Prevalence of Helicobacter pylori and Its Associated Factors among Healthy Asymptomatic Residents in the United Arab Emirates

 , , , and
, , , and
Abstract
:1. Introduction
2. Results
2.1. Socio-Demographic and Lifestyle Characteristics
2.2. Gastrointestinal Characteristics
2.3. Prevalence of H. pylori Infection in Asymptomatic Healthy UAE Residents
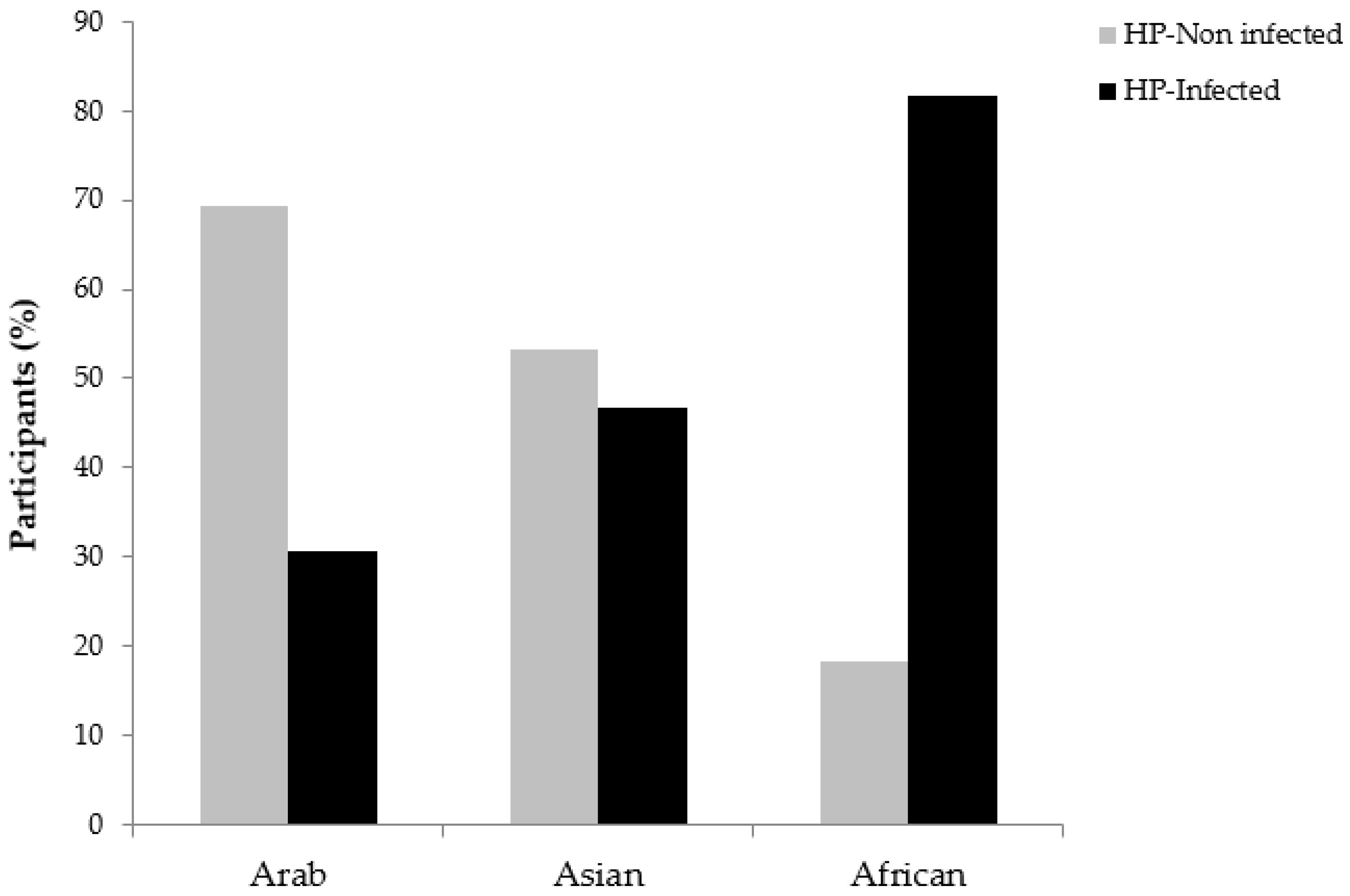
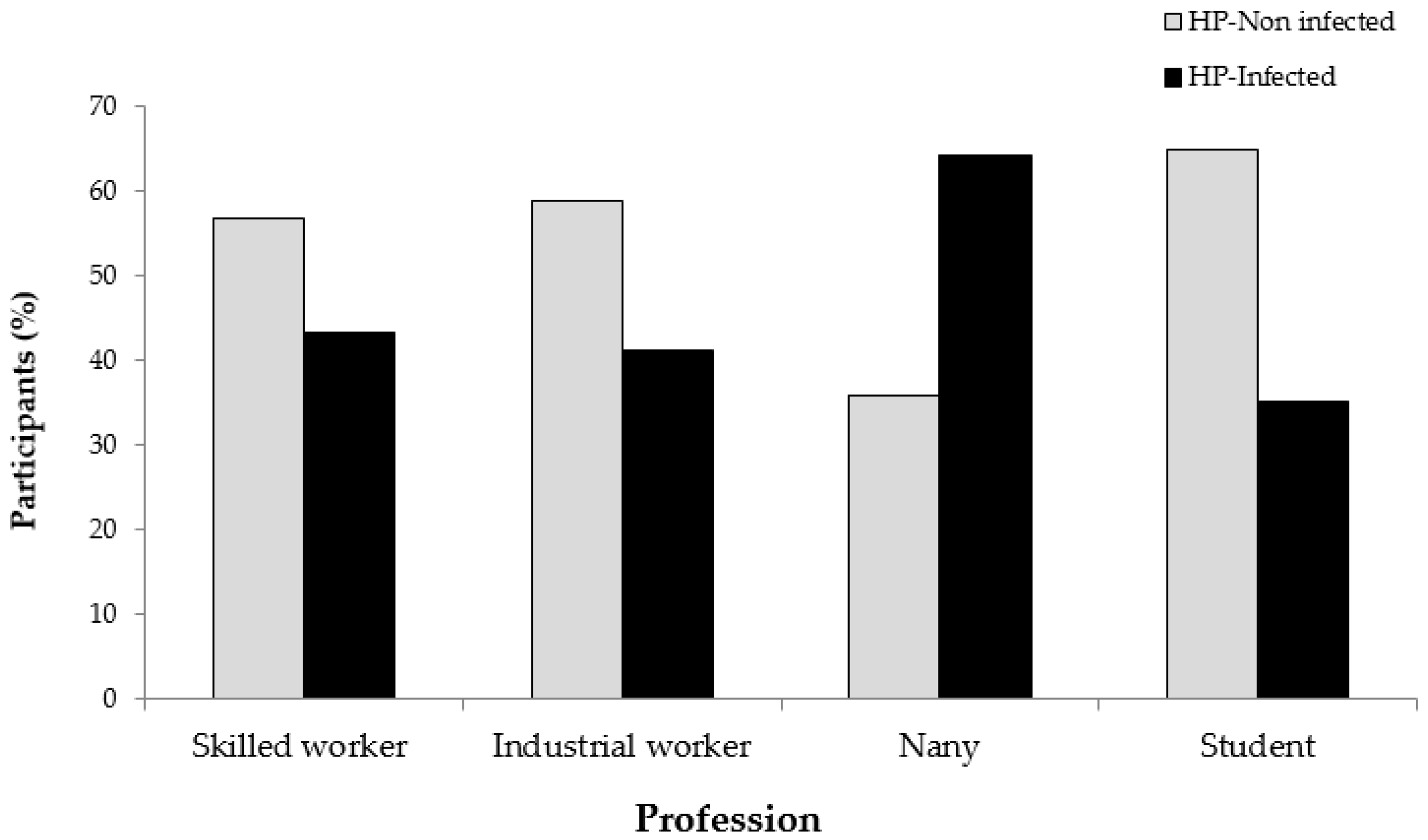
2.4. Association Between H. pylori Infection and Socio-Demographic, Lifestyle and Gastrointestinal Characteristics
3. Discussion
4. Materials and Methods
4.1. Ethical Statement
4.2. Study Design
4.3. H. pylori Stool Antigen Test (Premier Platinum HpSA)
4.4. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- ReferencesHooi, J.K.Y.; Lai, W.Y.; Ng, W.K.; Suen, M.M.Y.; Underwood, F.E.; Tanyingoh, D.; Malfertheiner, P.; Graham, D.Y.; Wong, V.W.S.; Wu, J.C.Y.; et al. Global Prevalence of Helicobacter pylori Infection: Systematic Review and Meta-Analysis. Gastroenterology 2017, 153, 420–429. [Google Scholar] [CrossRef]
- Cover, T.L.; Blaser, M.J. Helicobacter pylori in health and disease. Gastroenterology 2009, 136, 1863–1873. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muhammad, J.S.; Sugiyama, T.; Zaidi, S.F. Gastric pathophysiological ins and outs of helicobacter pylori: A review. J. Pak. Med. Assoc. 2013, 63, 1528–1533. [Google Scholar]
- International Agency for Research on Cancer (IARC). Schistosomes, Liver Flukes and Helicobacter Pylori; IARC: Lyon, France, 1994; pp. 1–241. [Google Scholar]
- Carrasco, G.; Corvalan, A.H. Helicobacter pylori-Induced Chronic Gastritis and Assessing Risks for Gastric Cancer. Gastroenterol. Res. Pract. 2013, 2013, 393015. [Google Scholar] [CrossRef]
- Uemura, N.; Okamoto, S.; Yamamoto, S.; Matsumura, N.; Yamaguchi, S.; Yamakido, M.; Taniyama, K.; Sasaki, N.; Schlemper, R.J. Helicobacter pylori infection and the development of gastric cancer. New Engl. J. Med. 2001, 345, 784–789. [Google Scholar] [CrossRef]
- Graham, D.Y. Helicobacter pylori update: gastric cancer, reliable therapy, and possible benefits. Gastroenterology 2015, 148, 719–731. [Google Scholar] [CrossRef] [PubMed]
- Muhammad, J.S.; Eladl, M.A.; Khoder, G. Helicobacter pylori-induced DNA Methylation as an Epigenetic Modulator of Gastric Cancer: Recent Outcomes and Future Direction. Pathogens 2019, 8, 23. [Google Scholar] [CrossRef] [PubMed]
- Yeh, J.M.; Kuntz, K.M.; Ezzati, M.; Goldie, S.J. Exploring the cost-effectiveness of Helicobacter pylori screening to prevent gastric cancer in China in anticipation of clinical trial results. Int. J. Cancer 2009, 124, 157–166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takenaka, R.; Okada, H.; Kato, J.; Makidono, C.; Hori, S.; Kawahara, Y.; Miyoshi, M.; Yumoto, E.; Imagawa, A.; Toyokawa, T.; et al. Helicobacter pylori eradication reduced the incidence of gastric cancer, especially of the intestinal type. Aliment. Pharmacol. Ther. 2007, 25, 805–812. [Google Scholar] [CrossRef] [Green Version]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed]
- Ferlay, J.; Shin, H.R.; Bray, F.; Forman, D.; Mathers, C.; Parkin, D.M. Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. Cancer J. Clin. 2010, 127, 2893–2917. [Google Scholar] [CrossRef] [Green Version]
- Ferro, A.; Peleteiro, B.; Malvezzi, M.; Bosetti, C.; Bertuccio, P.; Levi, F.; Negri, E.; La Vecchia, C.; Lunet, N. Worldwide trends in gastric cancer mortality (1980–2011), with predictions to 2015, and incidence by subtype. Eur. J. Cancer 2014, 50, 1330–1344. [Google Scholar] [CrossRef] [PubMed]
- Schulz, T.R.; McBryde, E.S.; Leder, K.; Biggs, B.A. Using stool antigen to screen for Helicobacter pylori in immigrants and refugees from high prevalence countries is relatively cost effective in reducing the burden of gastric cancer and peptic ulceration. PloS ONE 2014, 9, e108610. [Google Scholar] [CrossRef] [PubMed]
- Muhammad, J.S.; Zaidi, S.F.; Saeed, S.A.; Ishaq, M. Current status of Helicobacter pylori association with haematological and cardiovascular diseases: A mini review. J. Pak. Med. Assoc. 2017, 67, 907–911. [Google Scholar]
- Schwarz, S.; Morelli, G.; Kusecek, B.; Manica, A.; Balloux, F.; Owen, R.J.; Graham, D.Y.; van der Merwe, S.; Achtman, M.; Suerbaum, S. Horizontal versus familial transmission of Helicobacter pylori. PLoS Pathog. 2008, 4, e1000180. [Google Scholar] [CrossRef] [PubMed]
- Forman, D.; De Backer, G.; Elder, J.; Moller, H.; Damotta, L.C.; Roy, P.; Abid, L.; Tjonneland, A.; Boeing, H.; Haubrich, H.; et al. Epidemiology of, and risk factors for, Helicobacter pylori infection among 3194 asymptomatic subjects in 17 populations. Gut 1993, 34, 1672–1676. [Google Scholar]
- Graham, D.Y.; Malaty, H.M.; Evans, D.G.; Evans, D.J., Jr.; Klein, P.D.; Adam, E. Epidemiology of Helicobacter pylori in an asymptomatic population in the United States. Effect of age, race, and socioeconomic status. Gastroenterology 1991, 100, 1495–1501. [Google Scholar] [CrossRef]
- Venneman, K.; Huybrechts, I.; Gunter, M.J.; Vandendaele, L.; Herrero, R.; Van Herck, K. The epidemiology of Helicobacter pylori infection in Europe and the impact of lifestyle on its natural evolution toward stomach cancer after infection: A systematic review. Helicobacter 2018, 23, e12483. [Google Scholar] [CrossRef] [PubMed]
- Cutler, A.F.; Havstad, S.; Ma, C.K.; Blaser, M.J.; Perez-Perez, G.I.; Schubert, T.T. Accuracy of invasive and noninvasive tests to diagnose Helicobacter pylori infection. Gastroenterology 1995, 109, 136–141. [Google Scholar] [CrossRef]
- Burucoa, C.; Delchier, J.C.; Courillon-Mallet, A.; de Korwin, J.D.; Megraud, F.; Zerbib, F.; Raymond, J.; Fauchere, J.L. Comparative evaluation of 29 commercial Helicobacter pylori serological kits. Helicobacter 2013, 18, 169–179. [Google Scholar] [CrossRef]
- Vaira, D.; Malfertheiner, P.; Megraud, F.; Axon, A.T.; Deltenre, M.; Gasbarrini, G.; O’Morain, C.; Pajares Garcia, J.M.; Quina, M.; Tytgat, G.N.; The European Helicobacter pylori HpSA Study Group. Noninvasive antigen-based assay for assessing Helicobacter pylori eradication: A European multicenter study. Am. J. Gastroenterol. 2000, 95, 925–929. [Google Scholar] [CrossRef] [PubMed]
- Megraud, F.; Bessede, E.; Lehours, P. Diagnosis of Helicobacter pylori infection. La Rev. Du Prat. 2014, 64, 201–206. [Google Scholar]
- Vaira, D.; Malfertheiner, P.; Megraud, F.; Axon, A.T.; et al. Diagnosis of Helicobacter pylori infection by HpSA test. Lancet 1999, 354, 1732. [Google Scholar] [CrossRef]
- van Doorn, O.J.; Bosman, D.K.; van’t Hoff, B.W.; Taminiau, J.A.; ten Kate, F.J.; van der Ende, A. Helicobacter pylori Stool Antigen test: a reliable non-invasive test for the diagnosis of Helicobacter pylori infection in children. Eur. J. Gastroenterol. Hepatol. 2001, 13, 1061–1065. [Google Scholar] [CrossRef] [PubMed]
- Moubri, M.; Burucoa, C.; Kalach, N.; Larras, R.R.; Nouar, N.; Mouffok, F.; Arrada, Z. Performances of the IDEIA HpStAR Stool Antigen Test in Detection of Helicobacter pylori Infection Before and After Eradication Treatment in Algerian Children. J. Trop. Pediatrics 2018. [Google Scholar] [CrossRef]
- Queiroz, D.M.; Saito, M.; Rocha, G.A.; Rocha, A.M.; Melo, F.F.; Checkley, W.; Braga, L.L.; Silva, I.S.; Gilman, R.H.; Crabtree, J.E. Helicobacter pylori infection in infants and toddlers in South America: concordance between [13C] urea breath test and monoclonal H. pylori stool antigen test. J. Clin. Microbiol. 2013, 51, 3735–3740. [Google Scholar] [CrossRef]
- Nguyen, T.V.; Bengtsson, C.; Nguyen, G.K.; Granstrom, M. Evaluation of a novel monoclonal-based antigen-in-stool enzyme immunoassay (Premier Platinum HpSA PLUS) for diagnosis of Helicobacter pylori infection in Vietnamese children. Helicobacter 2008, 13, 269–273. [Google Scholar] [CrossRef]
- Koletzko, S.; Konstantopoulos, N.; Bosman, D.; Feydt-Schmidt, A.; van der Ende, A.; Kalach, N.; Raymond, J.; Russmann, H. Evaluation of a novel monoclonal enzyme immunoassay for detection of Helicobacter pylori antigen in stool from children. Gut 2003, 52, 804–806. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Gastroenterology, O. World Gastroenterology Organisation Global Guideline: Helicobacter pylori in developing countries. J. Clin. Gastroenterol. 2011, 45, 383–388. [Google Scholar] [CrossRef]
- Burucoa, C.; Axon, A. Epidemiology of Helicobacter pylori infection. Helicobacter 2017, 22 (Suppl. 1). [Google Scholar] [CrossRef]
- Hunt, R.H.; Xiao, S.D.; Megraud, F.; Leon-Barua, R.; Bazzoli, F.; van der Merwe, S.; Vaz Coelho, L.G.; Fock, M.; Fedail, S.; Cohen, H.; et al. Helicobacter pylori in developing countries. World Gastroenterology Organisation Global Guideline. J. Gastrointest. Liver Dis. 2011, 20, 299–304. [Google Scholar]
- Bener, A.; Uduman, S.A.; Ameen, A.; Alwash, R.; Pasha, M.A.; Usmani, M.A.; SR, A.I.-N.; Amiri, K.M. Prevalence of Helicobacter pylori infection among low socio-economic workers. J. Commun. Dis. 2002, 34, 179–184. [Google Scholar]
- Bener, A.; Adeyemi, E.O.; Almehdi, A.M.; Ameen, A.; Beshwari, M.; Benedict, S.; Derballa, M.F. Helicobacter pylori profile in asymptomatic farmers and non-farmers. Int. J. Environ. Health Res. 2006, 16, 449–454. [Google Scholar] [CrossRef]
- Adeyemi, E.O.; Fadlalla, H.; al-Homsi, M.; Nnalue, N.A.; Goodwin, S.; Boehme, D.; Sim, A.J. Clinicopathological assessment of gastric biopsy samples of patients with Helicobacter pylori infection--metronidazole resistance and compliance problems in the United Arab Emirates. Ital. J. Gastroenterol. 1992, 24, 436–439. [Google Scholar]
- Zaitoun, A.M. Histological study of chronic gastritis from the United Arab Emirates using the Sydney system of classification. J. Clin. Pathol. 1994, 47, 810–815. [Google Scholar] [CrossRef] [PubMed]
- Albawardi, A.; Almarzooqi, S.; Torab, F.C. Helicobacter pylori in sleeve gastrectomies: prevalence and rate of complications. Int. J. Clin. Exp. Med. 2013, 6, 140–143. [Google Scholar]
- Bener, A.; Micallef, R.; Afifi, M.; Derbala, M.; Al-Mulla, H.M.; Usmani, M.A. Association between type 2 diabetes mellitus and Helicobacter pylori infection. Turk. J. Gastroenterol. Off. J. Turk. Soc. Gastroenterol. 2007, 18, 225–229. [Google Scholar]
- Nimri, L.F.; Matalka, I.; Bani Hani, K.; Ibrahim, M. Helicobacter pylori genotypes identified in gastric biopsy specimens from Jordanian patients. BMC Gastroenterol. 2006, 6, 27. [Google Scholar] [CrossRef] [PubMed]
- Hussein, N.R.; Robinson, K.; Atherton, J.C. A study of age-specific Helicobacter pylori seropositivity rates in Iraq. Helicobacter 2008, 13, 306–307. [Google Scholar] [CrossRef]
- Al Qabandi, A.; Mustafa, A.S.; Siddique, I.; Khajah, A.K.; Madda, J.P.; Junaid, T.A. Distribution of vacA and cagA genotypes of Helicobacter pylori in Kuwait. Acta Trop. 2005, 93, 283–288. [Google Scholar] [CrossRef]
- Korstanje, A.; den Hartog, G.; Biemond, I.; Lamers, C.B. The serological gastric biopsy: A non-endoscopical diagnostic approach in management of the dyspeptic patient: Significance for primary care based on a survey of the literature. Scand. J. Gastroenterol. Suppl. 2002, 236, 22–26. [Google Scholar] [CrossRef]
- Bakka, A.S.; Salih, B.A. Prevalence of Helicobacter pylori infection in asymptomatic subjects in Libya. Diagn. Microbiol. Infect. Dis. 2002, 43, 265–268. [Google Scholar] [CrossRef]
- Mansour, K.B.; Keita, A.; Zribi, M.; Masmoudi, A.; Zarrouk, S.; Labbene, M.; Kallel, L.; Karoui, S.; Fekih, M.; Matri, S.; et al. Seroprevalence of Helicobacter pylori among Tunisian blood donors (outpatients), symptomatic patients and control subjects. Gastroenterol. Clin. Et Biol. 2010, 34, 75–82. [Google Scholar] [CrossRef]
- Benajah, D.A.; Lahbabi, M.; Alaoui, S.; El Rhazi, K.; El Abkari, M.; Nejjari, C.; Amarti, A.; Bennani, B.; Mahmoud, M.; Ibrahimi, S.A. Prevalence of Helicobacter pylori and its recurrence after successful eradication in a developing nation (Morocco). Clin. Res. Hepatol. Gastroenterol. 2013, 37, 519–526. [Google Scholar] [CrossRef]
- Fakhro, A.R.; Fateha Bel, D.; Amin Farid, I.M.; Jamsheer, H.M. The association between Helicobacter pylori infection and lymphoid reaction in patients suffering from dyspepsia in Bahrain. Saudi J. Gastroenterol. Off. J. Saudi Gastroenterol. Assoc. 1999, 5, 129–133. [Google Scholar]
- Zamani, M.; Ebrahimtabar, F.; Zamani, V.; Miller, W.H.; Alizadeh-Navaei, R.; Shokri-Shirvani, J.; Derakhshan, M.H. Systematic review with meta-analysis: the worldwide prevalence of Helicobacter pylori infection. Aliment. Pharmacol. Ther. 2018, 47, 868–876. [Google Scholar] [CrossRef]
- Wangda, S.; Richter, J.M.; Kuenzang, P.; Wangchuk, K.; Choden, T.; Tenzin, K.; Malaty, H.M. Epidemiology of Helicobacter pylori infection in asymptomatic schoolchildren in Bhutan. Helicobacter 2017, 22. [Google Scholar] [CrossRef]
- Toscano, E.P.; Madeira, F.F.; Dutra-Rulli, M.P.; Gonçalves, L.O.M.; Proença, M.A.; Borghi, V.S.; Cadamuro, A.C.T.; Mazzale, G.W.; Acayaba, R.; Silva, A.E. Epidemiological and Clinical-Pathological Aspects of Helicobacter pylori Infection in Brazilian Children and Adults. Gastroenterol. Res. Pract. 2018, 2018. [Google Scholar] [CrossRef] [PubMed]
- Galpin, O.P.; Whitaker, C.J.; Dubiel, A.J. Helicobacter pylori infection and overcrowding in childhood. Lancet 1992, 339, 619. [Google Scholar] [CrossRef]
- Kabir, S. Detection of Helicobacter pylori in faeces by culture, PCR and enzyme immunoassay. J. Med. Microbiol. 2001, 50, 1021–1029. [Google Scholar] [CrossRef] [Green Version]
- Kusters, J.G.; Gerrits, M.M.; Van Strijp, J.A.; Vandenbroucke-Grauls, C.M. Coccoid forms of Helicobacter pylori are the morphologic manifestation of cell death. Infect. Immun. 1997, 65, 3672–3679. [Google Scholar] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | Place of Residency | |||
|---|---|---|---|---|
| Abu Dhabi | Dubai | Sharjah | Ajman | |
| Collection period | 1 September to 20 December 2017 | 6 January to 6 February 2018 | 6 January to 30 April 2018 | 1 March to 30 April 2018 |
| Locations | The industrial area of Abu Dhabi- Musaffah, Abu Dhabi City. | Housemaid offices, Private schools, and nurseries. | The University of Sharjah, housemaid offices, private schools, and nurseries. | Ajman soccer club, Housemaid offices, Private schools, and nurseries. |
| Participants, n (%) | 118 (33.7) | 10 (2.9) | 168 (48) | 54 (15.4%) |
| Gender, n (%) | ||||
| Female | 3 (2.3) | 5 (3.8) | 90 (68.7) | 33 (25.2) |
| Male | 115 (52.5) | 5 (2.3) | 78 (35.6) | 21 (9.6) |
| Ethnicity, n (%) | ||||
| Arab | 3 (1.8) | 6 (3.7) | 131 (80.4) | 23 (14.1) |
| Asian | 115 (69.7) | 3 (1.8) | 32 (19.4) | 15 (9.1) |
| African | 0 (0) | 1 (4.5) | 5 (22.7) | 16 (72.8) |
| Age group, n (%) | ||||
| 0–1 | 0 | 0 | 13 (100) | 0 |
| 2–5 | 0 | 0 | 86 (96.6) | 3 (3.4) |
| 6–15 | 1 (2.5) | 2 (5) | 29 (72.5) | 8 (20) |
| 16–30 | 15 (21.4) | 3 (4.3) | 23 (32.9) | 29 (41.4) |
| >30 | 102 (73.9) | 5 (3.6) | 17 (12.3) | 14 (10.1) |
| Hp (+), n (%) | 51 (43.2) | 1 (10) | 58 (34.5) | 35 (64.8) |
| Variables | Total | HP(−) (n = 205) | Hp(+) (n = 145) | Chi-Square p-Value |
|---|---|---|---|---|
| Socio-Demographic data | ||||
| Gender | ||||
| Female | 131 (37) | 62 (47) | 69 (53) | 0.001 * |
| Male | 219 (63) | 143 (65) | 76 (35) | |
| Age group | ||||
| 0–1 | 13 (3.7) | 9 (69.2) | 4 (30.8) | 0.032 * |
| 2–5 | 89 (25.4) | 62 (69.7) | 27 (30.3) | |
| 6–15 | 40 (11.4) | 26 (65) | 14 (35) | |
| 16–30 | 70 (20) | 33 (47.1) | 37 (52.9) | |
| >30 | 138 (39.4) | 75 (54.3) | 63 (46) | |
| Ethnicity | ||||
| Arab | 163 (46.6) | 113 (69.3) | 50 (30.7) | <0.0001 * |
| Asian | 165 (47.1) | 88 (53.3) | 77 (46.7) | |
| African | 22 (6.3) | 4 (18.2) | 18 (81.8) | |
| Occupation | ||||
| Professional | 37 (10.6) | 21 (56.8) | 16 (43.2) | 0.001 * |
| Industrial | 97 (27.7) | 57 (58.8) | 40 (41.2) | |
| Nanny | 56 (16) | 20 (35.7) | 36 (64.3) | |
| Student | 145 (41.4) | 94 (64.8) | 51 (35.2) | |
| Unemployed | 15 (4.3) | 13 (86.7) | 2 (13.3) | |
| Household income, month/AED | ||||
| ≤10,000 | 133 (45.4) | 77 (52.2) | 56 (47.8) | 0.847 |
| 11,000–20,000 | 25 (7.1) | 16 (64) | 9 (36) | |
| >20,000 | 192 (36) | 112 (58.3) | 80 (41.7) | |
| Number of persons/house | ||||
| 1–3 | 31 (8.9) | 16 (51.6) | 15 (48.4) | 0.676 |
| 4–6 | 207 (59.1) | 124 (60) | 83 (40) | |
| ≥7 | 112 (32) | 65 (58) | 47 (42) | |
| Number of persons/room | ||||
| 1–2 | 156 (44.6) | 4 (66.7) | 2 (33.3) | <0.0001 * |
| ≥3 | 194 (55.4) | 97 (50) | 97 (50) | |
| Lifestyle characteristics | ||||
| Contact with domestic animals | ||||
| No | 305 (87.1) | 181 (59.3) | 124 (40.7) | 0.445 |
| Yes | 45 (12.9) | 24 (53.3) | 21 (46.7) | |
| Source of Drinking water | ||||
| Bottled | 283 (80.9) | 179 (63.3) | 104 (36.7) | 0.001 * |
| Tap | 58 (16.6) | 24 (41.4) | 34 (58.6) | |
| Boiled | 9 (2.6) | 7 (77.8) | 2 (22.2) | |
| Gastrointestinal Characteristics | ||||
| Gastrointestinal symptoms | ||||
| None | 288 (82.3) | 179 (62.2) | 109 (37.8) | 0.001 * |
| Bloating | 20 (5.7) | 12 (60) | 8 (40) | |
| Abdominal pain | 29 (8.3) | 7 (24.1) | 22 (75.9) | |
| Others | 13 (3.7) | 7 (53.8) | 6 (46.2) | |
| Parent gastric diseases history | ||||
| None | 293 (83.7) | 189 (64.5) | 104 (35.5) | <0.0001 * |
| Peptic ulcer | 31 (8.9) | 3 (9.7) | 28 (90.3) | |
| Others | 26 (7.4) | 13 (50) | 13 (50) | |
| Variable | Odds Ratio (95% Confidence Interval) | p Value |
|---|---|---|
| Gender | ||
| Male | 1 | |
| Female | 2.52 (1.16–5.50) | 0.020 * |
| Age groups (years) | ||
| 0–1 | 1 | |
| 2–5 | 1.67 (0.33–8.39) | 0.536 |
| 6–15 | 1.73 (0.31–9.85) | 0.534 |
| 16–30 | 1.35 (0.19–9.59) | 0.763 |
| >30 | 1.36 (0.17–10.71) | 0.771 |
| Ethnicity | ||
| Arab | 1 | |
| Asian | 7.98 (2.32–27.48) | 0.001 * |
| African | 29.75 (4.41–200.94) | <0.0001 * |
| Occupation | ||
| Professional | 1 | |
| Industrial | 0.42 (0.15–1.15) | 0.092 |
| Nanny | 2.79 (0.54–14.52) | 0.223 |
| Student | 0.20 (0.03–1.41) | 0.105 |
| Unemployed | 0.47 (0.05–4.85) | 0.526 |
| Source of drinking water | ||
| Bottled | 1 | |
| Tap | 1.11 (0.31–3.94) | 0.875 |
| Boiled | 3.17 (0.44–23.08) | 0.254 |
| Number of persons/room | ||
| 1–2 | 1 | |
| ≥3 | 3.76 (1.41–10.00) | 0.008 * |
| Parent gastric diseases history | ||
| None | 1 | |
| Peptic ulcer | 22.07 (6.01–81.11) | <0.0001 * |
| Others | 1.92 (0.75–4.92) | 0.176 |
| Gastrointestinal symptoms | ||
| None | 1 | |
| Bloating | 0.68 (0.20–2.31) | 0.536 |
| Abdominal pain | 6.87 (2.39–19.79) | <0.001 * |
| Others | 0.90 (0.25–3.28) | 0.869 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Khoder, G.; Muhammad, J.S.; Mahmoud, I.; Soliman, S.S.M.; Burucoa, C. Prevalence of Helicobacter pylori and Its Associated Factors among Healthy Asymptomatic Residents in the United Arab Emirates. Pathogens 2019, 8, 44. https://doi.org/10.3390/pathogens8020044
Khoder G, Muhammad JS, Mahmoud I, Soliman SSM, Burucoa C. Prevalence of Helicobacter pylori and Its Associated Factors among Healthy Asymptomatic Residents in the United Arab Emirates. Pathogens. 2019; 8(2):44. https://doi.org/10.3390/pathogens8020044
Chicago/Turabian StyleKhoder, Ghalia, Jibran Sualeh Muhammad, Ibrahim Mahmoud, Sameh S. M. Soliman, and Christophe Burucoa. 2019. "Prevalence of Helicobacter pylori and Its Associated Factors among Healthy Asymptomatic Residents in the United Arab Emirates" Pathogens 8, no. 2: 44. https://doi.org/10.3390/pathogens8020044