
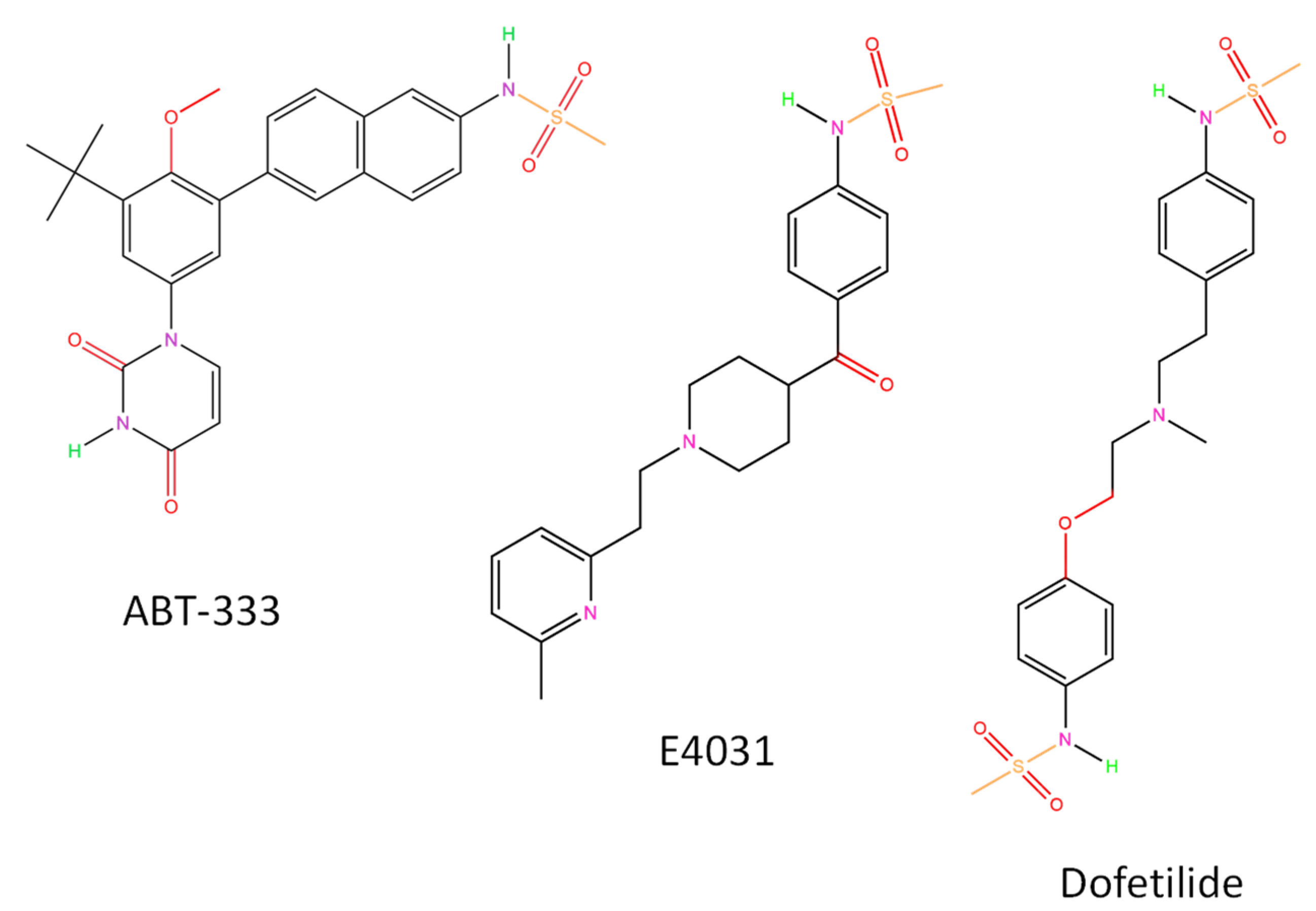
ABT-333 (Dasabuvir) Increases Action Potential Duration and Provokes Early Afterdepolarizations in Canine Left Ventricular Cells via Inhibition of IKr
 , , , and
, , , and
Abstract
:1. Introduction
2. Results
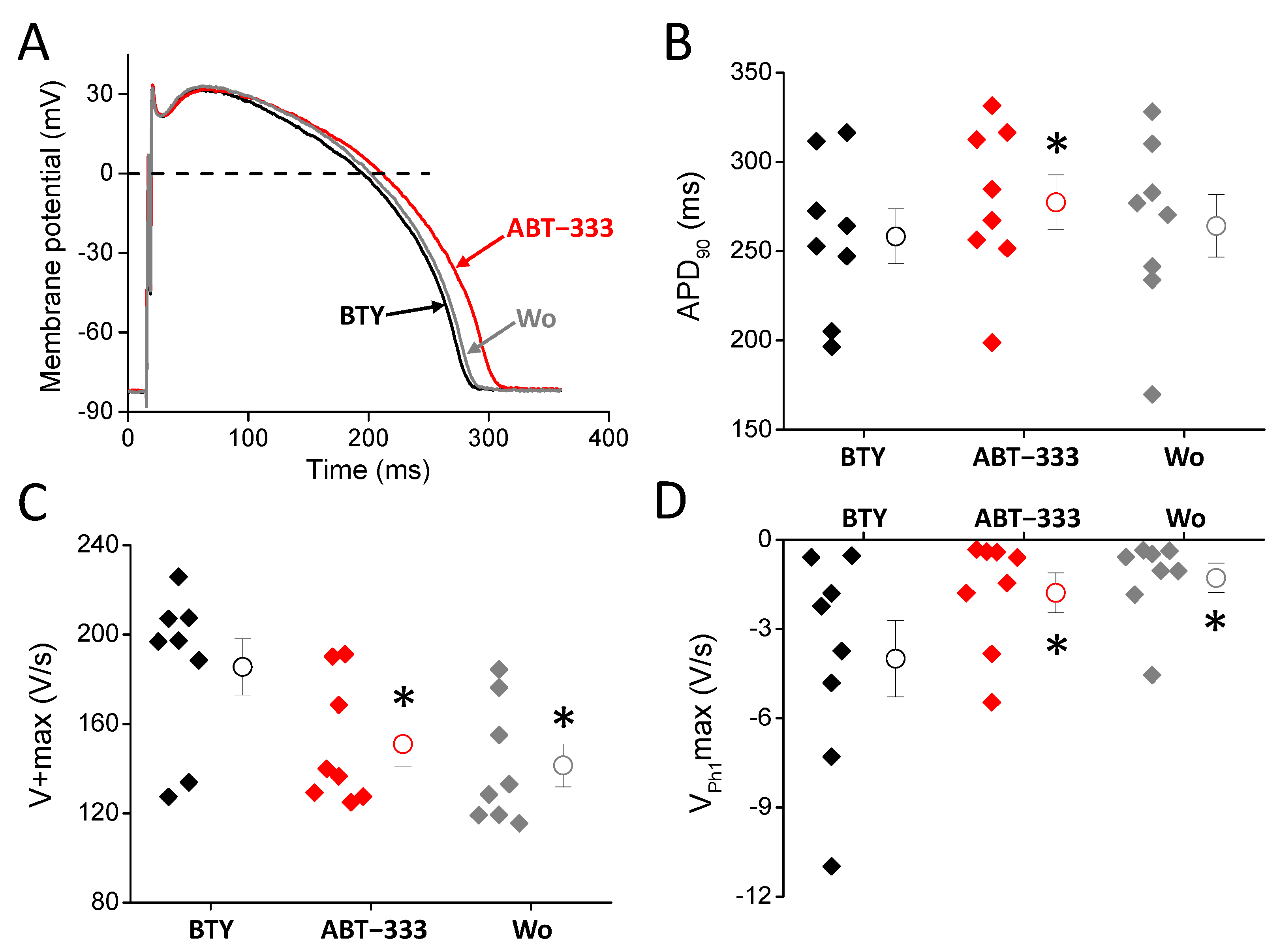
2.1. 1 µM ABT-333 Prolonged the Left Ventricular Action Potential
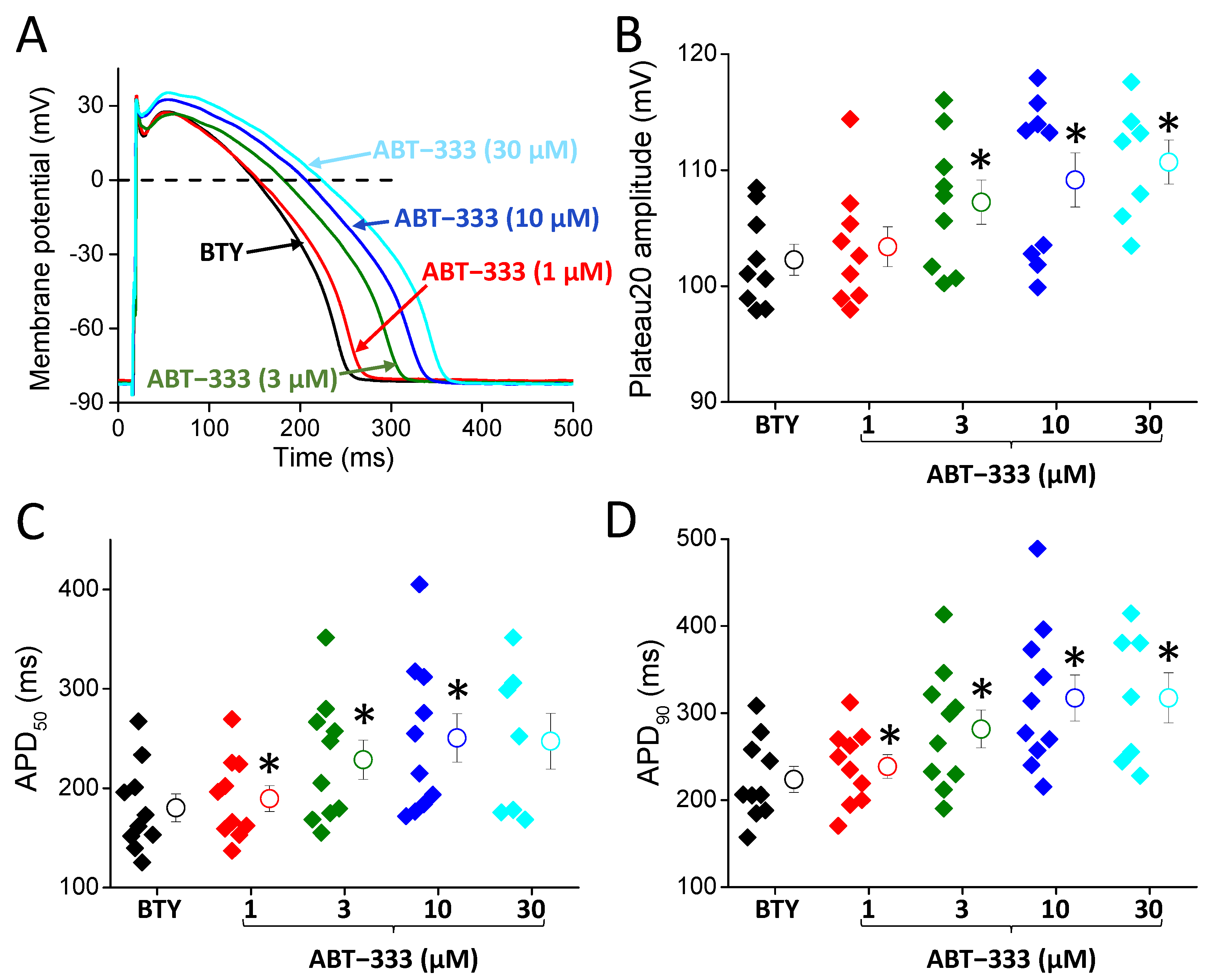
2.2. Concentration Dependent Actions of ABT-333 on the Ventricular Action Potential
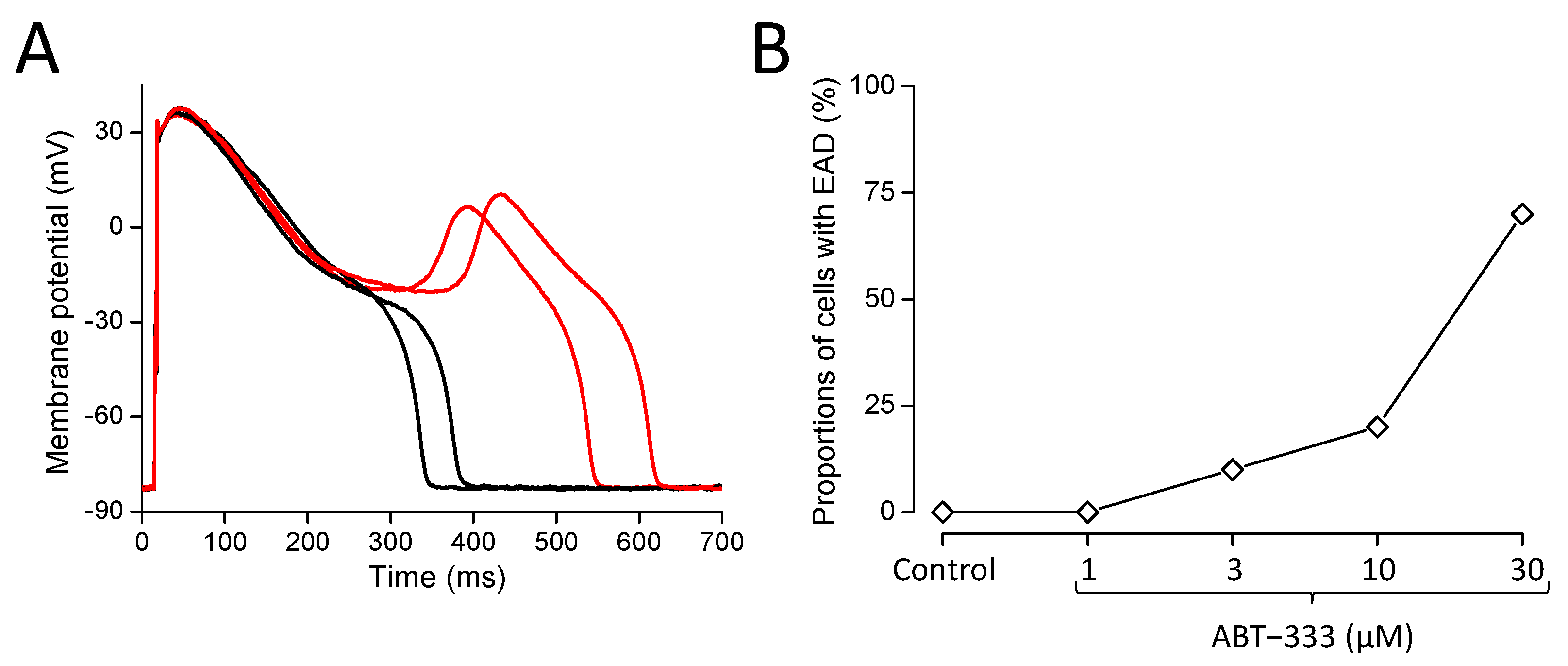
2.3. Development of Early Afterdepolarizations in the Presence of ABT-333
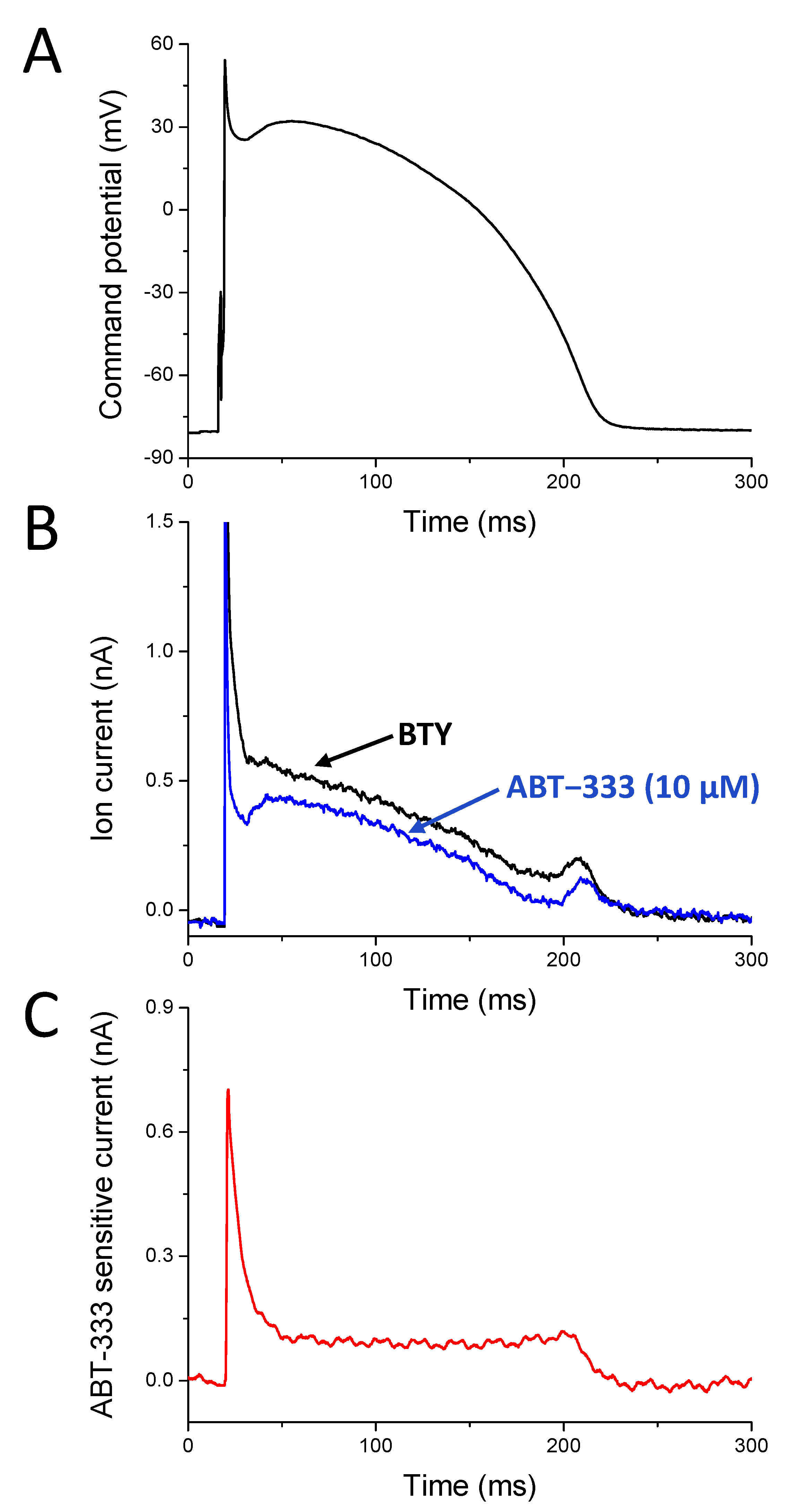
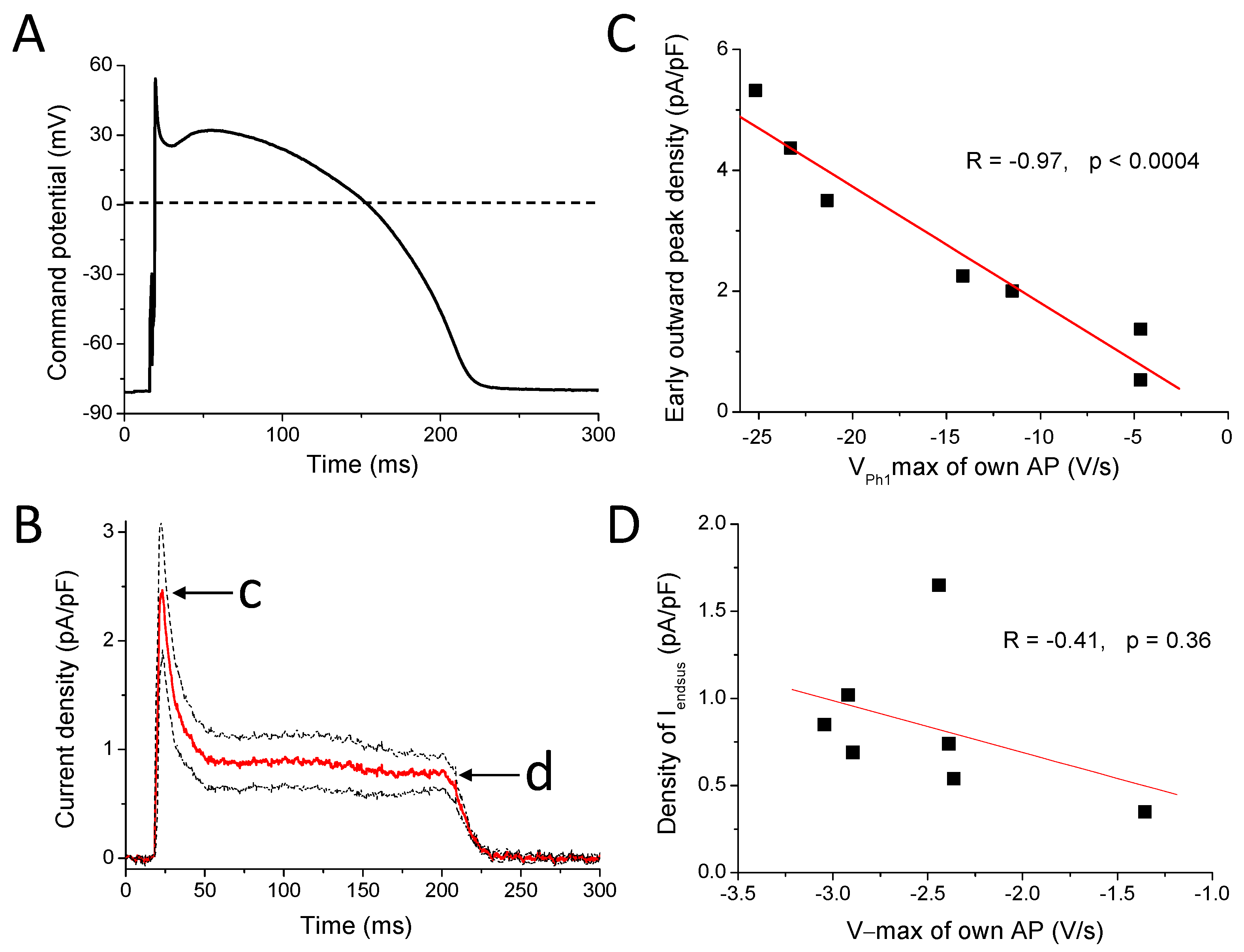
2.4. ABT-333-Sensitive Current Profile with AP Voltage Clamp (APVC)
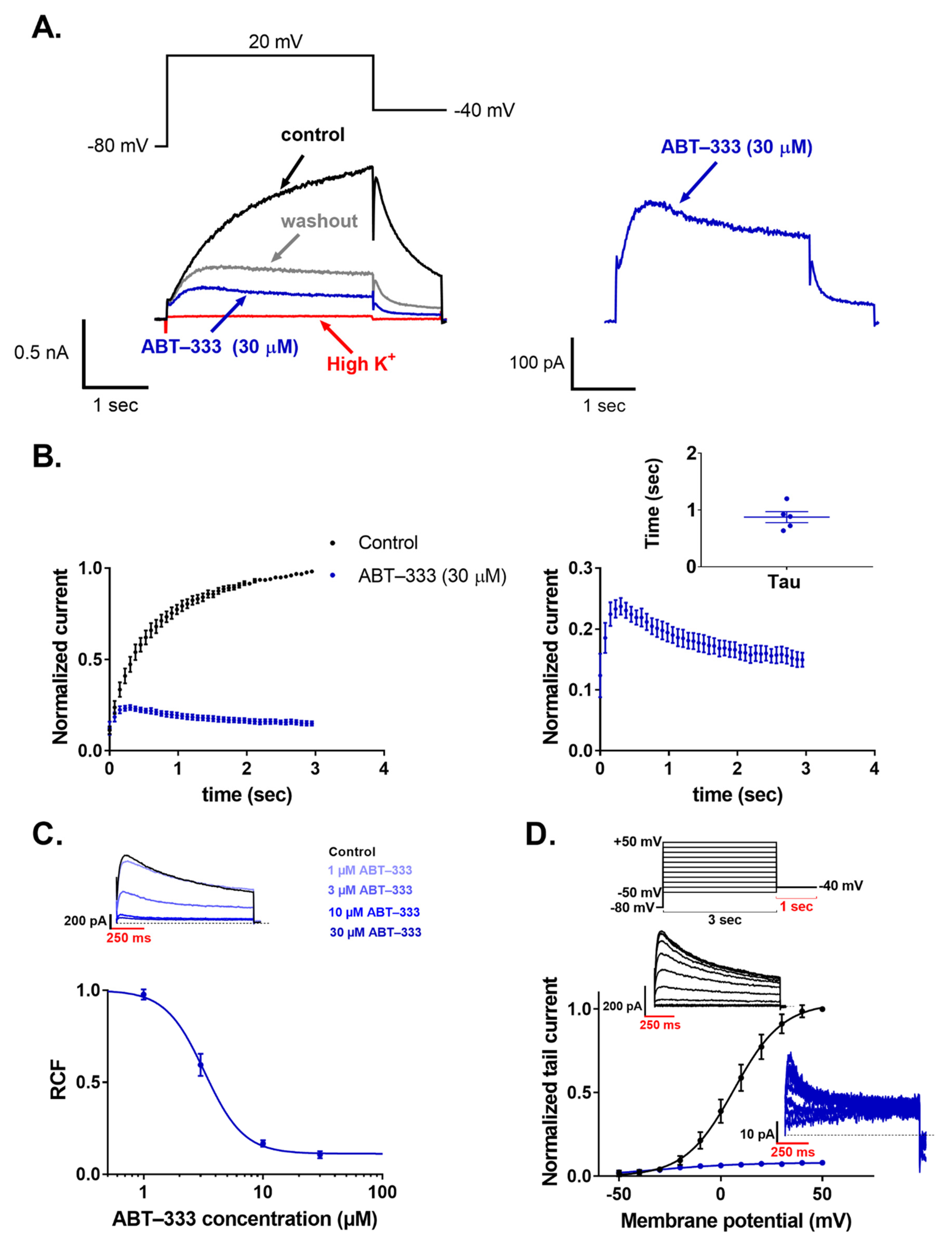
2.5. ABT-333 Blocked Expressed hERG Channels in a Time- and Concentration-Dependent Manner
3. Discussion
3.1. Effects of 1 µM ABT-333
3.2. Actions of Higher Concentrations of ABT-333
3.3. ABT-333-Sensitive Current Profile with APVC
3.4. ABT-333-Induced Reduction of hERG Channel Currents
3.5. Medical Relevance
3.6. Summary and Conclusions
4. Materials and Methods
4.1. Isolation of Canine Ventricular Myocytes
4.2. Electrophysiology
4.3. Recording of Action Potentials
4.4. Action Potential Voltage Clamp (APVC) Studies
4.5. Recording of hERG Currents
4.6. Statistical Analysis
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ABT-333 | another name of the dasabuvir molecule |
| AP | action potential |
| APA | action potential amplitude |
| APD | action potential duration |
| APD50 | action potential duration at 50% of repolarization |
| APD90 | action potential duration at 90% of repolarization |
| APVC | action potential voltage clamp |
| BTY | bicarbonate buffer containing Tyrode solution |
| Cmax | maximal plasma concentration |
| CYP2C8 | cytochrome P450 2C8 enzyme |
| EAD | early afterdepolarization |
| HCV | hepatitis C virus |
| HEK | human embryonic kidney |
| IC50 | half maximal inhibitory concentration |
| Iendsus | end of the ABT-333-sensitive sustained outward current |
| IK1 | inward rectifier potassium current |
| IKr | rapid component of the delayed rectifier potassium current |
| INa | sodium current |
| Ito | transient outward potassium current |
| LQTS2 | long QT syndrome type 2 |
| OSP | overshoot potential |
| VPh1max | maximal rate of phase 1 repolarization |
| Plateau20 amplitude | difference between RMP and membrane potential value of at 20% duration of APD90 |
| Plateau50 amplitude | difference between RMP and membrane potential value of at 50% duration of APD90 |
| RCF | remaining current fraction |
| RMP | resting membrane potential |
| SV | short-term variability of repolarization |
| TdP | torsade de pointes |
| V + max | maximal rate of phase 0 depolarization |
| V − max | maximal rate of phase 3 repolarization |
References
- Bányász, T.; Magyar, J.; Szentandrássy, N.; Horváth, B.; Birinyi, P.; Szentmiklósi, J.; Nánási, P.P. Action potential clamp fingerprints of K+ currents in canine cardiomyocytes: Their role in ventricular repolarization. Acta Physiol. 2007, 190, 189–198. [Google Scholar] [CrossRef]
- Horváth, B.; Kiss, D.; Dienes, C.; Hézső, T.; Kovács, Z.; Szentandrássy, N.; Almássy, J.; Magyar, J.; Bányász, T.; Nánási, P.P. Ion current profiles in canine ventricular myocytes obtained by the “onion peeling” technique. J. Mol. Cell. Cardiol. 2021, 158, 153–162. [Google Scholar] [CrossRef] [PubMed]
- Sanguinetti, M.C.; Zou, A. Molecular physiology of cardiac delayed rectifier K+ channels. Heart Vessel. 1997, (Suppl. S12), 170–172. [Google Scholar]
- Tseng, G.N. I(Kr): The hERG channel. J. Mol. Cell. Cardiol. 2001, 33, 835–849. [Google Scholar] [CrossRef] [PubMed]
- Vaughan Williams, E.M. Classifying antiarrhythmic actions: By facts or speculation. J. Clin. Pharmacol. 1992, 32, 964–977. [Google Scholar] [CrossRef] [PubMed]
- Christophe, B. Occurrence of early afterdepolarization under healthy or hypertrophic cardiomyopathy conditions in the human ventricular endocardial myocyte: In silico study using 109 torsadogenic or non-torsadogenic compounds. Toxicol. Appl. Pharmacol. 2022, 438, 115914. [Google Scholar] [CrossRef]
- Studenik, C.R.; Zhou, Z.; January, C.T. Differences in action potential and early afterdepolarization properties in LQT2 and LQT3 models of long QT syndrome. Br. J. Pharmacol. 2001, 132, 85–92. [Google Scholar] [CrossRef]
- Szentandrássy, N.; Kistamás, K.; Hegyi, B.; Horváth, B.; Ruzsnavszky, F.; Váczi, K.; Magyar, J.; Bányász, T.; Varró, A.; Nánási, P.P. Contribution of ion currents to beat-to-beat variability of action potential duration in canine ventricular myocytes. Pflug. Arch. 2015, 467, 1431–1443. [Google Scholar] [CrossRef] [Green Version]
- Baumert, M.; Porta, A.; Vos, M.A.; Malik, M.; Couderc, J.P.; Laguna, P.; Piccirillo, G.; Smith, G.L.; Tereshchenko, L.G.; Volders, P.G. QT interval variability in body surface ECG: Measurement, physiological basis, and clinical value: Position statement and consensus guidance endorsed by the European Heart Rhythm Association jointly with the ESC Working Group on Cardiac Cellular Electrophysiology. Europace 2016, 18, 925–944. [Google Scholar] [CrossRef]
- Shimizu, W.; Antzelevitch, C. Cellular basis for long QT, transmural dispersion of repolarization, and torsade de pointes in the long QT syndrome. J. Electrocardiol. 1999, 32, 177–184. [Google Scholar] [CrossRef]
- Curran, M.E.; Splawski, I.; Timothy, K.W.; Vincent, G.M.; Green, E.D.; Keating, M.T. A molecular basis for cardiac arrhythmia: HERG mutations cause long QT syndrome. Cell 1995, 80, 795–803. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Plante, I.; Vigneault, P.; Drolet, B.; Turgeon, J. Rosuvastatin blocks hERG current and prolongs cardiac repolarization. J. Pharm. Sci. 2012, 101, 868–878. [Google Scholar] [CrossRef] [PubMed]
- Feng, P.F.; Zhang, B.; Zhao, L.; Fang, Q.; Liu, Y.; Wang, J.N.; Xu, X.Q.; Xue, H.; Li, Y.; Yan, C.C.; et al. Intracellular Mechanism of Rosuvastatin-Induced Decrease in Mature hERG Protein Expression on Membrane. Mol. Pharm. 2019, 16, 1477–1488. [Google Scholar] [CrossRef]
- Thomas, D.; Hammerling, B.C.; Wu, K.; Wimmer, A.B.; Ficker, E.K.; Kirsch, G.E.; Kochan, M.C.; Wible, B.A.; Scholz, E.P.; Zitron, E.; et al. Inhibition of cardiac HERG currents by the DNA topoisomerase II inhibitor amsacrine: Mode of action. Br. J. Pharmacol. 2004, 142, 485–494. [Google Scholar] [CrossRef] [Green Version]
- Droc, G.; Istrate, M.; Mercan-Stanciu, A.; Dodot, M.; Isac, T.; Toma, L.; Zgura, A.; Trifan, A.; Serbanica, A.N.; Iliescu, L.; et al. Safety and Efficacy of Direct-acting Antiviral Therapies for Chronic HCV Infection in Hemodialysis Patients. In Vivo 2022, 36, 2918–2922. [Google Scholar] [CrossRef]
- Gentile, I.; Buonomo, A.R.; Borgia, G. Dasabuvir: A Non-Nucleoside Inhibitor of NS5B for the Treatment of Hepatitis C Virus Infection. Rev. Recent Clin. Trials 2014, 9, 115–123. [Google Scholar] [CrossRef] [PubMed]
- Zeuzem, S.; Jacobson, I.M.; Baykal, T.; Marinho, R.T.; Poordad, F.; Bourlière, M.; Sulkowski, M.S.; Wedemeyer, H.; Tam, E.; Desmond, P.; et al. Retreatment of HCV with ABT-450/r-ombitasvir and dasabuvir with ribavirin. N. Engl. J. Med. 2014, 370, 1604–1614. [Google Scholar] [CrossRef]
- Lavanchy, D. The global burden of hepatitis C. Liver Int. 2009, 29 (Suppl. S1), 74–81. [Google Scholar] [CrossRef]
- Raedler, L.A. Viekira Pak (Ombitasvir, Paritaprevir, and Ritonavir Tablets; Dasabuvir Tablets): All-Oral Fixed Combination Approved for Genotype 1 Chronic Hepatitis C Infection. Am. Health Drug Benefits 2015, 8, 142–147. [Google Scholar]
- Wong, J.B.; McQuillan, G.M.; McHutchison, J.G.; Poynard, T. Estimating future hepatitis C morbidity, mortality, and costs in the United States. Am. J. Public Health 2000, 90, 1562–1569. [Google Scholar] [CrossRef] [Green Version]
- Li, T.; Qu, Y.; Guo, Y.; Wang, Y.; Wang, L. Efficacy and safety of direct-acting antivirals-based antiviral therapies for hepatitis C virus patients with stage 4–5 chronic kidney disease: A meta-analysis. Liver Int. 2017, 37, 974–981. [Google Scholar] [CrossRef] [PubMed]
- Ucciferri, C.; Occhionero, A.; Vecchiet, J.; Falasca, K. Cardiac Toxicity Associated with HCV Direct Antiviral Agents. Mediterr. J. Hematol. Infect. Dis. 2018, 10, e2018069. [Google Scholar] [CrossRef] [PubMed]
- Özer Etik, D.; Suna, N.; Öcal, S.; Selçuk, H.; Dağlı, Ü.; Çolak, T.; Hilmioğlu, F.; Boyacıoğlu, A.S.; Haberal, M. Successful Treatment With Direct-Acting Antiviral Agents of Hepatitis C in Patients With End-Stage Renal Disease and Kidney Transplant Recipients. Exp. Clin. Transpl. 2019, 17, 52–58. [Google Scholar] [CrossRef]
- Pockros, P.J.; Reddy, K.R.; Mantry, P.S.; Cohen, E.; Bennett, M.; Sulkowski, M.S.; Bernstein, D.E.; Cohen, D.E.; Shulman, N.S.; Wang, D.; et al. Efficacy of Direct-Acting Antiviral Combination for Patients With Hepatitis C Virus Genotype 1 Infection and Severe Renal Impairment or End-Stage Renal Disease. Gastroenterology 2016, 150, 1590–1598. [Google Scholar] [CrossRef] [Green Version]
- Stark, J.E. Potential for a Significant Interaction Between Clopidogrel and Dasabuvir. Clin. Infect. Dis. 2015, 61, 134–135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arya, V.; Zhao, P.; Reynolds, K.S.; Mishra, P.; Younis, I.R. Utilizing PBPK Modeling to Evaluate the Potential of a Significant Drug-Drug Interaction Between Clopidogrel and Dasabuvir: A Scientific Perspective. Clin. Pharmacol. Ther. 2017, 102, 578–580. [Google Scholar] [CrossRef] [PubMed]
- Nánási, P.P.; Horváth, B.; Tar, F.; Almássy, J.; Szentandrássy, N.; Jost, N.; Baczkó, I.; Bányász, T.; Varró, A. Canine Myocytes Represent a Good Model for Human Ventricular Cells Regarding Their Electrophysiological Properties. Pharmaceuticals 2021, 14, 748. [Google Scholar] [CrossRef]
- Zygmunt, A.C.; Robitelle, D.C.; Eddlestone, G.T. Ito1 dictates behavior of ICl(Ca) during early repolarization of canine ventricle. Am. J. Physiol. 1997, 273, H1096–H1106. [Google Scholar] [CrossRef]
- Szentandrássy, N.; Nagy, D.; Ruzsnavszky, F.; Harmati, G.; Bányász, T.; Magyar, J.; Szentmiklósi, A.J.; Nánási, P.P. Powerful technique to test selectivity of agents acting on cardiac ion channels: The action potential voltage-clamp. Curr. Med. Chem. 2011, 18, 3737–3756. [Google Scholar] [CrossRef]
- Varró, A.; Tomek, J.; Nagy, N.; Virág, L.; Passini, E.; Rodriguez, B.; Baczkó, I. Cardiac transmembrane ion channels and action potentials: Cellular physiology and arrhythmogenic behavior. Physiol. Rev. 2021, 101, 1083–1176. [Google Scholar] [CrossRef] [PubMed]
- Sanguinetti, M.C.; Jurkiewicz, N.K. Two components of cardiac delayed rectifier K+ current. Differential sensitivity to block by class III antiarrhythmic agents. J. Gen Physiol. 1990, 96, 195–215. [Google Scholar] [CrossRef] [PubMed]
- Kati, W.; Koev, G.; Irvin, M.; Beyer, J.; Liu, Y.; Krishnan, P.; Reisch, T.; Mondal, R.; Wagner, R.; Molla, A.; et al. In vitro activity and resistance profile of dasabuvir, a nonnucleoside hepatitis C virus polymerase inhibitor. Antimicrob. Agents Chemother. 2015, 59, 1505–1511. [Google Scholar] [CrossRef] [Green Version]
- King, J.R.; Khatri, A.; Trinh, R.; Viani, R.M.; Ding, B.; Zha, J.; Menon, R. Pharmacokinetic Evaluation of Darunavir Administered Once or Twice Daily in Combination with Ritonavir or the Three-Direct-Acting Antiviral Regimen of Ombitasvir/Paritaprevir/Ritonavir and Dasabuvir in Adults Coinfected with Hepatitis C and Human Immunodeficiency Viruses. Antimicrob. Agents Chemother. 2017, 61, e02135-16. [Google Scholar] [CrossRef] [Green Version]
- King, J.R.; Zha, J.; Khatri, A.; Dutta, S.; Menon, R.M. Clinical Pharmacokinetics of Dasabuvir. Clin. Pharmacokinet. 2017, 56, 1115–1124. [Google Scholar] [CrossRef] [PubMed]
- Menon, R.M.; Badri, P.S.; Wang, T.; Polepally, A.R.; Zha, J.; Khatri, A.; Wang, H.; Hu, B.; Coakley, E.P.; Podsadecki, T.J.; et al. Drug-drug interaction profile of the all-oral anti-hepatitis C virus regimen of paritaprevir/ritonavir, ombitasvir, and dasabuvir. J. Hepatol. 2015, 63, 20–29. [Google Scholar] [CrossRef] [Green Version]
- Li, M.; Jiang, J.; Yue, L. Functional characterization of homo- and heteromeric channel kinases TRPM6 and TRPM7. J. Gen Physiol. 2006, 127, 525–537. [Google Scholar] [CrossRef] [Green Version]
- Prakriya, M.; Lewis, R.S. Potentiation and inhibition of Ca2+ release-activated Ca2+ channels by 2-aminoethyldiphenyl borate (2-APB) occurs independently of IP3 receptors. J. Physiol. 2001, 536, 3–19. [Google Scholar] [CrossRef]
- Zhou, J.; Augelli-Szafran, C.E.; Bradley, J.A.; Chen, X.; Koci, B.J.; Volberg, W.A.; Sun, Z.; Cordes, J.S. Novel potent human ether-a-go-go-related gene (hERG) potassium channel enhancers and their in vitro antiarrhythmic activity. Mol. Pharmacol. 2005, 68, 876–884. [Google Scholar] [CrossRef]
- Casis, O.; Olesen, S.P.; Sanguinetti, M.C. Mechanism of action of a novel human ether-a-go-go-related gene channel activator. Mol. Pharmacol. 2006, 69, 658–665. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hansen, R.S.; Diness, T.G.; Christ, T.; Wettwer, E.; Ravens, U.; Olesen, S.P.; Grunnet, M. Biophysical characterization of the new human ether-a-go-go-related gene channel opener NS3623 [N-(4-bromo-2-(1H-tetrazol-5-yl)-phenyl)-N′-(3′-trifluoromethylphenyl)urea]. Mol. Pharmacol. 2006, 70, 1319–1329. [Google Scholar] [CrossRef] [Green Version]
- Gerlach, A.C.; Stoehr, S.J.; Castle, N.A. Pharmacological removal of human ether-à-go-go-related gene potassium channel inactivation by 3-nitro-N-(4-phenoxyphenyl) benzamide (ICA-105574). Mol. Pharmacol. 2010, 77, 58–68. [Google Scholar] [CrossRef] [PubMed]
- Su, Z.; Limberis, J.; Souers, A.; Kym, P.; Mikhail, A.; Houseman, K.; Diaz, G.; Liu, X.; Martin, R.L.; Cox, B.F.; et al. Electrophysiologic characterization of a novel hERG channel activator. Biochem. Pharmacol. 2009, 77, 1383–1390. [Google Scholar] [CrossRef] [PubMed]
- Hamill, O.P.; Marty, A.; Neher, E.; Sakmann, B.; Sigworth, F.J. Improved patch-clamp techniques for high-resolution current recording from cells and cell-free membrane patches. Pflug. Arch. 1981, 391, 85–100. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | BTY (Control) | 1 μM ABT-333 | Washout |
|---|---|---|---|
| APA (mV) | 108.9 ± 2.5 | 106.4 ± 3.0 | 105.7 ± 3.6 |
| APD50 (ms) | 220.0 ± 13.1 | 236.7 ± 13.3 | 225.5 ± 15.0 |
| APD90 (ms) | 258.3 ± 15.4 | 277.4 ± 15.3 | 264.2 ± 17.5 |
| APD50/APD90 | 0.85 ± 0.01 | 0.85 ± 0.01 | 0.85 ± 0.01 |
| OSP (mV) | 17.6 ± 2.0 | 13.7 ± 3.0 | 12.0 ± 3.4 |
| VPh1max (V/s) | −4.00 ± 1.28 | −1.79 ± 0.67 | −1.29 ± 0.50 |
| Plateau20 amplitude (mV) | 106.6 ± 1.9 | 107.3 ± 2.4 | 107.0 ± 2.5 |
| Plateau50 amplitude (mV) | 90.0 ± 2.0 | 89.1 ± 2.3 | 89.2 ± 2.5 |
| RMP (mV) | −81.2 ± 1.4 | −82.6 ± 1.6 | −83.7 ± 1.3 |
| V + max (V/s) | 185.6 ± 12.6 | 151.0 ± 9.9 | 141.4 ± 9.6 |
| V − max (V/s) | −1.72 ± 0.08 | −1.64 ± 0.07 | −1.65 ± 0.08 |
| Parameter | BTY (Control) | ABT-333 (1 μM) | ABT-333 (3 μM) | ABT-333 (10 μM) | ABT-333 (30 μM) |
|---|---|---|---|---|---|
| APA (mV) | 115.9 ± 2.5 | 115.6 ± 2.4 | 117.0 ± 2.6 | 117.5 ± 2.5 | 115.9 ± 1.6 |
| APD50 (ms) | 198.8 ± 14.4 | 213.8 ± 14.2 | 252.2 ± 22.5 | 273.9 ± 25.3 | 284.3 ± 29.4 |
| APD90 (ms) | 223.8 ± 14.9 | 238.6 ± 13.6 | 281.7 ± 21.7 | 317.4 ± 26.5 | 317.5 ± 28.7 |
| APD50/APD90 | 0.80 ± 0.01 | 0.79 ± 0.02 | 0.81 ± 0.01 | 0.78 ± 0.02 | 0.77 ± 0.02 |
| OSP (mV) | 32.6 ± 2.7 | 31.3 ± 2.9 | 31.9 ± 2.9 | 33.3 ± 2.7 | 32.7 ± 2.5 |
| VPh1max (V/s) | −7.44 ± 1.47 | −6.69 ± 1.40 | −5.99 ± 1.37 | −4.21 ± 1.01 | −3.63 ± 1.15 |
| Plateau20 amplitude (mV) | 102.3 ± 1.2 | 103.4 ± 1.5 | 106.8 ± 1.8 | 108.6 ± 2.2 | 110.7 ± 1.9 |
| Plateau50 amplitude (mV) | 84.9 ± 1.2 | 84.5 ± 2.2 | 86.3 ± 1.5 | 84.4 ± 2.6 | 83.6 ± 2.5 |
| RMP (mV) | −81.3 ± 1.2 | −82.3 ± 1.6 | −83.0 ± 1.1 | −82.2 ± 1.2 | −83.1 ± 1.8 |
| V + max (V/s) | 189.6 ± 22.6 | 169.5 ± 18.0 | 167.4 ± 15.1 | 152.4 ± 14.3 | 123.5 ± 21.0 |
| V − max (V/s) | −1.78 ± 0.08 | −1.71 ± 0.09 | −1.69 ± 0.07 | −1.53 ± 0.07 | −1.42 ± 0.09 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kovács, Z.M.; Óvári, J.; Dienes, C.; Magyar, J.; Bányász, T.; Nánási, P.P.; Horváth, B.; Feher, A.; Varga, Z.; Szentandrássy, N. ABT-333 (Dasabuvir) Increases Action Potential Duration and Provokes Early Afterdepolarizations in Canine Left Ventricular Cells via Inhibition of IKr. Pharmaceuticals 2023, 16, 488. https://doi.org/10.3390/ph16040488
Kovács ZM, Óvári J, Dienes C, Magyar J, Bányász T, Nánási PP, Horváth B, Feher A, Varga Z, Szentandrássy N. ABT-333 (Dasabuvir) Increases Action Potential Duration and Provokes Early Afterdepolarizations in Canine Left Ventricular Cells via Inhibition of IKr. Pharmaceuticals. 2023; 16(4):488. https://doi.org/10.3390/ph16040488
Chicago/Turabian StyleKovács, Zsigmond Máté, József Óvári, Csaba Dienes, János Magyar, Tamás Bányász, Péter P. Nánási, Balázs Horváth, Adam Feher, Zoltan Varga, and Norbert Szentandrássy. 2023. "ABT-333 (Dasabuvir) Increases Action Potential Duration and Provokes Early Afterdepolarizations in Canine Left Ventricular Cells via Inhibition of IKr" Pharmaceuticals 16, no. 4: 488. https://doi.org/10.3390/ph16040488