
Amoxicillin and Clarithromycin Mucoadhesive Delivery System for Helicobacter pylori Infection in a Mouse Model: Characterization, Pharmacokinetics, and Efficacy

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Materials
2.2. Methods
2.2.1. Drug Product and Characterization
2.2.2. PK Study
Animals and Treatments
Drug Analysis with High-Performance Liquid Chromatography–Coupled Mass spectroscopy (HPLC-MS/MS)
2.2.3. PD Study
In Vitro Antibacterial Study of Amox and Clar
2.3. Animals, Infection Model, and Treatments
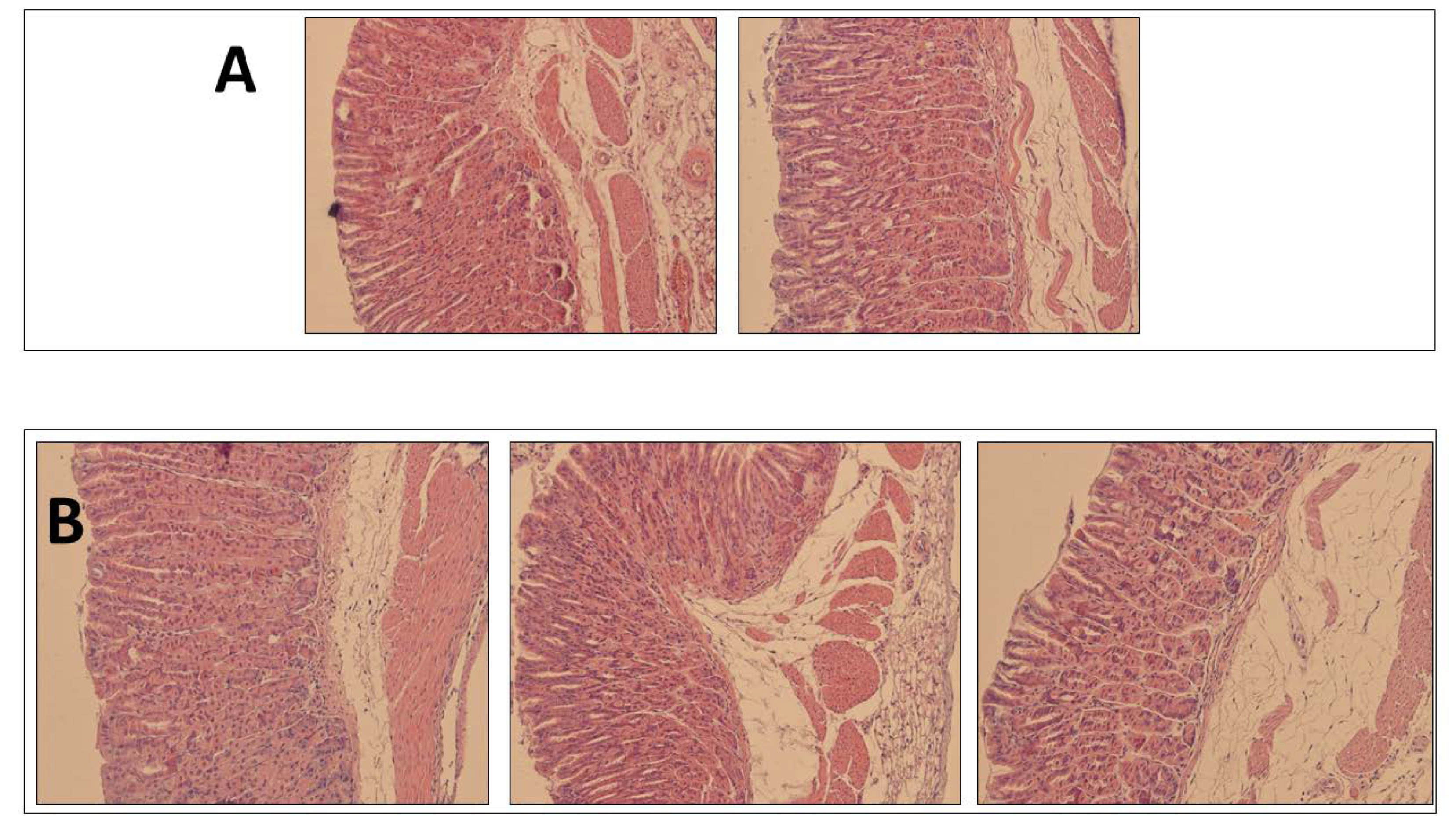
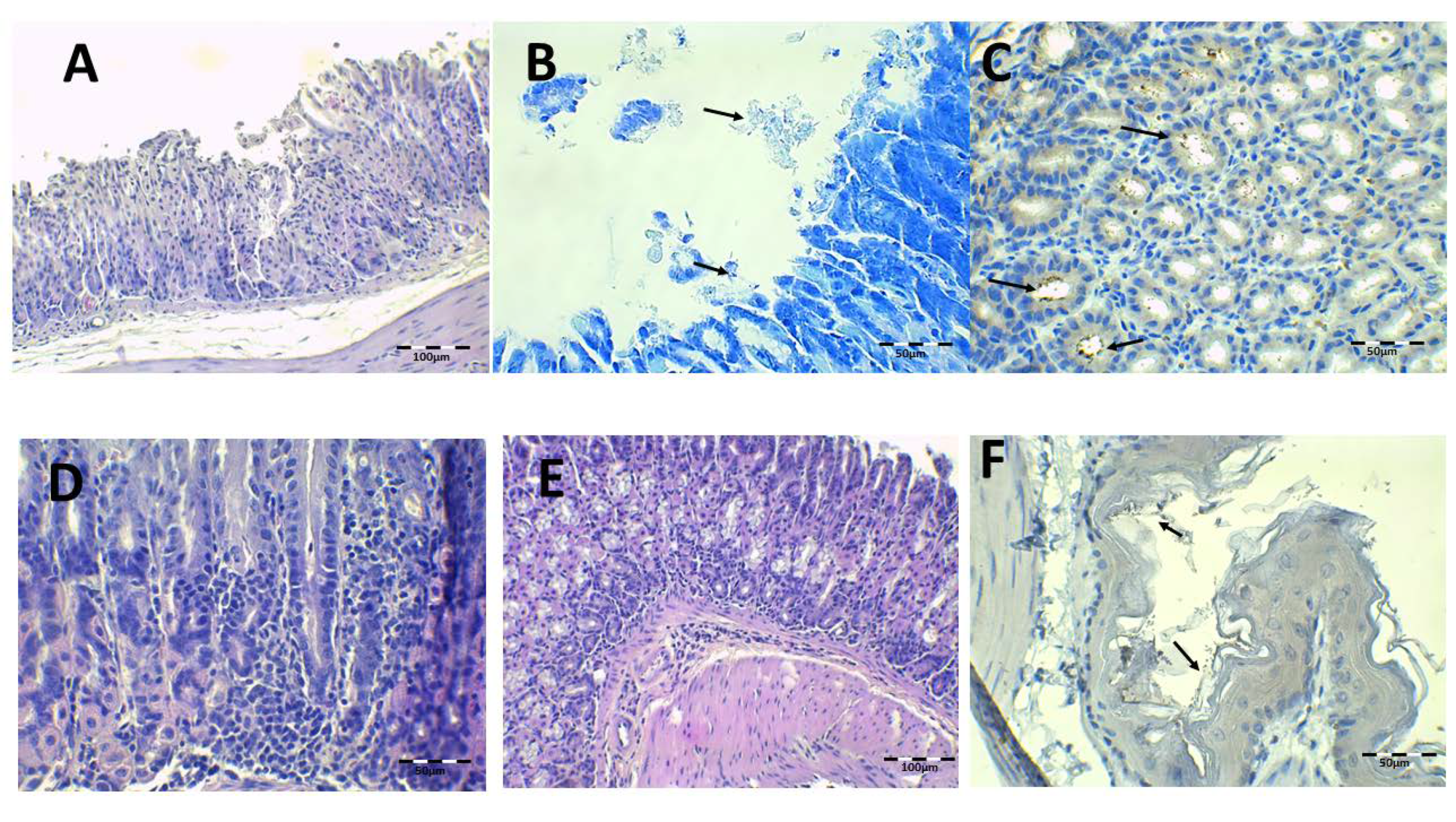
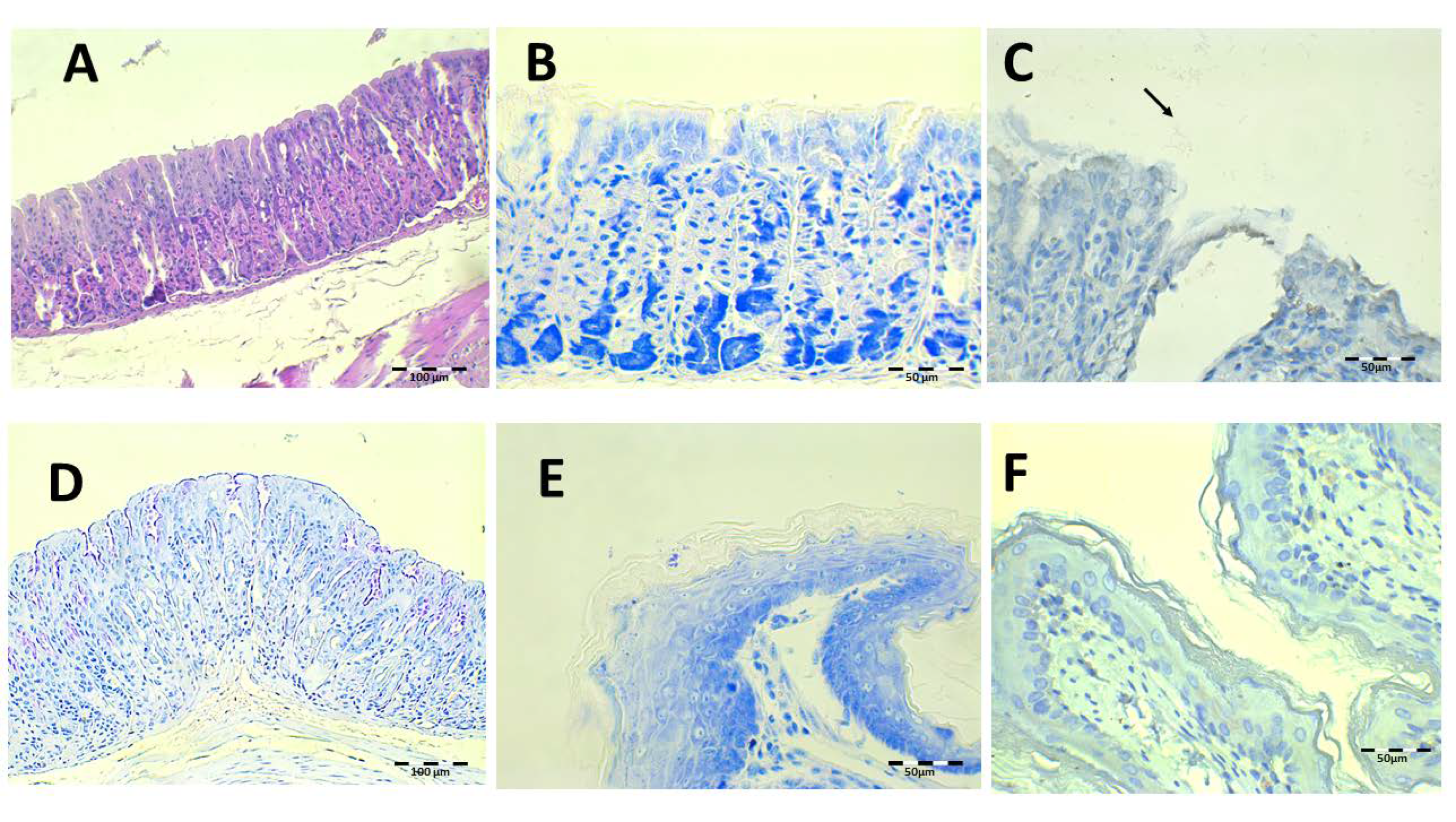
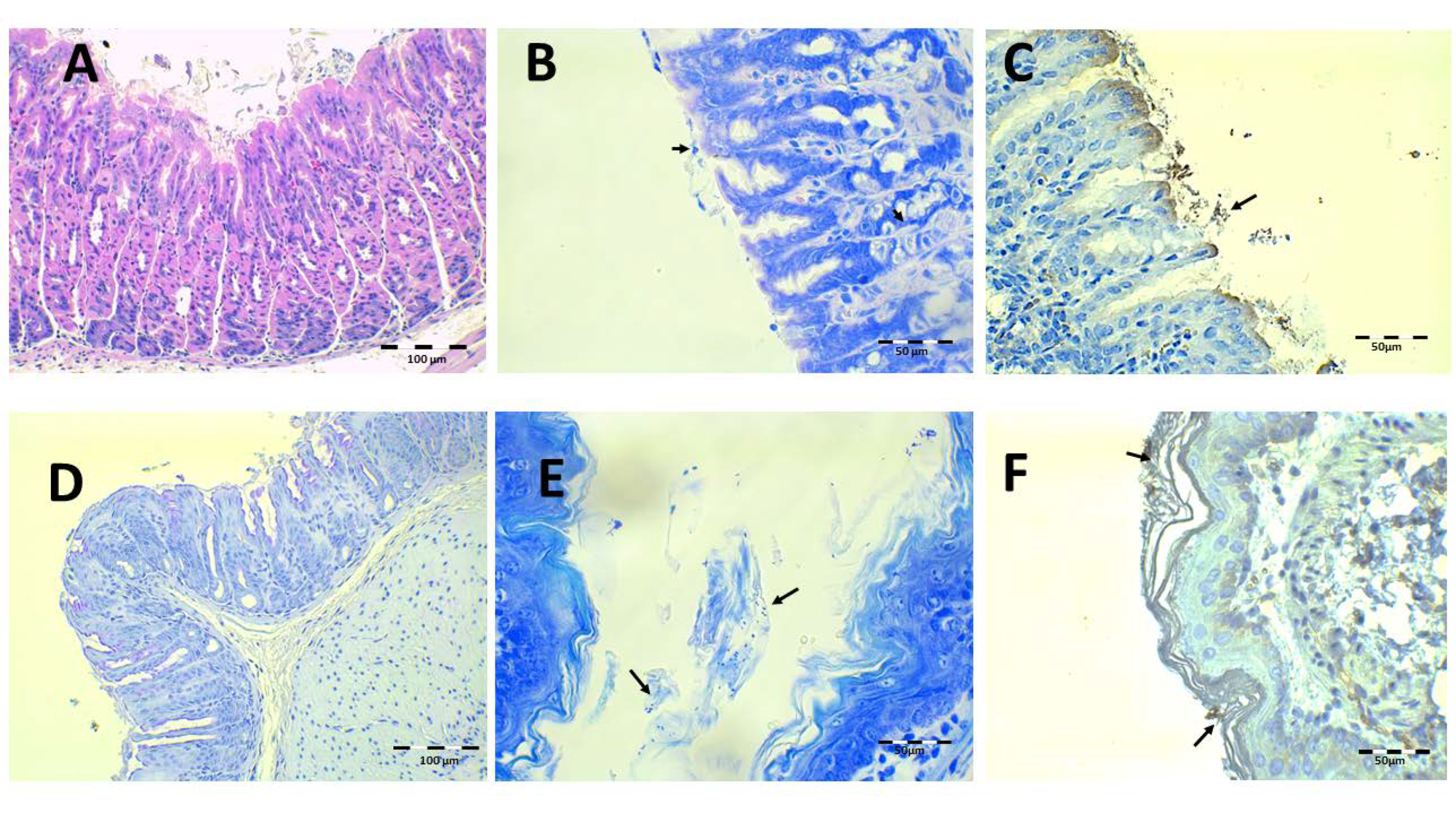
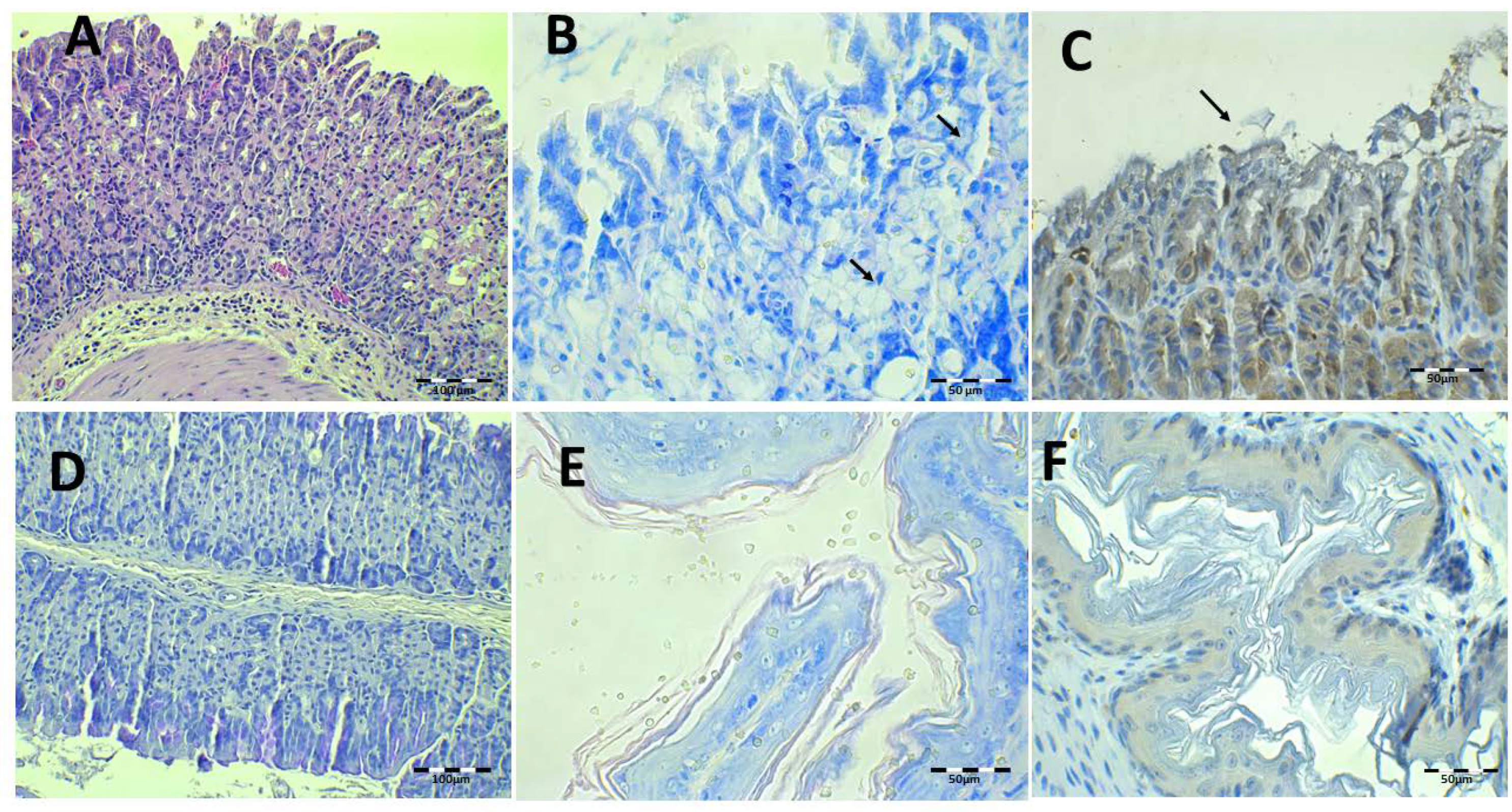
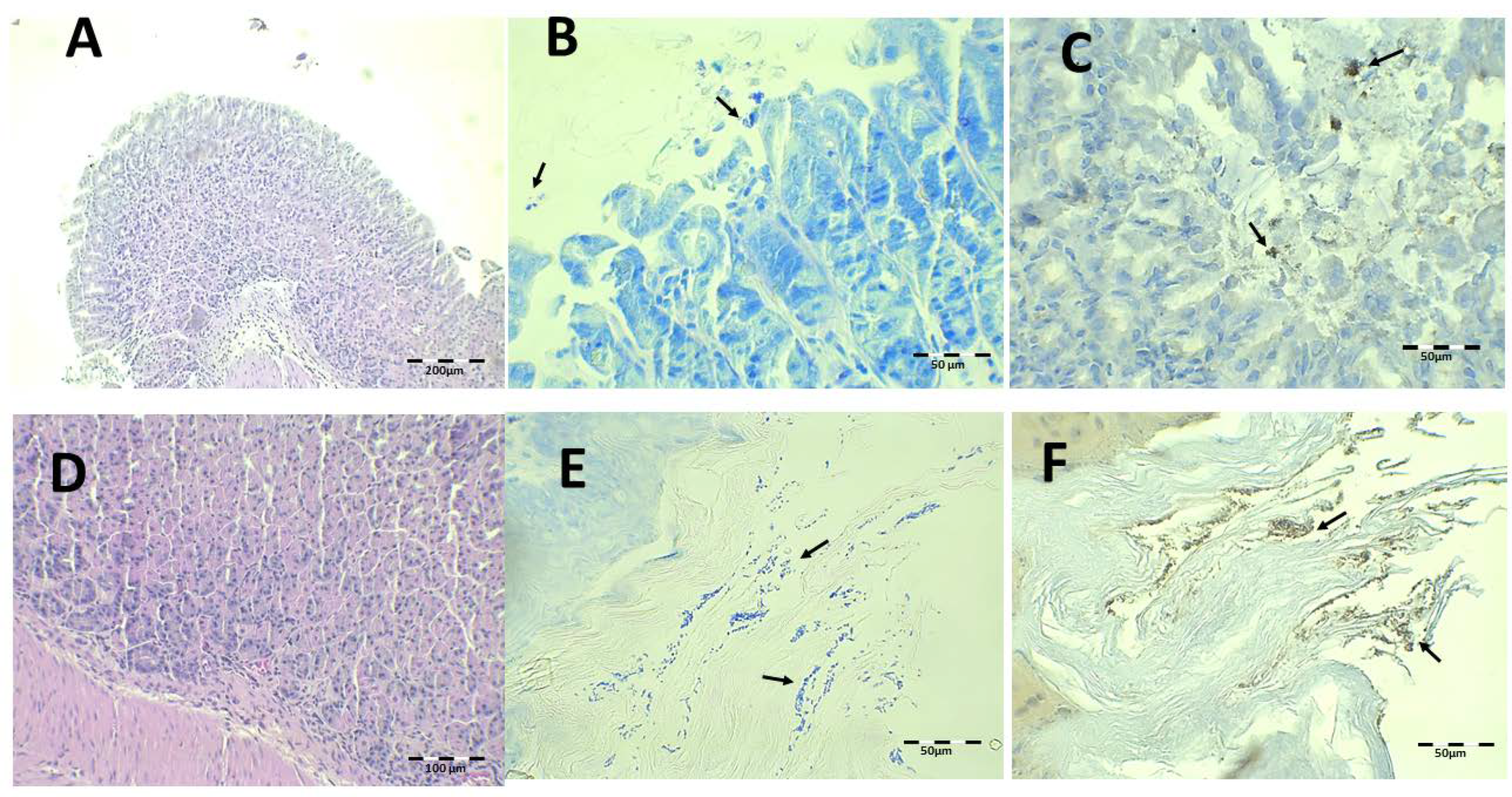
2.4. Histology
2.5. Biomarkers
2.6. Enzyme-Linked Immunosorbent Assay
2.7. Western Blot Analysis
3. Results
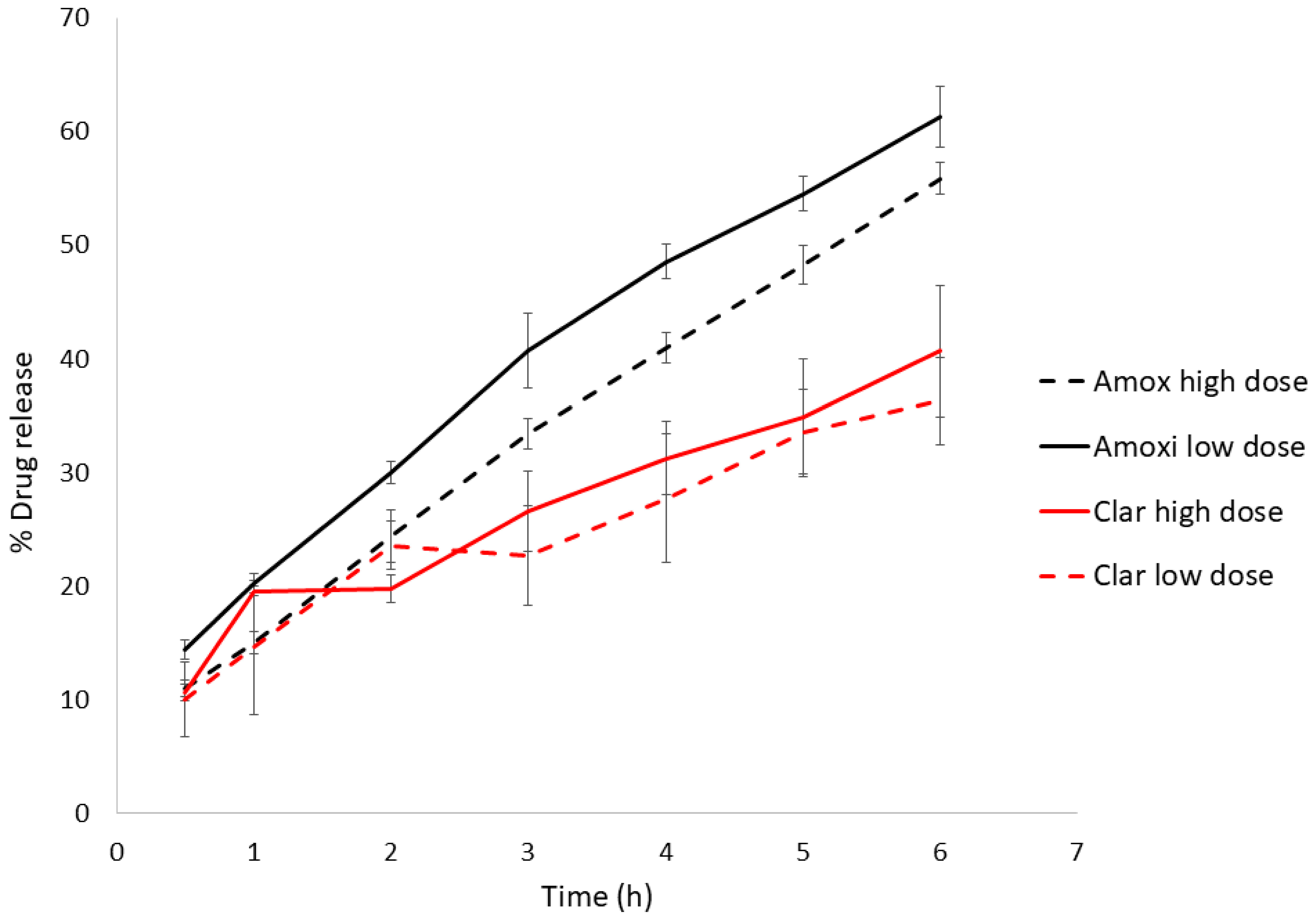
3.1. Drug Product and Administration
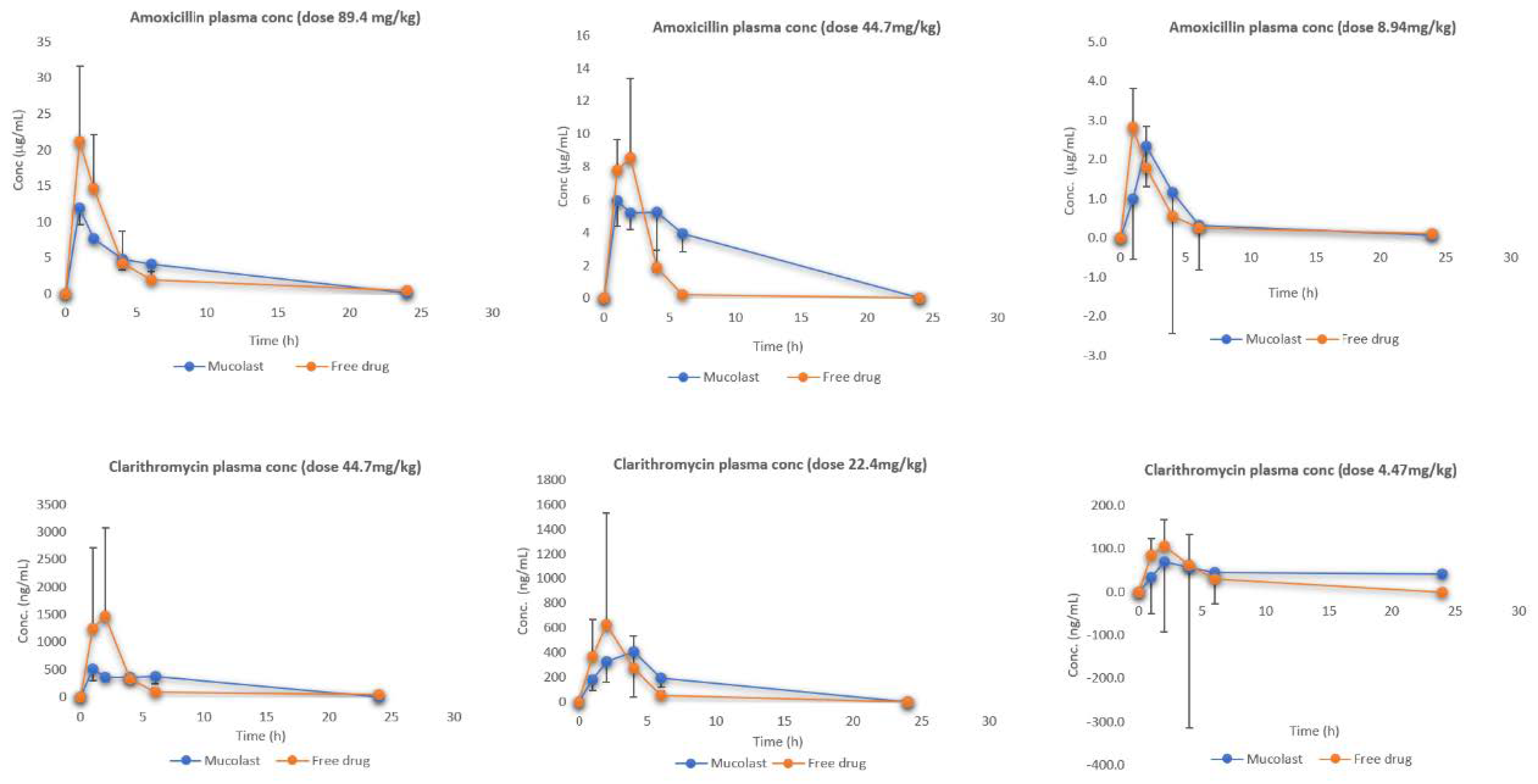
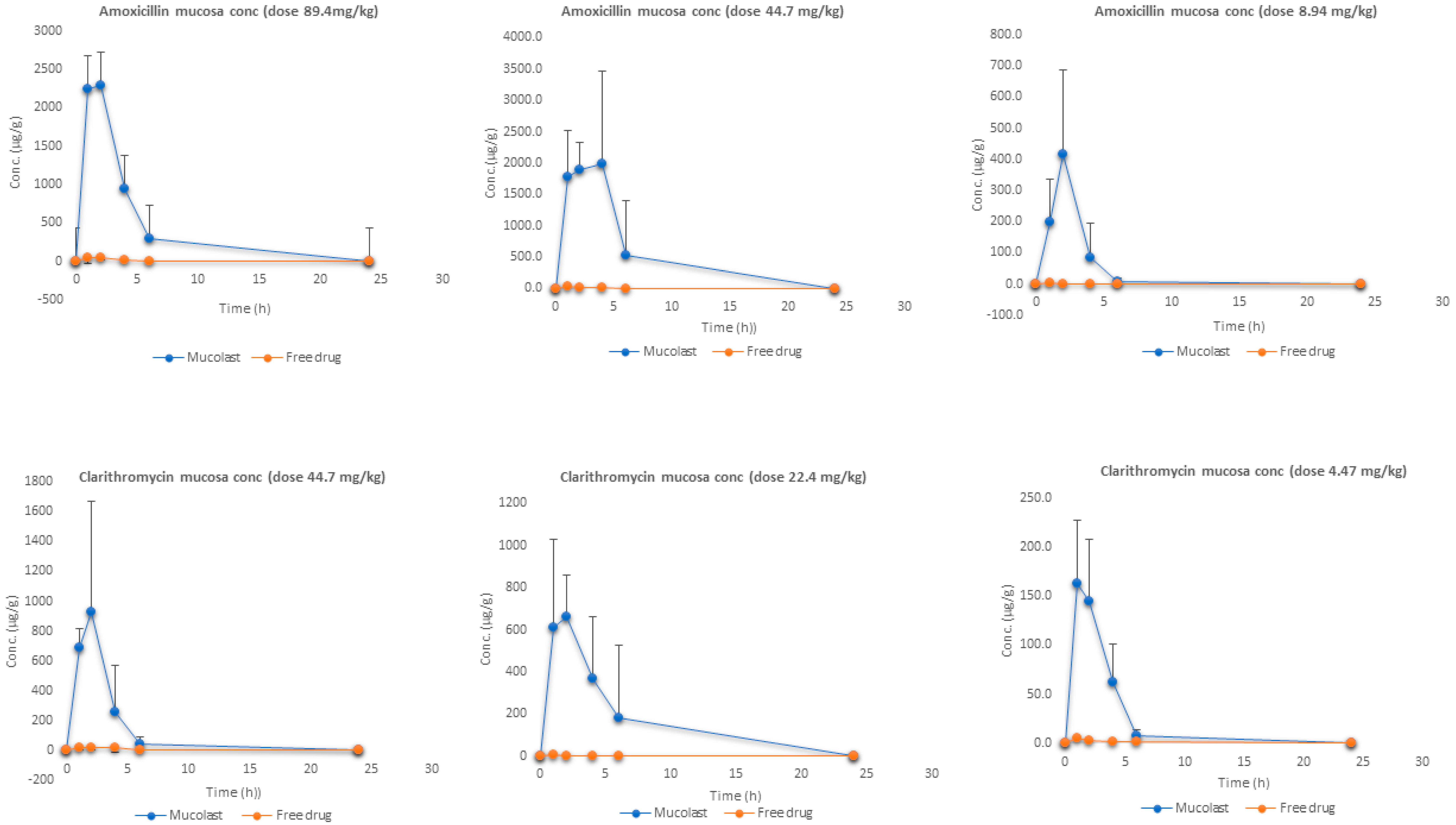
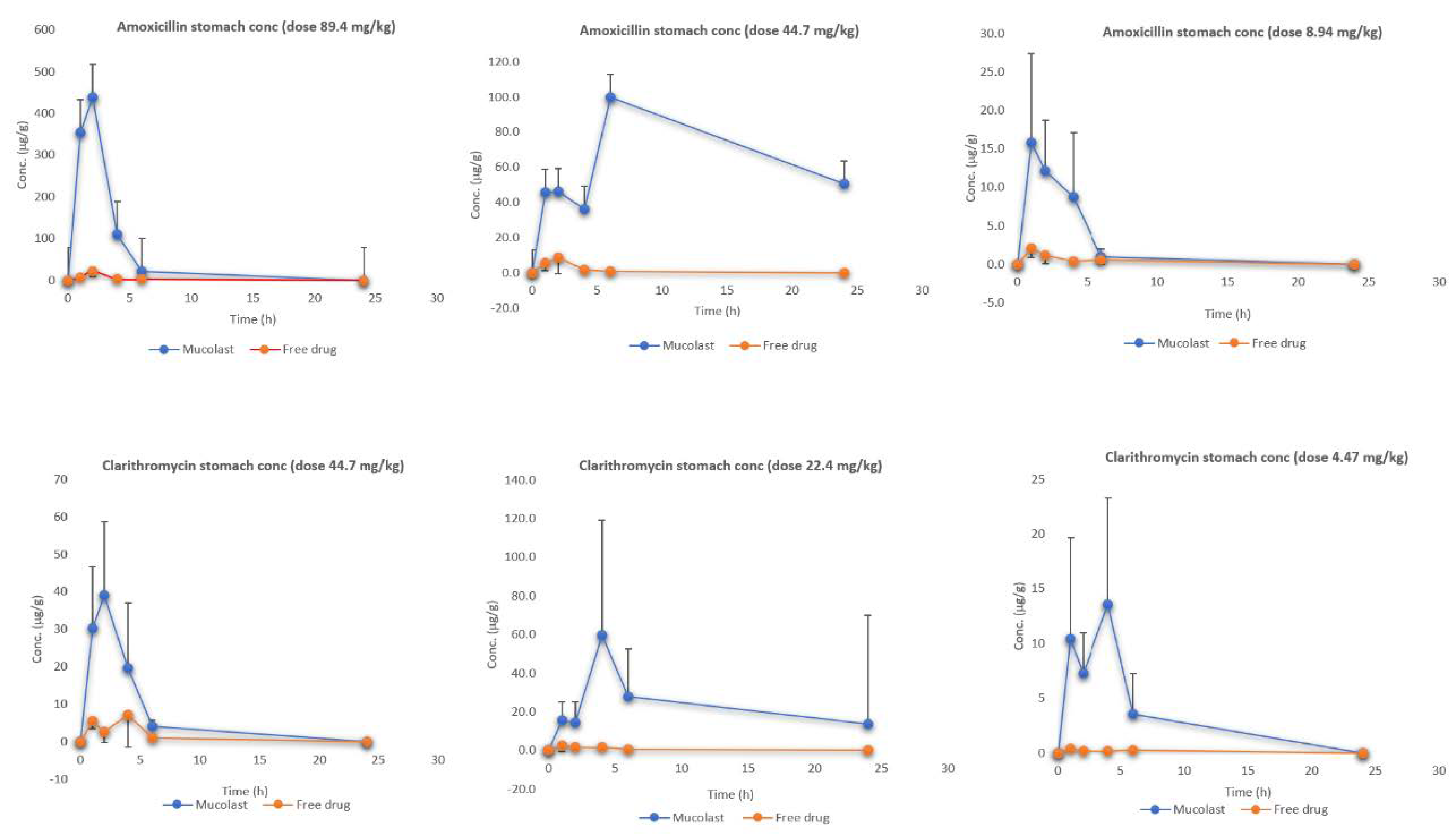
3.2. PK Study
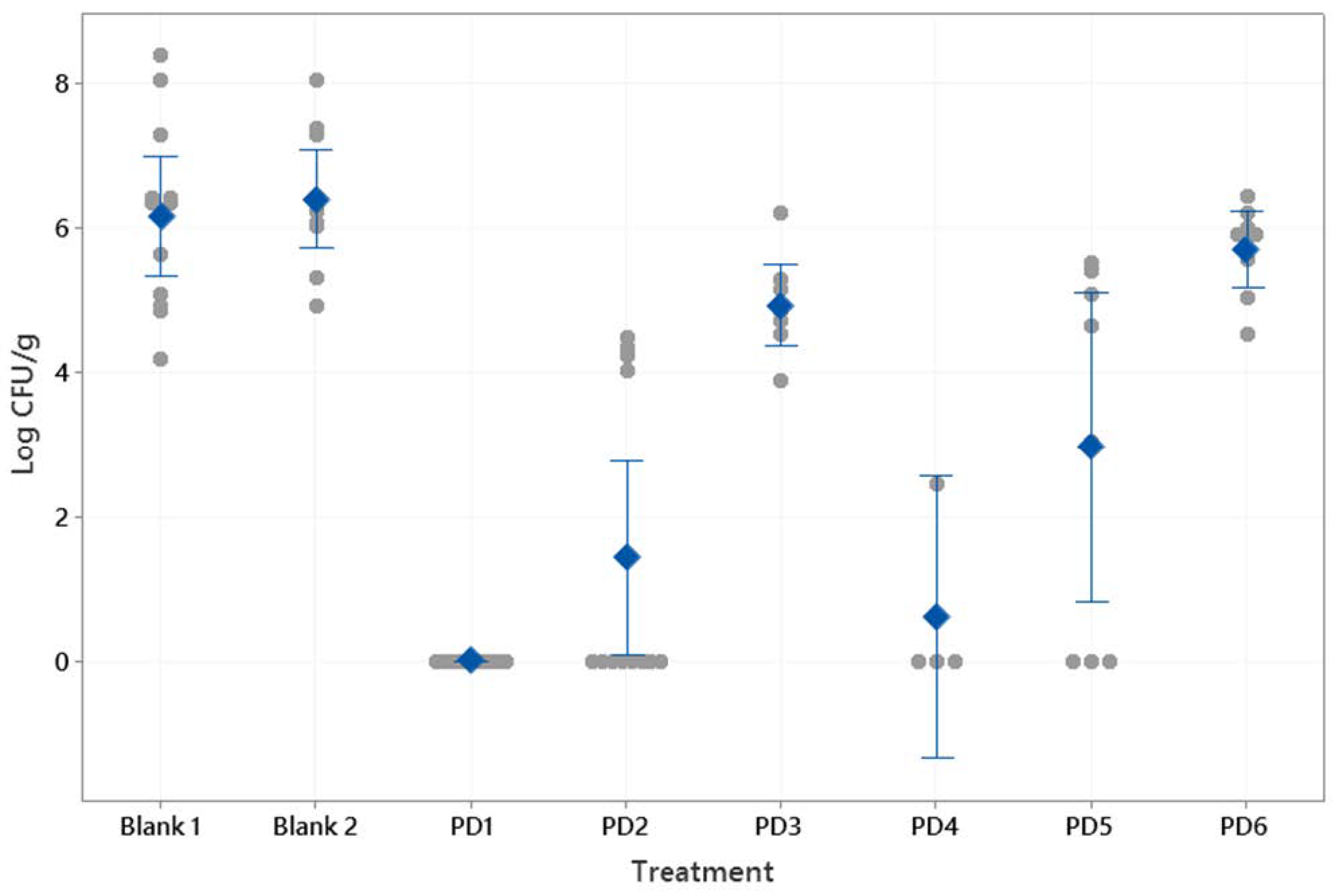
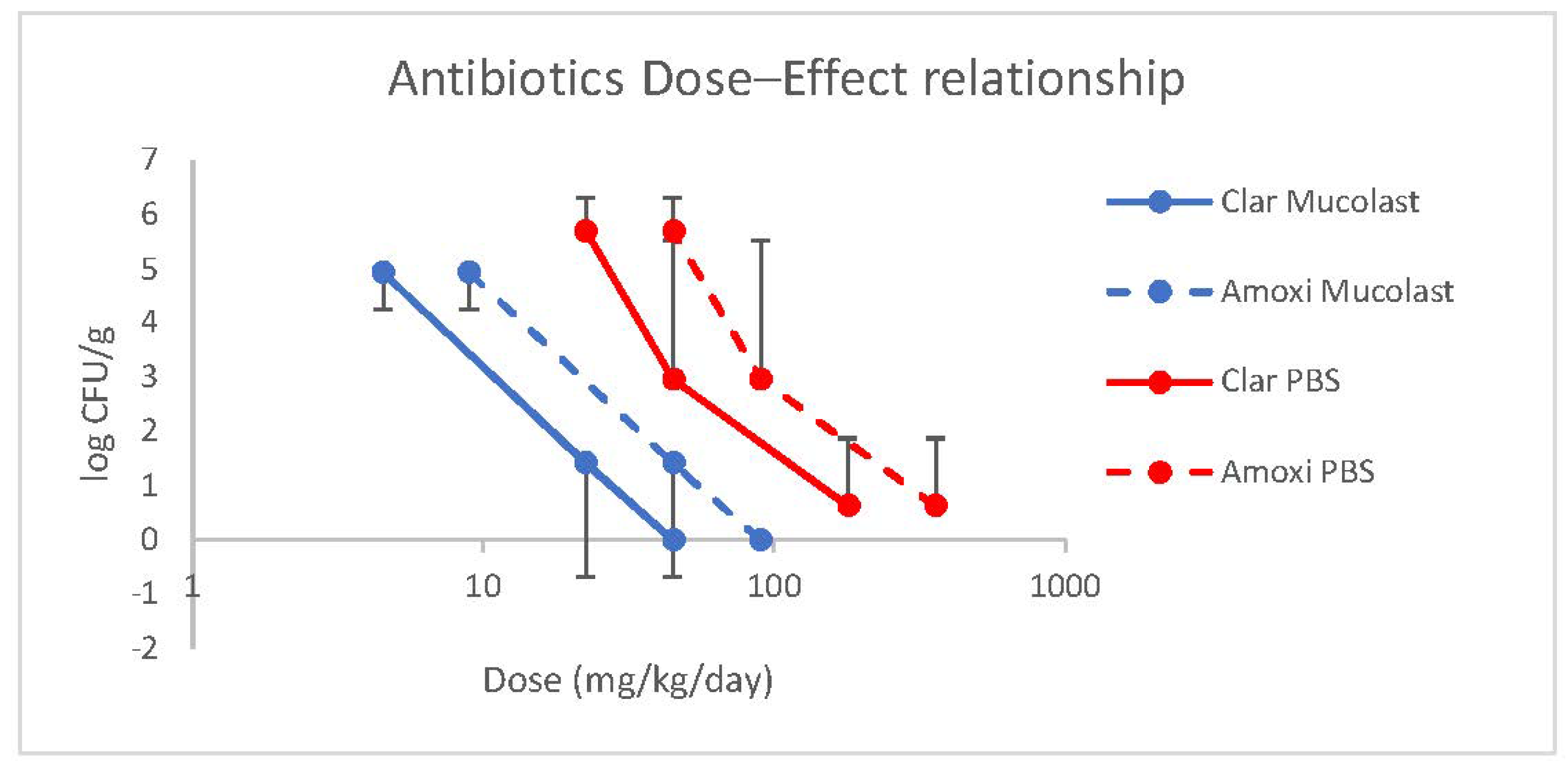
3.3. PD Study
3.3.1. In Vitro Antibacterial Study of Amox and Clar
3.3.2. In Vivo Study
Histological Evaluation
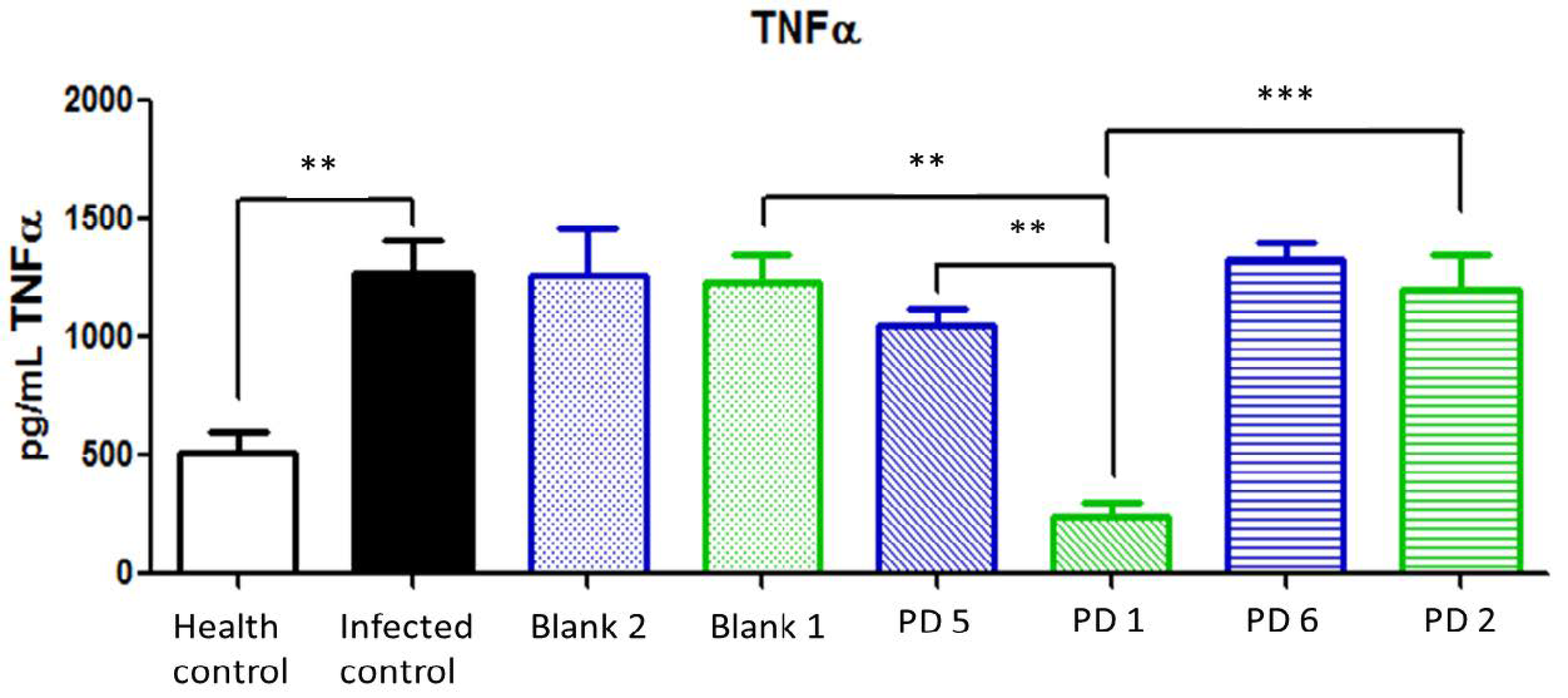
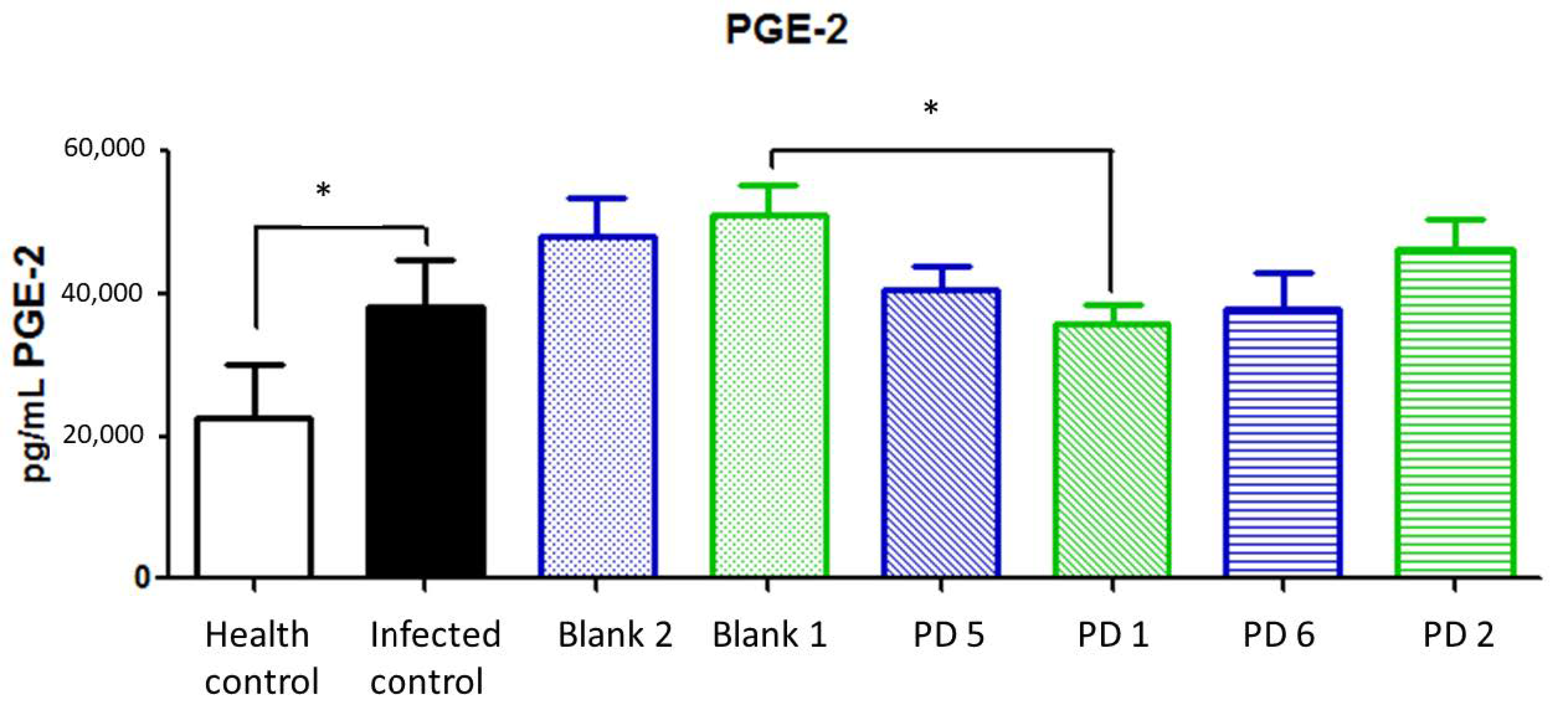
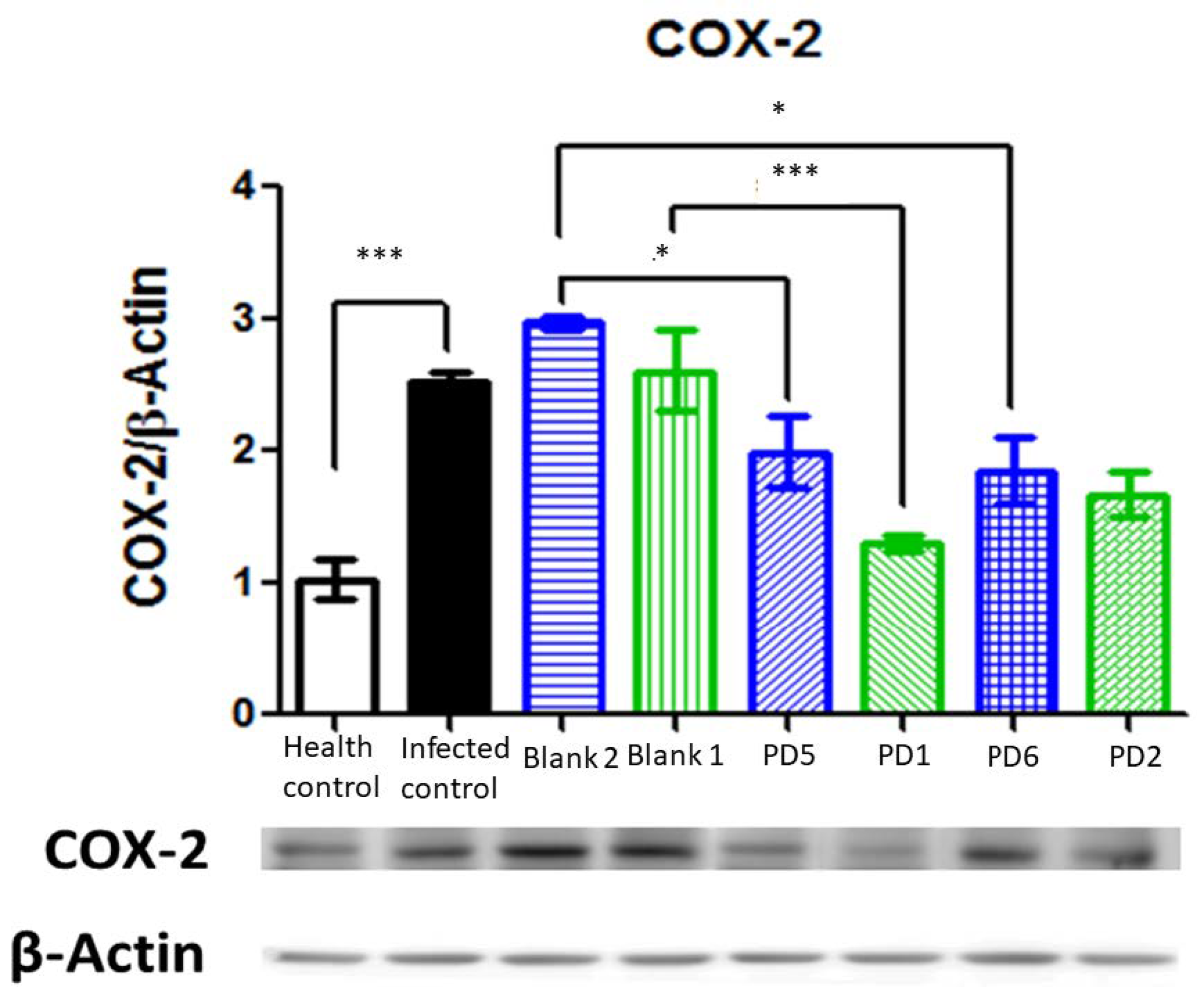
Biochemical Analysis
4. Conclusions
5. Patents
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Whalen, M.B.; Massidda, O. Helicobacter pylori: Enemy, commensal or, sometimes, friend? J. Infect. Dev. Ctries. 2015, 9, 674–678. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kusters, J.G.; Van Vliet, A.H.M.; Kuipers, E.J. Pathogenesis of Helicobacter pylori infection. Clin. Microbiol. Rev. 2006, 19, 449–490. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Makristathis, A.; Hirschl, A.M.; Mégraud, F.; Bessède, E. Review: Diagnosis of Helicobacter pylori infection. Helicobacter 2019, 24, e12641. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chey, W.D.; Leontiadis, G.I.; Howden, C.W.; Moss, S.F. ACG Clinical Guideline: Treatment of Helicobacter pylori Infection. Am. J. Gastroenterol. 2017, 112, 212–239. [Google Scholar] [CrossRef]
- Yuan, Y.; Ford, A.C.; Khan, K.J.; Gisbert, J.P.; Forman, D.; Leontiadis, G.I.; Tse, F.; Calvet, X.; Fallone, C.; Fischbach, L.; et al. Optimum duration of regimens for Helicobacter pylori eradication. Cochrane Database Syst. Rev. 2013, 2013, 1–205. [Google Scholar]
- O’Connor, A.; Liou, J.; Gisbert, J.P.; O’Morain, C. Review: Treatment of Helicobacter pylori Infection 2019. Helicobacter 2019, 24. [Google Scholar] [CrossRef] [Green Version]
- Alkim, H.; Koksal, A.R.; Boga, S.; Sen, I.; Alkim, C. Role of bismuth in the eradication of helicobacter pylori. Am. J. Ther. 2016, 24, E751–E757. [Google Scholar] [CrossRef]
- Arora, S.; Gupta, S.; Narang, R.K.; Budhiraja, R.D. Amoxicillin loaded chitosan-alginate polyelectrolyte complex nanoparticles as mucopenetrating delivery system for H. pylori. Sci. Pharm. 2011, 79, 673–694. [Google Scholar] [CrossRef] [Green Version]
- Patel, J.; Patel, M. Stomach Specific Anti-Helicobacter Pylori Therapy: Preparation and Evaluation of Amoxicillin-Loaded Chitosan Mucoadhesive Microspheres. Curr. Drug Deliv. 2006, 4, 41–50. [Google Scholar] [CrossRef]
- Umamaheshwari, R.B.; Ramteke, S.; Jain, N.K. Anti-Helicobacter pylori effect of mucoadhesive nanoparticles bearing amoxicilin in experimental gerbils model. AAPS Pharmscitech 2004, 5, 60. [Google Scholar] [CrossRef]
- Harsha, S. Dual drug delivery system for targeting H. pylori in the stomach: Preparation and in vitro characterization of amoxicillin-loaded Carbopol® nanospheres. Int. J. Nanomed. 2012, 7, 4787–4796. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ali, M.S.; Pandit, V.; Jain, M.; Dhar, K.L. Mucoadhesive microparticulate drug delivery system of curcumin against Helicobacter pylori infection: Design, development and optimization. J. Adv. Pharm. Technol. Res. 2014, 5, 48–56. [Google Scholar] [CrossRef] [PubMed]
- Pan-In, P.; Tachapruetinun, A.; Chaichanawongsaroj, N.; Banlunara, W.; Suksamrarn, S.; Wanichwecharungruang, S. Combating Helicobacter pylori infections with mucoadhesive nanoparticles loaded with Garcinia mangostana extract. Nanomedicine 2014, 9, 457–468. [Google Scholar] [CrossRef]
- da Silva Junior, I.F.; Balogun, S.O.; de Oliveira, R.G.; Damazo, A.S.; de Oliveira Martins, D.T. Piper umbellatum L.: A medicinal plant with gastric-ulcer protective and ulcer healing effects in experimental rodent models. J. Ethnopharmacol. 2016, 192, 123–131. [Google Scholar] [CrossRef] [PubMed]
- Ramteke, S.; Jain, N. Clarithromycin-and omeprazole-containing gliadin nanoparticles for the treatment of Helicobacter pylori. J. Drug Target. 2008, 16, 65–72. [Google Scholar] [CrossRef]
- Adebisi, A.O.; Conway, B.R. Modification of drug delivery to improve antibiotic targeting to the stomach. Ther. Deliv. 2005, 6, 741–762. [Google Scholar] [CrossRef]
- Shen, S.; Wu, Y.; Liu, Y.; Wu, D. High drug-loading nanomedicines: Progress, current status, and prospects. Int. J. Nanomed. 2017, 12, 4085–4109. [Google Scholar] [CrossRef] [Green Version]
- WO2017162822. Compositions for Mucosal Adhesion and Uses Thereof. Available online: https://patentscope.wipo.int/search/en/detail.jsf?docId=WO2017162822 (accessed on 2 November 2020).
- Amoxcillin Capsules. United States Pharmacopeia (USP) 2787; The United States Pharmacopeial Convention: Rockville, MD, USA, 2018. [Google Scholar]
- Clarithromycin Tablets. United States Pharmacopeia (USP) 3463; The United States Pharmacopeial Convention: Rockville, MD, USA, 2016. [Google Scholar]
- Zhang, Y.; Huo, M.; Zhou, J.; Zou, A.; Li, W.; Yao, C.; Xie, S. DDSolver: An add-in program for modeling and comparison of drug dissolution profiles. AAPS J. 2010, 12, 263–271. [Google Scholar] [CrossRef] [Green Version]
- Nair, A.; Jacob, S. A simple practice guide for dose conversion between animals and human. J. Basic Clin. Pharm. 2016, 7, 27. [Google Scholar] [CrossRef] [Green Version]
- Smith, G. European medicines agency guideline on bioanalytical method validation: What more is there to say? Bioanalysis 2012, 4, 865–868. [Google Scholar] [CrossRef]
- Goswami, S.; Bhakuni, R.S.; Chinniah, A.; Pal, A.; Kar, S.K.; Das, P.K. Anti-Helicobacter pylori potential of artemisinin and its derivatives. Antimicrob. Agents Chemother. 2012, 56, 4594–4607. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Navabi, N.; Johansson, M.E.V.; Raghavan, S.; Lindéna, S.K. Helicobacter pylori infection impairs the mucin production rate and turnover in the murine gastric mucosa. Infect. Immun. 2013, 81, 829–837. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosillo, M.A.; Sánchez-Hidalgo, M.; Cárdeno, A.; Aparicio-Soto, M.; Sánchez-Fidalgo, S.; Villegas, I.; de la Lastra, C.A. Dietary supplementation of an ellagic acid-enriched pomegranate extract attenuates chronic colonic inflammation in rats. Pharmacol. Res. 2012, 66, 235–242. [Google Scholar] [CrossRef] [PubMed]
- Vázquez-Román, V.; Utrilla, J.C.; Fernández-Santos, J.M.; Martín-Lacave, I. Immunohistochemical profiling of the ultimobranchial remnants in the rat postnatal thyroid gland. J. Morphol. 2017, 278, 1114–1124. [Google Scholar] [CrossRef] [PubMed]
- Bradford, M. A Rapid and Sensitive Method for the Quantitation of Microgram Quantities of Protein Utilizing the Principle of Protein-Dye Binding. Anal. Biochem. 1976, 72, 248–254. [Google Scholar] [CrossRef]
- Graham, D.Y. History of Helicobacter pylori, duodenal ulcer, gastric ulcer and gastric cancer. World J. Gastroenterol. 2014, 20, 5191–5204. [Google Scholar] [CrossRef]
- Fernández-Campos, F.; Obach, M.; Moreno, M.C.; García, A.; González, J. Pharmaceutical development of a generic corticoid semisolid formulation. J. Drug Deliv. Sci. Technol. 2017, 42. [Google Scholar] [CrossRef]
- European Committee on Antimicrobial Susceptibility Testing. EUCAST Clinical Breakpoint Table v. 5.0. Available online: https://www.eucast.org/fileadmin/src/media/PDFs/EUCAST_files/Breakpoint_tables/v_11.0_Breakpoint_Tables.pdf (accessed on 1 November 2020).
- Hong, J.B.; Zuo, W.; Wang, A.J.; Lu, N.H. Helicobacter pylori infection synergistic with IL-1β gene polymorphisms potentially contributes to the carcinogenesis of gastric cancer. Int. J. Med Sci. 2016, 13, 298–303. [Google Scholar] [CrossRef] [Green Version]
- Toller, I.M.; Hitzler, I.; Sayi, A.; Mueller, A. Prostaglandin E2 Prevents Helicobacter-Induced Gastric Preneoplasia and Facilitates Persistent Infection in a Mouse Model. YGAST 2010, 138, 1455–1467.e4. [Google Scholar] [CrossRef] [Green Version]
- Pomorski, T.; Meyer, T.F.; Naumann, M. Helicobacter pylori-induced Prostaglandin E 2 Synthesis Involves Activation of Cytosolic Phospholipase A 2 in Epithelial Cells. J. Biol. Chem. 2001, 276, 804–810. [Google Scholar] [CrossRef] [Green Version]
- Hisatsune, J.; Yamasaki, E.; Nakayama, M.; Shirasaka, D.; Kurazono, H.; Katagata, Y.; Hirayama, T. Helicobacter pylori VacA enhances prostaglandin E2 production through induction of cyclooxygenase 2 expression via a p38 mitogen-activated protein kinase/activating transcription factor 2 cascade in AZ-521 cells. Infect. Immun. 2007, 75, 4472–4481. [Google Scholar] [CrossRef] [PubMed] [Green Version]



















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | Vehicle | Amox | Clar | Subgroup | Sacrifice Time (h) |
|---|---|---|---|---|---|
| PK 1 | Mucolast® | 89.4 mg/kg/day | 44.7 mg/kg/day | a | 0 |
| b | 1 | ||||
| c | 2 | ||||
| d | 4 | ||||
| e | 6 | ||||
| f | 24 | ||||
| PK 2 | Mucolast® | 44.7 mg/kg/day | 22.35 mg/kg/day | a | 0 |
| b | 1 | ||||
| c | 2 | ||||
| d | 4 | ||||
| e | 6 | ||||
| f | 24 | ||||
| PK 3 | Mucolast® | 8.94 mg/kg/day | 4.47 mg/kg/day | a | 0 |
| b | 1 | ||||
| c | 2 | ||||
| d | 4 | ||||
| e | 6 | ||||
| f | 24 | ||||
| PK 4 | PBS | 89.4 mg/kg/day | 44.7 mg/kg/day | a | 0 |
| b | 1 | ||||
| c | 2 | ||||
| d | 4 | ||||
| e | 6 | ||||
| f | 24 | ||||
| PK 5 | PBS | 44.7 mg/kg/day | 22.35 mg/kg/day | a | 0 |
| b | 1 | ||||
| c | 2 | ||||
| d | 4 | ||||
| e | 6 | ||||
| f | 24 | ||||
| PK 6 | PBS | 8.94 mg/kg/day | 4.47 mg/kg/day | a | 0 |
| b | 1 | ||||
| c | 2 | ||||
| d | 4 | ||||
| e | 6 | ||||
| f | 24 | ||||
| Blank animals | -- | -- |
| Treatment | Vehicle | Amox Dose | Clar Dose | n |
|---|---|---|---|---|
| PD 1 | Mucolast® | 89.4 mg/kg/day | 44.7 mg/kg/day | 11 |
| PD 2 | Mucolast® | 44.7 mg/kg/day | 22.35 mg/kg/day | 12 |
| PD 3 | Mucolast® | 8.94 mg/kg/day | 4.47 mg/kg/day | 8 |
| PD 4 | PBS | 357.5 mg/kg/day | 178.8 mg/kg/day | 4 |
| PD 5 | PBS | 89.4 mg/kg/day | 44.7 mg/kg/day | 8 |
| PD 6 | PBS | 44.7 mg/kg/day | 22.35 mg/kg/day | 8 |
| Blank 1 | Mucolast® | - | - | 12 |
| Blank 2 | PBS | - | - | 10 |
| Formula | Xanthan Gum (%) | Xanthan Gum Hydration Time (h) | Xanthan Gum Hydration Temp (°C) | Viscosity (mPA·s) | G′ Slope | R2 | G′ (0.1 HZ) | Δ | Mucoadhe. Time (min) | Floatability |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2.00 | 2 | 70 | 15,300 | 0.2836 | 0.944 | 8.83 | 1.25 | 400 | NO |
| 2 | 2.00 | 2 | 75 | 12,500 | 0.2037 | 0.852 | 6.33 | 1.41 | NP | NO |
| 3 | 3.00 | 2.5 | 70 | 45,825 | 0.2201 | 0.971 | 76.20 | 0.63 | 238 | NO |
| 4 | 2.50 | 2 | 70 | 11,475 | 0.2183 | 0.924 | 14.57 | 0.93 | 400 | NO |
| Drug | Model | AIC Value | Parameters | Value (Mean ± SD) |
|---|---|---|---|---|
| Amox Low Dose | First-order | 29.0136 | K (h−1) | 0.291 ± 0.091 |
| Higuchi | 28.3848 | Kh (% h−1/2) | 23.862 ± 7.658 | |
| Weibull | 15.2055 | β | 0.610 ± 0.050 | |
| td (h) | 6.063 ± 0.921 | |||
| Kosmeyer–Peppas | 13.2034 | Kk-p (% h−n) | 20.572 ± 1.120 | |
| n | 0.610 ± 0.043 | |||
| Amox High Dose | First-order | 25.8038 | K (h−1) | 0.180 ± 0.064 |
| Higuchi | 34.5868 | Kh (% h−1/2) | 20.576 ± 8.997 | |
| Weibull | 15.6268 | β | 0.716 ± 0.044 | |
| td (h) | 6.223 ± 0.769 | |||
| Kosmeyer–Peppas | 13.6268 | Kk-p (% h−n) | 15.324 ± 1.232 | |
| n | 0.717 ± 0.031 | |||
| Clar Low Dose | First-order | 30.4070 | K (h−1) | 0.376 ± 0.062 |
| Higuchi | 25.7367 | Kh (% h−1/2) | 14.612 ± 2.021 | |
| Weibull | 29.0195 | β | 0.548 ± 0.099 | |
| td (h) | 3.101 ± 1.757 | |||
| Kosmeyer–Peppas | 27.0192 | Kk-p (% h−n) | 13.563 ± 2.884 | |
| n | 0.547 ± 0.091 | |||
| Clar High Dose | First-order | 33.9579 | K (h−1) | 0.419 ± 0.089 |
| Higuchi | 24.7305 | Kh (% h−1/2) | 15.887 ± 1.82 | |
| Weibull | 28.7287 | β | 0.502 ± 0.090 | |
| td (h) | 5.776 ± 1.897 | |||
| Kosmeyer–Peppas | 26.7287 | Kk-p (% h−n) | 15.843 ± 2.061 | |
| n | 0.502 ± 0.100 |
| Group | Tissue | Vehicle | Dose Amox | AUCall Amox (µg mL−1 h−1) | Dose Clar | AUCall Clar (ng mL−1 h−1) |
|---|---|---|---|---|---|---|
| PK 1 | Plasma | Mucolast® | 89.4 mg/kg/day | 75.9 | 44.7 mg/kg/day | 5470.5 |
| PK 2 | Mucolast® | 44.7 mg/kg/day | 63.7 | 22.35 mg/kg/day | 3371.5 | |
| PK 3 | Mucolast® | 8.94 mg/kg/day | 10.7 | 4.47 mg/kg/day | 1083.6 | |
| PK 4 | PBS | 89.4 mg/kg/day | 75.1 | 44.7 mg/kg/day | 5426.0 | |
| PK 5 | PBS | 44.7 mg/kg/day | 26.6 | 22.35 mg/kg/day | 2326.1 | |
| PK 6 | PBS | 8.94 mg/kg/day | 10.2 | 4.47 mg/kg/day | 672.1 |
| Group | Tissue | Vehicle | Dose Amox | AUCall Amox (µg g−1 h−1) | Dose Clar | AUCall Clar (µg g−1 h−1) |
|---|---|---|---|---|---|---|
| PK 1 | Gastric mucosa | Mucolast® | 89.4 mg/kg/day | 10,553.9 | 44.7 mg/kg/day | 3035.7 |
| PK 2 | Mucolast® | 44.7 mg/kg/day | 13,911.2 | 22.35 mg/kg/day | 4158.7 | |
| PK 3 | Mucolast® | 8.94 mg/kg/day | 1079.3 | 4.47 mg/kg/day | 576.4 | |
| PK 4 | PBS | 89.4 mg/kg/day | 206.4 | 44.7 mg/kg/day | 94.0 | |
| PK 5 | PBS | 44.7 mg/kg/day | 78.6 | 22.35 mg/kg/day | 27.7 | |
| PK 6 | PBS | 8.94 mg/kg/day | 31.8 | 4.47 mg/kg/day | 19.4 |
| Group | Tissue | Vehicle | Dose Amox | AUCall Amox (µg g−1 h−1) | Dose Clar | AUCall Clar (µg g−1 h−1) |
|---|---|---|---|---|---|---|
| PK 1 | Stomach | Mucolast® | 89.4 mg/kg/day | 1438.2 | 44.7 mg/kg/day | 169.0 |
| PK 2 | Mucolast® | 44.7 mg/kg/day | 1639.1 | 22.35 mg/kg/day | 557.5 | |
| PK 3 | Mucolast® | 8.94 mg/kg/day | 61.5 | 4.47 mg/kg/day | 84.1 | |
| PK 4 | PBS | 89.4 mg/kg/day | 68.4 | 44.7 mg/kg/day | 34.6 | |
| PK 5 | PBS | 44.7 mg/kg/day | 30.4 | 22.35 mg/kg/day | 14.1 | |
| PK 6 | PBS | 8.94 mg/kg/day | 10.3 | 4.47 mg/kg/day | 3.6 |
| Group | n | CFU/g (mean ± SD) |
|---|---|---|
| Heath control | 5 | 0.00 ± 0.00 |
| H. pylori 2 weeks | 5 | 6.15 ± 0.84 |
| H. pylori 3 weeks | 5 | 6.54 ± 1.10 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Villegas, I.; Rosillo, M.Á.; Alarcón-de-la-Lastra, C.; Vázquez-Román, V.; Llorente, M.; Sánchez, S.; Gil, A.G.; Alcalde, P.; González, E.; Rosell, E.; et al. Amoxicillin and Clarithromycin Mucoadhesive Delivery System for Helicobacter pylori Infection in a Mouse Model: Characterization, Pharmacokinetics, and Efficacy. Pharmaceutics 2021, 13, 153. https://doi.org/10.3390/pharmaceutics13020153
Villegas I, Rosillo MÁ, Alarcón-de-la-Lastra C, Vázquez-Román V, Llorente M, Sánchez S, Gil AG, Alcalde P, González E, Rosell E, et al. Amoxicillin and Clarithromycin Mucoadhesive Delivery System for Helicobacter pylori Infection in a Mouse Model: Characterization, Pharmacokinetics, and Efficacy. Pharmaceutics. 2021; 13(2):153. https://doi.org/10.3390/pharmaceutics13020153
Chicago/Turabian StyleVillegas, Isabel, María Ángeles Rosillo, Catalina Alarcón-de-la-Lastra, Victoria Vázquez-Román, Maria Llorente, Susana Sánchez, Ana Gloria Gil, Pilar Alcalde, Esther González, Elisabet Rosell, and et al. 2021. "Amoxicillin and Clarithromycin Mucoadhesive Delivery System for Helicobacter pylori Infection in a Mouse Model: Characterization, Pharmacokinetics, and Efficacy" Pharmaceutics 13, no. 2: 153. https://doi.org/10.3390/pharmaceutics13020153