
Effect of Local Administration of Meglumine Antimoniate and Polyhexamethylene Biguanide Alone or in Combination with a Toll-like Receptor 4 Agonist for the Treatment of Papular Dermatitis due to Leishmania infantum in Dogs
 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
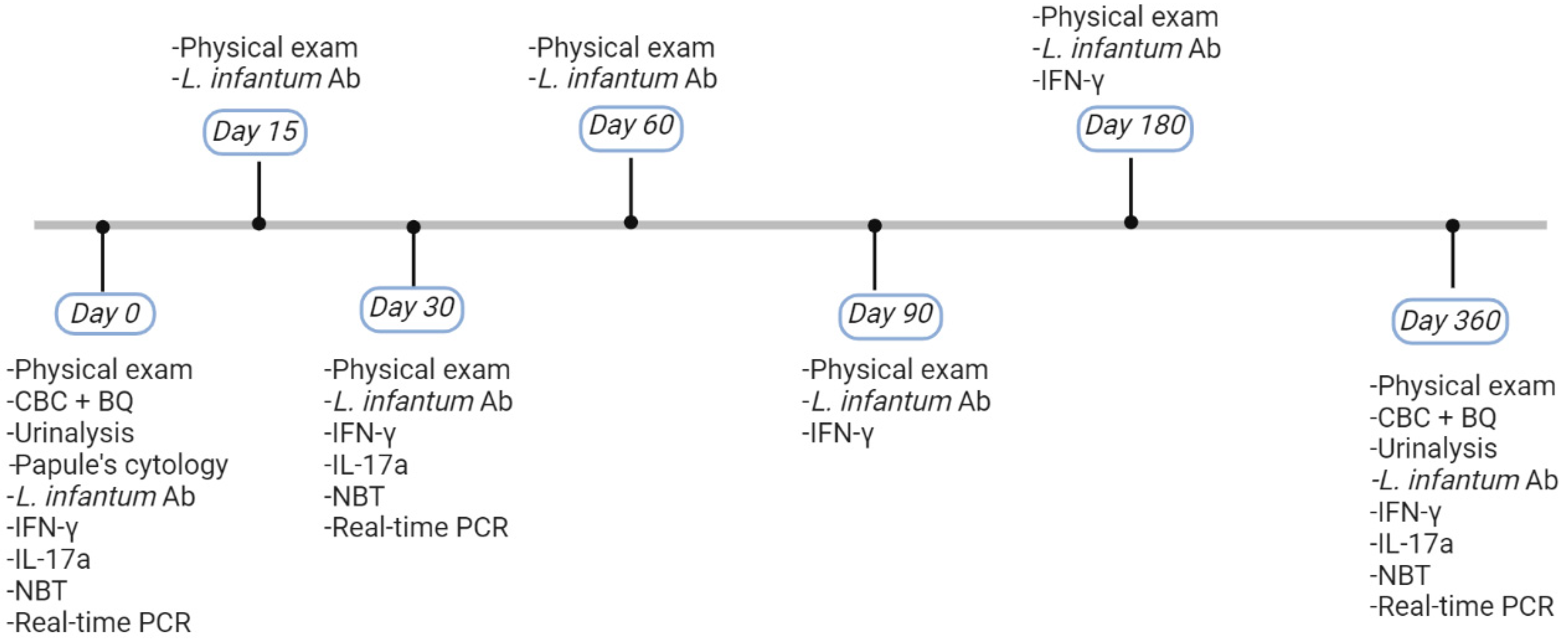
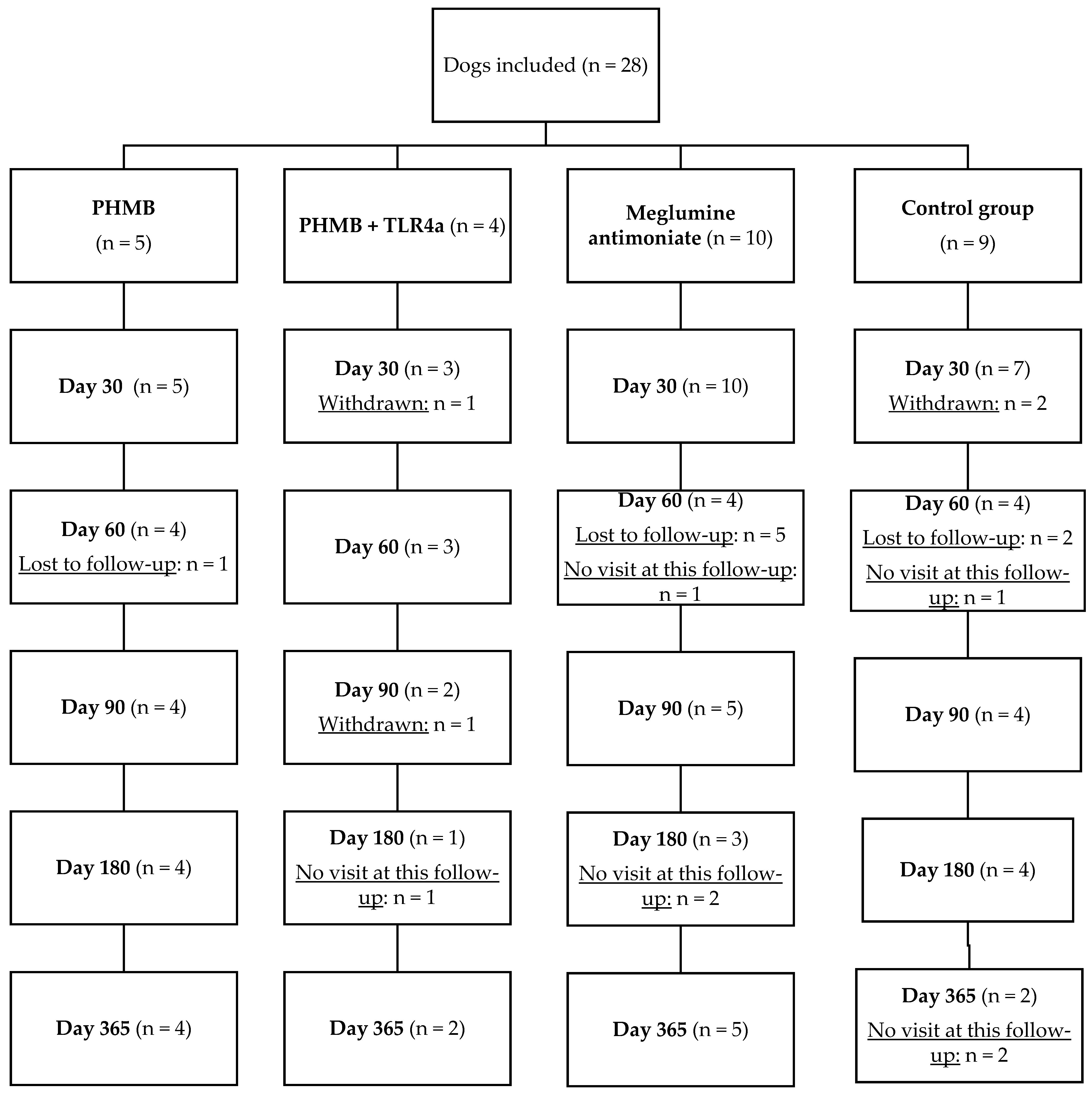
2.1. Dogs and Study Design
2.2. Treatment and Follow-Up
2.3. Safety Assessment
2.4. ELISA for specific L. infantum Antibody Detection
2.5. Cytokine Release Whole Blood Assay and Determination of Canine IFN-γ and IL-17a
2.6. Nitroblue Tetrazolium Reduction Test
2.7. Blood DNA Extraction and Leishmania Real-Time PCR
2.8. Statistical Analysis
3. Results
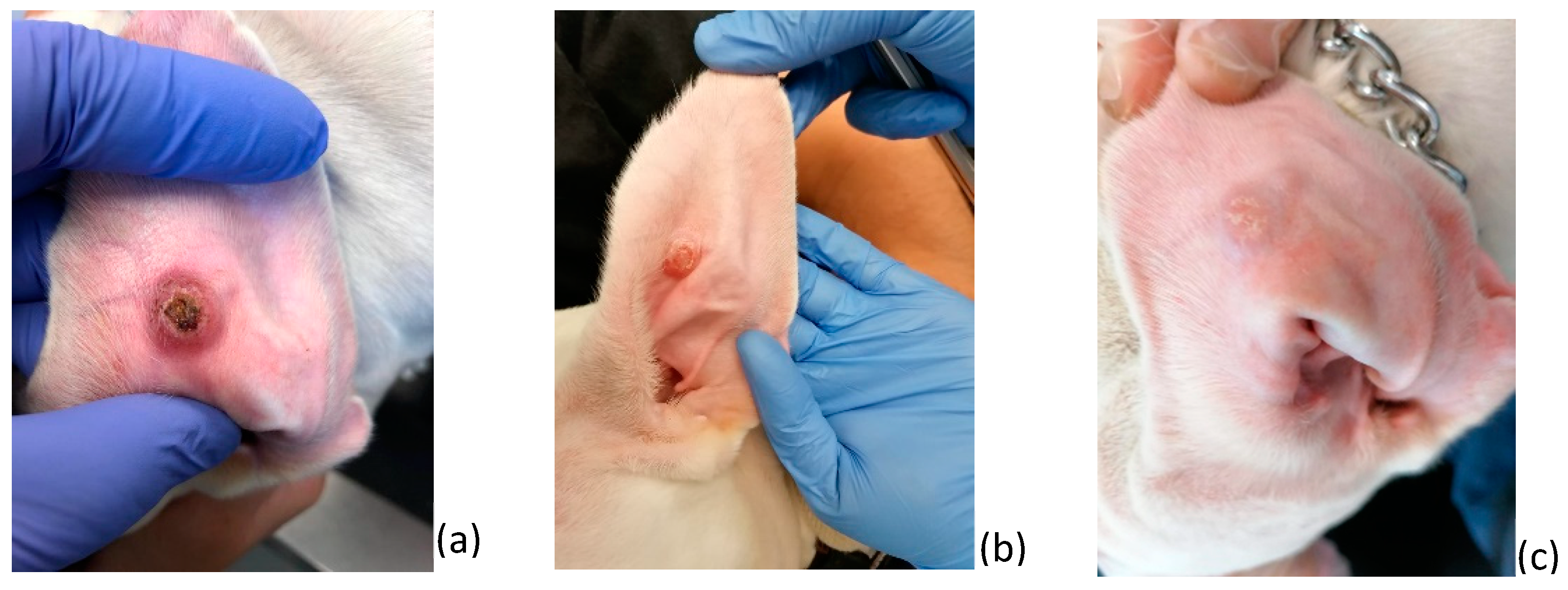
3.1. Dog Characteristics at the Time of Diagnosis
3.2. Safety and Clinical Efficacy of Treatments
3.3. Clinical Worsening (Withdrawal) and Lost to Follow-Up
3.4. Leishmania Infantum-Specific Antibody Levels at the Time of Diagnosis and Follow-Up
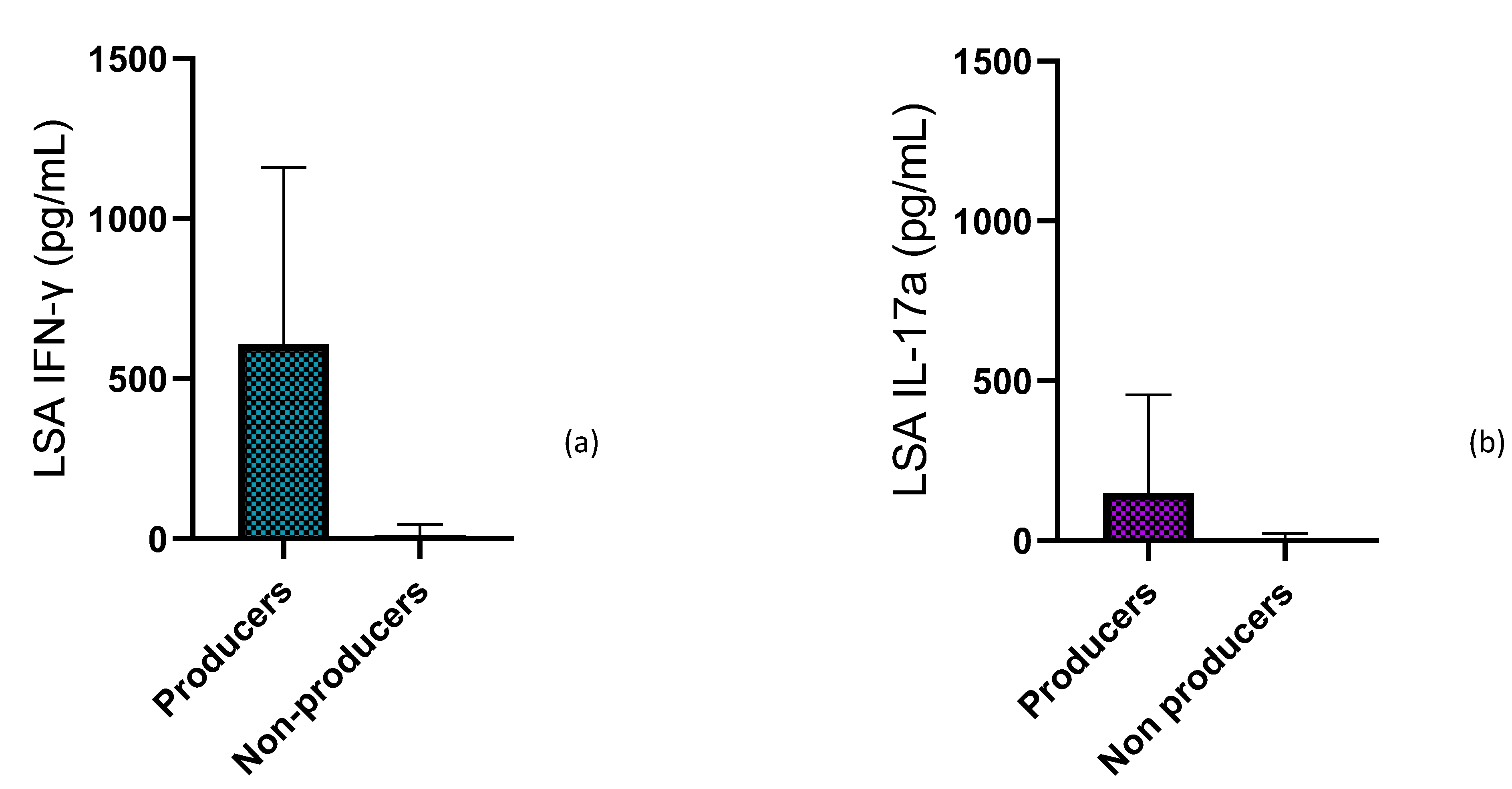
3.5. IFN-γ Concentration at the Time of Diagnosis and During Treatment Follow-Up
3.6. IL-17a Concentration at Time of Diagnosis and During Treatment Follow-Up
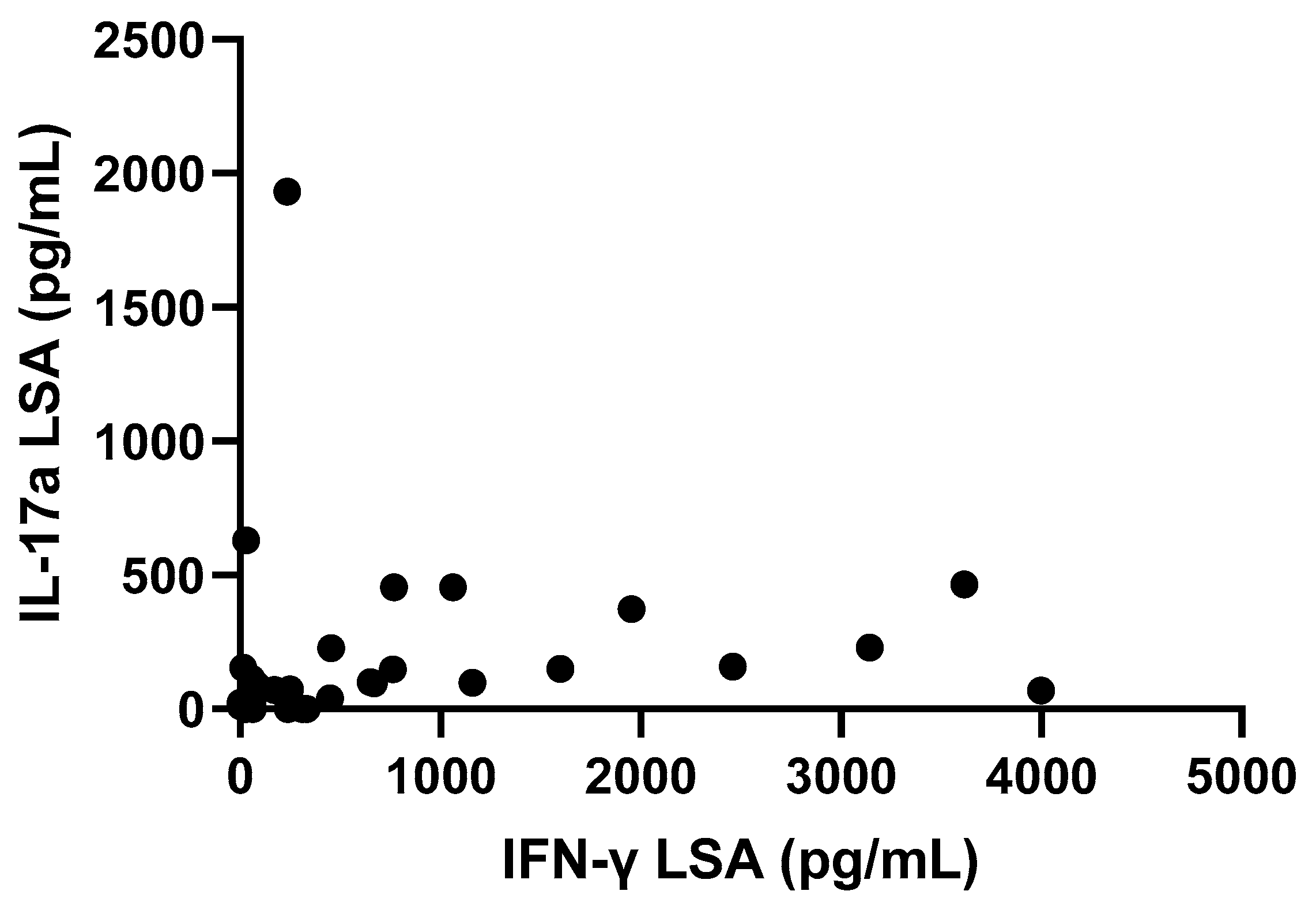
3.7. Correlation between Parameters Studied
3.8. Nitroblue Tetrazolium Reduction Test
3.9. Blood PCR
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Solano-Gallego, L.; Miró, G.; Koutinas, A.; Cardoso, L.; Pennisi, M.G.; Ferrer, L.; Bourdeau, P.; Oliva, G.; Baneth, G. LeishVet guidelines for the practical management of canine leishmaniosis. Parasites Vectors 2011, 4, 1–16. [Google Scholar] [CrossRef] [Green Version]
- Baneth, G.; Koutinas, A.F.; Solano-Gallego, L.; Bourdeau, P.; Ferrer, L. Canine leishmaniosis—New concepts and insights on an expanding zoonosis: Part one. Trends Parasitol. 2008, 24, 324–330. [Google Scholar] [CrossRef]
- Esteve, L.O.; Saz, S.V.; Hosein, S.; Solano-Gallego, L. Histopathological findings and detection of Toll-like receptor 2 in cutaneous lesions of canine leishmaniosis. Vet. Parasitol. 2015, 209, 157–163. [Google Scholar] [CrossRef] [PubMed]
- Lombardo, G.; Pennisi, M.G.; Lupo, T.; Chicharro, C.; Solano-Gallego, L. Papular dermatitis due to Leishmania infantum infection in seventeen dogs: Diagnostic features, extent of the infection and treatment outcome. Parasites Vectors 2014, 7, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Solano-Gallego, L.; Montserrrat-Sangrà, S.; Ordeix, L.; Martínez-Orellana, P. Leishmania infantum-specific production of IFN-γ and IL-10 in stimulated blood from dogs with clinical leishmaniosis. Parasites Vectors 2016, 9, 317. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Montserrat-Sangrà, S.; Ordeix, L.; Martínez-Orellana, P.; Solano-Gallego, L. Parasite specific antibody levels, interferon-γ and TLR2 and TLR4 transcripts in blood from dogs with different clinical stages of leishmaniosis. Vet. Sci. 2018, 5, 31. [Google Scholar] [CrossRef] [Green Version]
- Hosein, S.; Blake, D.P.; Solano-Gallego, L. Insights on adaptive and innate immunity in canine leishmaniosis. Parasitology 2017, 144, 95–115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Papadogiannakis, E.I.; Koutinas, A.F. Cutaneous immune mechanisms in canine leishmaniosis due to Leishmania infantum. Vet. Immunol. Immunopathol. 2015, 163, 94–102. [Google Scholar] [CrossRef]
- Hernandez-Bures, A.; Gillen, J.; Apostolidis, K.; Saridomichelakis, M.; Di Loria, A.; Santoro, D. Evaluation of the cutaneous inflammatory cells in dogs with leishmaniosis and in dogs without the disease that were naturally infected by Leishmania infantum (syn. L. chagasi). Vet. Dermatol. 2021, 32, 99-e19. [Google Scholar] [CrossRef]
- Nascimento, M.S.L.; Carregaro, V.; Lima-Júnior, D.S.; Costa, D.L.; Ryffel, B.; Duthie, M.S.; de Jesus, A.; de Almeida, R.P.; da Silva, J.S. Interleukin 17A acts synergistically with interferon γ to promote protection against Leishmania infantum infection. J. Infect. Dis. 2015, 211, 1015–1026. [Google Scholar] [CrossRef] [Green Version]
- Nascimento, M.S.L.; Albuquerque, T.D.R.; Nascimento, A.F.S. Impairment of Interleukin-17A Expression in Canine Visceral Leishmaniosis is Correlated with Reduced Interferon-γ and Inducible Nitric Oxide Synthase Expression. J. Comp. Pathol. 2015, 153, 197–205. [Google Scholar] [CrossRef] [PubMed]
- Rebech, G.T.; Venturin, G.L.; Siqueira Ito, L.T.; Bragato, J.P.; de Carvalho Fonseca, B.S.; Melo, L.M.; Costa, S.F.; de Rezende Eugênio, F.; Dos Santos, P.S.P.; de Lima, V.M.F. PD-1 regulates leishmanicidal activity and IL-17 in dogs with leishmaniasis. Vet. Immunol. Immunopathol. 2020, 219, 109970. [Google Scholar] [CrossRef]
- Toepp, A.J.; Petersen, C.A. The balancing act: Immunology of leishmaniosis. Res. Vet. Sci. 2020, 130, 19–25. [Google Scholar] [CrossRef]
- Esch, K.J.; Schaut, R.G.; Lamb, I.M.; Clay, G.; Lima, L.M.; Nascimento, R.P.; Whitley, E.M.; Jeronimo, S.M.; Sutterwala, F.S.; Haynes, J.S.; et al. Activation of Autophagy and Nucleotide-Binding Domain Leucine-Rich Repeat Containing-Like Receptor Family, Pyrin Domain Containing 3 Inflammasome during Leishmania infantum Associated Glomerulonephritis. Am. J. Pathol. 2015, 185, 2105–2117. [Google Scholar] [CrossRef] [Green Version]
- Gibson-Corley, K.N.; Hostetter, J.M.; Hostetter, S.J.; Mullin, K.; Ramer-Tait, A.E.; Boggiatto, P.M.; Petersen, C.A. Disseminated Leishmania infantum infection in two sibling foxhounds due to possible vertical transmission. Can. Vet. J. 2008, 49, 1005–1008. [Google Scholar]
- Gibson-corley, K.N.; Boggiatto, P.M.; Mukbel, R.M.; Petersen, C.A.; Jones, D.E. A deficiency in the B cell response of C57BL / 6 mice correlates with loss of macrophage-mediated killing of Leishmania amazonensis. Int. J. Parasitol. 2010, 40, 157–161. [Google Scholar] [CrossRef] [Green Version]
- Pereira-Fonseca, D.C.M.; Oliveira-Rovai, F.M.; Rodas, L.A.C.; Beloti, C.A.C.; Torrecilha, R.B.P.; Ito, P.K.R.K.; Avanço, S.V.; Cipriano, R.S.; Utsunomiya, Y.T.; Hiramoto, R.M.; et al. Dog skin parasite load, TLR-2, IL-10 and TNF-α expression and infectiousness. Parasite Immunol. 2017, 39, e12493. [Google Scholar] [CrossRef]
- Carpenter, S.; O’Neill, L.A.J. How important are Toll-like receptors for antimicrobial responses? Cell Microbiol. 2007, 9, 1891–1901. [Google Scholar] [CrossRef]
- Kumar, H.; Kawai, T.; Akira, S. Pathogen recognition by the innate immune system. Int. Rev. Immunol. 2011, 30, 16–34. [Google Scholar] [CrossRef] [PubMed]
- Kawai, T.; Akira, S. Toll-like Receptors and Their Crosstalk with Other Innate Receptors in Infection and Immunity. Immunity 2011, 34, 637–650. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ordeix, L.; Montserrat-Sangrà, S.; Martínez-Orellana, P.; Baxarias, M.; Solano-Gallego, L. Toll-like receptors 2, 4 and 7, interferon-gamma and interleukin 10, and programmed death ligand 1 transcripts in skin from dogs of different clinical stages of leishmaniosis. Parasites Vectors 2019, 12, 575. [Google Scholar] [CrossRef]
- Martínez-Orellana, P.; Baxarias, M.; Good, L.; Solano-Gallego, L. The effects of polyhexamethylene biguanide (PHMB) and TLR agonists alone or as polyplex nanoparticles against Leishmania infantum promastigotes and amastigotes. Vet. Sci. 2020, 7, 179. [Google Scholar] [CrossRef] [PubMed]
- Winterbourn, C.C.; Kettle, A.J.; Hampton, M.B. Reactive Oxygen Species and Neutrophil Function. Annu. Rev. Biochem. 2016, 85, 765–792. [Google Scholar] [CrossRef]
- Gómez-Ochoa, P.; Lara, A.; Couto, G.; Marcen, J.M.; Peris, A.; Gascón, M.; Castillo, J.A. The nitroblue tetrazolium reduction test in canine leishmaniosis. Vet. Parasitol. 2010, 172, 135–138. [Google Scholar] [CrossRef]
- Gómez-Ochoa, P.; Sabate, D.; Homedes, J.; Ferrer, L. Use of the nitroblue tetrazolium reduction test for the evaluation of Domperidone effects on the neutrophilic function of healthy dogs. Vet. Immunol. Immunopathol. 2012, 146, 97–99. [Google Scholar] [CrossRef] [PubMed]
- Dea-Ayuela, M.A.; Segarra, S.; Serrano, D.R.; Bolás-Fernández, F. Nucleotides and AHCC Enhance Th1 Responses in Vitro in Leishmania-Stimulated/Infected Murine Cells. Molecules 2020, 25, 3918. [Google Scholar] [CrossRef]
- Ordeix, L.; Rodríguez, A.; Martínez-Orellana Pamela Montserrat Sangrà, S.; Solano-Gallego, L. Clinical follow up of a series of dogs with papular dermatitis due to Leishmania infantum. In Proceedings of the 29th Annual Congress of the ESVD-ECVD, Lausanne, Switzerland, 14 September 2017. [Google Scholar]
- Aronson, N.; Herwaldt, B.L.; Libman, M.; Pearson, R.; Lopez-Velez, R.; Weina, P.; Carvalho, E.; Ephros, M.; Jeronimo, S.; Magill, A. Diagnosis and Treatment of Leishmaniasis: Clinical Practice Guidelines by the Infectious Diseases Society of America (IDSA) and the American Society of Tropical Medicine and Hygiene (ASTMH). Clin. Infect. Dis. 2016, 63, 1539–1557. [Google Scholar] [CrossRef] [Green Version]
- Garza-Tovar, T.F.; Sacriste-Hernández, M.I.; Juárez-Durán, E.R.; Arenas, R. An overview of the treatment of cutaneous leishmaniasis. Fac. Rev. 2020, 9, 28. [Google Scholar] [CrossRef]
- Burza, S.; Croft, S.L.; Boelaert, M. Leishmaniasis. Lancet 2018, 392, 951–970. [Google Scholar] [CrossRef]
- Nassif, P.W.; França, T.; Mello, P.D.E.; Navasconi, T.R.; Mota, C.A.; Demarchi, I.G.; Aristides, S.M.A.; Lonardoni, M.V.C.; Teixeira, J.J.V.; Silveira, T.G.V. Safety and efficacy of current alternatives in the topical treatment of cutaneous leishmaniasis: A systematic review. Parasitology 2017, 144, 995–1004. [Google Scholar] [CrossRef] [PubMed]
- Uribe-Restrepo, A.F.; Prieto, M.D.; Cossio, A.; Desai, M.M.; Del Mar Castro, M. Eligibility for Local Therapies in Adolescents and Adults with Cutaneous Leishmaniasis from Southwestern Colombia: A Cross-Sectional Study. Am. J. Trop. Med. Hyg. 2019, 100, 306–310. [Google Scholar] [CrossRef] [Green Version]
- Mulder, G.; Cavorsi, J.; Lee, D. Polyhexamethylene Biguanide (PHMB): An Addendum to Current Topical Antimicrobials. Wounds 2007, 19, 173–182. [Google Scholar]
- Firdessa, R.; Good, L.; Amstalden, M.C.; Chindera, K.; Kamaruzzaman, N.F.; Schultheis, M.; Röger, B.; Hecht, N.; Oelschlaeger, T.A.; Meinel, L.; et al. Pathogen- and Host-Directed Antileishmanial Effects Mediated by Polyhexanide (PHMB). PLoS Negl. Trop. Dis. 2015, 9, e0004041. [Google Scholar] [CrossRef]
- Berenguer, D.; Sosa, L.; Alcover, M.; Sessa, M.; Halbaut, L.; Guillén, C.; Fisa, R.; Calpena-Campmany, A.C.; Riera, C. Development and characterization of a semi-solid dosage form of meglumine antimoniate for topical treatment of cutaneous leishmaniasis. Pharmaceutics 2019, 11, 613. [Google Scholar] [CrossRef] [Green Version]
- Solano-Gallego, L.; Di Filippo, L.; Ordeix, L.; Planellas, M.; Roura, X.; Altet, L.; Martínez-Orellana, P.; Montserrat, S. Early reduction of Leishmania infantum-specific antibodies and blood parasitemia during treatment in dogs with moderate or severe disease. Parasites Vectors 2016, 9, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Solano-Gallego, L.; Villanueva-Saz, S.; Carbonell, M.; Trotta, M.; Furlanello, T.; Natale, A. Serological diagnosis of canine leishmaniosis: Comparison of three commercial ELISA tests (Leiscan®, ID Screen® and Leishmania 96®), a rapid test (Speed Leish K®) and an in-house IFAT. Parasites Vectors 2014, 7, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martínez-Orellana, P.; González, N.; Baldassarre, A.; Álvarez-Fernández, A.; Ordeix, L.; Paradies, P.; Soto, M.; Solano-Gallego, L. Humoral Responses and Ex Vivo IFN-γ Production after Canine Whole Blood Stimulation with Leishmania infantum Antigen or KMP11 Recombinant Protein. Vet. Sci. 2022, 9, 116. [Google Scholar] [CrossRef] [PubMed]
- Martín-Ezquerra, G.; Fisa, R.; Riera, C.; Rocamora, V.; Fernández-Casado, A.; Barranco, C.; Serra, T.; Baró, T.; Pujol, R. Role of Leishmania spp. infestation in nondiagnostic cutaneous granulomatous lesions: Report of a series of patients from a Western Mediterranean area. Br. J. Dermatol. 2009, 161, 320–325. [Google Scholar] [CrossRef] [PubMed]
- Piragauta, S.P.; Higuita-Castro, J.L.; Arbeláez, N.; Restrepo, A.M.; Archbold, R.; Quiñones, W.; Torres, F.; Echeverri, F.; Escobar, G.; Vélez, I.D.; et al. Utility of the combination of hederagenin glucoside saponins and chromane hydrazone in the topical treatment of canine cutaneous leishmaniasis. An observational study. Parasitol. Res. 2022, 121, 1419–1428. [Google Scholar] [CrossRef]
- Lago, J.; Fraga, D.; Guimarães, L.H.; Lago, T.; Santos, Y.; Lago, E.; Werneck, G.L.; Bacellar, O.; Carvalho, E.M. Efficacy of intralesional meglumine antimoniate in the treatment of canine tegumentary leishmaniasis: A Randomized controlled trial. PLoS Negl. Trop. Dis. 2023, 17, e0011064. [Google Scholar]
- Barbosa Santos, E.G.O.; Marzochi, M.C.A.; Conceição, N.F.; Brito, C.M.M.; Barroso, J.A.; Pacheco, R.S. N-methylglucamine antimonate (SbV+): Intralesional canine tegumentary leishmaniasis therapy. Parasite 1998, 5, 175–180. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aronson, N.E.; Joya, C.A. Cutaneous Leishmaniasis: Updates in Diagnosis and Management. Infect. Dis. Clin. N Am. 2019, 33, 101–117. [Google Scholar] [CrossRef] [Green Version]
- Moosavian Kalat, S.A.; Khamesipour, A.; Bavarsad, N.; Fallah, M.; Khashyarmanesha, Z.; Feizi, E.; Neghabi, K.; Abbasi, A.; Jaafari, M. Use of topical liposomes containing meglumine antimoniate (Glucantime) for the treatment of L. major lesion in BALB/c mice. Exp. Parasitol. 2014, 143, 5–10. [Google Scholar] [CrossRef]
- Moosavian, S.A.; Fallah, M.; Jaafari, M.R. The activity of encapsulated meglumine antimoniate in stearylamine-bearing liposomes against cutaneous leishmaniasis in BALB/c mice. Exp. Parasitol. 2019, 200, 30–35. [Google Scholar] [CrossRef]
- Momeni, A.; Rasoolian, M.; Momeni, A.; Navaei, A.; Emami, S.; Shaker, Z.; Mohebali, M.; Khoshdel, A. Development of liposomes loaded with anti-leishmanial drugs for the treatment of cutaneous leishmaniasis. J. Liposome Res. 2013, 23, 134–144. [Google Scholar] [CrossRef]
- Aragão Horoiwa, T.; Cortez, M.; Sauter, I.P.; Migotto, A.; Bandeira, C.L.; Cerize, N.N.P.; de Oliveira, A.M. Sugar-based colloidal nanocarriers for topical meglumine antimoniate application to cutaneous leishmaniasis treatment: Ex vivo cutaneous retention and in vivo evaluation. Eur. J. Pharm. Sci. 2020, 147, 105295. [Google Scholar] [CrossRef] [PubMed]
- Cosco, D.; Bruno, F.; Castelli, G.; Puleio, R.; Bonacci, S.; Procopio, A.; Britti, D.; Fresta, M.; Vitale, F.; Paolino, D. Meglumine antimoniate-loaded aqueous-core PLA nanocapsules: Old drug, new formulation against Leishmania-related diseases. Macromol. Biosci. 2021, 21, e2100046. [Google Scholar] [CrossRef] [PubMed]
- Nolff, M.C.; Winter, S.; Reese, S.; Meyer-Lindenberg, A. Comparison of polyhexanide, cold atmospheric plasma and saline in the treatment of canine bite wounds. J. Small Anim. Pract. 2019, 60, 348–355. [Google Scholar] [CrossRef]
- Llorens, E.; Calderón, S.; Del Valle, L.J.; Puiggalí, J. Polybiguanide (PHMB) loaded in PLA scaffolds displaying high hydrophobic, biocompatibility and antibacterial properties. Mater. Sci. Eng. C Mater. Biol. Appl. 2015, 50, 74–84. [Google Scholar] [CrossRef]
- Mills, P.C.; Ahlstrom, L.; Wilson, W.J. Ototoxicity and tolerance assessment of a TrisEDTA and polyhexamethylene biguanide ear flush formulation in dogs. J. Vet. Pharmacol. Ther. 2005, 28, 391–397. [Google Scholar] [CrossRef]
- Barrigah-Benissan, K.; Ory, J.; Sotto, A.; Salipante, F.; Lavigne, J.-P.; Loubet, P. Antiseptic Agents for Chronic Wounds: A Systematic Review. Antibiotics 2022, 11, 350. [Google Scholar] [CrossRef]
- Worsley, A.; Vassileva, K.; Tsui, J.; Song, W.; Good, L. Polyhexamethylene Biguanide_Polyurethane Blend Nanofibrous Membranes for Wound Infection Control. Polymers 2019, 11, 915. [Google Scholar] [CrossRef] [Green Version]
- Bagga, B.; Sharma, S.; Gour, R.P.S.; Mohamed, A.; Joseph, J.; MRathi, V.; Garg, P. A randomized masked pilot clinical trial to compare the efficacy of topical 1% voriconazole ophthalmic solution as monotherapy with combination therapy of topical 0.02% polyhexamethylene biguanide and 0.02% chlorhexidine in the treatment of Acanthamoeba keratitis. Eye 2021, 35, 1326–1333. [Google Scholar] [PubMed]
- Bottero, E.; Poggi, M.; Viglione, M. Lesioni papulari indotte da Leishmania spp. in 8 cani giovani. Veterinaria 2006, 20, 33–36. [Google Scholar]
- Gonçalves-de-albuquerque, C.; Gomes, L.; Sousa-paula LCDe Gaud, K.; Sales, S.; Boegel, A. Exploring IL-17 gene promoter polymorphisms in canine leishmaniasis. Acta Trop. 2022, 232, 106452. [Google Scholar] [CrossRef]
- Rodríguez-Cortés, A.; Ojeda, A.; López-Fuertes, L.; Timón, M.; Altet, L.; Solano-Gallego, L.; Sánchez-Robert, E.; Francino, O.; Alberola, J. A long term experimental study of canine visceral leishmaniasis. Int. J. Parasitol. 2007, 37, 683–693. [Google Scholar] [CrossRef]
- Pietro SDi Crinò, C.; Falcone, A.; Crupi, R.; Francaviglia, F.; Vitale, F.; Giudice, E. Parasitemia and its daily variation in canine leishmaniasis. Parasitol. Res. 2020, 119, 3541–3548. [Google Scholar] [CrossRef] [PubMed]
- Solano-Gallego, L.; Rodriguez-Cortes, A.; Trotta, M.; Zampieron, C.; Razia, L.; Furlanello, T.; Caldin, M.; Roura, X.; Alberola, J. Detection of Leishmania infantum DNA by fret-based real-time PCR in urine from dogs with natural clinical leishmaniosis. Vet. Parasitol. 2007, 147, 315–319. [Google Scholar] [CrossRef]
- Solano-Gallego, L.; Koutinas, A.; Miró, G.; Cardoso, L.; Pennisi, M.G.; Ferrer, L.; Bourdeau, P.; Oliva, G.; Baneth, G. Directions for the diagnosis, clinical staging, treatment and prevention of canine leishmaniosis. Vet. Parasitol. 2009, 165, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Ordeix, L.; Solano-Gallego, L.; Fondevila, D.; Ferrer, L.; Fondati, A. Papular dermatitis due to Leishmania spp. infection in dogs with parasite-specific cellular immune responses. Vet. Dermatol. 2005, 16, 187–191. [Google Scholar] [CrossRef]
- Belkaid, Y.; Mendez, S.; Lira, R.; Kadambi, N.; Milon, G.; Sacks, D. A natural model of Leishmania major infection reveals a prolonged “silent” phase of parasite amplification in the skin before the onset of lesion formation and immunity. J. Immunol. 2000, 165, 969–977. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aslan, H.; Oliveira, F.; Meneses, C.; Castrovinci, P.; Gomes, R.; Teixeira, C.; Derenge, C.A.; Orandle, M.; Gradoni, L.; Oliva, G.; et al. New insights into the transmissibility of Leishmania infantum from dogs to sand flies: Experimental vector-transmission reveals persistent parasite depots at bite sites. J. Infect. Dis. 2016, 213, 1752–1761. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Site | Number of Lesions | % |
|---|---|---|
| Inner surface of the pinna | 15 | 46.9 |
| Abdomen | 6 | 18.8 |
| Eyelid | 3 | 9.4 |
| Lips | 3 | 9.4 |
| Foreskin | 2 | 6.3 |
| Elbow | 1 | 3.1 |
| Bridge of the nose | 1 | 3.1 |
| Nose | 1 | 3.1 |
| Total Number of Dogs | % | Median Age (Minimum-Maximum Months) | |
|---|---|---|---|
| Autumn | 17 | 70.8 | 6 (3–84) |
| Female | 5 | 20.8 | 7 (3–84) |
| Male | 12 | 50 | 6 (4–6) |
| Winter | 4 | 16.7 | 6 (6–10) |
| Female | 3 | 12.5 | 6 (6–10) |
| Male | 1 | 4.2 | 5 |
| Spring | 2 | 8.3 | 3.5 (3–4) |
| Male | 2 | 8.3 | 3.5 (3–4) |
| Summer | 1 | 4.2 | 5 |
| Female | 1 | 4.2 | 5 |
| Total | 24 | 100 | 6 |
| Qualitative Characteristics | PHMB + PHMB with TLR4a (n = 9) | Meglumine Antimoniate (n = 6/10) * | Control Group (n = 9) | p-Value (Fisher’s Exact Test) | |
| Breed | Crossbred | 7 (78%) | 3 (50%) | 3 (33%) | 0.162 |
| Purebred | 2 (22%) | 3 (50%) | 6 (67%) | ||
| Sex | Male | 7 (78%) | 2 (33%) | 5 (56%) | 0.227 |
| Female | 2 (22%) | 4 (67%) | 4 (44%) | ||
| ELISA at day 0 | Low positive | 3 (33%) | 0 (0%) | 3 (33%) | 0.264 |
| Negative | 6 (67%) | 6 (100%) | 6 (67%) | ||
| Leishmania real-time PCR | Positive | 5 (56%) | 3 (50%) | 5 (56%) | 0.972 |
| Negative | 4 (44%) | 3 (50%) | 4 (44%) | ||
| IFN-γ | Producers | 7 (78%) | 3 (50%) | 2 (22%) | 0.1 |
| Non-prod. | 2 (22%) | 3 (50%) | 7 (78%) | ||
| IL-17a | Producers | 8 (89%) | 1 (17%) | 1 (11%) | 0.7 |
| Non-prod. | 1 (11%) | 5 (83%) | 8 (89%) | ||
| Quantitative Characteristics | Median (min-max) | Median (min-max) | Median (min-max) | p-Value (Kruskal-Wallis Test) | |
| Age (months) | 6 (3–8) | 5.5 (4–84) | 6 (3–36) | 0.875 | |
| IFN-γ (pg/mL) | 768.6 (11.6–3997.5) | 140.4 (0–762.4) | 23.6 (0–309) | 0.011 ** | |
| IL-17a (pg/mL) | 151.1 (0–1933.3) | 11.9 (0.148) | 0 (0–71.5) | 0.005 ** | |
| ELISA Units | 26 (7.1–227.1) | 5.7 (2.8–73.5) | 22.3 (4.8–100.9) | 0.11 | |
| Quantitative Characteristics | Mean ± SD | Mean ± SD | Mean ± SD | p-Value (Ordinary One-Way ANOVA) | |
| Cq PCR | 35.3 ± 1.9 | 35 ± 1.4 | 33.9 ± 2.7 | 0.58 | |
| Local Treatment (Number of Dogs) | Clinical Resolution (Number of Dogs/Total, %) | |||||
|---|---|---|---|---|---|---|
| 15 Days Post-Treatment | 30 Days Post-Treatment | |||||
| Without Resolution | Partial | Total | Without Resolution | Partial | Total | |
| PHMB alone (n = 5) | 1/5, 20% | 3/5, 60% | 1/5, 20% | 1/5, 20% | 2/5, 40% | 2/5, 40% |
| PHMB+ TLR4a (n = 4) | 1/4, 25% | 3/4, 75% | 0/4, 0% | 0/4, 0% | 4/4, 100% | 0/4, 0% |
| Meglumine antimoniate (n = 10) | 0/10, 0% | 8/10, 80% | 2/10, 20% | 0/10, 0% | 3/10, 30% | 7/10, 70% |
| Control group (n = 9): diluent (n = 5) + TLR4a (n = 4) | 7/9, 78% | 2/9, 22% | 0/9, 0% | 5/9, 56% | 3/9, 33% | 1/9, 11% |
| Total (n = 28) | 9 | 16 | 3 | 6 | 12 | 10 |
| Number of Seropositive Dogs (%) | Median ELISA Units (min-max) | Number of LSA IFN-γ Producers (%) | Median LSA IFN-γ (pg/mL) (min-max) | Number of LSA IL-17a Producers (%) | Median LSA IL-17a (pg/mL) (min-max) | PCR Positives (%) | Mean Cq ± SD | Mean NBT Rate ± SD (%) | |
|---|---|---|---|---|---|---|---|---|---|
| Day 0 | 6/24 (25%) | 21.4 (2.8–227.1) | 12/24 (50%) | 127.9 (0–3998) | 10/24 (42%) | 23.2 (0–1933) | 13 (54.2) | 34.7 ± 2.1 | 18 ± 6% |
| Day 15 | 8/23 (34.8%) | 17.8 (3.5–167.4) | - | - | - | - | - | ||
| Day 30 | 6/20 (30%) | 13.8 (2.9–121.6) | 9/20 (45%) | 61.7 (0–3614) | 11/20 (55%) | 85.2 (0–630.3) | 4 (20) | 37.1 ± 0.5 | 19± 5% |
| Day 60 | 4/14 (28.6%) | 13.3 (3.8–115.5) | - | - | - | - | - | ||
| Day 90 | 1/15 (6.7%) | 12.4 (2.8–161.6) | 9/12 (75%) | 444.1 (4.6–6002.9) | |||||
| Day 180 | 0/13 (0%) | 9.58 (3–26) | 5/11 (45.5%) | 41.6 (0–2660) | |||||
| Day 365 | 1/13 (8%) | 16.3 (2.4–213.7) | 5/12 (41.7%) | 1250.2 (0–6947.7) | 12 (92.3) | 34.7 ± 1.2 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martínez-Flórez, I.; Guerrero, M.J.; Dalmau, A.; Cabré, M.; Alcover, M.M.; Berenguer, D.; Good, L.; Fisa, R.; Riera, C.; Ordeix, L.; et al. Effect of Local Administration of Meglumine Antimoniate and Polyhexamethylene Biguanide Alone or in Combination with a Toll-like Receptor 4 Agonist for the Treatment of Papular Dermatitis due to Leishmania infantum in Dogs. Pathogens 2023, 12, 821. https://doi.org/10.3390/pathogens12060821
Martínez-Flórez I, Guerrero MJ, Dalmau A, Cabré M, Alcover MM, Berenguer D, Good L, Fisa R, Riera C, Ordeix L, et al. Effect of Local Administration of Meglumine Antimoniate and Polyhexamethylene Biguanide Alone or in Combination with a Toll-like Receptor 4 Agonist for the Treatment of Papular Dermatitis due to Leishmania infantum in Dogs. Pathogens. 2023; 12(6):821. https://doi.org/10.3390/pathogens12060821
Chicago/Turabian StyleMartínez-Flórez, Icíar, Maria Jose Guerrero, Annabel Dalmau, Maria Cabré, Maria Magdalena Alcover, Diana Berenguer, Liam Good, Roser Fisa, Cristina Riera, Laura Ordeix, and et al. 2023. "Effect of Local Administration of Meglumine Antimoniate and Polyhexamethylene Biguanide Alone or in Combination with a Toll-like Receptor 4 Agonist for the Treatment of Papular Dermatitis due to Leishmania infantum in Dogs" Pathogens 12, no. 6: 821. https://doi.org/10.3390/pathogens12060821