidative & Nitrosative Stress in Depression: Why so Much Stress? Neurosci. Biobehav. Rev. 2014, 45, 46–62. [Google Scholar] [CrossRef] [PubMed]
- Baig, K.; Sultana, A.; Rahman, K. A Randomized Comparative Study of Kakrasingi (Pistacia integerrima J. L. Stewart Ex Brandis) and Metronidazole in Bacterial Vaginosis. J. Herb. Med. 2022, 36, 100609. [Google Scholar] [CrossRef]
- Haggerty, C. Lower Quality of Life among Women with Chronic Pelvic Pain after Pelvic Inflammatory Disease. Obstet. Gynecol. 2003, 102, 934–939. [Google Scholar] [CrossRef]
- Li, X.H.; Liu, Y.R.; Jiang, D.H.; Tang, Z.S.; Qian, D.W.; Song, Z.X.; Chen, L.; Shi, X.B.; Yang, N.J.; Yan, Y.F.; et al. Research on the Mechanism of Chinese Herbal Medicine Radix Paeoniae Rubra in Improving Chronic Pelvic Inflammation Disease by Regulating PTGS2 in the Arachidonic Acid Pathway. Biomed. Pharmacother. 2020, 129, 110052. [Google Scholar] [CrossRef]
- Rafieian-kopaei, M.; Shakiba, A.; Sedighi, M.; Bahmani, M. The Analgesic and Anti-Inflammatory Activity of Linum usitatissimum in Balb/c Mice. J. Evid.-Based Complement. Altern. Med. 2017, 22, 892–896. [Google Scholar] [CrossRef] [PubMed]
- Reddy, P.R.T.; Vandana, K.; Prakash, S. Antibacterial and Anti-Inflammatory Properties of Plantago ovata Forssk. Leaves and Seeds against Periodontal Pathogens: An in Vitro Study. AYU Int. Q. J. Res. Ayurveda 2018, 39, 226–229. [Google Scholar] [CrossRef] [PubMed]
- Nowak, D.A.; Snyder, D.C.; Brown, A.J.; Demark-Wahnefried, W. The Effect of Flaxseed Supplementation on Hormonal Levels Associated with Polycystic Ovarian Syndrome: A Case Study. Curr. Top. Nutraceutical Res. 2007, 5, 177–181. [Google Scholar]
- Fons, F.; Gargadennec, A.; Rapior, S. Culture of Plantago Species as Bioactive Components Resources: A 20-Year Review and Recent Applications. Acta Bot. Gall. 2008, 155, 277–300. [Google Scholar] [CrossRef]
- Haroon, M.; Iqbal, M.J.; Hassan, W.; Ali, S.; Ahmed, H.; Hassan, S.U. Evaluation of Methanolic Crude Extract of Linum usitatissimum for the Removal of Biofilm in Diabetic Foot Isolates. Brazilian J. Biol. 2023, 83, 3–4. [Google Scholar] [CrossRef] [PubMed]
- Patton, T.; Barrett, J.; Brennan, J.; Moran, N. Use of a Spectrophotometric Bioassay for Determination of Microbial Sensitivity to Manuka Honey. J. Microbiol. Methods 2006, 64, 84–95. [Google Scholar] [CrossRef] [PubMed]
- Molan, P.C. Potential of Honey in the Treatment of Wounds and Burns. Am. J. Clin. Dermatol. 2001, 2, 13–19. [Google Scholar] [CrossRef] [PubMed]
- Omoigui, S. The biochemical origin of pain: The origin of all pain is inflammation and the inflammatory response. Part 2 of 3—Inflammatory profile of pain syndromes. Med. Hypotheses 2009, 69, 1169–1178. [Google Scholar] [CrossRef] [PubMed]
- Xu, S.X.; Gray-Owen, S.D. Gonococcal Pelvic Inflammatory Disease: Placing Mechanistic Insights into the Context of Clinical and Epidemiological Observations. J. Infect. Dis. 2021, 224, S56–S63. [Google Scholar] [CrossRef]
- Cheraghi, J.; Valadi, A. Effect of Antinociceptive and Anti-Inflammatory Component of Limonene. Iran J. Med. Aromaterapic Plants 2010, 6, 415–422. [Google Scholar]
- Morsi, E.A.; Ahmed, H.O.; Abdel-Hady, H.; El-Sayed, M.; Shemis, M.A. GC-Analysis, and Antioxidant, Anti-Inflammatory, and Anticancer Activities of Some Extracts and Fractions of Linum usitatissimum. Curr. Bioact. Compd. 2020, 16, 1306–1318. [Google Scholar] [CrossRef]
- Mechchate, H.; Es-Safi, I.; Conte, R.; Hano, C.; Amaghnouje, A.; Jawhari, F.Z.; Radouane, N.; Bencheikh, N.; Grafov, A.; Bousta, D. In Vivo and in Vitro Antidiabetic and Anti-Inflammatory Properties of Flax (Linum usitatissimum L.) Seed Polyphenols. Nutrients 2021, 13, 2759. [Google Scholar] [CrossRef]
- Al-jumaily, E.F.; Al-azawi, A.H. Hepatoprotective Activity Of Lignan Compound From Flaxseed (Linum usitatissimum L.) against Acetaminophen-Induced Hepatotoxicity In Rabbits. World J. Pharm. Pharm. Sci. 2013, 3, 56–72. [Google Scholar]
- Chaouche, T.M.; Haddouchi, F.; Ksouri, R.; Atik-Bekkara, F. Evaluation of Antioxidant Activity of Hydromethanolic Extracts of Some Medicinal Species from South Algeria. J. Chin. Med. Assoc. 2014, 77, 302–307. [Google Scholar] [CrossRef]
- Pareek, S.; Paliwal, R.; Mukherjee, S. Effect of Juice Extraction Methods and Processing Temperature-Time on Juice Quality of Nagpur Mandarin (Citrus reticulata Blanco) during Storage. J. Food Sci. Technol. 2011, 48, 197–203. [Google Scholar] [CrossRef]
- Nakhlawy, F.S. Inheritance of Oil Content, Unsaturated Fatty Acid Composition and Iodine Number of Oil in Flax. Menofiya J. Agric. Res. Egypt 1996, 20, 483–492. [Google Scholar]
- Ghannadi, A.R.; Ghassemi-Dehkordi, N. Pharmacognostical Investigations on Sambucus ebulus L. and Sambucus nigra L. DARU 1997, 7, 55–65. [Google Scholar]
- Samani, B.H.; Khoshtaghaza, M.H.; Lorigooini, Z.; Minaei, S.; Zareiforoush, H. Analysis of the Combinative Effect of Ultrasound and Microwave Power on Saccharomyces Cerevisiae in Orange Juice Processing. Innov. Food Sci. Emerg. Technol. 2015, 32, 110–115. [Google Scholar] [CrossRef]
- Patel, M.K.; Mishra, A.; Jha, B. Non-Targeted Metabolite Profiling and Scavenging Activity Unveil the Nutraceutical Potential of Psyllium (Plantago ovata Forsk). Front. Plant Sci. 2016, 7, 431. [Google Scholar] [CrossRef]
- Koo, K.L.K.; Ammit, A.J.; Tran, V.H.; Duke, C.C.; Roufogalis, B.D. Gingerols and Related Analogues Inhibit Arachidonic Acid-Induced Human Platelet Serotonin Release and Aggregation. Thromb. Res. 2001, 103, 387–397. [Google Scholar] [CrossRef] [PubMed]
- Lantz, R.C.; Chen, G.J.; Sarihan, M.; Sólyom, A.M.; Jolad, S.D.; Timmermann, B.N. The Effect of Extracts from Ginger Rhizome on Inflammatory Mediator Production. Phytomedicine 2007, 14, 123–128. [Google Scholar] [CrossRef]
- Jandali, R.; Agha, M.I.H. Lipoxygenase Inhibitory Activity of Some Extracts Prepared from Flaxseed (Linum usitatissimumv L.). Curr. Bioact. Compd. 2021, 18, e091221197172. [Google Scholar] [CrossRef]
- Abouzied, M.M.; Mahmoud, S.M.; Wahid, A.; Ahmed, A.E.; Okasha, A.M.; Soliman, H.A.; Thagfan, S.S.A.; Attia, E.Z. A Study of the Hepatoprotective Effect of Plantago psyllium L. Seed Extract against Carbon Tetrachloride Induced Hepatic Injury in Rats. J. Appl. Biomed. 2020, 18, 80–86. [Google Scholar] [CrossRef]
- Del Carmen Recio, M.; Giner, R.M.; Manez, S.; Rios, J.L. Structural Considerations on the Iridoids as Anti-Inflammatory Agents. Planta Med. 1994, 60, 232–234. [Google Scholar] [CrossRef]
- Murai, M.; Tamayama, Y.; Nishibe, S. Phenylethanoids in the Herb of Plantago Lanceolata and Inhibitory Effect on Arachidonic Acid-Induced Mouse Ear Edema. Planta Med. 1995, 61, 479–480. [Google Scholar] [CrossRef]
- Nishibe, S.; Sasahara, M.; Jiao, Y.; Yuan, C.L.; Tanaka, T. Phenylethanoid Glycosides from Plantago Depressa. Phytochemistry 1993, 32, 975–977. [Google Scholar] [CrossRef]
- De Jesus, N.Z.T.; de Souza Falcão, H.; Gomes, I.F.; de Almeida Leite, T.J.; de Morais Lima, G.R.; Barbosa-Filho, J.M.; Tavares, J.F.; da Silva, M.S.; de Athayde-Filho, P.F.; Batista, L.M. Tannins, Peptic Ulcers and Related Mechanisms. Int. J. Mol. Sci. 2012, 13, 3203–3228. [Google Scholar] [CrossRef] [PubMed]
- Al Waili, N.S.; Boni, N. Natural Honey Lowers Plasma Prostaglandin Concentrations in Normal Individuals. J. Med. Food 2003, 6, 129–133. [Google Scholar] [CrossRef] [PubMed]
- Ghule, A.E.; Jadhav, S.S.; Bodhankar, S.L. Renoprotective Effect of Linum Usitatissimum Seeds through Haemodynamic Changes and Conservation of Antioxidant Enzymes in Renal Ischaemia-Reperfusion Injury in Rats. Arab J. Urol. 2011, 9, 215–221. [Google Scholar] [CrossRef] [PubMed]
- Shakir, K.A.F.; Madhusudhan, B. Hypocholesterolemic and Hepatoprotective Effects of Flaxseed Chutney: Evidence from Animal Studies. Indian J. Clin. Biochem. 2007, 22, 117–121. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Taxonomy | Psyllium | Linseeds | Reference |
|---|---|---|---|
| Kingdom | Plantae | Plantae | [39,40] |
| Subkingdom | Viridiplantae | Viridiplantae | |
| Infrakingdom | Streptophyta | Streptophyta | |
| Superdivision | Embryophyta | Embryophyta | |
| Division | Tracheophyta | Tracheophyta | |
| Subdivision | Spermatophytina | Spermatophytina | |
| Class | Magnoliopsida | Magnoliopsida | |
| Superorder | Asteranae | Rosanae | |
| Order | Lamiales | Malpighiales | |
| Family | Plantaginaceae | Linaceae | |
| Genus | Plantago | Linum | |
| Species | Plantago ovata Forssk. | Linum usitatissimum L. |
| Parameters | Psyllium | Linseeds | Reference |
|---|---|---|---|
| Ash value (%) | |||
| Total ash | 3.47 | 6.84 | [13,24] |
| Acid insoluble ash | 0.90 | 3.76 | |
| Water soluble ash | 1.10 | 0.41 | |
| Successive extractive value (%) | |||
| Petroleum ether | 4.22 | 43.0 | |
| Chloroform | 1.40 | 1.1 | |
| Ethanol | 2.45 | 4.91 | |
| Water | - | 2.36 | |
| Moisture content (%) | 4.45 | 5.65 | |
| Mucilage | 22% | 4.46% | [41,42] |
| Total phenolics mgGAE/g | 286.8 ± 6.05 | 7.24 ± 0.14 | [21,42] |
| Total flavonoids | 101.83 ± 12.9 mgRE/g | 1.74 ± 0.57 mg QE/g | [21,42] |
| Total tannins | 39.33 ± 1.52 mgCE/g | 1.35 ± 0.03 | [21,42] |
| Parameters | Values | Reference |
|---|---|---|
| Refractive index at 20 °C | 1.485 | [43] |
| Ash (%) | 0.28 | |
| Moisture (%) | 20.83 | |
| Total Soluble Solids (°Brix) | 77.65 | |
| P fund (mm) | 103 | |
| Colour | Light Amber | |
| Specific gravity | 1.40 | |
| pH | 4.06 | |
| Electrical conductivity (dS/m) | 0.77 | |
| Total reducing sugar (%) | 69.36 | |
| Sucrose (%) | 2.94 | |
| Glucose | 33.77 | |
| Fructose | 35.59 | |
| Hydroxy Methyl Furfural | 27.30 |
| VAS for Lower Abdominal Pain | Pessary Group (n = 33) | Standard Group (n = 33) | p-Value |
|---|---|---|---|
| D0 | 3.45 ± 2.21 | 3.58 ± 2.65 | 0.841 |
| D7 | 1.85 ± 1.46 | 1.97 ± 1.78 | 0.763 |
| D14 | 0.67 ± 0.89 * | 0.82 ± 1.33 ** | 0.589 |
| D30 | 0.18 ± 0.46 * | 0.52 ± 1.09 ** | 0.112 |
| %Pain Reduction (PR) | 80.57% | 77.09% | |
| VAS for lower back ache | |||
| D0 | 2.48 ± 2.29 | 3.55 ± 2.69 | 0.090 |
| D7 | 1.42 ± 1.44 | 2.18 ± 1.98 | 0.080 |
| D14 | 0.64 ± 0.93 * | 1.12 ± 1.47 ** | 0.115 |
| D30 | 0.27 ± 0.63 * | 0.64 ± 1.08 ** | 0.100 |
| % Pain Reduction PR | 74.19% | 68.54% | |
| Modified McCormack Pain Scale (McPS) for pelvic tenderness | |||
| D0 | 3.82 ± 1.59 | 3.76 ± 1.50 | 0.874 |
| D7 | 2.52 ± 1.20 | 2.55 ± 1.00 | 0.912 |
| D14 | 0.94 ± 1.00 * | 1.21 ± 1.11 ** | 0.298 |
| D30 | 0.42 ± 0.66 * | 0.73 ± 1.01 ** | 0.154 |
| % Pain Reduction (PR) | 75.39% | 67.81% | |
| Abnormal Vaginal Discharge (AVD) | Pessary Group (n = 33) | Standard Group (n = 33) | p-Value | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Day 0 | 2.78 ± 0.41 | 2.72 ± 0.51 | 0.79 | ||||||
| Day 14 | 0.36 ± 0.54 | 0.60 ± 0.86 | 0.39 | ||||||
| p value | <0.0001 | <0.0001 | |||||||
| % AVD reduction | 87.05% | 77.94% | |||||||
| Associated symptoms | Present | Relieved | Present | Relieved | |||||
| Dyspareunia | |||||||||
| Day 0 | 21 (100) | 0 | 18 (100) | 0 | |||||
| Day 14 | 3 (14.28) | 18 (85.71) | 4 (22.22) | 14 (77.77) | 0.41 | ||||
| p value | <0.0001 | <0.0001 | |||||||
| Dysuria | |||||||||
| Day 0 | 10 (100) | 0 | 10 (100) | 0 (0) | |||||
| Day 14 | 0 (0) | 10 (100) | 2 (20) | 8 (80) | 0.23 | ||||
| Pruritus vulvae | 0 | ||||||||
| Day 0 | 23 (100) | 0 | 19 (100) | 0 | |||||
| Day 14 | 0 | 23 (100) | 3 (15.78) | 16 (84.21) | 0.08 | ||||
| AVD as per severity grading | |||||||||
| AVD Grading | 0 | 1 | 2 | 3 | 0 | 1 | 2 | 3 | -- |
| Day 0 | 0 | 0 | 7 (21.2) | 26 (78.8) | 0 | 1 (3) | 7 (21.2) | 25 (75.8) | - |
| Day 14 | 22 (66.7) | 10 (30.3) | 1 (3) | 0 * | 19 (57.6) | 10 (30.3) | 2 (6.1) | 2 (6.1) ** | - |
| Day 30 | 28 (84.8) | 5 (15.2) | 0 | 0 * | 25 (75.8) | 5 (15.2) | 2 (6.1) | 1 (3) ** | - |
| Domains SF-12 HRQoL | Period | Pessary Group (n = 33) | Standard Group (n = 33) | p-Value |
|---|---|---|---|---|
| Total score | Day 0 | 50.89 ± 23.38 | 49.38 ± 26.85 | 0.808 |
| Day 14 | 94.25 ± 5.80 a | 86.81 ± 13.14 b | 0.004 | |
| Day 30 | 95.50 ± 6.86 a | 92.43 ± 11.88 b | 0.203 | |
| Physical function (PF) | Day 0 | 37.88 ± 35.42 | 40.15 ± 33.62 | 0.79 |
| Day 14 | 87.12 ± 19.64 a | 79.55 ± 19.22 b | 0.118 | |
| Day 30 | 90.53 ± 18.50 a | 90.15 ± 18.69 b | 0.934 | |
| Role limitation due to Physical Problems (RF) | Day 0 | 57.58 ± 25.38 | 66.67 ± 27 | 0.164 |
| Day 14 | 98.48 ± 8.70 a | 100.00 ± 0.00 b | 0.321 | |
| Day 30 | 98.48 ± 8.70 a | 100.00 ± 0.00 b | 0.321 | |
| Role limitation due to Emotional Problems (RE) | Day 0 | 54.55 ± 38.25 | 56.06 ± 39.05 | 0.874 |
| Day 14 | 100.00 ± 0.00 a | 96.97 ± 17.41 b | 0.321 | |
| Day 30 | 100.00 ± 0.00 a | 96.97 ± 17.41 b | 0.321 | |
| Energy/Fatigue/Vitality (VT) | Day 0 | 41.21 ± 29.97 | 37.27 ± 33.66 | 0.617 |
| Day 14 | 90.30 ± 11.32 a | 82.73 ± 18.59 b | 0.05 | |
| Day 30 | 92.73 ± 10.98 a | 83.64 ± 21.91 b | 0.037 | |
| Emotional well-being Mental Health (MH) | Day 0 | 50.61 ± 30.1 | 51.52 ± 32.32 | 0.906 |
| Day 14 | 93.94 ± 9.33 a | 90.00 ± 12.25 b | 0.147 | |
| Day30 | 96.06 ± 8.99 a | 92.12 ± 12.19 b | 0.14 | |
| Social Functioning (SF) | Day 0 | 63.70 ± 33.69 | 61.21 ± 38.39 | 0.781 |
| Day 14 | 96.36 ± 12.45 a | 94.55 ± 9.05 b | 0.5 | |
| Day 30 | 96.36 ± 12.45 a | 96.97 ± 7.28 b | 0.81 | |
| Bodily Pain (BP) | Day 0 | 61.59 ± 26.07 | 52.27 ± 28.89 | 0.174 |
| Day 14 | 98.11 ± 10.88 a | 87.12 ± 17.81 b | 0.004 | |
| Day 30 | 98.11 ± 10.88 a | 94.69 ± 12.1 b | 0.39 | |
| General Health (GH) | Day 0 | 13.26 ± 16.52 | 16.67 ± 20.41 | 0.459 |
| Day 14 | 79.92 ± 18.73 a | 70.45 ± 19.22 b | 0.047 | |
| Day30 | 92.05 ± 18.70 a | 83.33 ± 20.41 b | 0.075 |
| Variables | Period | Pessary Group (n = 33) | Standard Group (n = 33) | p-Value |
|---|---|---|---|---|
| Random Blood Sugar (mg %) | Day 0 | 99.76 ± 12.97 | 99.88 ± 14.74 | 0.972 |
| Erythrocyte Sedimentation Rate (mm/1 h) | Day 0 | 35.85 ± 13.54 | 33.70 ± 14.59 | 0.537 |
| Day 14 | 30.91 ± 10.09 a | 35.36 ± 14.37 b | 0.15 | |
| Safety biomarkers | ||||
| Haemoglobin (Hb%) (gm%) | Day 0 | 11.35 ± 1.48 | 11.21 ± 1.15 | 0.665 |
| Day 14 | 11.17 ± 1.33 a | 11.26 ± 1.09 b | 0.779 | |
| Total Leucocyte Counts (cells/cumm) | Day 0 | 6515.15 ± 1439.21 | 6112.12 ± 1437.83 | 0.259 |
| Day 14 | 6309.09 ± 1673.20 a | 5975.75 ± 1267.4 b | 0.365 | |
| Aspartate aminotransferase (IU/L) | Day 0 | 22.28 ± 7.32 | 22.31 ± 9.52 | 0.988 |
| Day 14 | 21.33 ± 6.76 a | 22.24 ± 9.10 b | 0.647 | |
| Alanine transaminase (IU/L) | Day 0 | 24.62 ± 11.47 | 23.79 ± 11.3 | 0.769 |
| Day 14 | 23.76 ± 9.22 a | 24.97 ± 12.61 b | 0.657 | |
| Alkaline phosphatase (IU/L) | Day 0 | 199.60 ± 55.35 | 207.18 ± 42.04 | 0.533 |
| Day 14 | 204.52 ± 39.59 a | 202.27 ± 41.91 b | 0.824 | |
| Blood Urea (mg %) | Day 0 | 22.64 ± 5.63 | 23.12 ± 3.85 | 0.686 |
| Day 14 | 24.45 ± 3.59 a | 23.70 ± 4.21 b | 0.434 | |
| Serum Creatinine (mg %) | Day 0 | 0.76 ± 0.09 | 0.78 ± 0.10 | 0.52 |
| Day 14 | 0.76 ± 0.09 a | 0.75 ± 0.08 b | 0.579 | |
| Other investigations | ||||
| C-Reactive Protein | ||||
| Positive | Day 0 | 10 (100) | 8 (100) | 0.78 |
| Negative | Day 14 | 5 (50) | 5 (62.5) | 1.00 |
| Ultrasonography of abdomen | ||||
| Normal | - | 16 (48.5) | 21 (63.6) | 0.32 |
| PID | 17 (48.5) | 12 (36.4) | ||
| PH of vaginal discharge | Day 0 | 5.21 ± 1.05 | 4.70 ± 1.69 | 0.145 |
| Day 14 | 4.42 ± 0.71 | 3.48 ± 1.44 | 0.016 | |
| p value | 0.007 | 0.03 | ||
| Pap smear | ||||
| Normal | 6 (18.2) | 6 (18.2) | ||
| Inflammatory | Day 0 | 21 (63.6) | 24 (72.7) | 0.548 |
| Bacterial Vaginosis | 6 (18.2) | 3 (9.1) | ||
| Normal | 22 (66.7) | 10 (30.3) | ||
| Inflammatory | Day 14 | 11 (33.33) | 22 (66.7) | 0.003 |
| Bacterial Vaginosis | (0) | 1 (3) | ||
| p value | p < 0.001 | 0.365 | ||
| Cross Validation-Fold | Classifier | SENS | SPEC | ACC | PREC |
|---|---|---|---|---|---|
| 2 | DT | 57.40 | 59.80 | 57.40 | 55.70 |
| RF | 55.90 | 58.40 | 55.90 | 54.20 | |
| LR | 57.50 | 54.20 | 51.50 | 50.00 | |
| AB | 48.50 | 56.80 | 48.50 | 48.50 | |
| 5 | DT | 61.80 | 63.90 | 61.80 | 60.00 |
| RF | 52.90 | 55.60 | 52.90 | 51.40 | |
| LR | 48.50 | 51.50 | 48.50 | 46.90 | |
| AB | 50.00 | 54.20 | 50.00 | 50.20 | |
| 10 | DT | 51.50 | 54.20 | 51.50 | 50.30 |
| RF | 58.80 | 61.20 | 58.80 | 57.30 | |
| LR | 52.90 | 55.60 | 52.90 | 51.20 | |
| AB | 50.00 | 54.20 | 50.00 | 49.70 | |
| mean | 53.30 | 56.63 | 53.30 | 52.11 | |
| ±SD | 4.27 | 3.55 | 4.27 | 3.87 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Qayyum, S.; Sultana, A.; Heyat, M.B.B.; Rahman, K.; Akhtar, F.; Haq, A.u.; Alkhamis, B.A.; Alqahtani, M.A.; Gahtani, R.M. Therapeutic Efficacy of a Formulation Prepared with Linum usitatissimum L., Plantago ovata Forssk., and Honey on Uncomplicated Pelvic Inflammatory Disease Analyzed with Machine Learning Techniques. Pharmaceutics 2023, 15, 643. https://doi.org/10.3390/pharmaceutics15020643
Qayyum S, Sultana A, Heyat MBB, Rahman K, Akhtar F, Haq Au, Alkhamis BA, Alqahtani MA, Gahtani RM. Therapeutic Efficacy of a Formulation Prepared with Linum usitatissimum L., Plantago ovata Forssk., and Honey on Uncomplicated Pelvic Inflammatory Disease Analyzed with Machine Learning Techniques. Pharmaceutics. 2023; 15(2):643. https://doi.org/10.3390/pharmaceutics15020643
Chicago/Turabian StyleQayyum, Sana, Arshiya Sultana, Md Belal Bin Heyat, Khaleequr Rahman, Faijan Akhtar, Amin ul Haq, Batool Abdulelah Alkhamis, Mohammed Aedh Alqahtani, and Reem M. Gahtani. 2023. "Therapeutic Efficacy of a Formulation Prepared with Linum usitatissimum L., Plantago ovata Forssk., and Honey on Uncomplicated Pelvic Inflammatory Disease Analyzed with Machine Learning Techniques" Pharmaceutics 15, no. 2: 643. https://doi.org/10.3390/pharmaceutics15020643