
Therapeutic Monitoring of Orally Administered, Small-Molecule Anticancer Medications with Tumor-Specific Cellular Protein Targets in Peripheral Fluid Spaces—A Review

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
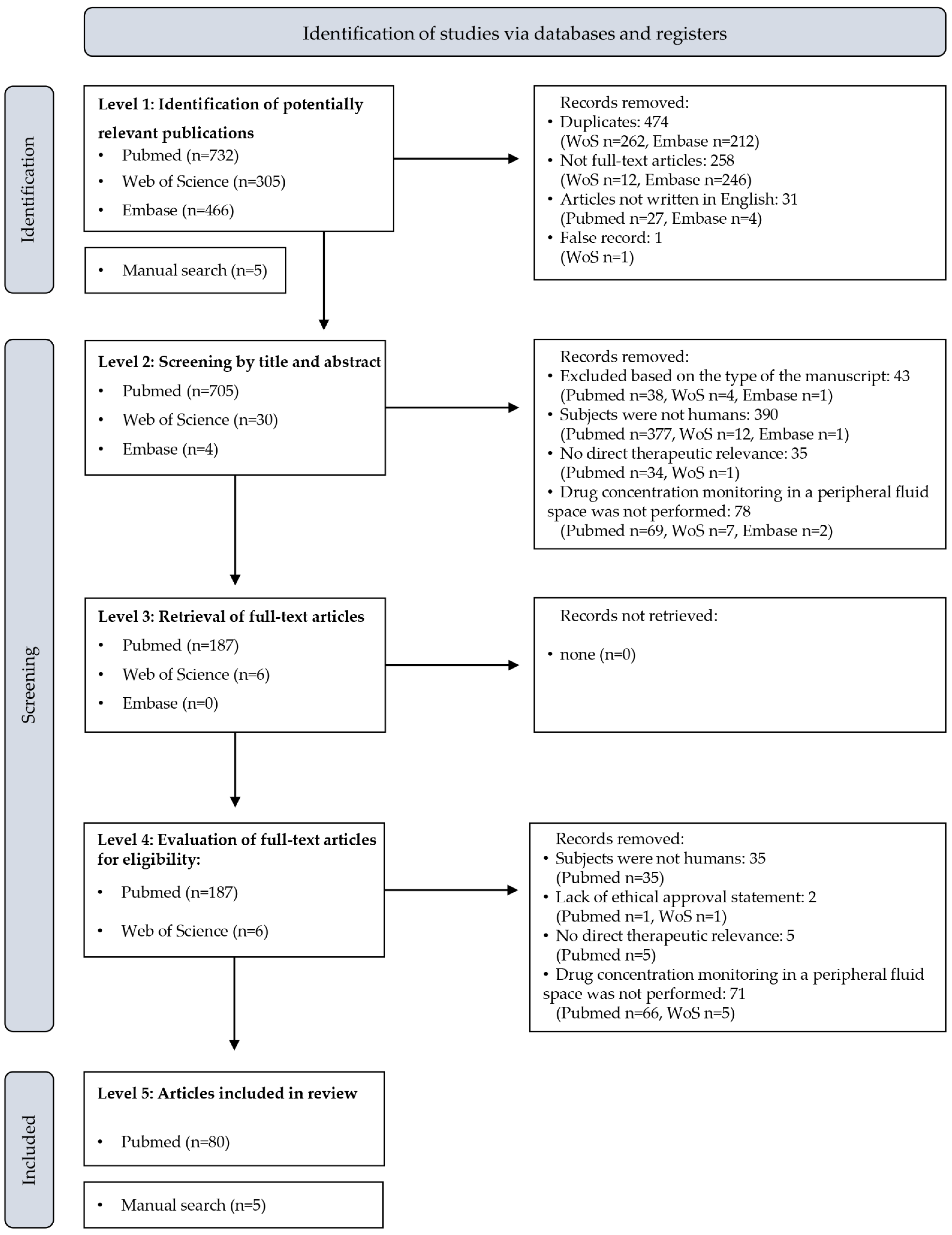
2.1. Database Search
2.2. Screening Eligible Database Records
2.3. Data Evaluation and Visualization
3. Results
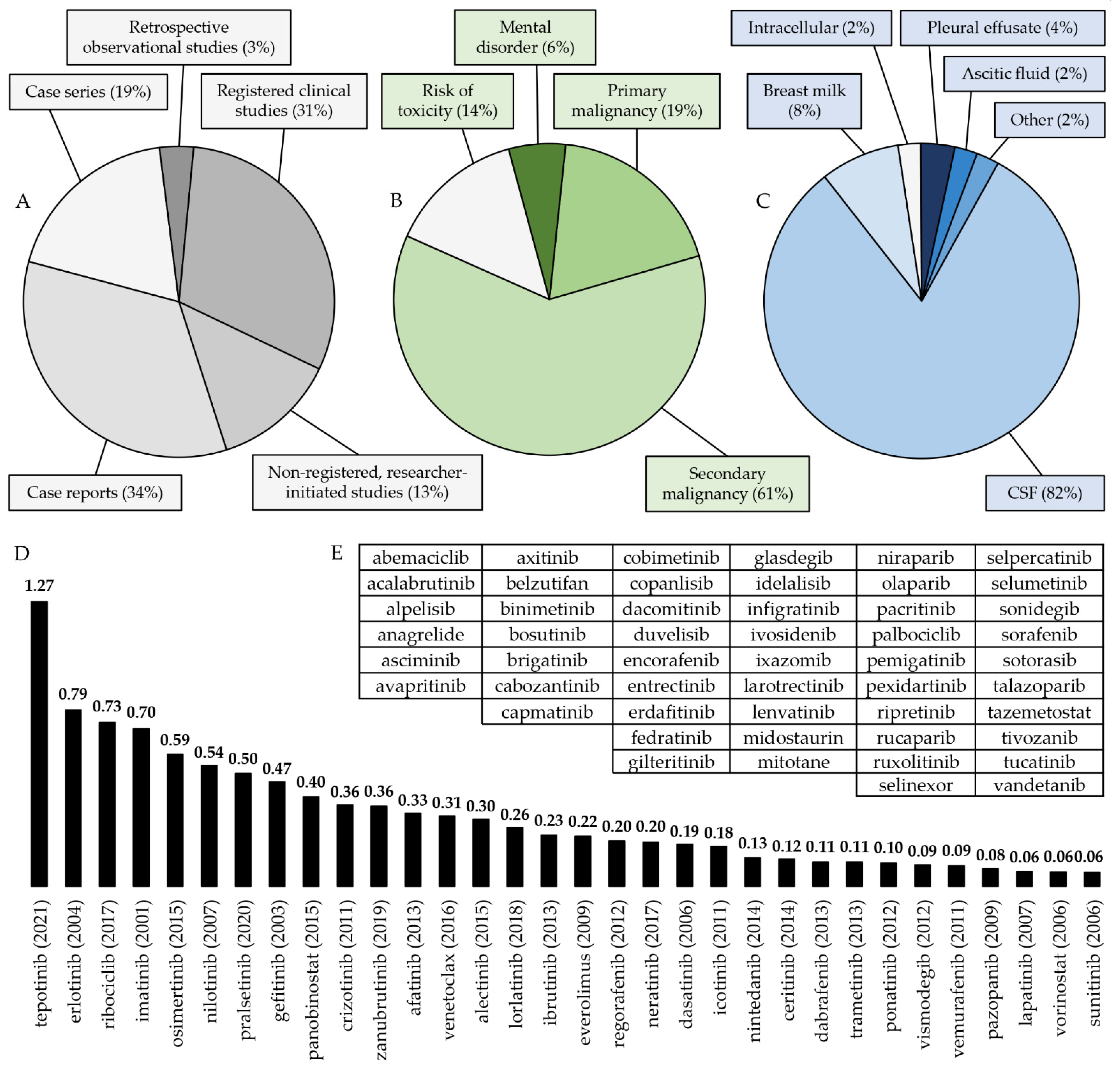
3.1. Summary of the Findings of the Literature Review
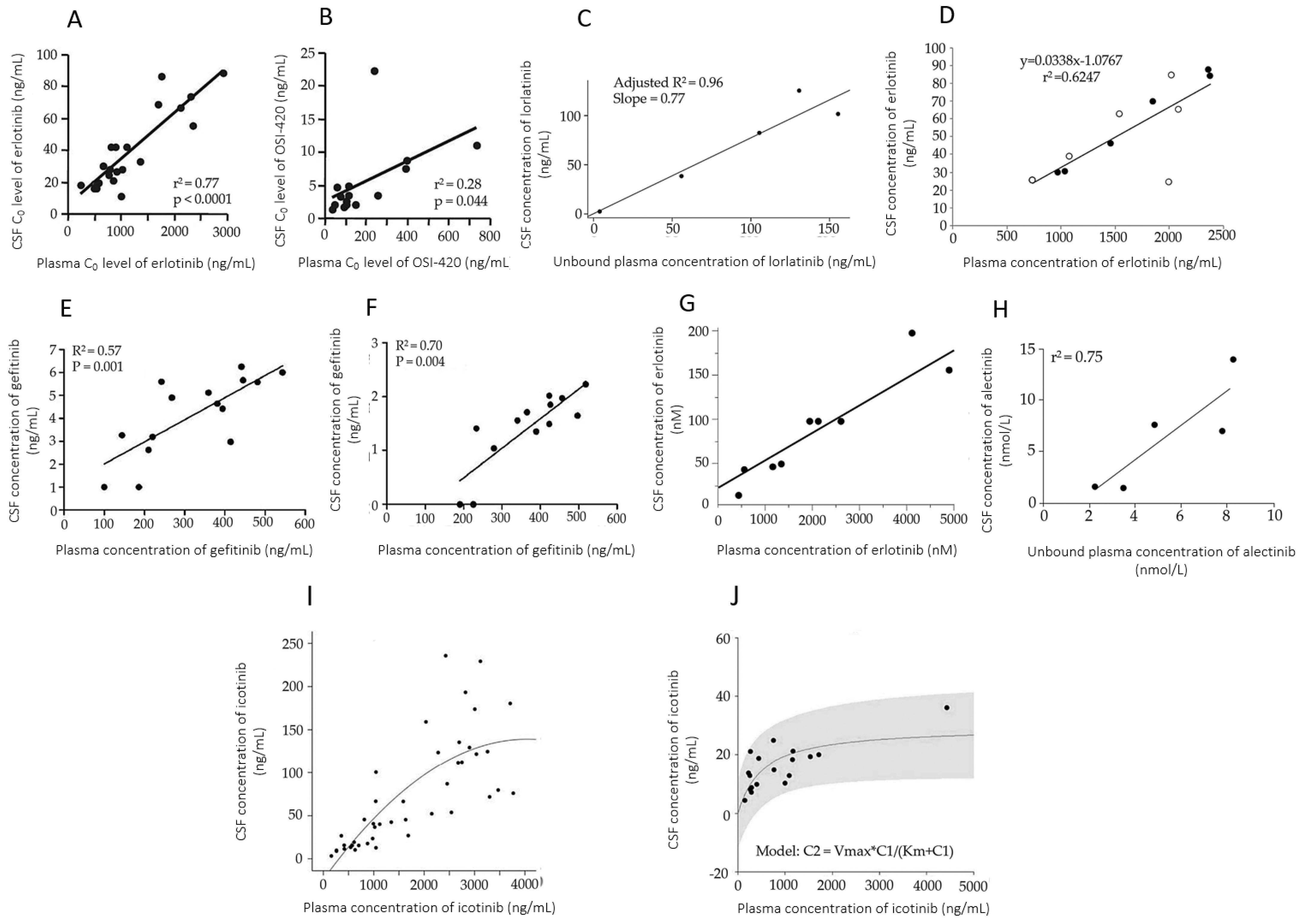
3.2. Monitoring the Concentrations of Oral Anticancer Drugs in Peripheral Fluids
3.2.1. Monitoring the Treatment of Primary Malignancies
Primary Malignant Central Nervous System Tumors
Other Primary Malignancies
3.2.2. Monitoring the Treatment of Malignant Tumor Metastases
Central Nervous System Metastases of Myeloproliferative Malignancies
Central Nervous System Metastases of Non Small-Cell Lung Cancer
Metastases of Other Malignancies in the Central Nervous System
Malignant Ascites
3.2.3. Monitoring OACDs to Control Toxicity
Monitoring the Exposure of the Infant to the Drug during Breastfeeding
Monitoring Other Types of Toxicity
3.2.4. Monitoring the Treatment of Mental Disorders
3.3. Bioanalytical Methods of Monitoring OACD Concentrations in Peripheral Fluid Spaces
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- McLaughlin, A.M.; Schmulenson, E.; Teplytska, O.; Zimmermann, S.; Opitz, P.; Groenland, S.L.; Huitema, A.D.R.; Steeghs, N.; Müller, L.; Fuxius, S.; et al. Developing a nationwide infratructure for therapeutic drug monitoring of targeted oral anticancer drugs: The ON-TARGET study protocol. Cancers 2021, 13, 6281. [Google Scholar] [CrossRef] [PubMed]
- Cohen, P.; Cross, D.; Jänne, P.A. Kinase drug discovery 20 years after imatinib: Progress and future directions. Nat. Rev. Drug Discov. 2021, 20, 551–569. [Google Scholar] [CrossRef] [PubMed]
- Reyner, E.; Lum, B.; Jing, J.; Kagedal, M.; Ware, J.A.; Dickmann, L.J. Intrinsic and extrinsic pharmacokinetic variability of small molecule targeted cancer therapy. Clin. Transl. Sci. 2020, 13, 410–418. [Google Scholar] [CrossRef] [PubMed]
- Verheijen, R.B.; Yu, H.; Schellens, J.H.M.; Beijnen, J.H.; Steeghs, N.; Huitema, A.D.R. Practical recommendations for therapeutic drug monitoring of kinase inhibitors in oncology. Clin. Pharm. Ther. 2017, 102, 765–776. [Google Scholar] [CrossRef]
- Saydam, G.; Ali, R.; Demir, A.M.; Eskazan, A.E.; Guvenc, B.; Haznedaroglu, I.C.; Mehmet, A.O.; Salim, O.; Sonmez, M.; Tuglular, A.T.; et al. The effects of comorbidities on the choice of tyrosine kinase inhibitors in patients with chronic myeloid leukemia. Int. J. Hematol. Oncol. 2022, 11, IJH38. [Google Scholar]
- Clarke, W.A.; Chatelut, E.; Fotoohi, A.K.; Larson, R.A.; Martin, J.H.; Mathijssen, R.H.J.; Salamone, S.J. Therapeutic drug monitoring in oncology: International Association of Therapeutic Drug Monitoring and Clinical Toxicology consensus guidelines for imatinib therapy. Eur. J. Cancer 2021, 157, 428–440. [Google Scholar] [CrossRef]
- Angeli, E.; Bousquet, G. Brain metastasis treatment: The place of tyrosine kinase inhibitors and how to facilitate their diffusion across the blood-brain barrier. Pharmaceutics 2021, 13, 1446. [Google Scholar] [CrossRef]
- Abruzzese, E.; Mauro, M.; Apperley, J.; Chelysheva, E. Tyrosine kinase inhibitors and pregnancy in chronic myeloid leukemia: Opinion, evidence, and recommendations. Ther. Adv. Hematol. 2020, 11, 2040620720966120. [Google Scholar] [CrossRef]
- Capone, F.; Albanese, A.; Quadri, G.; Di LAzzaro, V.; Falato, E.; Cortese, A.; De Giglio, L.; Ferraro, E. Disease-modifying drugs and breastfeeding in multiple sclerosis: A narrative literature review. Front. Neurol. 2022, 13, 851413. [Google Scholar] [CrossRef]
- Nash, P.; Kerschbaumer, A.; Dörner, T.; Dougados, M.; Fleishcmann, R.M.; Geissler, K.; McInnes, I.; Pope, J.E.; van der Heijde, D.; Stoffer-Marx, M.; et al. Points to consider for the treatment of immune-mediated inflammatory diseases with Janus kinase inhibitors: A consensus statement. Ann. Rheum. Dis. 2021, 80, 71–87. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Guntner, A.S.; Peyrl, A.; Mayr, L.; Englinger, B.; Berger, W.; Slavic, I.; Buchberger, W.; Gojo, J. Cerebrospinal fluid penetration of targeted therapeutics in pediatric tumor patients. Acta. Neuropathol. Commun. 2020, 8, 78. [Google Scholar] [CrossRef] [PubMed]
- Nambu, T.; Hamada, A.; Nakashima, R.; Yuki, M.; Kawaguchi, T.; Mitsuya, H.; Saito, H. Association of SLCO1B3 polymorphism with intracellular accumulation of imatinib in leukocytes in patients with chronic myeloid leukemia. Biol. Pharm. Bull. 2011, 34, 114–119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Francia, S.; D’Avolio, A.; Ariaudo, A.; Pirro, E.; Piccione, F.; Simiele, M.; Fava, C.; Calcagno, A.; Di Perri, G.; Saglio, G. Plasma and intracellular imatinib concentrations in patients with chronic myeloid leukemia. Ther. Drug Monit. 2014, 36, 410–412. [Google Scholar] [CrossRef]
- Petzer, A.; Gunsilius, E.; Hayes, M.; Stockhammer, G.; Duba, H.C.; Schneller, F.; Grünewald, K.; Poewe, W.; Gastl, G. Low concentrations of STI571 in the cerebrospinal fluid: A case report. Br. J. Haematol. 2002, 117, 623–625. [Google Scholar] [CrossRef]
- Takayama, N.; Sato, N.; O’Brian, S.G.; Ikeda, Y.; Okamoto, S. Imatinib mesylate has limited activity against the central nervous system invilvement of Philadelphia chromosome-positive acute lymphoblastic leukaemia due to poor penetration into cerebrospinal fluis. Br. J. Haematol. 2002, 119, 106–108. [Google Scholar] [CrossRef]
- Bornhauser, M.; Jenke, A.; Freiberg-Richter, J.; Radke, J.; Schuler, U.S.; Mohr, B.; Ehninger, G.; Schleyer, E. CNS blast crisis of chronic myelogenous leukemia in a patient with a major cytogenic response in bone marrow associated with low levels of imatinib mesylate and its N-desmethylated metabolite in cerebral spinal fluid. Ann. Hematol. 2004, 83, 401–402. [Google Scholar] [CrossRef]
- Le Coutre, P.; Kreuzer, K.A.; Pursche, S.; Bonin, M.V.; Leopold, T.; Baskaynak, G.; Dörken, B.; Ehningen, G.; Ottmann, O.; Jenke, A.; et al. Pharmacokinetics and cellular uptake of imatinib and its metabolite CGP74588. Cancer Chemother. Pharmacol. 2004, 53, 313–323. [Google Scholar] [CrossRef]
- Leis, J.F.; Stepan, D.E.; Curtin, P.T.; Ford, J.M.; Peng, B.; Schubach, S.; Druker, B.J.; Maziarz, R.T. Central nervous system failure in patients with chronic myelogenous leukemia lymphoid blast crisis and Philadelphia chromosome positive acute lymphoblastic leukemia treated with imatinib (STI-571). Leuk. Lymphoma 2004, 45, 695–698. [Google Scholar] [CrossRef]
- Russel, M.A.; Carpenter, M.W.; Akhtar, M.S.; Lagattuta, T.F.; Egorn, M.J. Imatinib mesylate and metabolite concentrations in maternal blood, umbilical cord blood, placenta and breast milk. J. Perinatol. 2007, 27, 241–243. [Google Scholar] [CrossRef]
- Gambacorti-Passerini, C.B.; Tornaghi, L.; Marangon, E.; Franceschino, A.; Pogliani, E.M.; D’Incalci, M.; Zucchetti, M. Imatinib concentrations in human milk. Blood 2007, 109, 1790. [Google Scholar] [CrossRef]
- Ali, R.; Ozkalemkas, F.; Kimya, Y.; Koksal, N.; Ozkocaman, V.; Gulten, T.; Yorulmaz, H.; Tunali, A. Imatinib use during pregnancy and breast feeding: A case report and review of the literature. Arch. Gynecol. Obstet. 2009, 280, 169–175. [Google Scholar] [CrossRef] [PubMed]
- Kronenberger, R.; Schleyer, E.; Bornhäuser, M.; Ehninger, G.; Gattermann, N.; Blum, S. Imatinib in breast milk. Ann. Hematol. 2009, 88, 1265–1266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burwick, R.M.; Kuo, K.; Brewer, D.; Druker, B.J. Maternal, Fetal, and Neonatal Imatinib Levels with Treatment of Chronic Myeloid Leukemia in Pregnancy. Obstet. Gynecol. 2017, 129, 831–834. [Google Scholar] [CrossRef] [PubMed]
- Terao, R.; Nil, M.; Asai, H.; Nohara, F.; Okamoto, T.; Nagaya, K.; Azuma, H. Breastfeeding in a patient with chronic myeloid leukemia during tyrosine kinase inhibitor therapy. J. Oncol. Pharm. Pract. 2021, 27, 756–760. [Google Scholar] [CrossRef]
- Chang, X.; Zhou, L.; Chen, X.; Xu, B.; Cheng, Y.; Sun, S.; Fang, M.; Xiang, Y. Impact of Imatinib on the Fertility of Male Patients with Chronic Myelogenous Leukaemia in the Chronic Phase. Target. Oncol. 2017, 12, 827–832. [Google Scholar] [CrossRef]
- Kondo, T.; Tasaka, T.; Matsumoto, K.; Matsumoto, R.; Koresawa, L.; Sano, F.; Tokunga, H.; Matsuhashi, Y.; Nakanishi, H.; Morita, K.; et al. Philadelphia chromosome-positive acute lymphoblastic leukemia with extramedullary and meningeal relapse after allogenic hematopoietic stem cell transplantation that was successfully treated with dasatinib. Springerplus 2014, 3, 177. [Google Scholar] [CrossRef] [Green Version]
- Gong, X.; Li, L.; Wei, H.; Liu, B.; Zhou, C.; Zhang, G.; Liu, K.; Lin, D.; Gong, B.; Wei, S.; et al. A higher Dose of Dasatinib May Increase the Possibility of Crossing the Blood-brain Barrier in the Treatment of Patients with Philadelphia Chromosome-positive Acute Lymphoblastic Leukemia. Clin. Ther. 2021, 43, 1265–1271. [Google Scholar] [CrossRef]
- Reinwald, M.; Schleyer, E.; Kiewe, P.; Blau, I.W.; Baurmeister, T.; Pursche, S.; Neumann, M.; Notter, M.; Thiel, E.; Hofmann, W.K.; et al. Efficacy and pharmacologic data of second-generation tyrosine kinase inhibitor nilotinib in BCR-ABL-positive leukemia patients with central nervous system relapse after allogenic stem cell transplantation. Biomed. Res. Int. 2014, 2014, 637059. [Google Scholar] [CrossRef] [Green Version]
- Liu, B.; Wang, Y.; Zhou, C.; Wei, H.; Lin, D.; Li, W.; Liu, K.; Zhang, G.; Wei, S.; Li, Y.; et al. Nilotinib combined with multi-agent chemotherapy in newly diagnosed Philadelphia chromosome-positive acute lymphoblastic leukemia: A single-center prospective study with long-term follow-up. Ann. Hematol. 2019, 98, 633–645. [Google Scholar] [CrossRef]
- Satoh, K.; Morisawa, S.; Okuyama, M.; Nakae, H. Severe pleural effusion associated with nilotinib for chronic myeloid leukaemia: Cross-intolerance with tyrosine kinase inhibitors. BMJ Case Rep. 2021, 14, e245671. [Google Scholar] [CrossRef] [PubMed]
- Pagan, F.; Hebron, M.; Valadez, E.H.; Torresy-Yaghi, Y.; Huang, X.; Mills, R.R.; Wilmarth, B.M.; Howard, H.; Dunn, C.; Carlson, A.; et al. Nilotinib Effects in Parkinson’s disease and Dementia with Lewy bodies. J. Parkinsons Dis. 2016, 6, 503–517. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pagan, F.L.; Hebron, M.L.; Wilmarth, B.; Torres-Yaghi, Y.; Lawler, A.; Mundel, E.E.; Yusuf, N.; Starr, N.J.; Arellano, J.; Howard, H.H.; et al. Pharmacokinetics and pharmacodynamics of a single dose Nilotinib in individuals with Parkinson’s disease. Pharmacol. Res. Perspect. 2019, 7, e00470. [Google Scholar] [CrossRef] [Green Version]
- Pagan, F.L.; Hebron, M.L.; Wilmarth, B.; Torres-Yaghi, Y.; Lawler, A.; Mundel, E.E.; Yusuf, N.; Starr, N.J.; Anjum, M.; Arello, J.; et al. Nilotinib Effects on Safety, Tolerability, and Potential Biomarkers in Parkinson Disease: A Phase 2 Randomized Clinical Trial. JAMA Neurol. 2020, 77, 309–317. [Google Scholar] [CrossRef] [Green Version]
- Simuni, T.; Fiske, B.; Merchant, K.; Coffey, C.S.; Klinger, E.; Caspell-Garcia, C.; Lafontant, D.E.; Matthews, H.; Wyse, R.K.; Brundin, P.; et al. Efficacy of Nilotinib in Patients With Moderately Advanced Parkinson Disease: A Randomized Clinical Trial. JAMA Neurol. 2021, 78, 312–320. [Google Scholar] [CrossRef] [PubMed]
- Turner, R.S.; Hebron, M.L.; Lawler, A.; Mundel, E.E.; Yusuf, N.; Starr, J.N.; Anjum, M.; Pagan, F.; Torres-Yaghi, Y.; Shi, W.; et al. Nilotinib Effects on Safety, Tolerability, and Biomarkers in Alzheimer’s Disease. Ann. Neurol. 2020, 88, 183–194. [Google Scholar] [CrossRef] [PubMed]
- Tanimura, K.; Yamassaki, K.; Okuhiro, Y.; Hira, K.; Nitani, C.; Okada, K.; Fujisaki, H.; Matsumoto, K.; Hara, J. Monitoring Ponatinib in a Child with Philadelphia Chromosome-Positive Acute Lymphoblastic Leukemia. Case Rep. Oncol. 2021, 14, 24–28. [Google Scholar] [CrossRef] [PubMed]
- Yamaguchi, T.; Isogai, S.; Okamura, T.; Uozu, S.; Mieno, Y.; Hoshino, T.; Goto, Y.; Hayashi, M.; Nakanishi, T.; Imaizumi, K. Pharmacokinetics of gefitinib in a patient with non-small cell lung cancer undergoing continuous ambulatory peritoneal dialysis. Case Rep. Oncol. 2015, 8, 78–82. [Google Scholar] [CrossRef]
- Fukuhara, T.; Saijo, Y.; Sakakibara, T.; Inoue, A.; Morikawa, N.; Kanamori, M.; Nakashima, I.; Nukiwa, T. Successful treatment of carcinomatous meningitis with gefitinib in a patient with lung adenocarcinoma harboring a mutated EGF receptor gene. Tohoku J. Exp. Med. 2008, 214, 359–363. [Google Scholar] [CrossRef] [Green Version]
- Zhao, J.; Chen, M.; Zhong, W.; Zhang, L.; Li, L.; Xiao, Y.; Nie, L.; Hu, P.; Wang, M. Cerebrospinal fluid concentrations of gefitinib in patients with lung adenocarcinoma. Clin. Lung Cancer 2013, 14, 188–193. [Google Scholar] [CrossRef]
- Zeng, Y.D.; Liao, H.; Qin, T.; Zhang, L.; Wei, W.D.; Liang, J.Z.; Xu, F.; Dinglin, X.X.; Ma, S.X.; Chen, L.K. Blood-brain barrier permeability of gefitinib in patients with brain metastases from non-small-cell lung cancer before and during whole brain radiation therapy. Oncotarget 2015, 6, 8366–8367. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.; Ye, X.; Xu, Y.; Chen, M.; Zhong, W.; Sun, Y.; Yang, Z.; Zhu, G.; Gu, Y.; Wang, M. EGFR mutation status of paired cerebrospinal fluid and plasma sample in EGFR mutant non-small cell lung cancer with leptomeningeal metastases. Cancer Chemother. Pharmacol. 2016, 78, 1305–1310. [Google Scholar] [CrossRef] [PubMed]
- Jackman, D.M.; Cioffredi, L.A.; Jacobs, L.; Sharmeen, F.; Morse, L.K.; Lucca, J.; Plotkin, S.R.; Marcoux, P.J.; Rabin, M.S.; Lynch, T.J.; et al. A phase I trial of high dose gefitinib for patients with leptomeningeal metastases from non-small cell lung cancer. Oncotarget 2015, 6, 4527–4536. [Google Scholar] [CrossRef] [Green Version]
- Fang, L.; Sun, X.; Song, Y.; Zhang, Y.; Li, F.; Xu, Y.; Ma, S.; Lin, N. Whole-brain radiation fails to boost intracerebral gefitinib concentration in patients with brain mestastatic non-small cell lung cancer: A self-controlled, pilot study. Cancer Chemother. Pharmacol. 2015, 76, 873–877. [Google Scholar] [CrossRef]
- Togashi, Y.; Masago, K.; Masuda, S.; Mizuno, T.; Fukudo, M.; Ikemi, Y.; Sakamori, Y.; Nagai, H.; Kim, Y.H.; Katsura, T.; et al. Cerebrospinal fluid concentration of gefitinib and erlotinib in patients with non-small cell lung cancer. Cancer Chemother. Pharmacol. 2012, 70, 399–405. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shriyan, B.; Patil, D.; Gurjar, M.; Nookala, M.; Patil, A.; Kannan, S.; Patil, V.; Joshi, A.; Noronha, V.; Prabhash, K.; et al. Safety and CSF distribution of high-dose erlotinib and gefitinib in patients of non-small cell lung cancer (NSCLC) with brain mtastases. Eur. J. Clin. Pharmacol. 2020, 76, 1427–1436. [Google Scholar] [CrossRef] [PubMed]
- Broniscer, A.; Panetta, J.C.; O’Shaunghnessy, M.; Fraga, C.; Bai, F.; Krasin, M.J.; Gajjar, A.; Stewart, C.F. Plasma and cerebrospinal fluid pharmacokinetics of erlotinib and its active metabolite OSI-420. Clin. Cancer Res. 2007, 13, 1511–1515. [Google Scholar] [CrossRef] [Green Version]
- Rogers, L.R.; LoRusso, P.; Nadler, P.; Malik, G.; Shields, A.; Kaelin, W. Erlotinib therapy for central nervous system hemangioblastomatosis associated with von Hippel-Lindau disease: A case report. J. Neurooncol. 2011, 101, 307–310. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Masago, K.; Togashi, Y.; Fukudo, M.; Terada, T.; Irisa, K.; Sakamori, Y.; Kim, Y.H.; Mio, T.; Inui, K.; Mishima, M. Plasma and pleural fluid pharmacokinetics of erlotinib and its active metabolite OSI-420 in patients with non-small-cell lung cancer with pleural effusion. Clin. Lung Cancer 2011, 12, 307–312. [Google Scholar] [CrossRef]
- Masuda, T.; Hattori, N.; Hamada, A.; Iwamoto, H.; Ohshimo, S.; Kanehara, M.; Ishikawa, N.; Fujitaka, K.; Haruta, Y.; Murai, H.; et al. Erlotinib efficacy and cerebrospinal fluid concentration in patients with lung adenocarcinoma developing leptomeningeal metastases during gefiinib therapy. Cancer Chemother. Pharmacol. 2011, 67, 1465–1469. [Google Scholar] [CrossRef]
- Togashi, Y.; Masago, K.; Fukudo, M.; Tereda, T.; Fujita, S.; Irisa, K.; Sakamori, Y.; Kim, Y.H.; Mio, T.M.; Inui, K.; et al. Cerebrospinal fluid concentration of erlotinib and its active metabolite OSI-420 in patients with central nervous system metastases of non-small cell lung cancer. J. Thorac. Oncol. 2010, 5, 950–955. [Google Scholar] [CrossRef] [PubMed]
- Deng, Y.; Feng, W.; Wu, J.; Chen, Z.; Tang, Y.; Zhang, H.; Liang, J.; Xian, H.; Zhang, S. The concentration of erlotinib in the cerebrospinal fluid of patients with brain metastasis from non-small-cell lung cancer. Mol. Clin. Oncol. 2014, 2, 116–120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sakata, Y.; Kawamura, K.; Shingu, N.; Ichikado, K. Erlotinib plus bevacizumab as an effective treatment for leptomeningeal metastases from EGFR mutation-positive non-small cell lung cancer. Lung Cancer 2016, 99, 120–122. [Google Scholar] [CrossRef] [PubMed]
- Clarke, J.L.; Pao, W.; Wu, N.; Miller, V.A.; Lassman, A.B. High dose weekly erlotinib achieves therapeutic concentrations in CSF and is effective in leptomeningeal metastases from epidermal growth factor receptor mutant lung cancer. J. Neurooncol. 2010, 99, 283–286. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, H.; Yang, X.; Zhang, Y.; Liu, X.; Deng, Q.; Zhao, M.; Xu, X.; He, J. Erlotinib in combination with pemetrexed/cisplatin for leptomeningeal metastases and cerebrospinal fluid drug concentrations in lung adenocarcinoma patients after gefitinib failure. Target Oncol. 2015, 10, 135–140. [Google Scholar] [CrossRef] [PubMed]
- Togashi, Y.; Masago, K.; Fukudo, M.; Tsuchido, Y.; Okuda, C.; Kim, Y.H.; Ikemi, Y.; Sakamori, Y.; Mio, T.; Katsura, T.; et al. Efficacy of increased-dose erlotinib for central nervous system metastases in non-small cell lung cancer patients with epidermal growth factor receptor mutation. Cancer Chemother. Pharmacol. 2011, 68, 1089–1092. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fukudo, M.; Ikemi, Y.; Togashi, Y.; Masago, K.; Kim, Y.H.; Mio, T.; Tereda, T.; Teramukai, S.; Mishima, M.; Inui, K.; et al. Population pharmacokinetics/pharmacodynamics of erlotinib and pharmacogenomic analysis of plasma and cerebrospinal fluid drug concentrations in Japanese patients with non-small cell lung cancer. Clin. Pharmacokinet. 2013, 52, 593–609. [Google Scholar] [CrossRef] [PubMed]
- Nosaki, K.; Yamanaka, T.; Hamada, A.; Shiraishi, Y.; Harada, T.; Himeji, D.; Kitazaki, T.; Ebi, N.; Shimose, T.; Seto, T.; et al. Erlotinib for Non-Small Cell Lung Cancer with Leptomeningeal metastases: A Phase II Study (LOGIK1101). Oncologist 2020, 25, e1869–e1878. [Google Scholar] [CrossRef] [PubMed]
- Hoffknecht, P.; Tufman, A.; Wehler, T.; Pelzer, T.; Wiewrodt, R.; Schütz, M.; Serke, M.; Stöhlmacher-Williams, J.; Märten, A.; Maria Huber, R.; et al. Efficacy of the irreversible ErbB family blocker afatinib in epidermal growth factor receptor (EGFR) tyrosine kinase inhibitor (TKI)-penetrated non-small-cell lung cancer patients with brain metastases or leptomeningeal disease. J. Thorac. Oncol. 2015, 10, 156–163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kawaguchi, Y.; Hanoka, J.; Hayashi, H.; Mizusaki, N.; Iihara, H.; Itoh, Y.; Sugiyama, T. Clinical Efficacy of Afatinib Treatment for a Patient with Leptomeningeal Carcinomatosis. Chemotherapy 2017, 62, 147–150. [Google Scholar] [CrossRef]
- Tamiya, A.; Tamiya, M.; Nishihara, T.; Shiroyama, T.; Nakao, K.; Tsuji, T.; Takeuchi, N.; Isa, S.I.; Omachi, N.; Okamoto, N.; et al. Cerebrospinal Fluid Penetration rate and Efficacy of Afatinib in Patients with EGFR Mutation-positive Non-small Cell Lung Cancer with Leptomeningeal Carcinomatosis: A Multicenter Prospective Study. Anticancer Res. 2017, 37, 4177–4182. [Google Scholar] [PubMed]
- Song, Y.; Liu, P.; Huang, Y.; Guan, Y.; Han, X.; Shi, Y. Osimertinib Quantitative and Gene Variation Analysis in Cerebrospinal Fluid and Plasma of a Non-small Cell Lung Cancer Patient with leptomeningeal Metastases. Curr. Cancer Drug Targets 2019, 19, 666–673. [Google Scholar] [CrossRef] [PubMed]
- Xing, L.; Pan, Y.; Shi, Y.; Shu, Y.; Feng, J.; Li, W.; Cao, L.; Wang, L.; Gu, W.; Song, Y.; et al. Biomarkers of Osimertinib Response in Patients with Refractory, EGFR-T790M-positive Non-Small Cell Lung Cancer and Central Nervous System Metastases: The APOLLO Study. Clin. Cancer Res. 2020, 26, 6168–6175. [Google Scholar] [CrossRef] [PubMed]
- Yamaguchi, H.; Wakuda, K.; Fukuda, M.; Kenmotsu, H.; Mukae, H.; Ito, K.; Chibana, K.; Inoue, K.; Tanaka, K. A Phase II Study of Osimertinib for Radiotherapy-Naive Central Nervous System Metastasis From NSCLC: Results for the T790M Cohort of the OCEAN Study (LOGIK1603/WJOG9116L). J. Thorac. Oncol. 2021, 16, 2121–2132. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Z.; Su, C.; Xiu, W.; Wang, W.; Zeng, S.; Huang, M.; Gong, Y.; Lu, Y.; Zhang, Y. Response to Pralsetinib Observed in Meningeal-Metastatic EGFR-Mutant NSCLC With Acquired RET Fusion: A Brief Report. JTO Clin. Res. Rep. 2022, 3, 100343. [Google Scholar] [CrossRef] [PubMed]
- Fan, Y.; Huang, Z.; Fang, L.; Miao, L.; Gong, L.; Yu, H.; Yang, H.; Lei, T.; Mao, W. A phase II study of icotinib and whole-brain radiotherapy in Chinese patients with brain metastases from non-small cell lung cancer. Cancer Chemother. Pharmacol. 2015, 76, 517–523. [Google Scholar] [CrossRef]
- Zhou, L.; He, J.; Xiong, W.; Liu, Y.; Xiang, J.; Yu, Q.; Liang, M.; Zhou, X.; Ding, Z.; Huang, M.; et al. Impact of whole brain radiation therapy on CSF penetration ability of Icotinib in EGFR-mutated non-small cell lung cancer patients with brain metastases: Results of phase I dose-escalation study. Lung Cancer 2016, 96, 93–100. [Google Scholar] [CrossRef] [PubMed]
- Sakji-Dupré, L.; Le Rhun, E.; Templier, C.; Desmedt, E.; Blanchet, B.; Mortier, L. Cerebrospinal fluid concentration of vemurafenib in patients treated for brain metastatic BRAF-V600 mutated melanoma. Melanoma Res. 2015, 25, 302–305. [Google Scholar] [CrossRef]
- Hottinger, A.F.; Bensaid, D.; Micheli, R.D.; Moura, B.; Mokhtari, K.; Cardoso, E.; Idbaih, A.; Stupp, R. Leptomeningeal tumor response to combined MAPK/ERK inhibition in V600E-mutated gliomas despite undetectable CSF drug levels. Ann. Oncol. 2019, 30, 155–156. [Google Scholar] [CrossRef]
- Costa, D.B.; Kobayashi, S.; Pandaya, S.S.; Yeo, W.; Shen, Z.; Tan, W.; Wilner, K.D. CSF concentration of the anaplastic lymphoma kinase inhibitor crizotinb. J. Clin. Oncol. 2011, 29, e443–e445. [Google Scholar] [CrossRef]
- Metro, G.; Lunardi, G.; Floridi, P.; Pascali, J.P.; Marcomigni, L.; Chiari, R.; Ludovini, V.; Crinó, L.; Gori, S. CSF Concentration of Crizotinib in Two ALK-Positive Non-Small-Cell Lung Cancer Patients with CNS metastases Deriving Clinical Benefit from Treatment. J. Thorac. Oncol. 2015, 10, e26–e27. [Google Scholar] [CrossRef] [PubMed]
- Okawa, S.; Shibayama, T.; Shimonishi, A.; Nishimura, J.; Ozeki, T.; Takada, K.; Kayatani, H.; Minami, D.; Sato, K.; Fujiwara, K.; et al. Success of Crizotinib Combined with Whole-Brain Radiotherapy for Brain Metastases in a Patient with Anaplastic Lymphoma Kinase Rearrangement-Positive Non-Small-Cell Lung Cancer. Case Rep. Oncol. 2018, 11, 777–783. [Google Scholar] [CrossRef]
- Okimoto, T.; Tsubasa, Y.; Hotta, T.; Hamaguchi, M.; Nakado, M.; Hamaguchi, S.I.; Hamada, A.; Isobe, T. A Low Crizotinib Concentration in the Cerebrospinal Fluid Causes Ineffective treatment of Anaplastic Lymphoma Kinase-positive Non-small Cell Lung Cancer with Carcinomatous Meningitis. Intern. Med. 2019, 58, 703–705. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mehta, S.; Fiorelli, R.; Bao, X.; Pennington-Krygier, C.; Derogatis, A.; Kim, S.; Yoo, W.; Li, J.; Sanai, N. A Phase 0 Trial of Ceritinib in Patients with Brain Metastasis and Recurrent Glioblastoma. Clin. Cancer Res. 2022, 28, 289–297. [Google Scholar] [CrossRef] [PubMed]
- Gadgeel, S.M.; Grandhi, L.; Riely, G.J.; Chiappori, A.A.; West, H.L.; Azada, M.C.; Morcos, P.N.; Lee, R.M.; Garcia, L.; Yu, L.; et al. Safety and activity of alectinib against systemic disease and brain metastases in patients with crizotinib-resistant ALK-rearranged non-small-cell lung cancer (AF-002JG): Results from the dose-finding portion of a phase 1/2 study. Lancet Oncol. 2014, 15, 1119–1128. [Google Scholar] [CrossRef]
- Metro, G.; Lunardi, G.; Bennati, C.; Chiarini, P.; Sperduti, I.; Ricciuti, B.; Marcomigni, L.; Costa, C.; Crinó, L.; Floridi, P.; et al. Alectinib’s activity against CNS metastases from ALK-positive non-small cell lung cancer: A single institution case series. J. Neurooncol. 2016, 129, 355–361. [Google Scholar] [CrossRef]
- Sun, S.; Pithavala, Y.K.; Martini, Y.F.; Chen, J. Evaluation of Lorlatinib Cerebrospinal Fluid Concentrations in Relation to Target Concentrations for Anaplastic lymphoma Kinase (ALK) Inhibition. J. Clin. Pharmacol. 2022, 62, 1170–1176. [Google Scholar] [CrossRef]
- Miller, T.W.; Traphagen, N.A.; Li, J.; Lewis, L.D.; Lopes, B.; Asthagiri, A.; Loomba, J.; de Jong, J.; Schiff, D.; Patel, S.H.; et al. Tumor pharmacokinetics and pharmacodynamics of the CDK4/6 inhibitor ribociclib in patients with recurrent glioblastoma. J. Neurooncol. 2019, 144, 563–572. [Google Scholar] [CrossRef]
- Tien, A.; Li, J.; Bao, X.; Derogatis, A.; Kim, S.; Mehta, S.; Sanai, N. A Phase 0 Trial of Ribociclib in Recurrent Glioblastoma Patients Incorporating a Tumor Pharmacodynamic- and Pharmacokinetic-Guided Expansion Cohort. Clin. Cancer Res. 2019, 25, 5777–5786. [Google Scholar] [CrossRef] [Green Version]
- DeWire, M.D.; Fuller, C.; Campagne, O.; Lin, T.; Pan, H.; Poussaint, T.Y.; Baxter, P.A.; Hwang, E.I.; Bukowinski, A.; Dorris, K.; et al. A Phase I and Surgical Study of Ribociclib and Everolimus in Children with Recurrent or Refractory Malignant Brain Tumors: A Pediatric Brain Tumor Consortium Study. Clin. Cancer Res. 2021, 27, 2442–2451. [Google Scholar] [CrossRef]
- Fiocchi, R.; D’Elia, E.; Vittori, C.; Sebastiani, R.; Strobelt, N.; Eleftheriou, G.; Introna, M.; Freddi, C.; Crippa, A. First Report of a Successful Pregnancy in an Everolimus-Treated Hear-Transplanted Patient: Neonatal Disappearance of Immunosuppressive Drugs. Am. J. Transplant. 2016, 16, 1319–1322. [Google Scholar] [CrossRef] [PubMed]
- Molenaar-Kuijsten, L.; Verheijen, R.B.; Jacobs, B.A.W.; Thijssen, B.; Rosing, H.; Dorlo, T.P.C.; Beijnen, J.H.; Steeghs, N.; Huitema, A.D.R. Everolimus Concentration in Saliva to Predict Stomatitis: A Feasibility Study in Patients with Cancer. Ther. Drug Monit. 2022, 44, 520–526. [Google Scholar] [CrossRef] [PubMed]
- Gori, S.; Lunardi, G.; Inno, A.; Foglietta, J.; Cardinali, B.; Del Mastro, L.; Crinó, L. Lapatinib concentration in cerebrospinal fluid in two patients with HER2-positive metastatic breast cancer and brain metastases. Ann. Oncol. 2014, 25, 912–913. [Google Scholar] [CrossRef]
- Freedman, R.A.; Gelman, R.S.; Agar, N.Y.R.; Santagata, S.; Randall, E.C.; Gimenez-Cassina Lopez, B.; Connolly, R.M.; Dunn, I.F.; Van Poznak, C.H.; Anders, C.K.; et al. Pre- and Postoperative Neratinib for HER2-Positive Breast Cancer Brain Metastases: Translational Breast Cancer Research Consortium 022. Clin. Breast Cancer 2020, 20, 145–151.e2. [Google Scholar] [CrossRef] [PubMed]
- Law, S.C.; Hoang, T.; O’Rourke, K.; Tobin, J.W.D.; Gunawardana, J.; Loo-Oey, D.; Bednarska, K.; de Long, L.M.; Sabdia, M.B.; Hapgood, G.; et al. Successful treatment of Epstein-Barr virus-associated primary central nervous system lymphoma due to post-transplantation lymphoproliferative disorder, with ibrutinib and third-party Epstein-Barr virus-specific T cells. Am. J. Transplant. 2021, 21, 3465–3471. [Google Scholar] [CrossRef]
- Yu, H.; Kong, H.; Li, C.; Dong, X.; Wu, Y.; Zhuang, Y.; Han, S.; Lei, T.; Yang, H. Bruton’s tyrosine kinase inhibitors in primary central nervous system lymphoma-evaluation of anti-tumor efficacy and brain distribution. Transl. Cancer Res. 2021, 10, 1975–1983. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Li, Y.; Zhuang, Z.; Wang, W.; Wei, C.; Zhao, D.; Zhou, D.; Zhang, W. Preliminary Evaluation of Zanubrutinib-Containing Regimens in DLBCL and the Cerebrospinal Fluid Distribution of Zanubrutinib: A 13-Case Series. Front. Oncol. 2021, 11, 760405. [Google Scholar] [CrossRef] [PubMed]
- Krens, S.D.; Mulder, S.F.; van Erp, N.P. Lost in third space: Altered tyrosine-kinase inhibitor pharmacokinetics in a patient with malignant ascites. Cancer Chemother. Pharmacol. 2022, 89, 271–274. [Google Scholar] [CrossRef] [PubMed]
- Zeiner, P.S.; Kinzig, M.; Divé, I.; Maurer, G.D.; Filipski, K.; Harter, P.N.; Senft, C.; Bähr, O.; Hattinen, E.; Steinbach, J.P.; et al. Regorafenib CSF Penetration, Efficacy, and MRI Patterns in Recurrent Malignant Glioma Patients. J. Clin. Med. 2019, 8, 2031. [Google Scholar] [CrossRef] [Green Version]
- Tanaka, H.; Taima, K.; Makiguchi, T.; Nakagawa, J.; Niiko, T.; Tasaka, S. Activity and bioavailability of tepotinib for leptomeningeal metastasis of NSCLC with MET exon skipping mutation. Cancer Commun. 2021, 41, 83–87. [Google Scholar] [CrossRef]
- Ninomaru, T.; Okada, H.; Fujishima, M.; Irie, K.; Fukushima, S.; Hata, A. Lazarus Response to Tepotinib for Leptomeningeal metastases in a Patient with MET Exon 14 Skipping Mutation-Positive Lung Adenocarcinoma. Case Report. JTO Clin. Res. Rep. 2021, 2, 100145. [Google Scholar] [CrossRef]
- Rasmussen, T.A.; Tolstrup, M.; Møller, H.J.; Brinkmann, C.R.; Olesen, R.; Erikstrup, C.; Laursen, A.L.; Østergaard, L.; Søgaard, O.S. Activation of latent human immunodeficiency virus by the histone deacetylase inhibitor panobinostat: A pilot study to assess effects on the central nervous system. Open Forum Infect. Dis. 2015, 2, ofv037. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goldberg, J.; Sulis, M.L.; Bender, J.; Jeha, S.; Gardner, R.; Pollard, J.; Aquino, V.; Laetsch, T.; Winick, N.; Fu, C.; et al. A phase I study of panobinostat in children with relapse and refractory hematologic malignancies. Pediatr. Hematol. Oncol. 2020, 37, 465–474. [Google Scholar] [CrossRef] [PubMed]
- Gajjar, A.; Stewart, C.F.; Ellison, D.W.; Kaste, S.; Kun, L.E.; Packer, R.J.; Goldman, S.; Chintagumpala, M.; Wallace, D.; Takebe, N.; et al. Phase I study of vismodegib in children with recurrent or refractory medulloblastoma: A pediatric brain tumor consortium study. Clin. Cancer Res. 2013, 19, 6305–6312. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reda, G.; Cassin, R.; Dovrtelova, G.; Matteo, C.; Giannotta, J.; D’Incalci, M.; Cortelezzi, A.; Zucchetti, M. Venetoclax penetrates in cerebrospinal fluid and may be effective in chronic lymphocytic leukemia with central nervous system involvement. Hematologica 2019, 104, e222–e223. [Google Scholar] [CrossRef] [Green Version]
- Condorelli, A.; Matteo, C.; Leotta, S.; Schininá, G.; Sciortino, R.; Piccolo, G.M.; Parrinello, N.L.; Proietto, M.; Camuglia, M.G.; Zucchetti, M.; et al. Venetoclax penetrates in cerebrospinal fluid of an acute myeloid leukemia patient with leptomeningeal involvement. Cancer Chemother. Pharmacol. 2022, 89, 267–270. [Google Scholar] [CrossRef]
- Bareschino, M.A.; Schettino, C.; Troiani, T.; Martinelli, E.; Morgillo, F.; Ciardiello, F. Erlotinib in cancer treatment. Ann. Oncol. 2007, 6, 35–41. [Google Scholar] [CrossRef]
- Psallidas, I.; Kalomenidis, I.; Porcel, J.M.; Robinson, B.W.; Stathopoulos, G.T. Malignant pleural effusion: From bench to bedside. Eur. Respir. Rev. 2016, 25, 189–198. [Google Scholar] [CrossRef]
- Deak, D.; Gorcea-Andronic, N.; Sas, V.; Teodorescu, P.; Constantinescu, C.; Iluta, S.; Pasca, S.; Hotea, I.; Turcas, C.; Moisoiu, V.; et al. A narrative review of central nervous system involvement in acute leukemias. Ann. Transl. Med. 2021, 9, 68. [Google Scholar] [CrossRef]
- Lenk, L.; Alsadeq, A.; Schewe, D.M. Involvement of the central nervous system in acute lymphoblastic leukemia: Opinions on molecular mechanisms and clinical implications based on recent data. Cancer Metastasis Rev. 2020, 39, 173–187. [Google Scholar] [CrossRef] [Green Version]
- Kretz, O.; Weiss, H.M.; Schumacher, M.M.; Gross, G. In vitro blood distribution and plasma protein binding of the tyrosine kinase inhibitor imatinib and its active metabolite, CGP74588, in rat, mouse, dog, monkey, healthy humans and patients acute lymphatic leukaemia. Br. J. Clin. Pharmacol. 2004, 58, 212–216. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Brahmer, J.; Messersmith, W.; Hidalgo, M.; Baker, S.D. Binding of gefitinib, an inhibitor of epidermal growth factor receptor-tyrosine kinase, to plasma proteins and blood cells: In vitro and in cancer patients. Invest. New Drugs 2006, 24, 291–297. [Google Scholar] [CrossRef] [PubMed]
- Muller, I.B.; De Langen, A.J.; Honeywell, R.J.; Giovanni, E.; Peters, G.J. Overcoming crizotinib resistance in ALK-rearranged NSCLC with the second-generation ALK-inhibitor ceritinib. Expert Rev. Anticancer Ther. 2016, 16, 147–157. [Google Scholar] [CrossRef] [PubMed]
- Wind, S.; Schnell, D.; Ebner, T.; Freiwald, M.; Stopfer, P. Clinical Pharmacokinetics and Pharmacodynamics of Afatinib. Clin. Pharmacokinet. 2017, 56, 235–250. [Google Scholar] [CrossRef] [Green Version]
- Andreu, I.; Lence, E.; González-Bello, C.; Mayorga, C.; Cuquerella, M.C.; Vayá, I.; Miranda, M.A. Protein Binding of Lapatinib and its N- and O-Dealkylated Metabolites Interrogated by Fluorescence, Ultrafast Spectroscopy and Molecular Dynamics Simulations. Front. Pharmacol. 2020, 11, 576495. [Google Scholar] [CrossRef]
- Zhang, W.; Heinzmann, D.; Grippo, J.F. Clinical Pharmacokinetics of Vemurafenib. Clin. Pharmacokinet. 2017, 56, 1033–1043. [Google Scholar] [CrossRef]
- Matsusaki, K.; Aridome, K.; Emoto, S.; Kajiyama, H.; Takagaki, N.; Takahashi, T.; Tsubamoto, H.; Nagao, S.; Watanabe, A.; Shimada, H.; et al. Clinical practice guideline for the treatment of malignant ascites: Section summary in Clinical Practice Guideline for peritoneal dissemination (2021). Int. J. Clin. Oncol. 2022, 27, 1–6. [Google Scholar] [CrossRef]
- Benn, C.L.; Dawson, L.A. Clinically precedented protein kinases: Rationale for their use in neurodegenerative disorders. Front. Aging Neurosci. 2020, 12, 242. [Google Scholar] [CrossRef]
- Xie, X.; Yuan, P.; Kou, L.; Chen, X.; Li, J.; Li, Y. Nilotinib in Parkinson’s disease: A systematic review and meta-analysis. Front. Aging Neurosci. 2022, 14, 996217. [Google Scholar] [CrossRef]
- Ancidoni, A.; Bacigalupo, I.; Remoli, G.; Lacorte, E.; Piscopo, P.; Sarti, G.; Corbo, M.; Vanacore, N.; Canevelli, M. Anticancer drugs repurposed for Alzheimer’s disease: A systematic review. Alzheimers Res. Ther. 2021, 13, 96. [Google Scholar]
- Hebron, M.L.; Lonskaya, I.; Moussa, C. E-H. Nilotinib reverses loss of dopamine neurons and improves motor behavior via autophagic degradation of α-synuclein in Parkinson’s disease models. Hum. Mol. Genet. 2013, 22, 3315–3328. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- La Barbera, L.; Vedele, F.; Nobili, A.; Krashia, P.; Spoleti, E.; Latagliata, E.C.; Cutuli, D.; Cauzzi, E.; Marino, R.; Viscomi, M.T.; et al. Nilotinib restores memory function by preventing dopaminergic neuron degeneration in a mouse model of Alzheimer’s Disease. Prog. Neurobiol. 2021, 202, 102031. [Google Scholar] [CrossRef] [PubMed]
- Lonskaya, I.; Hebron, M.L.; Desforges, N.M.; Schachter, J.B.; Moussa, C.E.-H. Nilotinib-induced autophagic changes increase endogenous parkin level and ubiquitination, leading to amyloid clearance. J. Mol. Med. 2014, 92, 373–386. [Google Scholar] [CrossRef] [PubMed]
- Jones, H.K.; Stafford, L.E.; Swaisland, H.C.; Payne, R. A sensitive assay for ZD1839 (Iressa) in human plasma by liquid-liquid extraction and high performance liquid chromatography with mass spectrometric detection: Validation and use in Phase I clinical trial. J. Pharm. Biomed. Anal. 2002, 29, 221–228. [Google Scholar] [CrossRef] [PubMed]
- Bakhtiar, R.; Lohne, J.; Ramos, L.; Khelmani, L.; Hayes, M.; Tse, F. High-throughput quantification of the anti-leukemia drug STI571 (Gleevec) and its main metabolite (CGP 74588) in human plasma using liquid chromatography-tandem mass spectrometry. J. Chromatogr. B Analyt Technol. Biomed. Life Sci. 2002, 768, 325–340. [Google Scholar] [CrossRef]
- Zhao, M.; He, P.; Rudek, M.A.; Hidalgo, M.; Baker, S.D. Specific method for determination of OSI-774 and its metabolite OSI-420 in human plasma by using liquid chromatography-tandem mass spectrometry. J. Chromatogr. B 2003, 793, 413–420. [Google Scholar] [CrossRef]
- Hayashi, H.; Kita, Y.; Iihara, H.; Yanase, K.; Ohno, Y.; Hirose, C.; Yamada, M.; Todoroki, K.; Kitaichi, K.; Minatoguchi, S.; et al. Simultaneous and rapid determination of gefitinib, erlotinib and afatinib plasma levels using liquid chromatography/tandem mass spectrometry in patients with non-small-cell lung cancer. Biomed. Chromatogr. 2016, 30, 1150–1154. [Google Scholar] [CrossRef]
- Bao, X.; Wu, J.; Sanai, N.; Li, J. A liquid chromatography with tandem mass spectrometry method for quantitating total and unbound ceritinib in patient plasma and brain tumor. J. Pharm. Biomed. Anal. 2018, 8, 20–26. [Google Scholar] [CrossRef]
- Roberts, M.S.; Turner, D.C.; Broniscer, A.; Stewart, C.F. Determination of crizotinib in human and mouse plasma by liquid chromatography electrospray ionization tandem mass spectrometry (LC-ESI-MS/MS). J. Chromatogr. B 2014, 960, 151–157. [Google Scholar] [CrossRef] [Green Version]
- Cardoso, E.; Mercier, T.; Wagner, A.D.; Homicsko, K.; Michielin, O.; Ellefsen-Lavoie, K.; Cagnon, L.; Diezi, M.; Buclin, T.; Widmer, N. Quantification of the next-generation oral anti-tumor drugs dabrafenib, trametinib, vemurafenib, cobimetinib, pazopanib, regorafenib and two metabolites in human plasma by liquid chromatography-tandem mass spectrometry. J. Chromatogr. B Analyt. Technol. Biomed. Life Sci. 2018, 1083, 124–136. [Google Scholar] [CrossRef]
- De Francia, S.; D’Avolio, A.; De Martino, F.; Pirro, E.; Baietto, L.; Siccardi, M.; Simiele, M.; Racca, S.; Saglio, G.; Di Carlo, F.; et al. New HPLC-MS method for the simultaneous quantification of the antileukemia drugs imatinib, dasatinib, and nilotonib in human plasma. J. Chromatogr. B 2009, 877, 1721–1726. [Google Scholar] [CrossRef] [PubMed]
- Masters, A.R.; Sweeney, C.J.; Jones, D.R. The quantification of erlotinib (OSI-774) and OSI-420 in human plasma by liquid chromatography-tandem mass spectrometry. J. Chromatogr. B 2007, 848, 379–383. [Google Scholar] [CrossRef] [PubMed]
- Thappali, S.R.S.; Varanasi, K.; Veeraraghavan, S.; Arla, R.; Chennupati, S.; Rajamanickam, M.; Vakkalanka, S.; Khagga, M. Simultaneous determination of celecoxib, erlotinib, and its metabolite desmethyl-erlotinib (OSI-420) in rat plasma by liquid chromatography/tandem mass spectrometry with positive/negative ion-switching electrospray ionisation. Sci. Pharm. 2012, 80, 633–646. [Google Scholar] [CrossRef] [Green Version]
- Lepper, E.R.; Swain, S.M.; Tan, A.R.; Figg, W.D.; Sparreboom, A. Liquid-chromatographic determination of erlotinib (OSI-774), an epidermal growth factor receptor tyrosine kinase inhibitor. J. Chromatogr. B 2003, 796, 181–188. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Siu, L.L.; Moore, M.J.; Chen, E.X. Simultaneous determination of OSI-774 and its major metabolite OSI-420 in human plasma by using HPLC with UV detection. J. Chromatogr. B Analyt Technol. Biomed. Life Sci. 2005, 814, 143–147. [Google Scholar] [CrossRef]
- Chromsystems Instruments and Chemicals G.m.b.H.: Chromsystems Instruction Manual for LC-MS/MS Analysis. MassTox Immunosuppressants in Whole Blood OneMinute Test for Automated Sample Preparation on Hamilton MassSTAR; Order No. 93900/1200/DWP. V1.0; Chromsystems Instruments and Chemicals G.m.b.H.: Gräfelfing, Germany, 2020.
- Verheijen, R.B.; Atrafi, F.; Schellens, J.H.M.; Beijnen, J.H.; Huitema, A.D.R.; Mathijsen, R.H.J.; Steeghs, N. Pharmacokinetic optimization of everolimus dosing in oncology: A randomized crossover trial. Clin. Pharmacokinet. 2018, 57, 637–644. [Google Scholar] [CrossRef] [Green Version]
- McKillop, D.; Partridge, E.A.; Hitchison, M.; Rhead, S.A.; Parry, A.C.; Bardsley, J.; Woodman, H.M.; Swaisland, H.C. Pharmacokinetics of gefitinib, an epidermal growth factor receptor tyrosine kinase inhibitor, in rat and dog. Xenobiotica 2004, 34, 901–915. [Google Scholar] [CrossRef]
- Fang, L.; Song, Y.; Weng, X.; Li, F.; Xu, Y.; Lin, N. Highly sensitive HPLC-DAD method for the assay of gefitinib in patient plasma and cerebrospinal fluid: Application to a blood-brain barrier penetration study. Biomed. Chromatogr. 2015, 29, 1937–1940. [Google Scholar] [CrossRef]
- Zhao, M.; Hartke, C.; Jimeno, A.; Li, J.; He, P.; Zabelina, Y.; Hidalgo, M.; Baker, S.D. Specific method for determination of gefitinib in human plasma, mouse -plasma and tissues using high performance liquid chromatography coupled to tandem mass spectrometry. J. Chromatogr. B 2005, 819, 73–80. [Google Scholar] [CrossRef]
- Yang, H.; Li, C.; Chen, Z.; Mou, H.; Gu, L. Determination of chidamide in rat plasma and cerebrospinal fluid. Regul. Toxicol. Pharmacol. 2018, 98, 24–30. [Google Scholar] [CrossRef]
- Parise, R.A.; Ramanathan, R.K.; Hayes, M.J.; Egorin, M.J. Liquid chromatographic-mass spectrometric assay for quantitation of imatinib and its main metabolite (CGP 74588) in plasma. J. Chromatogr. B 2003, 791, 39–44. [Google Scholar] [CrossRef] [PubMed]
- D’Avolio, A.; Simiele, M.; De Francia, S.; Ariaudo, A.; Baietto, L.; Cusato, J.; Fava, C.; Saglio, G.; Di Carlo, F.; Di Perri, G. HPLC-MS method for the simultaneous quantification of the antileukemia drugs imatinib, dasatinib and nilotinib in human peripheral blood mononuclear cell (PBMC). J. Pharm. Biomed. Anal. 2012, 59, 109–116. [Google Scholar] [CrossRef] [PubMed]
- Pursche, S.; Ottmann, O.G.; Ehninger, G.; Schleyer, E. High-performance liquid chromatography method with ultraviolet detection for the quantification of the BCR-ABL inhibitor nilotinib (AMN107) in plasma, urine, culture medium and cell preparations. J. Chromatogr. B 2007, 852, 208–216. [Google Scholar] [CrossRef] [PubMed]
- Andriamanana, I.; Gana, I.; Duretz, B.; Hulin, A. Simultaneous analysis of anticancer agents bortezomib, imatinib, nilotinib, dasatinib, erlotinib, lapatinib, sorafenib, sunitinib and vandetanib in human plasma using LC/MS/MS. J. Chromatogr. B. Analyt. Technol. Biomed. Life Sci. 2013, 926, 83–91. [Google Scholar] [CrossRef]
- Bao, X.; Wu, J.; Sanai, N.; Li, J. Determination of total and unbound ribociclib in human plasma and brain tumor tissues using liquid chromatography coupled with tandem mass spectrometry. J. Pharm. Biomed. Anal. 2019, 166, 197–204. [Google Scholar] [CrossRef]
- Kala, A.; Patel, Y.T.; Davis, A.; Stewart, C.F. Development and validation of LC-MS/MS methods for the measurement of ribociclib, a CDK4/6 inhibitor, in mouse plasma and Ringer’s solution and its application to a cerebral microdialysis study. J. Chromatogr. B 2017, 1057, 110–117. [Google Scholar] [CrossRef]
- Zhen, Y.; Thomas-Schoemann, A.; Sakji, L.; Boudou-Rouquette, P.; Dupin, N.; Mortier, L.; Vidal, M.; Goldwasser, F.; Blanchet, B. An HPLC-UV method for the simultaneous quantification of vemurafenib and erlotinib in plasma from cancer patients. J. Chromatogr. B Analyt Technol. Biomed. Life Sci. 2013, 28, 93–97. [Google Scholar] [CrossRef]
- Salem, A.H.; Hu, B.; Freise, K.J.; Agarwal, S.K.; Sidhu, D.S.; Wong, S.L. Evaluation of the pharmacokinetic interaction between venetoclax, a selective BCL-2 inhibitor, and warfarin in healthy volunteers. Clin. Drug Investig. 2017, 37, 303–309. [Google Scholar] [CrossRef]
- Ding, X.; Chou, B.; Graham, R.A.; Cheeti, S.; Percey, S.; Matassa, L.C.; Reuschel, S.A.; Meng, M.; Liu, S.; Voelker, T.; et al. Determination of GDC-0449, a small-molecule inhibitor of the Hedgehog signaling pathway, in human plasma by solid phase extraction-liquid chromatographic-tandem mass spectrometry. J. Chromatogr. B 2010, 878, 785–790. [Google Scholar] [CrossRef]
- Seidel, C.; Viehweger, C.; Kortmann, R.-D. Is there an indication for first-line radiotherapy in primary CNS lymphoma? Cancers 2021, 13, 2580. [Google Scholar] [CrossRef]
- Xu, K.; Huang, Y.; Yao, J.; He, X. Whole-brain radiotherapy and chemotherapy in the treatment of patients with breast cancer and brain metastases. Int. J. Clin. Exp. Med. 2021, 14, 1250–1257. [Google Scholar]
- Hart, E.; Odé, Z.; Derieppe, M.P.P.; Groenink, L.; Heymans, M.W.; Otten, R.; Lequin, M.H.; Janssens, G.O.R.; Hoving, E.W.; van Vuurden, D.G. Blood-brain barrier permeability following conventional photon radiotherapy—A systematic review and meta-analysis of clinical and preclinical studies. Clin. Transl. Radiat. Oncol. 2022, 35, 44–55. [Google Scholar] [CrossRef] [PubMed]
- Mantovani, C.; Gastino, A.; Cerrato, M.; Badellino, S.; Ricardi, U.; Levis, M. Brain metastases from non-small cell lung cancer: Current approaches and future directions. Front. Oncol. 2021, 11, 772789. [Google Scholar] [CrossRef] [PubMed]
- Toh, Y.L.; Pah, Y.Y.; Shwe, M.; Kanesvaran, R.; Toh, C.K.; Chan, A.; Ho, H.K. HPLC-MS/MS coupled with equilibrium dialysis method for quantification of free drug concentration of pazopanib in plasma. Heliyon 2020, 27, e03813. [Google Scholar] [CrossRef] [PubMed]
- Roy, K.S.; Nazdrajic, E.; Shimelis, O.I.; Ross, M.J.; Chen, Y.; Cramer, H.; Pawliszyn, J. Optimizing a high-throughtput solid-phase microextraction system to determine the plasma protein binding of drugs in human plasma. Anal. Chem. 2021, 93, 11061–11065. [Google Scholar] [CrossRef] [PubMed]
- Mamada, H.; Iwamoto, K.; Nomura, Y.; Uesawa, Y. Predicting blood-to-plasma concentration ratios of drugs from chemical structures and volumes of distribution in humans. Mol. Divers. 2021, 25, 1261–1270. [Google Scholar] [CrossRef]
- Cao, B.; Soerjomataram, I.; Bray, F. The burden and prevention of premature deaths from noncommunicable diseases, including cancer: A global perspective. In World Cancer Report: Cancer Research for Cancer Prevention; Wild, C.P., Weiderpass, E., Stewart, B.W., Eds.; International Agency for Research on Cancer, World Health Organization: Lyon, France, 2020; pp. 16–22. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| ATC Code | International Nonproprietary Name | Target Cellular Protein | Monitored Peripheral Fluid | Ref. |
|---|---|---|---|---|
| L01EA01 | Imatinib | BCR-ABL tyrosine kinase | CSF, breast milk, leukocytes, PBMC, semen | [12,13,14,15,16,17,18,19,20,21,22,23,24,25,26] |
| L01EA02 | Dasatinib | BCR-ABL tyrosine kinase | CSF | [12,27,28] |
| L01EA03 | Nilotinib | BCR-ABL tyrosine kinase | CSF, pleural fluid | [29,30,31,32,33,34,35,36] |
| L01EA05 | Ponatinib | BCR-ABL tyrosine kinase | CSF | [37] |
| L01EB01 | Gefitinib | Epidermal growth factor receptor tyrosine kinase | CSF, pleural fluid, peritoneal dialysis fluid | [38,39,40,41,42,43,44,45,46] |
| L01EB02 | Erlotinib | Epidermal growth factor receptor tyrosine kinase | CSF, pleural fluid | [45,46,47,48,49,50,51,52,53,54,55,56,57,58] |
| L01EB03 | Afatinib | Epidermal growth factor receptor tyrosine kinase | CSF | [59,60,61] |
| L01EB04 | Osimertinib | Epidermal growth factor receptor tyrosine kinase | CSF | [62,63,64,65] |
| L01EB08 | Icotinib | Epidermal growth factor receptor tyrosine kinase | CSF | [66,67] |
| L01EC01 | Vemurafenib | B-raf serine-threonine kinase | CSF | [68] |
| L01EC02 | Dabrafenib | B-raf serine-threonine kinase | CSF | [69] |
| L01ED01 | Crizotinib | Anaplastic lymphoma kinase | CSF | [70,71,72,73] |
| L01ED02 | Ceritinib | Anaplastic lymphoma kinase | CSF | [74] |
| L01ED03 | Alectinib | Anaplastic lymphoma kinase | CSF | [75,76] |
| L01ED05 | Lorlatinib | Anaplastic lymphoma kinase | CSF | [77] |
| L01EE01 | Trametinib | Mitogen-activated protein kinase | CSF | [69] |
| L01EF02 | Ribociclib | Cycline dependent kinase | CSF | [12,78,79,80] |
| L01EG02 | Everolimus | Mammalian target of rapamycin | breast milk, saliva | [81,82] |
| L01EH01 | Lapatinib | Human epidermal growth factor receptor 2 tyrosine kinase | CSF | [83] |
| L01EH02 | Neratinib | Human epidermal growth factor receptor 2 tyrosine kinase | CSF | [84] |
| L01EL01 | Ibrutinib | Bruton’s tyrosine kinase | CSF | [85,86] |
| L01EL03 | Zanubrutinib | Bruton’s tyrosine kinase | CSF | [87] |
| L01EX01 | Sunitinib | Other protein kinase | Ascitic fluid | [88] |
| L01EX03 | Pazopanib | Other protein kinase | Ascitic fluid | [88] |
| L01EX05 | Regorafenib | Other protein kinase | CSF | [12,89] |
| L01EX09 | Nintedanib | Other protein kinase | CSF | [12] |
| L01EX21 | Tepotinib | Other protein kinase | CSF | [90,91] |
| L01EX23 | Pralsetinib | Other protein kinase | CSF | [65] |
| L01XH01 | Vorinostat | Histone deacetylase | CSF | [12] |
| L01XH03 | Panobinostat | Histone deacetylase | CSF | [12,92,93] |
| L01XJ01 | Vismodegib | Hedgehog pathway proteins | CSF | [94] |
| L01XX52 | Venetoclax | bcl-2 protein | CSF | [95,96] |
| First Author, Year | Drug | Type of Study | Patient Population | Number of Subjects Donating Samples for TDM | Period of Recruitment | Outcomes Measured | Ref. |
|---|---|---|---|---|---|---|---|
| Hoffknecht, 2015 | Afatinib | Case series | 2 adults with advanced NSCLC with brain metastasis or leptomeningeal disease | Blood: 2 PFS: 2 | May 2010 to December 2013 | Afatinib in CSF and in plasma | [59] |
| Kawaguchi, 2017 | Afatinib | Case report | Adult (female, 41 years) with stage IV lung adenocarcinoma and cerebral metastasis | Blood: 1 PFS: 1 | Not applicable | Afatinib in CSF and in plasma | [60] |
| Tamiya, 2017 | Afatinib | Registered clinical study (UMIN000014065) | 11 adults with histologically proven EGFR mutation-positive NSCLC with LMC | Blood: 11 PFS: 8 | April 2014 to November 2015 | Afatinib in CSF and in plasma | [61] |
| Gadgeel, 2014 | Alectinib | Registered clinical study (NCT01588028) | 47 adults with locally advanced or metastatic NSCLC with ALK gene rearrangement | Blood: 5 PFS: 5 | 3 May 2012 to 26 July 2013 | Alectinib in CSF and in plasma | [75] |
| Metro, 2016 | Alectinib | Case series | 11 ALK-positive NSCLC patients with CNS metastasis | Blood: 2 PFS sample: 2 | December 2013 to August 2015 | Alectinib in CSF and in serum | [76] |
| Mehta, 2021 | Ceritinib | Registered clinical study (NCT02605746) | 10 adults with glioblastoma necessitating resection | Blood: 10 PFS: 8 | Not reported | Ceritinib in CSF and in plasma | [74] |
| Costa, 2011 | Crizotinib | Case report | Adult (male, 29 years) with stage IV NSCLC and CNS metastasis | Blood: 1 PFS: 1 | Not applicable | Crizotinib in CSF and in plasma | [70] |
| Metro, 2015 | Crizotinib | Case series | 2 adults with ALK-positive advanced NSCLC and CNS metastasis | Blood: 2 PFS: 2 | Not applicable | Crizotinib in CSF and in plasma | [71] |
| Okawa, 2018 | Crizotinib | Case report | Adult (male, 60 years) with NSCLC and isolated CNS failure | Blood: 1 PFS: 1 | Not applicable | Crizotinib in CSF and in plasma | [72] |
| Okimoto, 2019 | Crizotinib | Case report | Adult (male, 61 years) with NSCLC and carcinomatous meningitis | Blood: 1 PFS: 1 | Not applicable | Crizotinib in CSF and in plasma | [73] |
| Hottinger, 2019 | Dabrafenib, trametinib | Case series | 2 adults with leptomeningeal tumor | Blood: 2 PFS: 2 | 2017 | Dabrafenib and trametinib in CSF and in plasma | [69] |
| Guntner, 2020 | Dasatinib, imatinib, nintedanib, panobinostat, regorafenib, ribociclib, vorinostat | Case series | 12 pediatric patients (ages: 7.5–20.3) with primary and secondary malignant brain tumors | Blood: 1 PFS: 9 | Not reported | Imatinib, dasatinib, nintedanib, panobinostat, regorafenib, ribociclib and vorinostat in CSF | [12] |
| Kondo, 2014 | Dasatinib | Case report | Adult (female, 58 years) with Ph + ALL and meningeal leukemia | Blood: 1 PFS: 1 | Not applicable | Dasatinib in CSF and in plasma | [27] |
| Gong, 2021 | Dasatinib | Registered clinical study (NCT02523976) | 31 adults with newly diagnosed Ph + ALL | Blood: 31 PFS: 31 | January 2016 to April 2018 | Dasatinib in CSF and in plasma | [28] |
| Shriyan, 2020 | Erlotinib, gefitinib | Non-registered, researcher-initiated study | 20 adults with NSCLC and brain metastasis | Blood: 20 PFS: 20 | August 2014 to July 2017 | Erlotinib in CSF and in plasma, gefitinib in CSF and in plasma | [46] |
| Broniscer, 2007 | Erlotinib | Case report | Pediatric patient (female, 8 years) with glioblastoma | Blood: 1 PFS: 1 | Not applicable | Erlotinib in CSF and in plasma | [47] |
| Rogers, 2010 | Erlotinib | Case report | Adult (female, 33 years) with CNS hemangioblastomatosis associated with von Hippel-Lindau disease | Blood: 1 PFS: 1 | Not reported | Erlotinib in CSF and in plasma | [48] |
| Masago, 2011 | Erlotinib | Non-registered, researcher-initiated study | 9 adult patients with advanced NSCLC | Blood: 9 PFS: 9 | June 2009 to December 2009 | Erlotinib and OSI-420 in pleural effusate and in plasma | [49] |
| Masuda, 2011 | Erlotinib | Case series | 3 adults (NSCLC with LM) | Blood: 3 PFS: 3 | Not applicable | Erlotinib in CSF and in plasma | [50] |
| Togashi, 2010 | Erlotinib | Case series | 4 adults with NSCLC and CNS metastasis | Blood: 4 PFS: 4 | Not reported | Erlotinib in CSF and in plasma | [51] |
| Deng, 2013 | Erlotinib | Non-registered, researcher-initiated study | 6 adults (NSCLC) | Blood: 6 PFS: 6 | March 2011 to March 2012 | Erlotinib in CSF and in plasma | [52] |
| Sakata, 2016 | Erlotinib | Case report | Adult (female, 54 years) with NSCLC and LM | Blood: 1 PFS: 1 | Not applicable | Erlotinib in CSF and in plasma | [53] |
| Clarke, 2010 | Erlotinib | Case report | Adult (female, 54 years) with stage IV NSCLC and LM | Blood: 1 PFS: 1 | Not applicable | Erlotinib in CSF and in plasma | [54] |
| Yang, 2015 | Erlotinib | Retrospective observational study | 9 adults with lung adenocarcinoma and refractory CNS metastases | Blood: 6 PFS: 6 | January 2011 to June 2013 | Erlotinib in CSF and in plasma | [55] |
| Togashi, 2011 | Erlotinib | Case series | 9 adults with NSCLC and CNS metastasis | Blood: 9 PFS: 9 | Not reported | Erlotinib in CSF and in plasma | [56] |
| Fukudo, 2013 | Erlotinib | Non-registered, researcher-initiated study | 88 adults with NSCLC | Blood: 88 PFS: 23 | June 2009 to March 2012 | Erlotinib in CSF and in plasma | [57] |
| Nosaki, 2020 | Erlotinib | Registered clinical study (UMIN000007020) | 21 adults (stage IV NSCLC or its recurrence with LM) | Blood: 14 PFS: 12 | December 2011 to May 2015 | Erlotinib in CSF and in plasma | [58] |
| DeWire, 2021 | Everolimus, ribociclib | Registered clinical study (NCT03387020) | 22 pediatric patients (ages: 3.9–20.4) with a recurrent, progressive or refractory brain tumor | Blood: 22 PFS: 5 | January 2018 to April 2020 | Ribociclib in CSF and in plasma, everolimus in blood | [80] |
| Fiocchi, 2016 | Everolimus | Case report | Adult (female, 40 years) with pregnancy after undergoing heart transplant | Blood: 1 PFS: 1 | Not applicable | Everolimus in breast milk (colostrum) and in plasma | [81] |
| Molenaar-Kuijsten, 2022 | Everolimus | Registered clinical study (EudraCT 2014-004,833-25; NTR4908) | 10 adults with stomatitis | Blood: 10 PFS: 10 | Not reported | Everolimus in saliva and in plasma | [82] |
| Yamaguchi, 2015 | Gefitinib | Case report | Adult (male, 72 years) lung adenocarcinoma and brain metastasis | Blood: 1 PFS: 1 | Not applicable | Gefitinib in pleural effusate, peritoneal effusate dialysate, and plasma | [38] |
| Fukuhara, 2008 | Gefitinib | Case report | Adult (male, 62 years) with stage IV lung cancer and carcinomatous meningitis | Blood: 1 PFS: 1 | Not applicable | Gefitinib in CSF and in plasma | [39] |
| Zhao, 2013 | Gefitinib | Non-registered, researcher-initiated study | 22 adults (NSCLC) | Blood: 22 PFS: 22 | March 2007 to December 2010 | Gefitinib in CSF and in plasma | [40] |
| Zeng, 2015 | Gefitinib | Non-registered, researcher-initiated study | 28 adults with NSCLC and brain metastasis | Blood: 28 PFS: 28 | October 2009 to March 2011 | Gefitinib in CSF and in plasma | [41] |
| Zhao, 2016 | Gefitinib | Case series | 7 adults with NSCLC with intracranial and/or extracranial progression | Blood: 5 PFS: 5 | February 2009 to May 2013 | Gefitinib in CSF and in plasma | [42] |
| Jackman, 2015 | Gefitinib | Registered clinical study (NCT00372515) | 7 adults with NSCLC and LM | Blood: 7 PFS: 7 | May 2006 and July 2008 | Gefitinib in CSF and in plasma | [43] |
| Fang, 2015 | Gefitinib | Case series | 3 adults with lung adenocarcinoma and brain metastasis | Blood: 3 PFS: 3 | Not reported | Gefitinib in CSF and in plasma | [44] |
| Togashi, 2012 | Gefitinib, erlotinib | Non-registered, researcher-initiated study | 15 adults (NSCLC with CNS metastases with EGFR mutations) | Gefitinib: Blood: 8 PFS: 8 Erlotinib: Blood: 9 PFS: 9 | April 2010 to March 2012 |
| [45] |
| Law, 2021 | Ibrutinib | Case series | 2 adults with Epstein–Barr virus-associated primary CNS lymphoma | Blood: 1 PFS: 1 | Not applicable | Ibritunib in CSF and in plasma | [85] |
| Yu, 2021 | Ibrutinib | Retrospective observational study | 3 adults with primary central nervouos system lymphoma | Blood: 3 PFS: 1 | August 2017 to May 2020 | Ibrutinib in CSF and in plasma | [86] |
| Fan, 2015 | Icotinib | Registered clinical study (NCT01514877) | 20 adults with NSCLC and brain metastasis | Blood: 10 PFS: 10 | February 2012 to March 2013 | Icotinib in CSF and in plasma | [66] |
| Zhou, 2016 | Icotinib | Registered clinical study (NCT01516983) | 15 adults with NSCLC and brain metastasis | Blood: 15 PFS: 13 | 13 February 2012 to 24 July 2013 | Icotinib in CSF and in plasma | [67] |
| Nambu, 2011 | Imatinib | Non-registered, researcher-initiated study | 15 adults with CML | Blood: 15 PFS: 15 | 2003 to 2008 | Imatinib in leukocytes and in plasma | [13] |
| De Francia, 2014 | Imatinib | Non-registered, researcher-initiated study | 24 adults with Ph + CML | Blood: 24 PFS: 24 | Not reported | Imatinib in PBMC’s and in plasma | [14] |
| Petzer, 2002 | Imatinib | Case report | Adult (male, 52 years) with CML with CNS relapse | Blood: 1 PFS: 1 | Not applicable | Imatinib in CSF and in plasma | [15] |
| Takayama, 2002 | Imatinib | Case report | Adult (female, 32 years) with Ph + ALL and CNS leukemia | Blood: 1 PFS: 1 | Not applicable | Imatinib in CSF and in plasma | [16] |
| Bornhauser, 2004 | Imatinib | Case report | Adult (female, 56 years) with Ph + CML and CNS leukemia | Blood: 1 PFS: 1 | Not applicable | Imatinib and N-desmethyl imatinib in CSF and in plasma | [17] |
| le Coutre, 2004 | Imatinib | Non-registered, researcher-initiated study | 97 subjects with BCR/ABL + CML or BCR/ABL + ALL | Blood: 97 PFS: 17 | Not reported | Imatinib and N-desmethyl imatinib in CSF and in plasma | [18] |
| Leis, 2004 | Imatinib | Registered clinical study (CSTI5710102, CSTI15710109 | 42 adults with CML in blast crisis, or Ph + ALL | Blood: 4 PFS: 4 | Not reported | Imatinib in CSF and in plasma | [19] |
| Russell, 2007 | Imatinib | Case series | 2 adults with Ph + CML | Blood: 1 PFS: 1 | Not applicable | Imatinib in breast milk and in plasma | [20] |
| Gambacorti-Passerini, 2007 | Imatinib | Case report | Adult (female, 40 years) with CML | Blood: 1 PFS: 1 | Not applicable | Imatinib in breast milk and in plasma | [21] |
| Ali, 2009 | Imatinib | Case report | Adult (female, 27 years) with Ph + CML | Blood: 1 PFS: 1 | Not applicable | Imatinib in breast milk and in plasma | [22] |
| Kronenberger, 2009 | Imatinib | Case report | Adult (female, 34 years) with CML | Blood: 1 PFS: 1 | Not applicable | Imatinib in breast milk and in plasma | [23] |
| Burwick, 2017 | Imatinib | Case report | Adult (female, 29 years) with Ph + CML | Blood: 1 PFS: 1 | Not applicable | Imatinib in breast milk and in plasma | [24] |
| Terao, 2020 | Imatinib | Case report | Adult (female, 32 years) with Ph + CML | Blood: 1 PFS: 1 | Not applicable | Imatinib in breast milk and in plasma | [25] |
| Chang, 2017 | Imatinib | Non-registered, researcher-initiated study | 108 males (15–51 years) with CML-CP, infertility, or controls | Blood: 48 PFS: 11 | January 2010 to December 2014 | Imatinib in semen and in plasma | [26] |
| Gori, 2014 | Lapatinib | Case series | 2 adults with HER2 + metastatic breast cancer | Blood: 2 PFS: 2 | Not applicable | Lapatinib in CSF and in plasma | [83] |
| Sun, 2022 | Lorlatinib | Registered clinical study (NCT01970865) | 54 patients with NSCLC and suspected or confirmed leptomeningeal carcinomatosis or carcinomatous meningitis | Blood: 54 PFS: 5 | Not reported | Lorlatinib in CSF and in plasma | [77] |
| Freedman, 2020 | Neratinib | Registered clinical study (NCT01494662) | 5 adults with HER2 + breast cancer and brain metastases in whom craniotomy was indicated | Blood: 2 PFS: 3 | 22 May 2013 to 18 October 2016 | Neratinib in CSF and in plasma | [84] |
| Reinwald, 2014 | Nilotinib | Case series | 4 patients aged > 15 years with BCR-ABL + ALL or CML-BC | Blood: 4 PFS: 4 | Not reported | Nilotinib in CSF and in plasma | [29] |
| Liu, 2019 | Nilotinib | Registered clinical study (ChiCTR-ONC-12002469) | 30 subjects aged > 15 years with newly diagnosed Ph + ALL | Blood: 30 PFS: 30 | 14 September 2011 to 21 November 2013 | Nilotinib in CSF and in plasma | [30] |
| Satoh, 2021 | Nilotinib | Case report | Adult (male, 23 years) with CML | Blood: 1 PFS: 1 | Not applicable | Nilotinib in pleural effusate and in plasma | [31] |
| Pagan, 2016 | Nilotinib | Registered clinical study (NCT02281474) | 12 adults with Parkinson’s disease or Dementia with Lewy Bodies | Blood: 12 PFS: 12 | Not reported | Nilotinib in CSF and in plasma | [32] |
| Pagan, 2019 | Nilotinib | Registered clinical study (NCT02954978) | 75 adults with Parkinson’s disease | Blood: 75 PFS: 75 | Not reported | Nilotinib in CSF and in plasma | [33] |
| Pagan, 2020 | Nilotinib | Registered clinical study(NCT02954978) | 75 adults with Parkinson’s disease | Blood: 75 PFS: 75 | 17 May 2017 to 28 April 2018 | Nilotinib in CSF and in plasma | [34] |
| Simuni, 2021 | Nilotinib | Registered clinical study (NCT03205488) | 76 adults with Parkinson’s disease | Blood: 41 PFS: 42 | November 2017 to December 2018 | Nilotinib in CSF and in plasma | [35] |
| Turner, 2020 | Nilotinib | Registered clinical study (NCT02947893) | 37 adults with Alzheimer’s disease | Blood: 37 PFS: 37 | Not reported | Nilotinib in CSF and in plasma | [36] |
| Song, 2019 | Osimertinib | Case report | Adult with NSCLC and LM | Blood: 1 PFS: 1 | Not applicable | Osimertinib in CSF and in plasma | [62] |
| Xing, 2020 | Osimertinib | Registered clinical study (NCT02972333) | 38 adults with refractory NSCLC and CNS metastasis | Blood: 12 PFS: 12 | January 2017 to September 2017 | Osimertinib in CSF and in plasma | [63] |
| Yamaguchi, 2021 | Osimertinib | Registered clinical study (UMIN000024218, jRCTs071180017) | 40 adults with confirmed NSCLC and CNS metastasis | Blood: 37 PFS: 7 | 27 December 2016 to 4 July 2019 | Osimertinib in CSF and in plasma | [64] |
| Rasmussen, 2015 | Panobinobstat | Registered clinical study (NCT01680094) | 15 adults with HIV infection | Blood: 0 PFS: 11 | September 2012 to February 2014 | Panobinostat in CSF | [92] |
| Goldberg, 2020 | Panobinostat | Registered clinical study (NCT01321346) | 22 pediatric patients with relapsed or refractory acute leukemia or lymphoma | Blood: 9 PFS: not reported | 3 November 2011 to 31 July 2015 | Panobinostat in CSF and in plasma | [93] |
| Krens, 2021 | Pazopanib | Case report | Adult (male, 79 years) with metastatic papillary renal cell carcinaoma and malignant ascites | Blood: 1 PFS: 1 | Not applicable | Pazopanib in ascitic fluid and in plasma | [88] |
| Tanimura, 2021 | Ponatinib | Case report | Pediatric patient (girl, 3 years) with Ph + ALL and CNS infiltration | Blood: 1 PFS: 1 | Not applicable | Ponatinib in CSF and in plasma | [37] |
| Zhao, 2022 | Pralsetinib | Case report | Adult (female, 43 years) with lung cancer and meningeal metastases | Blood: 1 PFS: 1 | Not applicable | Pralsetinib in CSF and in plasma | [65] |
| Zeiner, 2019 | Regorafenib | Retrospective observational study | 21 adults with recurrent malignant glioma | Blood: 3 PFS: 3 | August 2018 to July 2019 | Regorafenib in CSF and in serum | [89] |
| Miller, 2019 | Ribociclib | Registered clinical tudy (NCT02345824, IND125168) | 3 adults with recurrent glioblastoma | Blood: 3 PFS: 1 | First surgery dates: 29 March 2012 to 26 September 2014 | Ribociclib in CSF and in plasma | [78] |
| Tien, 2019 | Ribociclib | Registered clinical study (NCT02933736) | 12 adults with a recurrent glioblastoma | Blood: 12 PFS: 12 | Not reported | Ribociclib in CSF and in plasma | [79] |
| Tanaka, 2020 | Tepotinib | Case report | Adult (male, 56 years) with with lung adenocarcinoma and LM | Blood: 1 PFS: 1 | Not applicable | Tepotinib in CSF and in plasma | [90] |
| Ninomaru, 2021 | Tepotinib | Case report | Adult (female, 77 years) with NSCLC and LM | Blood: 1 PFS: 1 | Not applicable | Tepotinib in CSF and in plasma | [91] |
| Sakji-Dupré, 2015 | Vemurafenib | Case series | 6 adults with melanoma and brain metastasis | Blood: 6 PFS: 6 | February 2012 to January 2013 | Vemurafenib in CSF and in plasma | [68] |
| Reda, 2019 | Venetoclax | Case report | Adult (male, 58 years) with trisomy 12, IGHV unmutated (VH4L) chronic lymphocytic leukemia | Blood: 1 PFS: 1 | Not applicable | Venetoclax in CSF and in plasma | [95] |
| Condorelli, 2022 | Venetoclax | Case report | Adult (male, 52 years) with AML and CNS leukemia | Blood: 1 PFS: 1 | Not applicable | Venetoclax in CSF and in plasma | [96] |
| Gajjar, 2013 | Vismodegib | Registered clinical study (NCT0082248) | 33 pediatric patients (ages: 3.9–21 yeatrs) with recurrent, progressive or refractory medulloblastoma | Blood: 33 PFS: 3 | Not reported | Vismodegib in CSF and in plasma | [94] |
| Zhang, 2021 | Zanubrutinib | Case series | 13 adults with diffuse large B-cell lymphoma and CNS involvement | Blood: 13 PFS: 13 | August 2020 to December 2020 | Zanubrutinib in CSF and in plasma | [87] |
| International Non-Proprietary Name | Peripheral Compartment | Indication of Monitoring | Pathological Condition | Ref. |
|---|---|---|---|---|
| Afatinib | CSF | Secondary malignancy | NSCLC with CNS metastasis and/or leptomeningeal disease | [59] |
| CSF | Secondary malignancy | NSCLC with leptomeningeal carcinomatosis | [60] | |
| CSF | Secondary malignancy | NSCLC with leptomeningeal carcinomatosis | [61] | |
| Alectinib | CSF | Secondary malignancy | NSCLC with CNS metastasis and systemic disease | [75] |
| CSF | Secondary malignancy | NSCLC with CNS metastasis | [76] | |
| Ceritinib | CSF | Secondary malignancy | CNS metastasis of breast tumor, head and neck tumor or melanoma, recurrent glioblastoma | [74] |
| Crizotinib | CSF | Secondary malignancy | NSCLC with leptomeningeal metastasis | [70] |
| CSF | Secondary malignancy | NSCLC with CNS metastasis | [71] | |
| CSF | Secondary malignancy | NSCLC with CNS metastasis | [72] | |
| CSF | Secondary malignancy | NSCLC with carcinomatous meningitis | [73] | |
| Dabrafenib | CSF | Primary malignancy | Glioma | [69] |
| Dasatinib | CSF | Primary malignancy | CNS tumor | [12] |
| CSF | Secondary malignancy | AML with extramedullary and meningeal relapse | [27] | |
| CSF | Secondary malignancy | ALL and CNS leukemia prophylaxis | [28] | |
| Erlotinib | CSF | Secondary malignancy | NSCLC with CNS metastasis | [45] |
| CSF | Secondary malignancy | NSCLC with CNS metastasis | [46] | |
| CSF | Primary malignancy | Glioblastoma | [47] | |
| CSF | Primary malignancy | CNS hemangioblastoma with von Hippel-Lindau disease | [48] | |
| CSF | Secondary malignancy | NSCLC with leptomeningeal metastasis | [50] | |
| CSF | Secondary malignancy | NSCLC with CNS metastasis | [51] | |
| CSF | Secondary malignancy | NSCLC with CNS metastasis | [52] | |
| CSF | Secondary malignancy | NSCLC with leptomeningeal metastasis | [53] | |
| CSF | Secondary malignancy | NSCLC with leptomeningeal meatastasis | [54] | |
| CSF | Secondary malignancy | NSCLC with refractory CNS metastasis | [55] | |
| CSF | Secondary malignancy | NSCLC with CNS metastasis | [56] | |
| CSF | Secondary malignancy | NSCLC with CNS metastasis | [57] | |
| CSF | Secondary malignancy | NSCLC with leptomeningeal metastasis | [58] | |
| Pleural effusate | Primary malignancy | NSCLC | [49] | |
| Everolimus | Breastmilk | Risk of toxicity | Pregnancy in everolimus-treated heart-transplanted patient | [81] |
| Saliva | Risk of toxicity | Cancer patients (breast, renal cell, neuroendocrine tumors) | [82] | |
| Gefitinib | CSF | Secondary malignancy | NSCLC with carcinomatous meningitis | [39] |
| CSF | Secondary malignancy | NSCLC with lung adenocarcinoma | [40] | |
| CSF | Secondary malignancy | NSCLC with CNS metastasis | [41] | |
| CSF | Secondary malignancy | NSCLC with leptomeningeal metastasis | [42] | |
| CSF | Secondary malignancy | NSCLC with leptomeningeal metastasis | [43] | |
| CSF | Secondary malignancy | NSCLC with CNS metastasis | [44] | |
| CSF | Secondary malignancy | NSCLC with CNS metastasis | [45] | |
| CSF | Secondary malignancy | NSCLC with CNS metastasis | [46] | |
| Pleural effusate, peritoneal effusate dialysate | Primary malignancy | NSCLC | [38] | |
| Ibrutinib | CSF | Primary malignancy | Epstein–Barr associated primary CNS lymphoma | [85] |
| CSF | Primary malignancy | PCNSL | [86] | |
| Icotinib | CSF | Secondary malignancy | NSCLC with CNS metastasis | [44] |
| CSF | Secondary malignancy | NSCLC with CNS metastatis | [67] | |
| Imatinib | Breast milk | Risk of toxicity | CML during pregnancy | [20] |
| Breast milk | Risk of toxicity | CML during pregnancy | [21] | |
| Breast milk | Risk of toxicity | CML during pregnancy and breastfeeding | [22] | |
| Breast milk | Risk of toxicitiy | CML during pregnancy and breastfeeding | [23] | |
| Breast milk | Risk of toxicity | CML in early pregnancy and breastfeedng | [24] | |
| Breast milk | Risk of toxicity | CML during pregnancy and breastfeeding | [25] | |
| CSF | Primary malignancy | CNS tumor | [12] | |
| CSF | Secondary malignancy | CML with lymphoid blast crisis | [15] | |
| CSF | Secondary malignancy | ALL with CNS leukemia | [16] | |
| CSF | Secondary malignancy | CML with CNS leukemia | [17] | |
| CSF | Secondary malignancy | CML and ALL with meningeous leukemia | [18] | |
| CSF | Secondary malignancy | CML with lymphoid blast crisis and AML | [19] | |
| Leukocytes | Primary malignancy | CML | [13] | |
| PBMC’s | Primary malignancy | CML | [14] | |
| Semen | Risk of toxicity | CML | [26] | |
| Lapatinib | CSF | Secondary malignancy | Breast cancer with CNS metastasis | [83] |
| Lorlatinib | CSF | Secondary malignancy | NSCLC with CNS metastasis | [77] |
| Neratinib | CSF | Secondary malignancy | Breast cancer with CNS metastasis | [84] |
| Nilotinib | CSF | Secondary malignancy | Leukemia with CNS infiltration | [29] |
| CSF | Secondary malignancy | ALL and CNS leukemia prophylaxis | [30] | |
| CSF | Treatment of a mental disorder | Parkinson’s disease, dementia | [32] | |
| CSF | Treatment of a mental disorder | Parkinson’s disease | [33] | |
| CSF | Treatment of a mental disorder | Parkinson’s disease | [34] | |
| CSF | Treatment of a mental disorder | Parkinson’s disease | [35] | |
| CSF | Treatment of a mental disorder | Alzheimer’s disease | [36] | |
| Pleural effusate | Risk of toxicity | CML | [31] | |
| Nintedanib | CSF | Primary malignancy | CNS tumor | [12] |
| Osimertinib | CSF | Secondary malignancy | NSCLC with leptomeningeal metastasis | [62] |
| CSF | Secondary malignancy | NSCLC wth CNS metastasis | [63] | |
| CSF | Secondary malignancy | NSCLC with CNS metastasis | [64] | |
| CSF | Secondary malignancy | NSCLC with meningeal metastasis | [65] | |
| Panobinostat | CSF | Primary malignancy | CNS tumor | [12] |
| CSF | Risk of toxicity | HIV infection | [92] | |
| CSF | Risk of toxicity | Recurrent or refractory haematologic malignancies (leukemia and lymphoma) | [93] | |
| Pazopanib | Ascitic fluid | Secondary malignancy | Metastatic papillary renal cell carcinoma and malignant ascites | [88] |
| Ponatinib | CSF | Secondary malignancy | ALL with CNS leukemia | [37] |
| Pralsetinib | CSF | Secondary malignancy | NSCLC with meningeal metastasis | [65] |
| Regorafenib | CSF | Primary malignancy | CNS tumor | [12] |
| CSF | Primary malignancy | Recurrent malignant glioma | [89] | |
| Ribociclib | CSF | Primary malignancy | CNS tumor | [12] |
| CSF | Primary malignancy | Recurrent glioblastma | [78] | |
| CSF | Primary malignancy | Recurrent glioblastoma | [79] | |
| CSF | Primary malignancy | Recurrent or refractory malignant CNS tumor | [80] | |
| Sunitinib | Ascitic fluid | Secondary malignancy | Metastatic papillary renal cell carcinoma and malignant ascites | [88] |
| Tepotinib | CSF | Secondary malignancy | NSCLC with leptomeningeal metastasis | [90] |
| CSF | Secondary malignancy | NSCLC with leptomeningeal metastasis | [91] | |
| Trametinib | CSF | Primary malignancy | Glioma | [69] |
| Vemurafenib | CSF | Secondary malignancy | Melanoma with CNS metastasis | [68] |
| Venetoclax | CSF | Secondary malignancy | CLL with CNS involvement | [95] |
| CSF | Secondary malignancy | AML with leptomeningeal involvement | [96] | |
| Vismodegib | CSF | Primary malignancy | Recurrent or refractory medulloblastoma | [94] |
| Vorinostat | CSF | Primary malignancy | CNS tumor | [12] |
| Zanubrutinib | CSF | Primary malignancy | CNS lymphoma | [87] |
| Drug | Matrix | Internal Standard | Chromatography | Mass Spectrometry | UV–VIS (nm) | Sample Preparation | Ref. | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Stationary Phase | Mobile Phases | Type of Separation | Ioniza-tion | Analyte ions | IS Ions | ||||||
| Afatinib | CSF | Isotope-labeled afatinib | Reversed phase | NS | Gradient | ESI (+) | NS | NS | Not used | None | [59] |
| Afatinib | CSF | Imatinib | XBridge Shield RP18 (50 × 2.1 mm, 3.5 µm) | Acetonitrile (10 mmol/L ammonium hydroxide), water (1 mmol/L ammonium hydroxide), pH = 10.5 | Isocratic (70:30) | ESI (+) | 486.0 > 371.3 | 494.1 > 394.4 | Not used | LLE | [60,117] |
| Afatinib | CSF | None | Inertsil ODS-2 (150 × 2.1 mm, 5 µm) | Water (0.1% ammonium acetate, pH = 8.5), acetonitrile, triethylamine | Isocratic (55:44:0.5) | Not applicable | 254 | SPE | [61] | ||
| Alectinib | CSF | Liquid chromatography–mass spectrometry was used. | [75] | ||||||||
| Alectinib | CSF | Liquid chromatography–tandem mass spectrometry was used. Sample preparation consisted of deprot. with methanol. | [76] | ||||||||
| Ceritinib | CSF | 13C6-ceritinib | Acquity UPLC BEH C18 (50 × 2.1 mm, 1.7 µm) | Water (0.1% FA), methanol (0.1% FA) | Gradient | ESI (+) | 558.0 > 433.0 | 564.3 > 438.9 | Not used | Deprot. | [74,118] |
| Crizotinib | CSF | Liquid chromatography-tandem mass spectrometry was used. | [70] | ||||||||
| Crizotinib | CSF | 2H5,13C2-crizotinib | Discovery C18 (50 × 2.1 mm, 5 µm) | Water (0.3% FA), methanol (0.3% FA) | Gradient | ESI (+) | 450.2 > 260.2 | 457.2 > 267.3 | Not used | SPE | [71,119] |
| Crizotinib | CSF | Liquid chromatography-tandem mass spectrometry was used. | [72] | ||||||||
| Crizotinib | CSF | No details of the employed analytical methodology are disclosed. | [73] | ||||||||
| Dabrafenib | CSF | 2H9-dabrafenib | XSelect HSS T3 (75 × 2.1 mm, 3.5 µm) | Water (2 mmol/L ammonium acetate, 0.1% FA), acetonitrile (0.1% FA) | Gradient | ESI (+) | 520.1 > 292.0 | 529.1 > 316.2 | Not used | Deprot. | [69,120] |
| Dasatinib | CSF | Carbamazepine | Nucleoshell C18 (150 × 3 mm, 2.7 µm) | Water (0.1% FA), methanol | Gradient | ESI (+) | 488.17 > 232.1 488.17 > 193.1 488.17 > 161.0 | 237.1 > 194.2 237.1 > 165.1 237.1 > 121.1 | Not used | Deprot. | [12] |
| Dasatinib | CSF | Quinoxaline | Atlantis C18 (150 × 4.6 mm, 5 µm) | Water (0.05% FA), acetonitrile (0.05% FA) | Gradient | ESI (+) | 487.5 | 313.0 | Not used | Deprot. | [27,121] |
| Dasatinib | CSF | 2H8-dasatinib | Shim-Pack XR-ODSII (50 × 2 mm, 2.2 µm) | Water (0.1% FA), acetonitrile (0.1% FA) | Gradient | ESI (+) | 488.0 > 401.0 | 496 > 406 | Not used | NS | [28] |
| Erlotinib | CSF | Midazolam | C18 Luna (150 × 4.6 mm, 5 µm) | Acetonitrile, 5 mmol/L ammonium acetate | Isocratic (45:55) | ESI (+) | 394.1 > 278.0 394.1 > 336.0 | 326.2 > 291.0 | Not used | LLE | [45,122] |
| Erlotinib | CSF | Desmethyl erlotinib | Zorbax C18 (150 × 3 mm, 1.8 µm) | Acetonitrile, water (15 mmol/L ammonium acetate) | Gradient | ESI (+) | 394.5 > 278.1 | 313.8 > 243.9 | Not used | Deprot. | [46,123] |
| Erlotinib | CSF | Midazolam | Xterra octadecylsilica (50 × 2.1 mm, 3.5 µm) | Acetonitrile (0.1% FA), water (0.1% FA) | Isocratic (70:30) | ESI (+) | 394 > 278 | 326 > 286.1 | Not used | Deprot. | [47,116] |
| Erlotinib | CSF | Liquid chromatography–tandem mass spectrometry were used. | [48] | ||||||||
| Erlotinib | CSF | OSI-597 | Nova-Pak C18 (150 × 3.9 mm, 4 µm) | Acetonitrile, water (pH = 2.0) | Isocratic (60:40) | Not applicable | 348 | LLE | [50,124] | ||
| Erlotinib | CSF | None | Symmetry C18 (150 × 4.6 mm, 5 µm) | Acetonitrile, 0.05 mol/L aqueous potassium phosphate (0.2% triethylamine, pH = 4.8) | Isocratic (42:58) | Not applicable | 345 | LLE | [51,52,56,57,125] | ||
| Erlotinib | CSF | High-performance liquid chromatography was used. | [53] | ||||||||
| Erlotinib | CSF | Deprot. with methanol-acetonitrile 1:4, v/v%. Liquid chromatography-tandem mass spectrometry was used. | [54] | ||||||||
| Erlotinib | CSF | Liquid chromatography–tandem mass spectrometry was used. | [55] | ||||||||
| Erlotinib | CSF | Liquid–liquid extraction and high-performance liquid chromatography with mass spectrometric detection was used. | [58] | ||||||||
| Erlotinib | pleural effusate | None | Symmetry C18 (150 × 4.6 mm, 5 µm) | Acetonitrile, 0.05 mol/L aqueous potassium phosphate (0.2% triethylamine, pH = 4.8) | Isocratic (42:58) | Not applicable | 345 | LLE | [49,125] | ||
| Everolimus | Breast milk | 2H4-everolimus | NS | NS | Gradient | ESI (+) | 975.6 > 908.5 | 979.6 > 912.5 | Not used | Online enrichment | [81,126] |
| Everolimus | Saliva | 13C,2H3-everolimus | Sunfire C18 | Water (20 mmol/L ammonium formate), methanol | Gradient | NS | NS | NS | Not used | LLE | [82,127] |
| Gefitinib | CSF | 2H8-gefitinib | XTerra phenyl (50 × 4.6 mm, 5 µm) | Water (0.1% ammonia), acetonitrile | Isocratic (30:70) | APCI (+) | 447.2 > 128.0 | 455.4 > 136.0 | Not used | LLE | [39,40,42,43,114,128] |
| Gefitinib | CSF | Vandetanib | Intersil ODS3 (150 × 2.1 mm, 3 µm) | Water (0.02 mol/L ammonium acetate), acetonitrile. | Isocratic (70:30) | ESI (+) | 447.2 > 128.1 | 475.6 > 112.0 | Not used | LLE | [41,114] |
| Gefitinib | CSF | Erlotinib | Zorbax Eclipse XDB-C18 (150 × 4.6 mm, 5 µm) | Water (0.1% triethylamine, pH = 4.8), acetonitrile | Gradient | Not applicable | 344 | SPE | [44,129] | ||
| Gefitinib | CSF | 2H8-gefitinib | Xterra octadecylsilica (50 × 2.1 mm, 3.5 µm) | Acetonitrile (0.1% FA), water (0.1% FA) | Isocratic (70:30) | ESI (+) | 447.1 > 128.0 | 455.1 > 136.0 | Not used | Deprot. | [45,130] |
| Gefitinib | pleural and peritoneal effusate | Liquid chromatography–tandem mass spectrometry was used. | [38] | ||||||||
| Ibrutinib | CSF | 2H5-ibrutinib | nLC EASY-Spray (50 cm) | NS | Gradient | Not specified (+) | 441.2034 > 138.0900 | 446.2347 > 138.0900 | Not used | Deprot. | [85] |
| Ibrutinib | CSF | Propranolol | Zorbax SB-C18 (150 × 2.1 mm, 5 µm) | Methanol, water (0.1% FA) | Gradient | ESI (+) | NS | NS | Not used | Deprot. | [86,131] |
| Icotinib | CSF | Liquid chromatography–tandem mass spectrometry was used. | [66] | ||||||||
| Icotinib | CSF | Liquid chromatography–tandem mass spectrometry was used. | [67] | ||||||||
| Imatinib | Breast milk | 2H8-imatinib | Luna C18 (50 × 4.6 mm, 5 µm) | Methanol (0.1% FA), water (0.1% FA) | Gradient | ESI (+) | 493.7 | 501.7 | Not used | Deprot. | [20,132] |
| Imatinib | Breast milk | None | Luna C18 (50 × 4.6 mm, 5 µm) | Methanol (0.1% FA), water (0.1% FA) | Gradient | ESI (+) | 494 > 394 | Not used | Not used | Deprot. | [21,132] |
| Imatinib | Breast milk | Liquid chromatography–tandem mass spectrometry was used. Deprot. was employed as sample preparation. | [22] | ||||||||
| Imatinib | Breast milk | No details of the employed analytical methodology are disclosed. | [23] | ||||||||
| Imatinib | Breast milk | No details of the employed analytical methodology are disclosed. | [24] | ||||||||
| Imatinib | Breast milk | No details of the employed analytical methodology are disclosed. | [25] | ||||||||
| Imatinib | CSF | Carbamazepine | Nucleoshell C18 (150 × 3 mm, 2.7 µm) | Water (0.1% FA), methanol | Gradient | ESI (+) | 494.27 > 394.2, 494.27 > 247.1, 494.27 > 217.2. | 237.1 > 194.2 237.1 > 165.1 237.1 > 121.1 | Not used | Deprot. | [12] |
| Imatinib | CSF | Liquid chromatography–tandem mass spectrometry was used. | [15] | ||||||||
| Imatinib | CSF | 2H8-imatinib | Symmetry Shield-RP8 (50 × 4.6 mm, 3.5 µm) | Methanol (0.05% ammonium acetate), water (0.05% ammonium acetate) | Isocratic (72:28) | APCI (+) | 494.3 > 394.3 | 502.2 > 394.3 | Not used | Deprot. | [16,115] |
| Imatinib | CSF | No details of the analytical methodology are disclosed. | [17] | ||||||||
| Imatinib | CSF | None | ZirChromPDB-ZrO2 (50 × 4.6 mm, 3 µm) | Water (0.01 mol/L KH2PO4, 0.09 mol/L K2HPO4), methanol | Isocratic (60:40) | Not used | 260 | Deprot., online enrichment | [18] | ||
| Imatinib | CSF | No details of the analytical methodology are disclosed. | [19] | ||||||||
| Imatinib | Leukocytes | Clozapine | Symmetry Shield-RP8 (50 × 4.6 mm, 3.5 µm) | Methanol (0.05% ammonium acetate), Water (0.05% ammonium acetate) | Isocratic (72:28) | Not applicable | 261 | SPE | [13] | ||
| Imatinib | PBMC | Quinoxaline | Atlantis T3 C18 (150 × 2.1 mm, 3 µm) | Water (0.05% FA), acetonitrile (0.05% FA) | Gradient | ESI (+) | 493.8 | 313.0 | Not used | Deprot. | [14,133] |
| Imatinib | semen | NS | CAPCELLPAK-C18 | Water (2 mmol/L ammonium acetate, 0.05% TFA), acetonitrile-methanol 1:1 (0.05% TFA) | NS | ESI (+) | NS | NS | Not used | NS | [26] |
| Lapatinib | CSF | High-performance liquid chromatography–mass spectrometry was used. | [83] | ||||||||
| Neratinib | CSF | Liquid chromatography–tandem mass spectrometry was used. | [84] | ||||||||
| Nilotinib | CSF | NS | Nucleosil C18 HD (125 × 2 mm, 3.5 µm) | Acetonitrile, 0.05 mol/L aqueous potassium dihydrogenphosphate (pH = 4.03) | Isocratic (37:63) | Not applicable | 258 | Online enrichment | [29,134] | ||
| Nilotinib | CSF | No details of the analytical methodology are disclosed. | [30] | ||||||||
| Nilotinib | CSF | 13C,2H3-nilotinib | Acquity BEH C18 (50 × 2.1 mm, 1.7 µm) | NS | NS | ESI (+) | 530.27 > 289.01 | NS | Not used | Deprot. | [32,33,34,36] |
| Nilotinib | CSF | High-performance liquid chromatography and tandem mass spectrometry were used. The internal standard was 2H6-nilotinib. | [35] | ||||||||
| Nilotinib | Pleural effusate | Liquid chromatography–tandem mass spectrometry was used. | [31] | ||||||||
| Nintedanib | CSF | Carbamazepine | Nucleoshell C18 (150 × 3 mm, 2.7 µm) | Water (0.1% FA), methanol | Gradient | ESI (+) | 540.26 > 113.1 540.26 > 70.2 540.26 > 42.2 | 237.1 > 194.2 237.1 > 165.1 237.1 > 121.1 | Not used | Deprot. | [12] |
| Osimertinib | CSF | Liquid chromatography–tandem mass spectrometry was used. | [62] | ||||||||
| Osimertinib | CSF | Sample pretreatment consisted of deprot. Liquid chromatography-tandem mass spectrometry was used. | [63] | ||||||||
| Osimertinib | CSF | Liquid chromatography–tandem mass spectrometry was used. | [64] | ||||||||
| Panobiostat | CSF | Carbamazepine | Nucleoshell C18 (150 × 3 mm, 2.7 µm) | Water (0.1% FA), methanol | Gradient | ESI (+) | 350.2 > 158.2 350.2 > 143.1 | 237.1 > 194.2 237.1 > 165.1 237.1 > 121.1 | Not used | Deprot. | [12] |
| Panobinostat | CSF | Liquid chromatography–tandem mass spectrometry was used. | [92] | ||||||||
| Panobinostat | CSF | No details of the employed analytical methodology are disclosed. | [93] | ||||||||
| Pazopanib | ascitic fluid | No details of the employed analytical methodology are disclosed. | [88] | ||||||||
| Ponatinib | CSF | NS | Hypersil Gold PFP (100 × 2.1 mm, 1.9 µm) | Water (10 mmol/L formate ammonium buffer, 0.1% FA), acetonitrile (0.1% FA) | Gradient | ESI | NS | NS | Not used | Deprot. | [37,135] |
| Regorafenib | CSF | Carbamazepine | Nucleoshell C18 (150 × 3 mm, 2.7 µm) | Water (0.1% FA), methanol | Gradient | ESI (+) | 483.09 > 288.1 483.09 > 270.1 483.09 > 202.0 | 237.1 > 194.2 237.1 > 165.1 237.1 > 121.1 | Not used | Deprot. | [12] |
| Regorafenib | CSF | 2H5-moxifloxacin | Kinetex F5 (50 × 4.6 mm, 2.5 µm) | Water (0.1% FA), methanol (0.1% FA) | Gradient | NS, (+) polarity | 483.1 > 270.1 | 407.4 > 266.4 | Not used | Deprot. | [89] |
| Ribociclib | CSF | Carbamazepine | Nucleoshell C18 (150 × 3 mm, 2.7 µm) | Water (0.1% FA), methanol | Gradient | ESI (+) | 435.3 > 322.1 435.3 > 294.1 435.3 > 252.1 | 237.1 > 194.2 237.1 > 165.1 237.1 > 121.1 | Not used | Deprot. | [12] |
| Ribociclib | CSF | 13C6-ribociclib | Xbridge Amide (100 × 4.6 mm, 3.5 µm) | Acetonitrile, water (10 mmol/L ammonium formate, pH = 3.0) | Isocratic (75:25) | ESI (+) | 435.3 > 367.2 | 441.3 > 373.2 | Not used | Deprot. | [78,79,136] |
| Ribociclib | CSF | 2H6-ribociclib | Polaris C8 (50 × 2.0 mm, 5 µm) | Water (0.1% FA), acetonitrile (0.1% FA) | Gradient | ESI (+) | 435.2 > 252.1 | 441.2 > 252.1 | Not used | Dilution, acidification, centrifugation | [80,137] |
| Sunitinib | ascitic fluid | No details of the employed analytical methodology are disclosed. | [88] | ||||||||
| Tepotinib | CSF | Ultra-performance liquid chromatography was used. | [90] | ||||||||
| Tepotinib | CSF | Liquid chromatography–tandem mass spectrometry was used. | [91] | ||||||||
| Trametinib | CSF | 13C6-trametinib | XSelect HSS T3 (75 × 2.1 mm, 3.5 µm) | Water (2 mmol/L ammonium acetate, 0.1% FA), acetonitrile (0.1% FA) | Gradient | ESI (+) | 616.1 > 254.1 616.1 > 491.3 | 622.0 > 497.2 | Not used | Deprot. | [69,120] |
| Vemurafenib | CSF | Sorafenib | XTerra C8 MS (250 × 4.6 mm, 5 µm) | Water (100 mmol/L glycine, pH = 9.0), acetonitrile | Isocratic (45:55) | Not applicable | 249 | Deprot. | [68,138] | ||
| Venetoclax | CSF | 2H8-venetoclax | Atlantis C18 (50 × 2.1 mm, 3 µm) | Acetonitrile, water (0.1% FA) | Isocratic (55:45) | ESI (+) | 868 > 321 | 876 > 329 | Not used | Deprot. | [95,139] |
| Venetoclax | CSF | 2H8-venetoclax | Atlantis C18 (50 × 2.1 mm, 3 µm) | Acetonitrile, water (0.1% FA) | Isocratic (55:45) | ESI (+) | 868 > 321 | 876 > 329 | Not used | LLE | [96,139] |
| Vismodegib | CSF | 2H5-vismodegib | Betasil C18 (100 × 2.1 mm) | Water (0.1% FA), acetonitrile | Isocratic (40:60) | ESI (+) | 421.1 > 139.2 | 426.1 > 139.1 | Not used | SPE | [94,140] |
| Vorinostat | CSF | Carbamazepine | Nucleoshell C18 (150 × 3 mm, 2.7 µm) | Water (0.1% FA), methanol | Gradient | ESI (+) | 265.16 > 232.1 265.16 > 77.1 265.16 > 55.1 | 237.1 > 194.2 237.1 > 165.1 237.1 > 121.1 | Not used | Deprot. | [12] |
| Zanubrutinib | CSF | Tolbutamide | Zorbax SB-C18 (150 × 2.1 mm, 5 µm) | Methanol, water (0.1% FA) | Gradient | ESI (+) | NS | NS | Not used | Deprot. | [86,131] |
| Zanubrutinib | CSF | NS | Acquity BEH C18 (50 × 2.1 mm, 1.7 µm) | Water (0.15 FA), acetonitrile (0.1% FA) | NS | ESI (+) | NS | NS | Not used | Deprot. | [87] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Köllő, Z.; Garami, M.; Vincze, I.; Vásárhelyi, B.; Karvaly, G.B. Therapeutic Monitoring of Orally Administered, Small-Molecule Anticancer Medications with Tumor-Specific Cellular Protein Targets in Peripheral Fluid Spaces—A Review. Pharmaceutics 2023, 15, 239. https://doi.org/10.3390/pharmaceutics15010239
Köllő Z, Garami M, Vincze I, Vásárhelyi B, Karvaly GB. Therapeutic Monitoring of Orally Administered, Small-Molecule Anticancer Medications with Tumor-Specific Cellular Protein Targets in Peripheral Fluid Spaces—A Review. Pharmaceutics. 2023; 15(1):239. https://doi.org/10.3390/pharmaceutics15010239
Chicago/Turabian StyleKöllő, Zoltán, Miklós Garami, István Vincze, Barna Vásárhelyi, and Gellért Balázs Karvaly. 2023. "Therapeutic Monitoring of Orally Administered, Small-Molecule Anticancer Medications with Tumor-Specific Cellular Protein Targets in Peripheral Fluid Spaces—A Review" Pharmaceutics 15, no. 1: 239. https://doi.org/10.3390/pharmaceutics15010239