
Mucosal Antibody Response to SARS-CoV-2 in Paediatric and Adult Patients: A Longitudinal Study

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Results
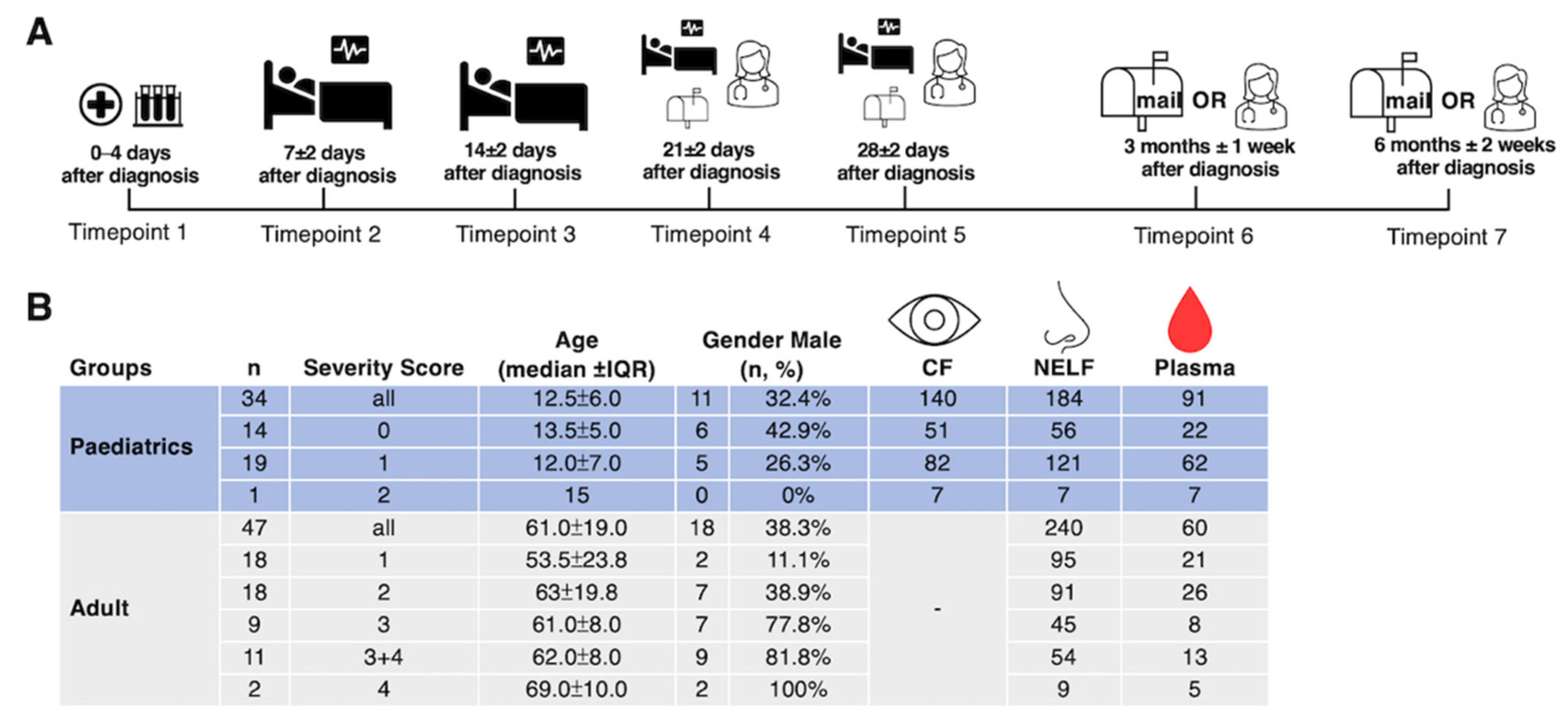
2.1. Demographics of the Subjects
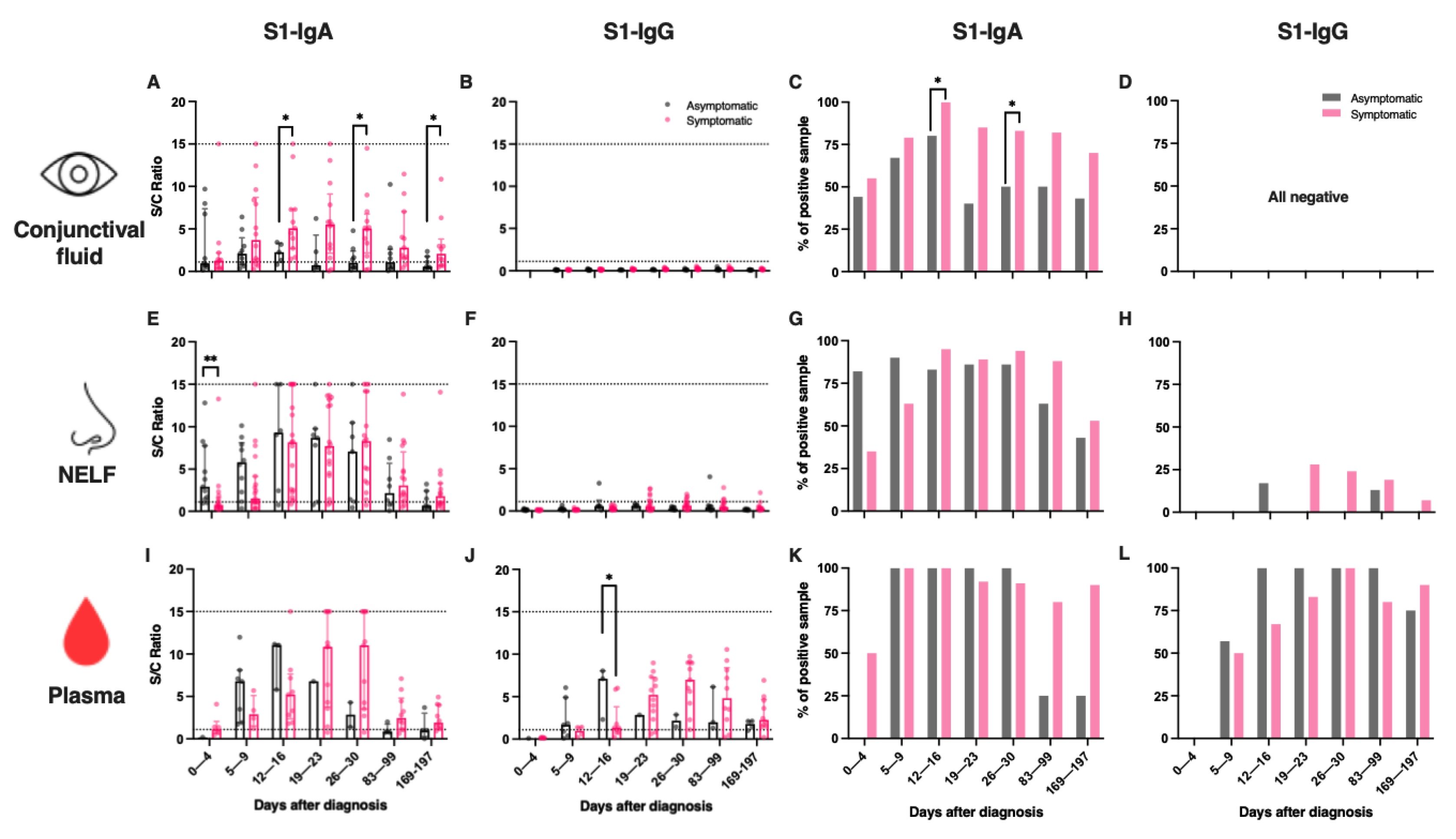
2.2. SARS-CoV-2 S1-Specific IgA Dominated Conjunctival and Nasal Epithelial Lining Fluids
2.3. Symptomatic COVID-19 Paediatric Patients Had a Higher Level of IgA in CF
2.4. Asymptomatic Paediatric Patients Had an Early Induction of IgA in Their Nasal Mucosa and a Higher Level of IgG in Their Plasma
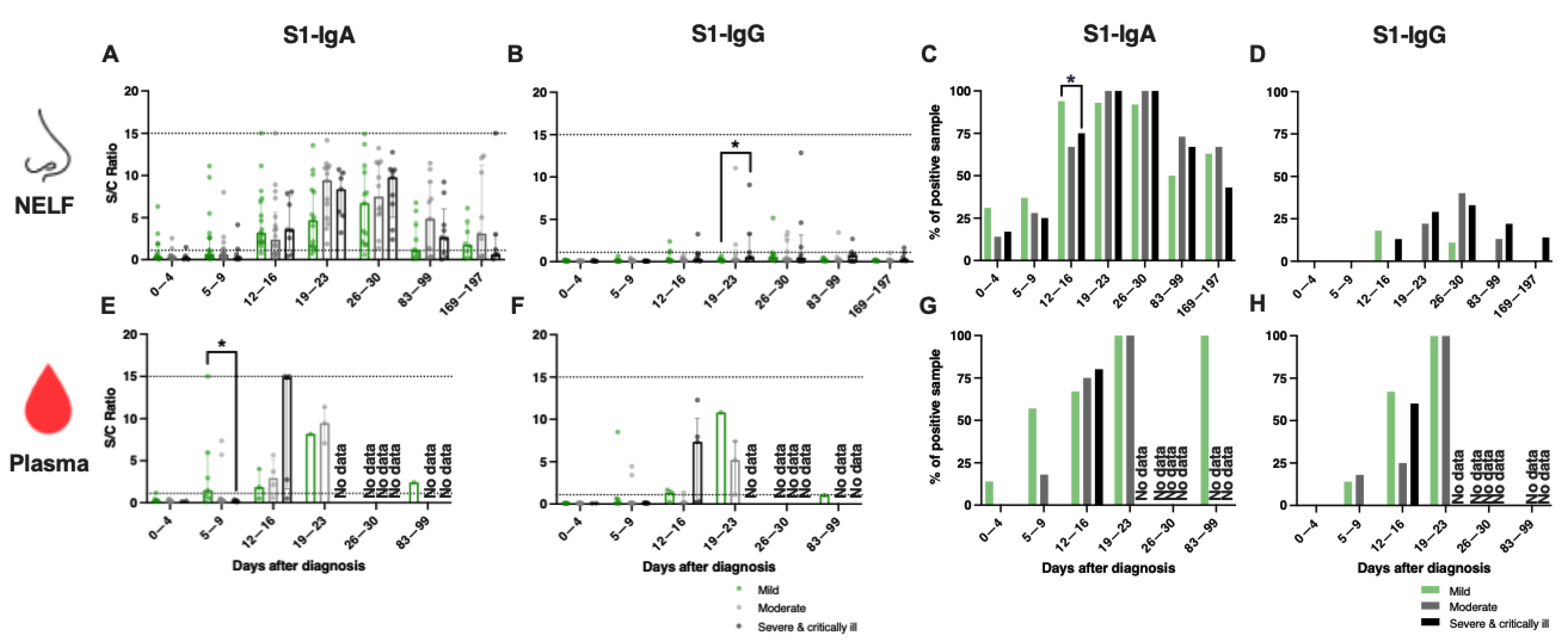
2.5. A Similar Percentage of IgA-Positive NELF in Adult Patients of Different Disease Severity
2.6. Early Induction of IgA in the Plasma of Adult Patients with Mild Disease
2.7. Symptomatic Paediatric Patients Had a Higher Level of IgA in Their Plasma during the Early Phase of SARS-CoV-2 Infection Than Adult Patients with Mild Disease
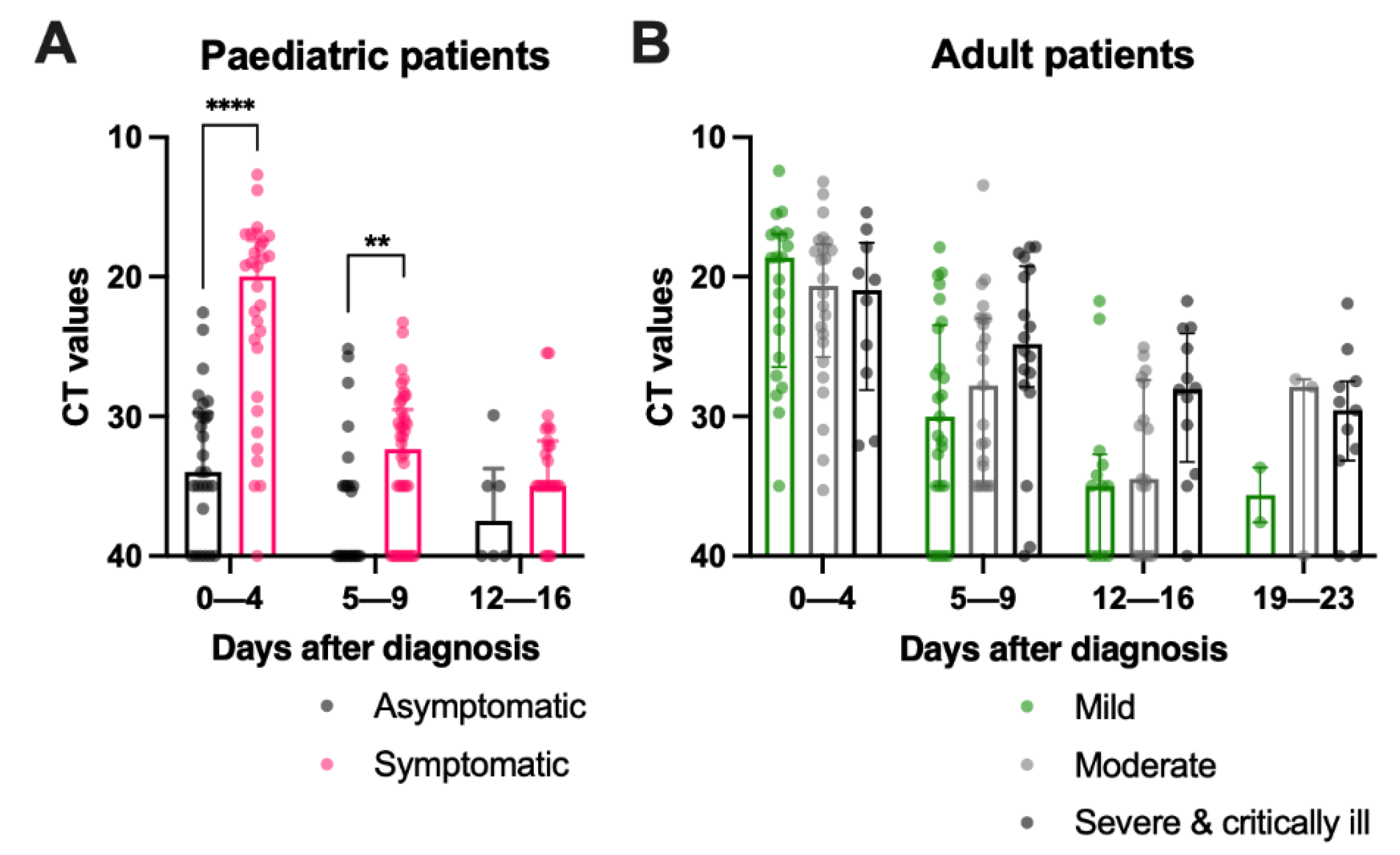
2.8. Asymptomatic Paediatric Patients Had a Lower Viral Load during Admission, while Adult Patients with Mild Disease Had a Sharp Reduction in Viral Load in the First Week after Diagnosis
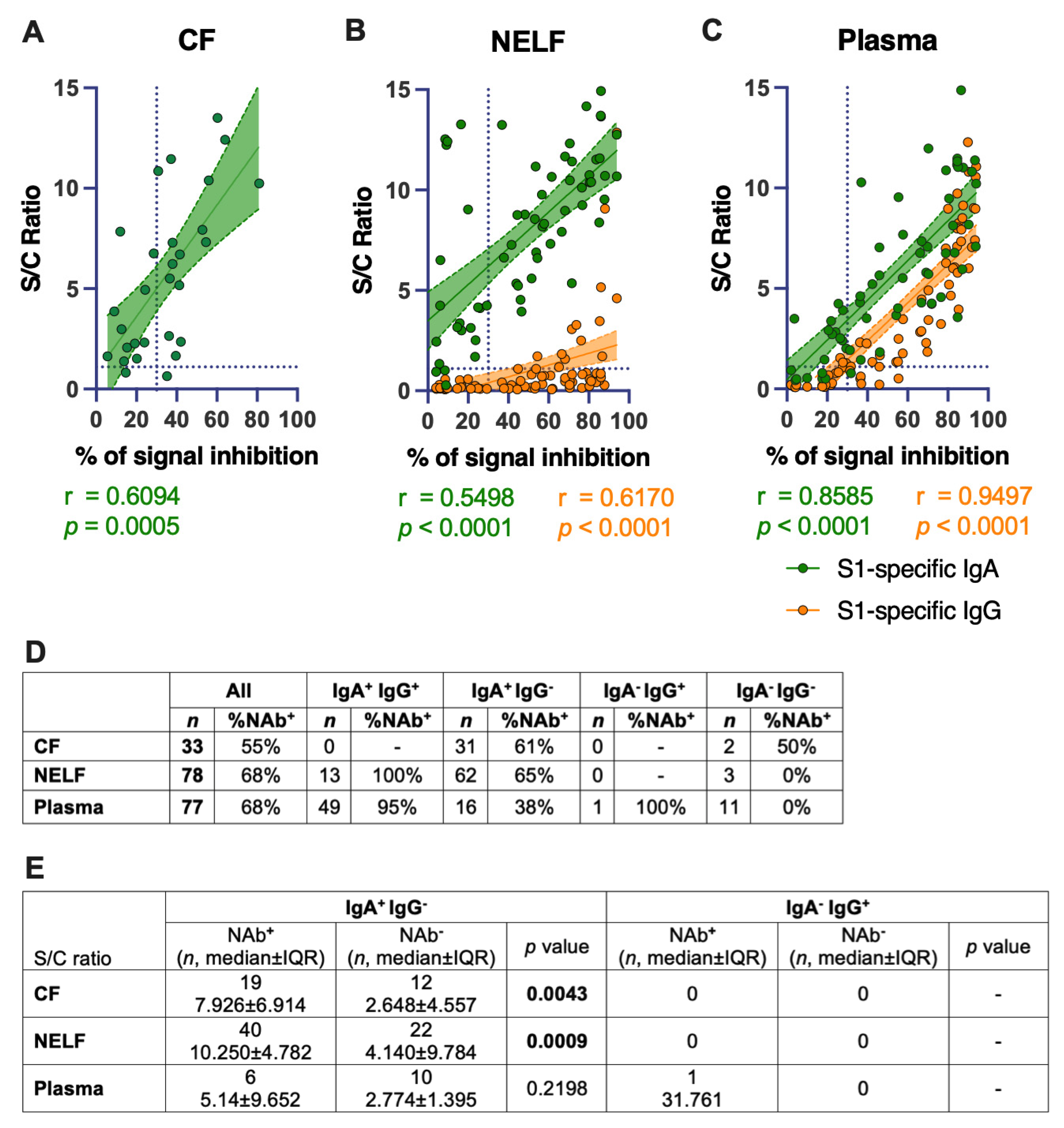
2.9. IgA Levels Correlated Positively with the SARS-CoV-2-Neutralizing Effect of the Mucosal and Plasma Samples
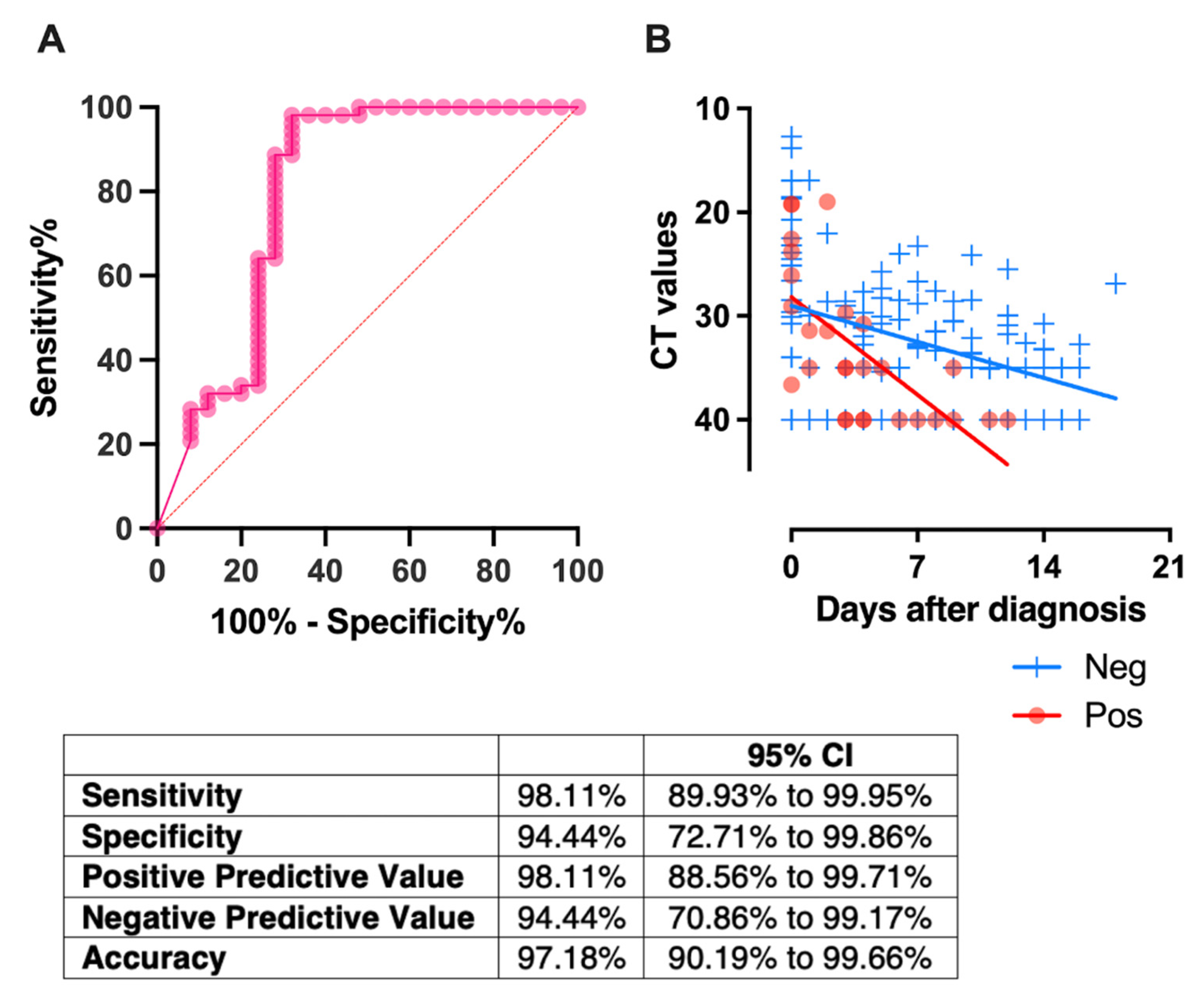
2.10. Receptor-Blocking IgA in NELF, Detected in the First Week of Diagnosis, Correlated with a Rapid Decrease in Viral Load
3. Discussion
4. Materials and Methods
4.1. Subject Recruitment
4.2. Severity Scoring
4.3. Asymptomatic Paediatric Subject Recruitment
4.4. CF and NELF Collection
4.5. Elution of CF and NELF and the Preparation of Plasma
4.6. Measurement of SARS-CoV-2 Spike Protein-Specific IgA and IgG
4.7. Measurement of SARS-CoV-2 Neutralizing Antibody (NAb)
4.8. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sungnak, W.; Huang, N.; Becavin, C.; Berg, M.; Queen, R.; Litvinukova, M.; Talavera-Lopez, C.; Maatz, H.; Reichart, D.; Sampaziotis, F.; et al. SARS-CoV-2 entry factors are highly expressed in nasal epithelial cells together with innate immune genes. Nat. Med. 2020, 26, 681–687. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walls, A.C.; Park, Y.-J.; Tortorici, M.A.; Wall, A.; McGuire, A.T.; Veesler, D. Structure, Function, and Antigenicity of the SARS-CoV-2 Spike Glycoprotein. Cell 2020, 181, 281–292.e6. [Google Scholar] [CrossRef] [PubMed]
- Baig, A.M.; Ahmad, S.; Khaleeq, A.; Rafique, H.; Rajput, S.; Angez, M.; Hameed, A.; Nawaz, T.; Katyara, P. Ocular COVID-19: Eyes as a Reservoir to Conceal and Spread SARSCoV-2. Infect. Disord. Drug Targets 2021, 21, 480–483. [Google Scholar] [CrossRef] [PubMed]
- Ma, R.; Gan, L.; Jiang, S.; Ding, P.; Chen, D.; Wu, J.; Qian, J. High expression of SARS-CoV-2 entry factors in human conjunctival goblet cells. Exp. Eye Res. 2021, 205, 108501. [Google Scholar] [CrossRef]
- Cervia, C.; Nilsson, J.; Zurbuchen, Y.; Valaperti, A.; Schreiner, J.; Wolfensberger, A.; Raeber, M.E.; Adamo, S.; Weigang, S.; Emmenegger, M.; et al. Systemic and mucosal antibody responses specific to SARS-CoV-2 during mild versus severe COVID-19. J. Allergy Clin. Immunol. 2021, 147, 545–557.e9. [Google Scholar] [CrossRef]
- Zhao, J.; Yuan, Q.; Wang, H.; Liu, W.; Liao, X.; Su, Y.; Wang, X.; Yuan, J.; Li, T.; Li, J.; et al. Antibody Responses to SARS-CoV-2 in Patients With Novel Coronavirus Disease 2019. Clin. Infect. Dis. 2020, 71, 2027–2034. [Google Scholar] [CrossRef]
- Long, Q.-X.; Liu, B.-Z.; Deng, H.-J.; Wu, G.-C.; Deng, K.; Chen, Y.-K.; Liao, P.; Qiu, J.-F.; Lin, Y.; Cai, X.-F.; et al. Antibody responses to SARS-CoV-2 in patients with COVID-19. Nat. Med. 2020, 26, 845–848. [Google Scholar] [CrossRef] [PubMed]
- Kiyono, H.; Fukuyama, S. NALT- versus PEYER’S-patch-mediated mucosal immunity. Nat. Rev. Immunol. 2004, 4, 699–710. [Google Scholar] [CrossRef] [PubMed]
- Gallo, O.; Locatello, L.G.; Mazzoni, A.; Novelli, L.; Annunziato, F. The central role of the nasal microenvironment in the transmission, modulation, and clinical progression of SARS-CoV-2 infection. Mucosal Immunol. 2021, 14, 305–316. [Google Scholar] [CrossRef] [PubMed]
- Knop, N.; Knop, E. Conjunctiva-associated lymphoid tissue in the human eye. Investig. Ophthalmol. Vis. Sci. 2000, 41, 1270–1279. [Google Scholar]
- Tschernig, T.; Pabst, R. Bronchus-Associated Lymphoid Tissue (BALT) Is Not Present in the Normal Adult Lung but in Different Diseases. Pathobiology 2000, 68, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Xu, B.; Wagner, N.; Pham, L.N.; Magno, V.; Shan, Z.; Butcher, E.C.; Michie, S.A. Lymphocyte Homing to Bronchus-associated Lymphoid Tissue (BALT) Is Mediated by L-selectin/PNAd, α4β1 Integrin/VCAM-1, and LFA-1 Adhesion Pathways. J. Exp. Med. 2003, 197, 1255–1267. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johansen, F.-E.; Baekkevold, E.S.; Carlsen, H.S.; Farstad, I.N.; Soler, D.; Brandtzaeg, P. Regional induction of adhesion molecules and chemokine receptors explains disparate homing of human B cells to systemic and mucosal effector sites: Dispersion from tonsils. Blood 2005, 106, 593–600. [Google Scholar] [CrossRef] [PubMed]
- Chen, K.; Magri, G.; Grasset, E.K.; Cerutti, A. Rethinking mucosal antibody responses: IgM, IgG and IgD join IgA. Nat. Rev. Immunol. 2020, 20, 427–441. [Google Scholar] [CrossRef]
- Suzuki, T.; Kawaguchi, A.; Ainai, A.; Tamura, S.-I.; Ito, R.; Multihartina, P.; Setiawaty, V.; Pangesti, K.N.A.; Odagiri, T.; Tashiro, M.; et al. Relationship of the quaternary structure of human secretory IgA to neutralization of influenza virus. Proc. Natl. Acad. Sci. USA 2015, 112, 7809–7814. [Google Scholar] [CrossRef] [Green Version]
- Wang, Z.; Lorenzi, J.C.C.; Muecksch, F.; Finkin, S.; Viant, C.; Gaebler, C.; Cipolla, M.; Hoffmann, H.-H.; Oliveira, T.Y.; Oren, D.A.; et al. Enhanced SARS-CoV-2 neutralization by dimeric IgA. Sci. Transl. Med. 2021, 13, eabf1555. [Google Scholar] [CrossRef] [PubMed]
- Ejemel, M.; Li, Q.; Hou, S.; Schiller, Z.A.; Tree, J.A.; Wallace, A.; Amcheslavsky, A.; Yilmaz, N.K.; Buttigieg, K.R.; Elmore, M.J.; et al. A cross-reactive human IgA monoclonal antibody blocks SARS-CoV-2 spike-ACE2 interaction. Nat. Commun. 2020, 11, 4198. [Google Scholar] [CrossRef]
- Sterlin, D.; Mathian, A.; Miyara, M.; Mohr, A.; Anna, F.; Claër, L.; Quentric, P.; Fadlallah, J.; Devilliers, H.; Ghillani, P.; et al. IgA dominates the early neutralizing antibody response to SARS-CoV-2. Sci. Transl. Med. 2021, 13, eabd2223. [Google Scholar] [CrossRef] [PubMed]
- Giannaccare, G.; Blalock, W.; Fresina, M.; Vagge, A.; Versura, P. Intolerant contact lens wearers exhibit ocular surface impairment despite 3 months wear discontinuation. Graefe’s Arch. Clin. Exp. Ophthalmol. 2016, 254, 1825–1831. [Google Scholar] [CrossRef]
- VanDerMeid, K.R.; Su, S.P.; Krenzer, K.L.; Ward, K.W.; Zhang, J.-Z. A method to extract cytokines and matrix metalloproteinases from Schirmer strips and analyze using Luminex. Mol. Vis. 2011, 17, 1056–1063. [Google Scholar] [PubMed]
- Ambrose, C.S.; Wu, X.; Jones, T.; Mallory, R.M. The role of nasal IgA in children vaccinated with live attenuated influenza vaccine. Vaccine 2012, 30, 6794–6801. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hansel, T.T.; Tunstall, T.; Trujillo-Torralbo, M.-B.; Shamji, B.; Del-Rosario, A.; Dhariwal, J.; Kirk, P.; Stumpf, M.P.; Koopmann, J.; Telcian, A.; et al. A Comprehensive Evaluation of Nasal and Bronchial Cytokines and Chemokines Following Experimental Rhinovirus Infection in Allergic Asthma: Increased Interferons (IFN-γ and IFN-lambda;) and Type 2 Inflammation (IL-5 and IL-13). EBioMedicine 2017, 19, 128–138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chan, R.W.; Chan, K.C.; Chan, K.Y.; Lui, G.C.; Tsun, J.G.; Wong, R.Y.; Yu, M.W.; Wang, M.H.; Chan, P.K.; Lam, H.S.; et al. SARS-CoV-2 detection by nasal strips: A superior tool for surveillance of paediatric population. J. Infect. 2021, 82, 84–123. [Google Scholar] [CrossRef] [PubMed]
- Ejemel, M.; Li, Q.; Hou, S.; Schiller, Z.A.; Wallace, A.L.; Amcheslavsky, A.; Yilmaz, N.K.; Toomey, J.R.; Schneider, R.; Close, B.J.; et al. IgA MAb blocks SARS-CoV-2 Spike-ACE2 interaction providing mucosal immunity. bioRxiv 2020. [Google Scholar] [CrossRef]
- Wilbanks, G.A.; Streilein, J.W. Distinctive humoral immune responses following anterior chamber and intravenous administration of soluble antigen. Evidence for active suppression of IgG2-secreting B lymphocytes. Immunology 1990, 71, 566–572. [Google Scholar] [PubMed]
- Steven, P.; Gebert, A. Conjunctiva-Associated Lymphoid Tissue–Current Knowledge, Animal Models and Experimental Prospects. Ophthalmic Res. 2009, 42, 2–8. [Google Scholar] [CrossRef]
- Caselli, E.; Soffritti, I.; Lamberti, G.; D’Accolti, M.; Franco, F.; Demaria, D.; Contoli, M.; Passaro, A.; Contini, C.; Perri, P. Anti-SARS-Cov-2 IgA Response in Tears of COVID-19 Patients. Biology 2020, 9, 374. [Google Scholar] [CrossRef]
- Chan, R.W.Y.; Liu, S.; Cheung, J.Y.; Tsun, J.G.S.; Chan, K.C.; Chan, K.Y.Y.; Fung, G.P.G.; Li, A.M.; Lam, H.S. The Mucosal and Serological Immune Responses to the Novel Coronavirus (SARS-CoV-2) Vaccines. Front. Immunol. 2021, 12, 12:744887. [Google Scholar] [CrossRef] [PubMed]
- Russell, M.W.; Moldoveanu, Z.; Ogra, P.L.; Mestecky, J. Mucosal Immunity in COVID-19: A Neglected but Critical Aspect of SARS-CoV-2 Infection. Front. Immunol. 2020, 11, 611337. [Google Scholar] [CrossRef]
- Callow, K.A. Effect of specific humoral immunity and some non-specific factors on resistance of volunteers to respiratory coronavirus infection. J. Hyg. 1985, 95, 173–189. [Google Scholar] [CrossRef] [Green Version]
- Yan, X.; Chen, G.; Jin, Z.; Zhang, Z.; Zhang, B.; He, J.; Yin, S.; Huang, J.; Fan, M.; Li, Z.; et al. Anti-SARS-CoV-2 IgG levels in relation to disease severity of COVID-19. J. Med. Virol. 2021, 94, 380–383. [Google Scholar] [CrossRef] [PubMed]
- Isho, B.; Abe, K.T.; Zuo, M.; Jamal, A.J.; Rathod, B.; Wang, J.H.; Li, Z.; Chao, G.; Rojas, O.L.; Bang, Y.M.; et al. Persistence of serum and saliva antibody responses to SARS-CoV-2 spike antigens in COVID-19 patients. Sci. Immunol. 2020, 5, eabe5511. [Google Scholar] [CrossRef] [PubMed]
- Imai, K.; Kitagawa, Y.; Tabata, S.; Kubota, K.; Nagura-Ikeda, M.; Matsuoka, M.; Miyoshi, K.; Sakai, J.; Ishibashi, N.; Tarumoto, N.; et al. Antibody response patterns in COVID-19 patients with different levels of disease severity in Japan. J. Med. Virol. 2021, 93, 3211–3218. [Google Scholar] [CrossRef]
- Chan, R.W.Y.; Liu, S.; Cheung, J.; Tsun, J.G.S.; Chan, K.; Chan, K.Y.Y.; Fung, G.P.G.; Li, A.; Lam, H.S. Study on the mucosal and serological immune response to the Novel Coronavirus (SARS-CoV-2) vaccines. medRxiv 2021. [Google Scholar] [CrossRef]
- Smith, N.; Goncalves, P.; Charbit, B.; Grzelak, L.; Beretta, M.; Planchais, C.; Bruel, T.; Rouilly, V.; Bondet, V.; Hadjadj, J.; et al. Distinct systemic and mucosal immune responses during acute SARS-CoV-2 infection. Nat. Immunol. 2021, 22, 1428–1439. [Google Scholar] [CrossRef] [PubMed]
- Long, Q.-X.; Tang, X.-J.; Shi, Q.-L.; Li, Q.; Deng, H.-J.; Yuan, J.; Hu, J.-L.; Xu, W.; Zhang, Y.; Lv, F.-J.; et al. Clinical and immunological assessment of asymptomatic SARS-CoV-2 infections. Nat. Med. 2020, 26, 1200–1204. [Google Scholar] [CrossRef] [PubMed]
- Hachim, A.; Kavian, N.; Cohen, C.A.; Chin, A.W.H.; Chu, D.K.W.; Mok, C.K.P.; Tsang, O.T.Y.; Yeung, Y.C.; Perera, R.A.P.M.; Poon, L.L.M.; et al. ORF8 and ORF3b antibodies are accurate serological markers of early and late SARS-CoV-2 infection. Nat. Immunol. 2020, 21, 1293–1301. [Google Scholar] [CrossRef]
- Dowell, A.C.; Butler, M.S.; Jinks, E.; Tut, G.; Lancaster, T.; Sylla, P.; Begum, J.; Bruton, R.; Pearce, H.; Verma, K.; et al. Children develop robust and sustained cross-reactive spike-specific immune responses to SARS-CoV-2 infection. Nat. Immunol. 2021, 23, 1–10. [Google Scholar] [CrossRef]
- Dugas, M.; Grote-Westrick, T.; Merle, U.; Fontenay, M.; Kremer, A.E.; Hanses, F.; Vollenberg, R.; Lorentzen, E.; Tiwari-Heckler, S.; Duchemin, J.; et al. Lack of antibodies against seasonal coronavirus OC43 nucleocapsid protein identifies patients at risk of critical COVID-19. J. Clin. Virol. 2021, 139, 104847. [Google Scholar] [CrossRef]
- World Health Organization. COVID-19 Clinical Management; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]





 and below
and below  the thresholds level are plotted against time. For this panel data, a fixed-effect regression model was applied to compare the changes of the CT values across time between these 2 groups. A statistically significant difference was found in the decline rate of the viral load at p = 0.002.
and below the thresholds level are plotted against time. For this panel data, a fixed-effect regression model was applied to compare the changes of the CT values across time between these 2 groups. A statistically significant difference was found in the decline rate of the viral load at p = 0.002.
the thresholds level are plotted against time. For this panel data, a fixed-effect regression model was applied to compare the changes of the CT values across time between these 2 groups. A statistically significant difference was found in the decline rate of the viral load at p = 0.002.
and below the thresholds level are plotted against time. For this panel data, a fixed-effect regression model was applied to compare the changes of the CT values across time between these 2 groups. A statistically significant difference was found in the decline rate of the viral load at p = 0.002.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Nasal Epithelial Lining Fluid (NELF) | ||||||||
|---|---|---|---|---|---|---|---|---|
| Days Post Diagnosis | IgA | 0–4 | 5–9 | 12–16 | 19–23 | 26–30 | 83–99 | 169–197 |
| Symptomatic paediatric patients | n | 17 | 19 | 19 | 18 | 17 | 16 | 15 |
| Median ± IQR | 0.7 ± 0.13 | 1.5 ± 3.1 | 8.2 ± 12.7 | 7.7 ± 8.8 | 8.3 ± 10.7 | 3.1 ± 5.6 | 1.8 ± 2.4 | |
| % | 35 | 63 | 95 | 89 | 94 | 88 | 53 | |
| Adult patients with mild disease | n | 13 | 17 | 18 | 15 | 14 | 10 | 8 |
| Median ± IQR | 0.3 ± 1.7 | 1.1 ± 4.0 | 3.4 ± 5.5 | 4.7 ± 6.7 | 5.9 ± 8.5 | 1.1 ± 4.2 | 1.7 ± 3.9 | |
| % | 31 | 47 | 89 | 93 | 93 | 50 | 63 | |
| Mann-Whitney test between groups | 0.3203 | 0.2676 | 0.1701 | 0.1004 | 0.2619 | 0.1089 | 0.8746 | |
| Fisher’s Exact test between groups | ns | 0.5027 | 0.6039 | ns | ns | 0.0687 | ns | |
| IgG | ||||||||
| Symptomatic paediatric patients | n | 16 | 18 | 18 | 18 | 17 | 16 | 15 |
| Median ± IQR | 0.1 ± 0.0 | 0.1 ± 0.1 | 0.2 ± 0.2 | 0.5 ± 1.2 | 0.6 ± 1.0 | 0.4 ± 0.8 | 0.2 ± 0.3 | |
| % | 0 | 0 | 0 | 28 | 24 | 19 | 7 | |
| Adult with mild disease | n | 10 | 10 | 10 | 10 | 9 | 8 | 7 |
| Median ± IQR | 0.1 ± 0.1 | 0.1 ± 0.1 | 0.1 ± 1.0 | 0.2 ± 0.2 | 0.6 ± 0.8 | 0.1 ± 0.3 | 0.1 ± 0.1 | |
| % | 0 | 0 | 20 | 0 | 11 | 0 | 0 | |
| Mann-Whitney test between groups | 0.8664 | 0.1632 | 0.2400 | 0.0821 | 0.6723 | 0.0034 | 0.0085 | |
| Fisher’s Exact test between groups | ns | ns | 0.1190 | 0.1282 | 0.6279 | 0.5257 | ns | |
| Plasma | ||||||||
|---|---|---|---|---|---|---|---|---|
| Days Post Diagnosis | IgA | 0–4 | 5–9 | 12–16 | 19–23 | 26–30 | 83–99 | 169–197 |
| Symptomatic paediatric patients | n | 6 | 4 | 9 | 12 | 11 | 10 | 10 |
| Median ± IQR | 1.1 ± 1.4 | 2.9 ± 3.6 | 5.2 ± 5.3 | 10.9 ± 11.2 | 11.0 ± 11.5 | 2.5 ± 3.7 | 1.9 ± 2.8 | |
| % | 50 | 100 | 100 | 92 | 91 | 80 | 90 | |
| Adult patients with mild disease | n | 7 | 8 | 4 | 1 | 0 | 1 | 0 |
| Median ± IQR | 0.2 ± 0.3 | 2.2 ± 4.9 | 2.9 ± 7.3 | 8.2 | 2.4 | - | ||
| % | 14 | 63 | 75 | 100 | - | 100 | - | |
| Mann-Whitney test between groups | p value | 0.0082 | 0.8081 | 0.5035 | - | - | - | - |
| Fisher’s Exact test between groups | p value | 0.2657 | 0.4909 | 0.3077 | - | - | - | - |
| IgG | ||||||||
| Symptomatic paediatric patients | n | 6 | 4 | 9 | 12 | 11 | 10 | 10 |
| Median ± IQR | 0.1 ± 0.1 | 1.0 ± 1.1 | 1.3 ± 3.0 | 5.2 ± 4.7 | 7.0 ± 4.8 | 4.8 ± 6.6 | 2.3 ± 3.2 | |
| % | 0 | 50 | 67 | 83 | 100 | 80 | 90 | |
| Adult with mild disease | n | 7 | 8 | 4 | 1 | 0 | 1 | 0 |
| Median ± IQR | 0.1 ± 0.0 | 0.3 ± 0.7 | 1.5 ± 1.8 | 10.8 | - | 1.1 | - | |
| % | 0 | 13 | 75 | 100 | - | 0 | - | |
| Mann-Whitney test between groups | p value | 0.0734 | 0.2828 | 0.8252 | - | - | - | - |
| Fisher’s Exact test between groups | p value | ns | 0.2364 | ns | - | - | - | - |
| A. CT Values | ||||||
|---|---|---|---|---|---|---|
| Days Post-Diagnosis | 0–4 | 5–9 | 12–16 | 19–23 | 26–30 | |
| Paediatric patients | ||||||
| Asymptomatic | n | 29 | 23 | 6 | 0 | 0 |
| Median range | 34.0 22.6–40.0 | 40.0 25.12–40.0 | 37.5 29.9–40.0 | - | - | |
| Symptomatic | n | 30 | 42 | 24 | 1 | 0 |
| Median range | 20.0 12.7–27.3 | 32.3 23.3–40.0 | 35.0 25.4–40.0 | 40.0 - | - | |
| Mann–Whitney test between groups | p value | <0.0001 | 0.0234 | 0.2218 | - | - |
| Adult patients | ||||||
| Mild disease | n | 21 | 25 | 12 | 2 | 0 |
| Median range | 18.6 12.4–35.0 | 30.0 17.9–40.0 | 35.0 21.7–40.0 | 35.6 33.7–37.6 | - | |
| Moderate disease | n | 24 | 23 | 17 | 3 | 1 |
| Median range | 20.7 13.2–35.3 | 27.8 13.4–35.0 | 34.5 25.1–40.0 | 27.9 27.4–40.0 | 35.0 - | |
| Severe and critically ill | n | 10 | 18 | 12 | 11 | 1 |
| Median range | 21.0 15.4–32.1 | 24.8 17.9–40.0 | 28.0 21.7–40.0 | 29.6 21.9–40.0 | 30.0 - | |
| Kruskal–Wallis test among adult groups | p value | 0.7533 | 0.0938 | 0.0689 | 0.4966 | - |
| Kruskal–Wallis test among all groups | p value | <0.0001 | <0.0001 | 0.0157 | - | - |
| Dunn’s multiple comparisons test | ||||||
| Asymptomatic vs symptomatic paediatric patients | <0.0001 | 0.6680 | ns | - | - | |
| Asymptomatic paediatric patients vs. adult patients—mild disease | <0.0001 | 0.0107 | ns | - | - | |
| Asymptomatic paediatric patients vs. adult patients—moderate disease | <0.0001 | 0.0004 | ns | - | - | |
| Asymptomatic paediatric patients vs. adult patients—severe and critically ill | 0.0024 | <0.0001 | 0.0328 | - | - | |
| Symptomatic paediatric patients vs. adult patients—mild disease | ns | 0.631 | ns | - | - | |
| Symptomatic paediatric patients vs. adult patients—moderate disease | ns | 0.0466 | ns | - | - | |
| Symptomatic paediatric patients vs. adult patients—severe and critically ill | ns | 0.0007 | 0.0361 | - | - | |
| Adult patients: mild disease vs. moderate disease | ns | ns | ns | - | - | |
| Adult patients: mild disease vs. severe and critically ill | ns | 0.3646 | ns | - | - | |
| Adult patients: mild disease vs. severe and critically ill | ns | ns | ns | - | - | |
| Days Post-Diagnosis | 0–4 vs. 5–9 | 0–4 vs. 12–16 | 0–4 vs. 19–23 | 5–9 vs. 12–16 | 5–9 vs. 19–23 | 12–16 vs. 19–23 |
|---|---|---|---|---|---|---|
| Asymptomatic paediatric patients | 0.0564 | ns | - | ns | - | - |
| Symptomatic paediatric patients | ns | <0.0001 | - | <0.0001 | - | - |
| Adult patients—mild disease | <0.0001 | 0.0006 | - | ns | - | - |
| Adult patients—moderate disease | 0.0012 | 0.0053 | 0.0075 | ns | ns | ns |
| Adult patients—severe & critically ill | ns | ns | 0.0593 | ns | 0.1322 | 0.8198 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chan, R.W.Y.; Chan, K.C.C.; Lui, G.C.Y.; Tsun, J.G.S.; Chan, K.Y.Y.; Yip, J.S.K.; Liu, S.; Yu, M.W.L.; Ng, R.W.Y.; Chong, K.K.L.; et al. Mucosal Antibody Response to SARS-CoV-2 in Paediatric and Adult Patients: A Longitudinal Study. Pathogens 2022, 11, 397. https://doi.org/10.3390/pathogens11040397
Chan RWY, Chan KCC, Lui GCY, Tsun JGS, Chan KYY, Yip JSK, Liu S, Yu MWL, Ng RWY, Chong KKL, et al. Mucosal Antibody Response to SARS-CoV-2 in Paediatric and Adult Patients: A Longitudinal Study. Pathogens. 2022; 11(4):397. https://doi.org/10.3390/pathogens11040397
Chicago/Turabian StyleChan, Renee W. Y., Kate C. C. Chan, Grace C. Y. Lui, Joseph G. S. Tsun, Kathy Y. Y. Chan, Jasmine S. K. Yip, Shaojun Liu, Michelle W. L. Yu, Rita W. Y. Ng, Kelvin K. L. Chong, and et al. 2022. "Mucosal Antibody Response to SARS-CoV-2 in Paediatric and Adult Patients: A Longitudinal Study" Pathogens 11, no. 4: 397. https://doi.org/10.3390/pathogens11040397