Impact of Immunoglobulin M-Type Donor-Specific Human Leukocyte Antigen–Antibody Levels in Supernatants from Cultured Peripheral Blood Mononuclear Cells as Predictors of Antibody-Mediated Rejection

Abstract
:1. Introduction
2. Results
2.1. Participants Characteristics
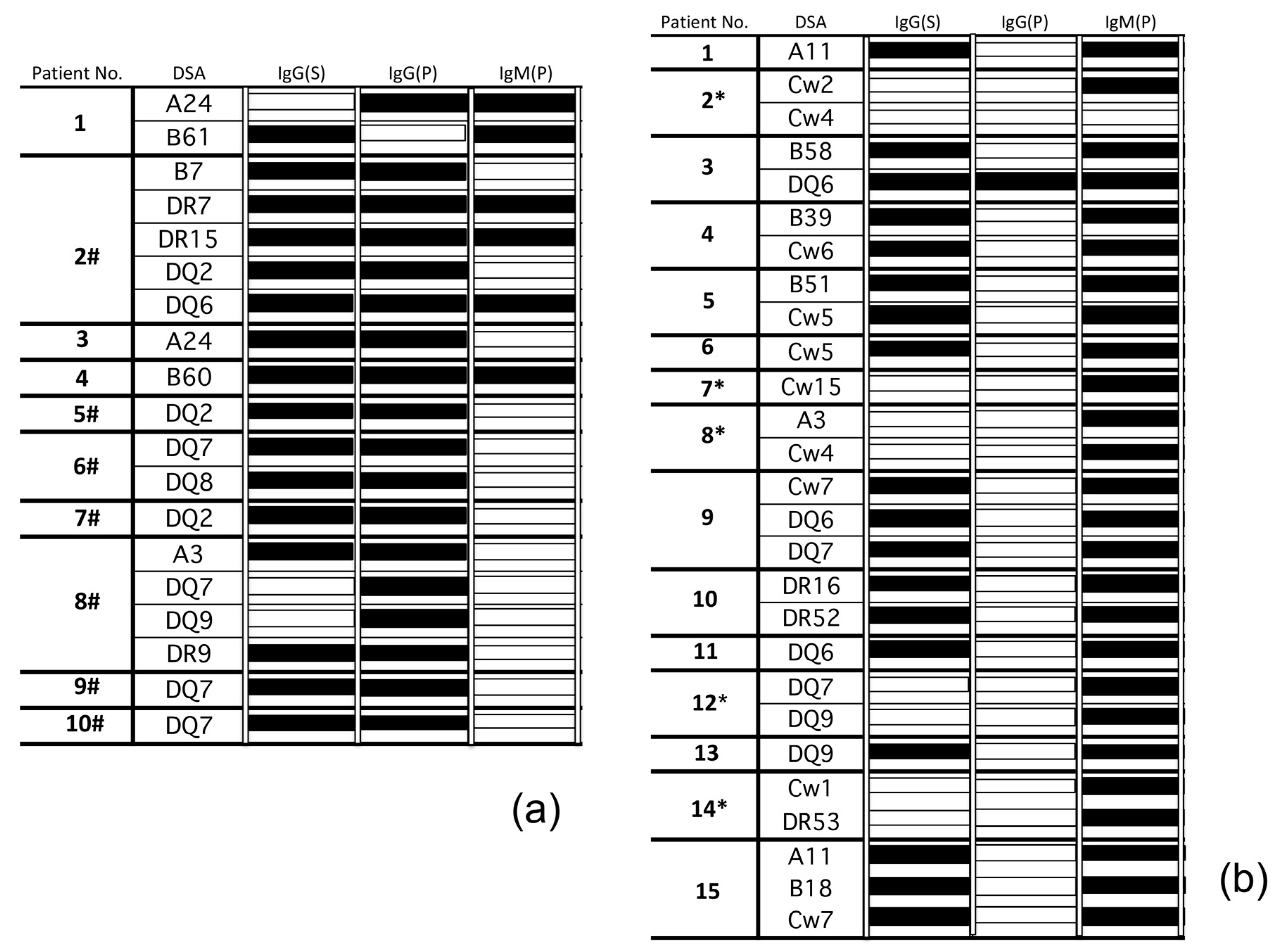
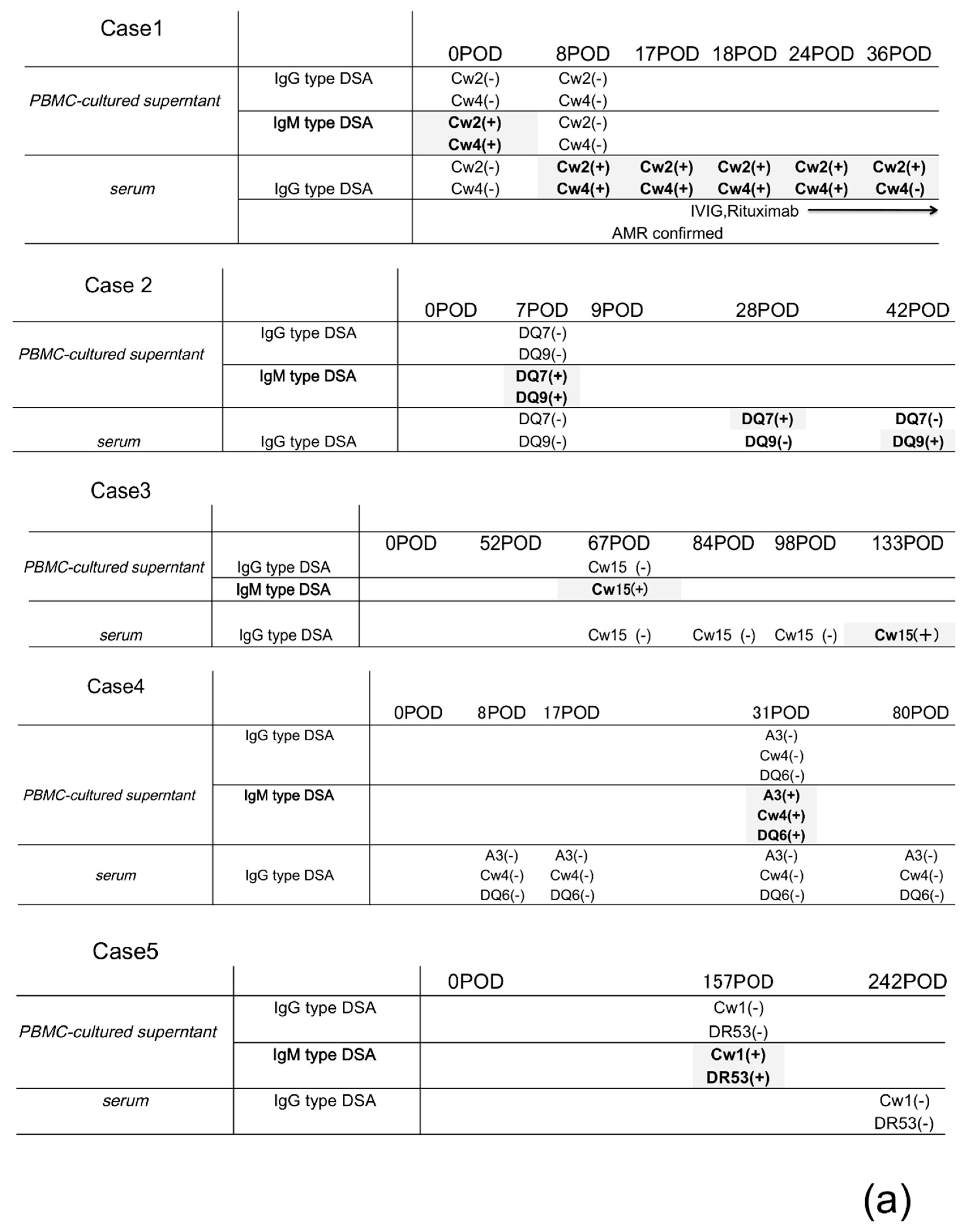
2.2. Isotypes (IgG or IgM) of DSAs Produced from PBMC Culture Supernatants Reflect the Activation Level of Humoral Immune Responses against Donor-Specific Antigen; Several IgM DSAs May Be a Precursor of the Production of IgG DSAs in the Patient Sera
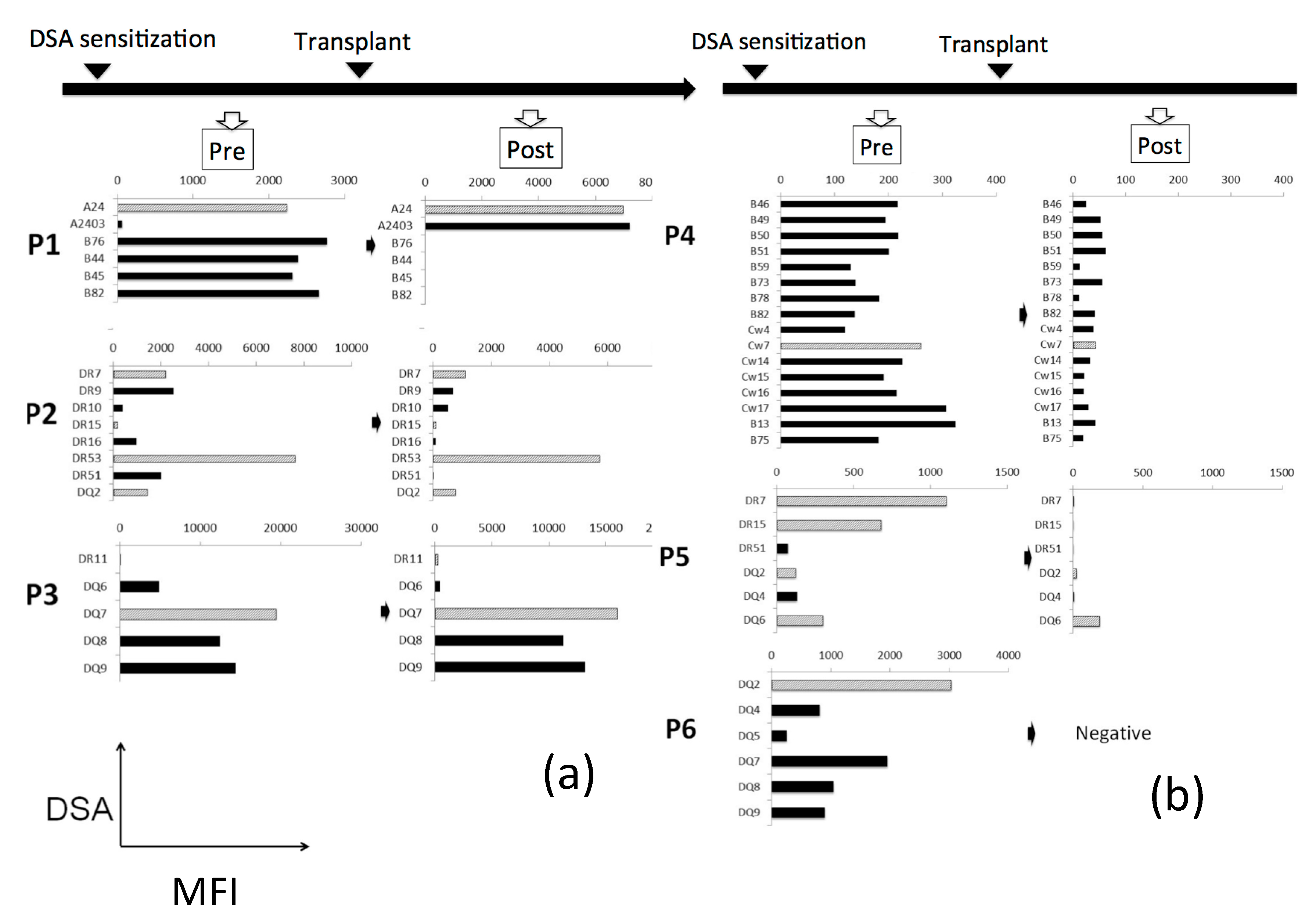
2.3. IgM-Secreting mBCs Are More Sensitive to the Standard Immunosuppressive Therapy Than IgG-Secreting mBCs
3. Discussion
4. Materials and Methods
4.1. Isolation and Culture of PBMCs
4.2. Reagents
4.3. Detection of HLA Antibodies in the Culture Supernatants
4.4. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Aubert, O.; Loupy, A.; Hidalgo, L.; van Huyen, J.P.D.; Higgins, S.; Viglietti, D.; Jouven, X.; Glotz, D.; Legendre, C.; Lefaucheur, C.; et al. Antibody-Mediated Rejection Due to Preexisting versus De Novo Donor-Specific Antibodies in Kidney Allograft Recipients. J. Am. Soc. Nephrol. 2017, 28, 1912–1923. [Google Scholar] [CrossRef] [Green Version]
- Kim, Y.C.; Yu, M.Y.; Lee, J.P.; Lee, H.; Min, S.I.; Ha, J.; Kim, Y.S. The effect of desensitization therapy in kidney transplantation. Clin. Exp. Nephrol. 2018, 22, 179–187. [Google Scholar] [CrossRef] [PubMed]
- Shaffer, D.; Feurer, I.D.; Crowe, D.; Schaefer, H. Early and Sustained Reduction in Donor-Specific Antibodies in Desensitized Living Donor Kidney Transplant Recipients: A 3-Year Prospective Study. Transplant. Direct 2016, 11, 2. [Google Scholar] [CrossRef] [PubMed]
- De Silva, N.S.; Klein, U. Dynamics of B cells in germinal centres. Nat. Rev. Immunol. 2015, 15, 137–148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McHeyzer-Williams, L.J.; Malherbe, L.P.; McHeyzer-Williams, M.G. Helper T cell-regulated B cells immunity. Curr. Top. Microbiol. Immunol. 2006, 311, 59–83. [Google Scholar]
- Marrari, M.; Duquesnoy, R.J. Detection of donor-specific HLA antibodies before and after removal of a rejected kidney transplant. Transpl. Immunol. 2010, 22, 105–109. [Google Scholar] [CrossRef]
- Radbruch, A.; Muehlinghaus, G.; Luger, E.O.; Inamine, A.; Smith, K.G.; Dörner, T.; Hiepe, F. Competence and competition: The challenge of becoming a long-lived plasma cell. Nat. Rev. Immunol. 2006, 6, 741–750. [Google Scholar] [CrossRef]
- Yoshiko, M.; Minnie, M.S. Unraveling the Role of Allo-Antibodies and Transplant Injury. Front. Immunol. 2016, 7, 432. [Google Scholar]
- Toyoda, M.; Shin, B.H.; Ge, S.; Mirocha, J.; Thomas, D.; Chu, M.; Rodriguez, E.; Chao, C.; Petrosyan, A.; Galera, O.A.; et al. Impact of Desensitization on Antiviral Immunity in HLA-Sensitized Kidney Transplant Recipients. J. Immunol. Res. 2017, 2017, 5672523. [Google Scholar] [CrossRef]
- Lúcia, M.; Luque, S.; Crespo, E.; Melilli, E.; Cruzado, J.M.; Martorell, J.; Jarque, M.; Gil-Vernet, S.; Manonelles, A.; Grinyó, J.M.; et al. Preformed circulating HLA-specific memory B cells predict high risk of humoral rejection in kidney transplantation. Kidney Int. 2015, 88, 874–887. [Google Scholar] [CrossRef] [Green Version]
- Lynch, R.J.; Silva, I.A.; Chen, B.J.; Punch, J.D.; Cascalho, M.; Platt, J.L. Cryptic B cell response to renal transplantation. Am. J. Transplant. 2013, 13, 1713–1723. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Terasaki, P.I.; Cai, J. Human leukocyte antigen antibodies and chronic rejection: From association to causation. Transplantation 2008, 86, 377–383. [Google Scholar] [CrossRef] [PubMed]
- Lee, P.C.; Terasaki, P.I.; Takemoto, S.K.; Lee, P.H.; Hung, C.J.; Chen, Y.L.; Tsai, A.; Lei, H.Y. All chronic rejection failures of kidney transplants were preceded by the development of HLA antibodies. Transplantation 2002, 74, 1192–1194. [Google Scholar] [CrossRef] [PubMed]
- Key, T.; Watson, C.J.; Clatworthy, M.R.; O’Rourke, C.M.; Goodman, R.S.; Taylor, C.J.; Butler, A.J. The kinetics of donor HLA class I-specific antibody absorption following a combined split liver and kidney transplant. NDT Plus 2010, 3, 579–581. [Google Scholar] [CrossRef] [PubMed]
- Heidt, S.; Roelen, D.L.; de Vaal, Y.J.; Kester, M.G.; Eijsink, C.; Thomas, S.; van Besouw, N.M.; Volk, H.D.; Weimar, W.; Claas, F.H.; et al. A NOVel ELISPOT assay to quantify HLA-specific B cells in HLA-immunized individuals. Am. J. Transplant. 2012, 12, 1469–1478. [Google Scholar] [CrossRef]
- Han, M.; Rogers, J.A.; Lavingia, B.; Stastny, P. Peripheral blood B cells producing donor-specific HLA antibodies in vitro. Hum. Immunol. 2009, 70, 29–34. [Google Scholar] [CrossRef]
- Bellatin, M.F.; Han, M.; Fallena, M.; Fan, L.; Xia, D.; Olsen, N.; Branch, V.; Karp, D.; Stastny, P. Production of autoantibodies against citrullinated antigens/peptides by human B cells. J. Immunol. 2012, 188, 3542–3550. [Google Scholar] [CrossRef] [Green Version]
- Weber, M.; Weiss, E.; Engel, A.M. Combining EL4-B5-based B-cell stimulation and phage display technology for the successful isolation of human anti-Scl-70 autoantibody fragments. J. Immunol. Methods 2003, 278, 249–259. [Google Scholar] [CrossRef]
- Einecke, G.; Sis, B.; Reeve, J.; Mengel, M.; Campbell, P.M.; Hidalgo, L.G.; Kaplan, B.; Halloran, P.F. Antibody-Mediated microcirculation injury is the major cause of late kidney transplant failure. Am. J. Transplant. 2009, 9, 2520–2531. [Google Scholar] [CrossRef]
- Piazza, A.; Poggi, E.; Borrelli, L.; Servetti, S.; Monaco, P.I.; Buonomo, O.; Valeri, M.; Torlone, N.; Adorno, D.; Casciani, C.U. Impact of donor-specific antibodies on chronic rejection occurrence and graft loss in renal transplantation: Posttransplant analysis using flow cytometric techniques. Transplantation 2001, 71, 1106–1112. [Google Scholar] [CrossRef] [Green Version]
- Lefaucheur, C.; Suberbielle-Boissel, C.; Hill, G.S.; Nochy, D.; Andrade, J.; Antoine, C.; Gautreau, C.; Charron, D.; Glotz, D. Clinical Relevance of Preformed HLA Donor-Specific Antibodies in Kidney Transplantation. Am. J. Transplant. 2008, 8, 324–331. [Google Scholar] [CrossRef] [PubMed]
- Tangye, S.G. Staying alive: Regulation of plasma cell survival. Trends Immunol. 2011, 32, 595–602. [Google Scholar] [CrossRef] [PubMed]
- Pani, G.; Kozlowski, M.; Cambier, J.C.; Mills, G.B.; Siminovitch, K.A. Identification of the tyrosine phosphatase PTP1C as a B cell antigen receptor-associated protein involved in the regulation of B cell signaling. J. Exp. Med. 1995, 181, 2077–2084. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bryant, V.L.; Ma, C.S.; Avery, D.T.; Li, Y.; Good, K.L.; Corcoran, L.M.; de Waal Malefyt, R.; Tangye, S.G. Cytokine-Mediated regulation of human B cell differentiation into Ig-secreting cells: Predominant role of IL-21 produced by CXCR5+ T follicular helper cells. J. Immunol. 2007, 179, 8180–8190. [Google Scholar] [CrossRef] [Green Version]
- Rydyznski, C.; Daniels, K.A.; Karmele, E.P.; Brooks, T.R.; Mahl, S.E.; Moran, M.T.; Li, C.; Sutiwisesak, R.; Welsh, R.M.; Waggoner, S.N. Generation of cellular immune memory and B-cell immunity is impaired by natural killer cells. Nat. Commun. 2015, 6, 6375. [Google Scholar] [CrossRef] [Green Version]
- Sala, E.; Kuka, M. The Suppressive Attitude of Inflammatory Monocytes in Antiviral Antibody Responses. Viral Immunol. 2020, 33, 327–333. [Google Scholar] [CrossRef]
- Ayroldi, E.; Cannarile, L.; Migliorati, G.; Riccardi, C. PMA inhibits NK cell generation, cytotoxic activity and NK-1.1 expression. Int. J. Immunopharmacol. 1993, 15, 11–17. [Google Scholar] [CrossRef]
- Burger, D.; Dayer, J.M. The role of human T-lymphocyte-monocyte contact in inflammation and tissue destruction. Arthritis Res. 2002, 4 (Suppl. S3), S169–S176. [Google Scholar] [CrossRef]
- Seifert, M.; Przekopowitz, M.; Taudien, S.; Lollies, A.; Ronge, V.; Drees, B.; Lindemann, M.; Hillen, U.; Engler, H.; Singer, B.B.; et al. Functional capacities of human IgM memory B cells in early inflammatory responses and secondary germinal center reactions. Proc. Natl. Acad. Sci. USA 2015, 112, E546–E555. [Google Scholar] [CrossRef] [Green Version]
- Morales-Buenrostro, L.E.; Terasaki, P.I.; Marino-Vázquez, L.A.; Lee, J.H. Natural human leukocyte antigen antibodies found in nonalloimmunized healthy males. Transplantation 2008, 86, 1111–1115. [Google Scholar] [CrossRef]
- Pozsonyi, E.; György, B.; Berki, T.; Bánlaki, Z.; Buzás, E.; Rajczy, K.; Hossó, A.; Prohászka, Z.; Szilágyi, A.; Cervenak, L.; et al. HLA-Association of serum levels of natural antibodies. Mol. Immunol. 2009, 46, 1416–1423. [Google Scholar] [CrossRef] [PubMed]
- Urlacher, A.; Tongio, M.M.; Pasquali, J.L. IgM anti-idiotypes that block anti-HLA antibodies: Naturally occurring or immune antibodies? Clin. Exp. Immunol. 1991, 83, 116–120. [Google Scholar] [CrossRef] [PubMed]
- Kosmoliaptsis, V.; Bradley, J.A.; Peacock, S.; Chaudhry, A.N.; Taylor, C.J. Detection of immunoglobulin G human leukocyte antigen-specific alloantibodies in renal transplant patients using single-antigen-beads is compromised by the presence of immunoglobulin M human leukocyte antigen-specific alloantibodies. Transplantation 2009, 87, 813–820. [Google Scholar] [CrossRef] [PubMed]
- Yoshiko, M.; Ryoich, I.; Shiro, T. Evaluation of Antigen-Specific IgM and IgG Production during an In Vitro Peripheral Blood Mononuclear Cell Culture Assay. Front. Immunol. 2017, 8, 794. [Google Scholar]
- Wiebe, C.; Gibson, I.W.; Blydt-Hansen, T.D.; Pochinco, D.; Birk, P.E.; Ho, J.; Karpinski, M.; Goldberg, A.; Storsley, L.; Rush, D.N.; et al. Rates and determinants of progression to graft failure in kidney allograft recipients with de novo donor-specific antibody. Am. J. Transplant. 2015, 15, 2921–2930. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Graft function Stable (N = 10) | AMR Confirmed (N = 7) | Non-DSA Sensitized (N = 12) | HLA Non-Sensitized (N = 10) | p-Value | |
|---|---|---|---|---|---|---|
| Gender (Male/Female) | N (%) | 4(40%)/6(60%) | 5(71.4%)/2(28.6%) | 6(50%)/6(50%) | 5(50%)/5(50%) | N.S |
| Age at transplant (Year) | Mean ± SD | 48.8 ± 9.6 | 41.6 ± 19.0 | 49.8 ± 11.4 | 36.8 ± 15.9 | N.S |
| ABO compatibility (Compatible/Incompatible) | N (%) | 10(100%)/0(0%) | 7(100%)/0(0%) | 11(91.7%)/1(8.3%) | 9(90.0%)/1(10%) | N.S |
| Immunosuppression | ||||||
| Maint. Pred (Yes/No) | N (%) | 10(100%)/0(0%) | 7(100%)/0(0%) | 11(91.7%)/1(8.3%) | 7(70%)/3(30%) | N.S |
| 1 = Tac, 2 = CyA | N (%) | 10(100%)/0(0%) | 7(100%)/0(0%) | 12(100%)/0(0%) | 10/(100%)/0(0%) | N.S |
| 1 = MMF, 2 = MZ | N (%) | 10(100%)/0(0%) | 7(100%)/0(0%) | 12(100%)/0(0%) | 10/(100%)/0(0%) | N.S |
| Kidney biopsy | ||||||
| g + ptc | Mean ± SD | 0.83 ± 0.69 | 3.5 ± 1.0 | <0.001 *** | ||
| C4d (0–3) | Mean ± SD | 0.33 ± 0.75 | 2.0 ± 1.22 | <0.05 * |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Imamura, R.; Matsuda, Y.; Tsutahara, K.; Nonomura, N.; Takahara, S. Impact of Immunoglobulin M-Type Donor-Specific Human Leukocyte Antigen–Antibody Levels in Supernatants from Cultured Peripheral Blood Mononuclear Cells as Predictors of Antibody-Mediated Rejection. Pathogens 2020, 9, 733. https://doi.org/10.3390/pathogens9090733
Imamura R, Matsuda Y, Tsutahara K, Nonomura N, Takahara S. Impact of Immunoglobulin M-Type Donor-Specific Human Leukocyte Antigen–Antibody Levels in Supernatants from Cultured Peripheral Blood Mononuclear Cells as Predictors of Antibody-Mediated Rejection. Pathogens. 2020; 9(9):733. https://doi.org/10.3390/pathogens9090733
Chicago/Turabian StyleImamura, Ryoichi, Yoshiko Matsuda, Koichi Tsutahara, Norio Nonomura, and Shiro Takahara. 2020. "Impact of Immunoglobulin M-Type Donor-Specific Human Leukocyte Antigen–Antibody Levels in Supernatants from Cultured Peripheral Blood Mononuclear Cells as Predictors of Antibody-Mediated Rejection" Pathogens 9, no. 9: 733. https://doi.org/10.3390/pathogens9090733