
Hymenolepis diminuta Infection in a Romanian Child from an Urban Area
by
 ,
,
Felicia Galoș
1,2, 
Mălina Anghel
1,
Andreea Ioan
1,
Mara-Ioana Ieșanu
1,*,
Cătălin Boboc
1 and
Anca Andreea Boboc
1,2 1
Department of Pediatrics, Marie Curie Emergency Children’s Hospital, 041451 Bucharest, Romania
2
Department of Pediatrics, Carol Davila University of Medicine and Pharmacy, 020021 Bucharest, Romania
*
Author to whom correspondence should be addressed.
Pathogens 2022, 11(3), 322; https://doi.org/10.3390/pathogens11030322
Submission received: 7 February 2022
/
Revised: 2 March 2022
/
Accepted: 3 March 2022
/
Published: 7 March 2022
(This article belongs to the Special Issue Advances in Parasitic Diseases)
{kind=link}
Abstract
:Hymenolepis diminuta is primarily a rodent parasite that is ubiquitously distributed worldwide, but with only a few cases described as human infections. We report a case of Hymenolepis diminuta infection in a 15-month-old child, living in an urban setting, with no previous medical history. The patient presented with two episodes of seizures, and complaints of abdominal pain, vomiting, and diarrhea, with no apparent history of rodent contact. Furthermore, the patient’s gastrointestinal symptoms were linked to the emission of suspected tapeworm proglottids in the feces. After excluding other possible etiologies, a diagnosis of Hymenolepis diminuta infection was made, based on the examination of characteristic eggs in a concentrated stool specimen. The infant was successfully treated with praziquantel and fully recovered. After two weeks, the stool sample was free of Hymenolepis diminuta eggs. The clinical follow-up over the next 3 years was normal. Hymenolepis diminuta is rarely found in humans, and, when present, the infection is frequently asymptomatic. Abdominal pain, irritability, itching, eosinophilia, and seizures have also been reported. In this paper, we report, for the first time in the literature, an infection with Hymenolepis diminuta in a Romanian infant who had atypical neurological presentation, with full recovery, without subsequent neurological sequelae.
1. Introduction
The zoonotic cestode Hymenolepis diminuta (H. diminuta) is primarily a rat tapeworm, found in the small intestine of rodents, which are the definitive hosts. Humans can enter the tapeworm’s life cycle by accidental consumption of infected insects (intermediate hosts), which contain the helminth’s cysticercoids in their body cavity [1].
H. diminuta infection in humans is rare, even in developing countries, typically occurring in isolated cases, such as case reports describing a single affected individual. Surveys of various groups have found infection rates ranging from 0.001 to 5.5%, especially in children [2,3,4,5,6,7,8]. The infection is paucisymptomatic, with pruritus, abdominal pain, and diarrhea as the main manifestations. The diagnosis of H. diminuta infection in humans is confirmed by the presence of the characteristic eggs in the stool sample. Cases have been reported all over the world. In Romania, sporadic cases have also been reported [9,10].
Herein, we report an H. diminuta infection in an infant from a tertiary center in Romania, presenting with afebrile seizures, with a favorable outcome after receiving antiparasitic drugs. To the best of our knowledge, this is the first documented case of H. diminuta infection in a human from Romania, with atypical presentation, such as afebrile seizures.
2. Case Presentation
A 15-month-old female infant, living in the urban area of Bucharest, Romania, was referred to the Emergency Department of Marie Curie Emergency Children’s Hospital for two episodes of generalized tonic–clonic seizures, lasting approximately 10 min, and followed by postictal sleep. The length of time between seizures was 30 min. The onset of symptoms was 24 h before the presentation, with vomiting, mild diarrhea, and abdominal pain, due to the emission of suspected tapeworm proglottids in her stool. The patient’s previous medical history was negative, and she had no recent travel history. The subsequent physical examination, complemented by cerebral computed tomography, electroencephalography, and chest X-ray, was normal. No abnormalities were revealed by blood and urine analyses.
The first seizure episode was treated with diazepam. Phenytoin was introduced after the second seizure, with subsequent tapering for 14 days.
Considering the emission of a suspicious worm in the patient’s stool, a parasitological examination of a concentrated stool sample was performed. Direct microscopic examination of the eggs in an unstained moist mount is required for this investigation. To improve the accuracy of diagnosing infections, concentration techniques and multiple tests are needed. The first examination of the stool sample described parasite eggs of unknown identity. The morphological description revealed spherical eggs, 70 μm in diameter, with a striated outer membrane and a thin inner membrane, containing six central hooklets, but no polar filaments. The diagnosis of H. diminuta infection was subsequently made after consulting an experienced parasitologist. The identified H. diminuta eggs were distinguished from H. nana eggs, which have a similar appearance, but are smaller and feature two evident polar thickenings, from which four to eight polar filaments arise.
Treatment with praziquantel (10 mg/kg/day) was administered for 7 days. After two weeks, the infant was clinically stable and the stool sample was clear of H. diminuta eggs. Follow-up over the subsequent 3 years was marked by normal growth, no seizures, and proper neurological development.
3. Discussion
3.1. Prevalence
The zoonotic cestode H. diminuta belongs to the Hymenolepididae family [1]. H. diminuta infection in humans is uncommon, typically occurring as isolated cases. As a result, only a few hundred cases have been reported, mainly in children [11,12,13,14,15,16,17,18,19,20] and rarely in adults [21,22]. One recent review identified 1561 published records of H. diminuta infection in humans, from 80 countries, estimating the total number of human cases worldwide, mostly with no evidence of the existence of infected rodents [1]. Most of the published literature describes isolated case reports. In Romania, only a couple of human infections were documented. According to the latest report, a routine stool examination revealed H. diminuta eggs in an asymptomatic 3-year-old girl [9].
In other countries, different situations were reported. For example, in a 5-year-old girl infected with H. diminuta, with occasional abdominal pain and anal pruritus, the authors reported cyanosis, loss of consciousness, stiffness of the limbs, followed by drowsiness and hypotonia induced by crying, according to their description [14]. In 1989, a child from Jamaica became the first documented case of H. diminuta in a human in Jamaica, West Indies [23]. H. diminuta eggs were also discovered in a 12-year-old girl residing in a small village in rural India, an area extensively infested with rats and cockroaches [11]. In addition, in an urban area of Rome, a 2-year-old boy was infected with H. diminuta. In this case, however, the investigators found no evidence of rodent or other suspected sources of infection [13], similar to our situation. All these examples emphasize the rarity of H. diminuta infection and its worldwide distribution.
3.2. Life Cycle
First, H. diminuta eggs are passed from the infected definitive host’s feces (e.g., rodents, man). Intermediate hosts, such as arthropods, consume the mature eggs, and oncospheres are released, piercing the host’s intestinal wall. These develop into cysticercoid larvae, which survive as the arthropod develops into adulthood. The mammalian host contracts H. diminuta infection after ingesting a cysticercoid larvae-carrying intermediate host. Humans can become accidentally infected by eating insects from precooked cereals or other foods, as well as directly from the environment (e.g., oral exploration of the environment by children). The contaminated arthropod’s tissue is degraded after ingestion, releasing cysticercoid larvae into the stomach and small intestine. The scolexes are everted shortly after the cysticercoid larvae are expelled.
The parasite attaches to the small intestinal wall using the four suckers on the scolex. The worms mature in 20 days, and adult parasites can grow up to 30 cm in length. Tapeworms are hermaphrodites, and each proglottid carries a set of female and male reproductive organs. Gravid proglottids release eggs into the small intestine, which disintegrate after breaking off from the adult parasites. Finally, the eggs are released into the environment through the feces of the mammalian host [24].
In humans, H. diminuta infection spreads by the consumption of infected intermediate hosts. H. diminuta cysticercoids have been found in more than 30 insect species, including moths, grain beetles, and fleas, as well as other arthropods, such as millipedes [25]. However, due to variances in their distribution, abundance, capability to be infected in multiple phases of their life cycle, and adaptation to survive in anthropogenic ecosystems, it is rather unclear if these insects play a substantial role in the transmission of H. diminuta to humans.
3.3. Symptoms, Treatment, and Outcome
Most human infections with H. diminuta lead to gastrointestinal symptoms, such as abdominal pain and diarrhea, but also fever [1,12,17,18,19,20]. Extraintestinal symptoms, including pruritus, irritability, and arthromyalgia, have also been associated with H. diminuta infection in some cases [1,11,13,14]. A fatal outcome has been reported in an adult patient. However, the infection coexisted with an underlying intra-abdominal malignancy, which made the fatal outcome more likely [21].
H. diminuta infection may also cause eosinophilia, due to mucosal damage to the intestinal villi [1,14,18], but reports on this are inconsistent [1,19].
In terms of therapy, there is no clear evidence of its effectiveness, due to a lack of controlled studies and evidence, suggesting that many infected and untreated patients become asymptomatic over time. Nonetheless, for the treatment of H. diminuta infection, praziquantel seems to be the drug of choice [11,12,15,16,17,18,26], even though its safety profile in the pediatric population is not well established. Niclosamide is a treatment alternative given to children especially, but there is low availability of this drug in many countries [13,14,21,27,28].
3.4. Hymenolepis Diminuta and Nana Difference
Hymenolepiasis is, in fact, caused by two cestodes species, H. diminuta, the rat tapeworm, and H. nana, the dwarf tapeworm. In humans, infection with H. nana is much more common than infection with H. diminuta. H. nana is probably the tapeworm encountered most in humans, since it can be directly propagated from one person to another, having no need for an intermediate host [29]. Direct human-to-human transmission appears to be the most prevalent route of infection, especially in environments where poor hygiene and inadequate sanitation are present [30,31]. These cestodes have almost identical clinical presentations and alike treatment strategies, with praziquantel being the treatment of choice.
3.5. Hymenolepis Diminuta and Immunity
An interesting feature of H. diminuta infection is that it can act as a promising therapeutic candidate to alleviate inflammatory diseases, which have proven to be resistant to pharmacological interventions. Infection occurs through ingestion, and the worm does not migrate through the host; rather, it remains in the small intestine. Bearing no teeth or hooks, it causes no obvious abrasive damage to the host. It is not auto-infective, as its life cycle requires an intermediate arthropod host, so there is no direct person-to-person spread [33].
This theory is supported by the fact that helminths have evolved to manipulate their hosts’ immune systems [34]. Indeed, animal studies suggest that helminth parasite infection lowers the severity of inflammatory diseases [35,36,37,38,39]. In chronic worm infections, allergic symptoms are common, owing to the persistent state of immunological activation, defined by dominating Th2-type cytokines, including interleukin-10, which has an anti-inflammatory effect, and IgE-mediated responses [40]. Infections with parasitic helminths induce Th2-dominated immunity, while pro-inflammatory Th1 cytokine production is maintained at low levels [40].
3.6. Case Particularities
In the present case, the patient came from an urban area, and the house and its surroundings, as well as the areas frequently visited by the infant, had no evidence of rodents or other possible sources of infection. This may indicate the possibility of another indirect mechanism of transmission, such as food grains from a rat-infested mill or drinking water contaminated with intermediate hosts, adding difficulty to the diagnosis.
The particularity of this case originates from the rarity of H. diminuta infection in humans in Romania, along with the particular presentation. Furthermore, because this infection is more often encountered in tropical and subtropical areas, and Romania has a temperate climate, this occurrence is all the more surprising.
Moreover, the patient had an atypical presentation, with afebrile seizures. Although the first differential diagnosis targeted the causes of seizures during infancy, the results came back negative. The relationship between seizures and H. diminuta infection was difficult to establish because this symptom was unusual. The latest worldwide review of H. diminuta infections did not include seizures as a clinical sign [1]. A single case report was found in the literature describing febrile seizures in a child with H. diminuta infection; however, the patient had a positive medical history for febrile seizures [41].
Regarding laboratory analysis, H. diminuta infection can cause eosinophilia, but in our patient, this finding was not detected.
Praziquantel is the treatment of choice for H. diminuta infection. To ensure parasite eradication, our patient was prescribed praziquantel (10 mg/kg/day) for 7 days, with a good safety profile. The following parasitological examination of the stool revealed no eggs, suggesting that the treatment had high efficacy. However, currently, therapeutic handbooks do not exactly cover the treatment of H. diminuta, possibly due to its low prevalence. Therefore, given the lack of information regarding praziquantel treatment, every case of H. diminuta infection should be recorded, particularly data on treatment procedures, and parasitological and clinical outcomes.
4. Conclusions
We report, for the first time, an H. diminuta infection in a Romanian infant with atypical manifestations, such as generalized seizures and non-specific gastrointestinal symptoms, who made a full recovery following praziquantel treatment. This case report highlights that a precise parasitological diagnosis requires proper district laboratories and qualified personnel.
To increase our understanding regarding the epidemiology, mode of transmission, and therapeutic protocol, and to improve the management of this rare infection, we recommend that every H. diminuta infection in a human should be reported and investigated.
Author Contributions
F.G., M.A.: drafting the original manuscript, collecting data, and literature searching. M.-I.I.: editing the manuscript, critical revision, and literature searching. A.I., C.B.: editing the manuscript. A.A.B., F.G.: editing the manuscript, critical revision, literature searching, and supervision. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Written informed consent has been obtained from the patient and his legal guardian to publish this paper.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Panti-May, J.A.; Rodríguez-Vivas, R.I.; García-Prieto, L.; Servián, A.; Costa, F. Worldwide Overview of Human Infections with Hymenolepis Diminuta. Parasitol. Res. 2020, 119, 1997–2004. [Google Scholar] [CrossRef] [PubMed]
- Lo, C.T.; Ayele, T.; Birrie, H. Helminth and Snail Survey in Harerge Region of Ethiopia with Special Reference to Schistosomiasis. Ethiop. Med. J. 1989, 27, 73–83. [Google Scholar] [PubMed]
- McMillan, B.; Kelly, A.; Walker, J.C. Prevalence of Hymenolepis Diminuta Infection in Man in the New Guinea Highlands. Trop. Geogr. Med. 1971, 23, 390–392. [Google Scholar] [PubMed]
- Mercado, R.; Arias, B. Taenia sp. and other intestinal cestode infections in individuals from public outpatient clinics and hospitals from the northern section of Santiago, Chile (1985–1994). Bol. Chil. Parasitol. 1995, 50, 80–83. [Google Scholar]
- Chung, W.C.; Fan, P.C.; Chiu, H.M. Survey of helminthic infections and treatment of Taenia species infection among the aborigines in Chien-Shih District, Hsin-Chu County, northern Taiwan. Chin. J. Microbiol. Immunol. 1985, 18, 96–103. [Google Scholar]
- Pampiglione, S.; Visconti, S.; Pezzino, G. Human intestinal parasites in Subsaharan Africa. II. Sao Tomé and Principe. Parassitologia 1987, 29, 15–25. [Google Scholar]
- Stafford, E.E.; Sudomo, M.; Masri, S.; Brown, R.J. Human Parasitoses in Bali, Indonesia. Southeast Asian J. Trop. Med. Public Health 1980, 11, 319–323. [Google Scholar]
- Rahman, H.U.; Khan, W.; Mehmood, S.A.; Ahmed, S.; Yasmin, S.; Ahmad, W.; Haq, Z.U.; Shah, M.I.A.; Khan, R.; Ahmad, U.; et al. Prevalence of Cestodes Infection among School Children of Urban Parts of Lower Dir District, Pakistan. Braz. J. Biol. Rev. Brasleira Biol. 2021, 82, e242205. [Google Scholar] [CrossRef]
- Barabas, E.C.; Barabas, A.; Cretu, C.M.; Man, A. Case Report of a Rare Human Parasitic Infection with Hymenolepis Diminuta in Romania. Acta Microbiol. Immunol. Hung. 2016, 64 (Suppl. S1), 8–9. [Google Scholar] [CrossRef] [Green Version]
- Gherman, I.; Juvara, A.M. Considerations on 4 new cases of Hymenolepiasis caused by Hemenolepis diminuta. Rev. Med. Chir. Soc. Med. Nat. Iasi 1964, 68, 193–196. [Google Scholar]
- Tiwari, S.; Karuna, T.; Rautaraya, B. Hymenolepis Diminuta Infection in a Child from a Rural Area: A Rare Case Report. J. Lab. Physicians 2014, 6, 58–59. [Google Scholar] [CrossRef] [PubMed]
- Rohela, M.; Ngui, R.; Lim, Y.A.; Kalaichelvan, B.; Wan Hafiz, W.I.; Mohd Redzuan, A.N. A Case Report of Hymenolepis Diminuta Infection in a Malaysian Child. Trop. Biomed. 2012, 29, 224–230. [Google Scholar] [PubMed]
- Marangi, M.; Zechini, B.; Fileti, A.; Quaranta, G.; Aceti, A. Hymenolepis Diminuta Infection in a Child Living in the Urban Area of Rome, Italy. J. Clin. Microbiol. 2003, 41, 3994–3995. [Google Scholar] [CrossRef] [Green Version]
- Patamia, I.; Cappello, E.; Castellano-Chiodo, D.; Greco, F.; Nigro, L.; Cacopardo, B. A Human Case of Hymenolepis Diminuta in a Child from Eastern Sicily. Korean J. Parasitol. 2010, 48, 167–169. [Google Scholar] [CrossRef] [PubMed]
- Tena, D.; Simón, M.P.; Gimeno, C.; Pomata, M.T.P.; Illescas, S.; Amondarain, I.; González, A.; Domínguez, J.; Bisquert, J. Human Infection with Hymenolepis Diminuta: Case Report from Spain. J. Clin. Microbiol. 1998, 36, 2375–2376. [Google Scholar] [CrossRef] [Green Version]
- Kołodziej, P.; Rzymowska, J.; Stępień-Rukasz, H.; Lorencowicz, R.; Lucińska, M.; Dzióbek, M. Analysis of a Child Infected with Hymenolepis Diminuta in Poland. Ann. Agric. Environ. Med. 2014, 21, 510–511. [Google Scholar] [CrossRef] [Green Version]
- Sharifdini, M.; Hajialilo, E.; Ghanbarzadeh, L.; Saraei, M. Infection with Hymenolepis Diminuta (Rodolphi, 1819) in a Child from North of Iran: Case Report. Iran. J. Public Health 2019, 48, 1528–1531. [Google Scholar] [CrossRef]
- Singh, C.; Sharma, B.; Aneja, A.; Lal, S.B.; Khurana, S. Coinfection with Hymenolepis Nana and Hymenolepis Diminuta Infection in a Child from North India: A Rare Case Report. Trop. Parasitol. 2020, 10, 56–58. [Google Scholar] [CrossRef]
- Gupta, P.; Gupta, P.; Bhakri, B.K.; Kaistha, N.; Omar, B.J. Hymenolepis Diminuta Infection in a School Going Child: First Case Report from Uttarakhand. J. Clin. Diagn. Res. 2016, 10, DD04–DD05. [Google Scholar] [CrossRef]
- Kalaivani, R.; Nandhini, L.; Seetha, K.S. Hymenolepis Diminuta Infection in a School-Going Child: A Rare Case Report. Australas. Med. J. 2014, 7, 379–381. [Google Scholar] [CrossRef]
- Wiwanitkit, V. Overview of Hymenolepis Diminuta Infection Among Thai Patients. Medscape Gen. Med. 2004, 6, 7. [Google Scholar]
- Ahmad, A.F.; Ngui, R.; Ong, J.; Sarip, F.; Ismail, W.H.W.; Omar, H.; Nor, Z.M.; Amir, A.; Lim, Y.A.L.; Mahmud, R. Case Report: A Symptomatic Case of Hymenolepis Diminuta Infection in an Urban-Dwelling Adult in Malaysia. Am. J. Trop. Med. Hyg. 2017, 97, 163–165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cohen, I.P. A Case Report of a Hymenolepis Diminuta Infection in a Child in St James Parish, Jamaica. J. La. State Med. Soc. 1989, 141, 23–24. [Google Scholar]
- Andreassen, J.; Bennet-Jenkins, E.M.; Bryant, C. Immunology and Biochemistry of Hymenolepis Diminuta. Adv. Parasitol. 1999, 42, 223–275. [Google Scholar] [CrossRef]
- Burt, M.D.B. Aspects of the Life History and Systematics of Hymenolepis Diminuta. In Biology of the Tapeworm Hymenolepis Diminuta; Arai, H.P., Ed.; Academic Press: Cambridge, MA, USA, 1980; pp. 1–57. ISBN 978-0-12-058980-7. [Google Scholar]
- Sanford, J.P. The Sanford Guide to Antimicrobial Therapy, 50th ed.; Antimicrobial Therapy: Sperryville, VA, USA, 1996; ISBN 978-1-944272-13-5. [Google Scholar]
- Jones, W.E. Niclosamide as a Treatment for Hymenolepis Diminuta and Dipylidium Caninum Infection in Man. Am. J. Trop. Med. Hyg. 1979, 28, 300–302. [Google Scholar] [CrossRef]
- Hamrick, H.J.; Bowdre, J.H.; Church, S.M. Rat Tapeworm (Hymenolepis Diminuta) Infection in a Child. Pediatr. Infect. Dis. J. 1990, 9, 216–219. [Google Scholar] [CrossRef]
- Schantz, P.M. Tapeworms (Cestodiasis). Gastroenterol. Clin. N. Am. 1996, 25, 637–653. [Google Scholar] [CrossRef]
- Korzeniewski, K.; Augustynowicz, A.; Lass, A. Prevalence of Intestinal Parasites in Afghan Community on the Example of Patients Treated in Ghazni Provincial Hospital. Int. Marit. Health 2014, 65, 68–72. [Google Scholar] [CrossRef] [Green Version]
- Amare, B.; Ali, J.; Moges, B.; Yismaw, G.; Belyhun, Y.; Gebretsadik, S.; Woldeyohannes, D.; Tafess, K.; Abate, E.; Endris, M.; et al. Nutritional Status, Intestinal Parasite Infection and Allergy among School Children in Northwest Ethiopia. BMC Pediatr. 2013, 13, 7. [Google Scholar] [CrossRef] [Green Version]
- Wittner, M.; White, A.C.; Tanowitz, H.B. Chapter 121—Taenia and Other Tapeworm Infections. In Tropical Infectious Diseases: Principles, Pathogens and Practice, 3rd ed.; Guerrant, R.L., Walker, D.H., Weller, P.F., Eds.; W.B. Saunders: Edinburgh, UK, 2011; pp. 839–847. ISBN 978-0-7020-3935-5. [Google Scholar]
- McKay, D.M. The Immune Response to and Immunomodulation by Hymenolepis Diminuta. Parasitology 2010, 137, 385–394. [Google Scholar] [CrossRef]
- Ryan, S.M.; Eichenberger, R.M.; Ruscher, R.; Giacomin, P.R.; Loukas, A. Harnessing Helminth-Driven Immunoregulation in the Search for Novel Therapeutic Modalities. PLoS Pathog. 2020, 16, e1008508. [Google Scholar] [CrossRef] [PubMed]
- Hunter, M.M.; Wang, A.; Hirota, C.L.; McKay, D.M. Neutralizing Anti-IL-10 Antibody Blocks the Protective Effect of Tapeworm Infection in a Murine Model of Chemically Induced Colitis. J. Immunol. 2005, 174, 7368–7375. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, P.; Mangan, N.E.; Walsh, C.M.; Fallon, R.E.; McKenzie, A.N.J.; van Rooijen, N.; Fallon, P.G. Infection with a Helminth Parasite Prevents Experimental Colitis via a Macrophage-Mediated Mechanism. J. Immunol. 2007, 178, 4557–4566. [Google Scholar] [CrossRef] [PubMed]
- Mishra, P.K.; Patel, N.; Wu, W.; Bleich, D.; Gause, W.C. Prevention of Type 1 Diabetes through Infection with an Intestinal Nematode Parasite Requires IL-10 in the Absence of a Th2-Type Response. Mucosal Immunol. 2013, 6, 297–308. [Google Scholar] [CrossRef]
- McSorley, H.J.; Blair, N.F.; Robertson, E.; Maizels, R.M. Suppression of OVA-Alum Induced Allergy by Heligmosomoides Polygyrus Products Is MyD88-, TRIF-, Regulatory T- and B Cell-Independent, but Is Associated with Reduced Innate Lymphoid Cell Activation. Exp. Parasitol. 2015, 158, 8–17. [Google Scholar] [CrossRef]
- Li, S.; Rajeev, S.; Wang, A.; McKay, D.M. Infection with Hymenolepis Diminuta Blocks Colitis and Hastens Recovery While Colitis Has Minimal Impact on Expulsion of the Cestode from the Mouse Host. Pathogens 2021, 10, 994. [Google Scholar] [CrossRef]
- Ieşanu, M.-I.; Cliveti, R.; Anghel, M.; Stoicescu, M.-M.; Boboc, C.; Ioan, A.; Galoş, F. Parasite-Induced Th2 Polarization-An Unusual Cause of Paediatric Hepatic Abscess. Medicina 2021, 57, 1322. [Google Scholar] [CrossRef]
- Sethi, S.; Gupta, S.; Jayshree, M.; Mewara, A.; Khurana, S. Hymenolepis Diminuta Infection in a Child from Urban Area of North India: A Rare Case Report. Trop. Parasitol. 2018, 8, 118–120. [Google Scholar] [CrossRef]
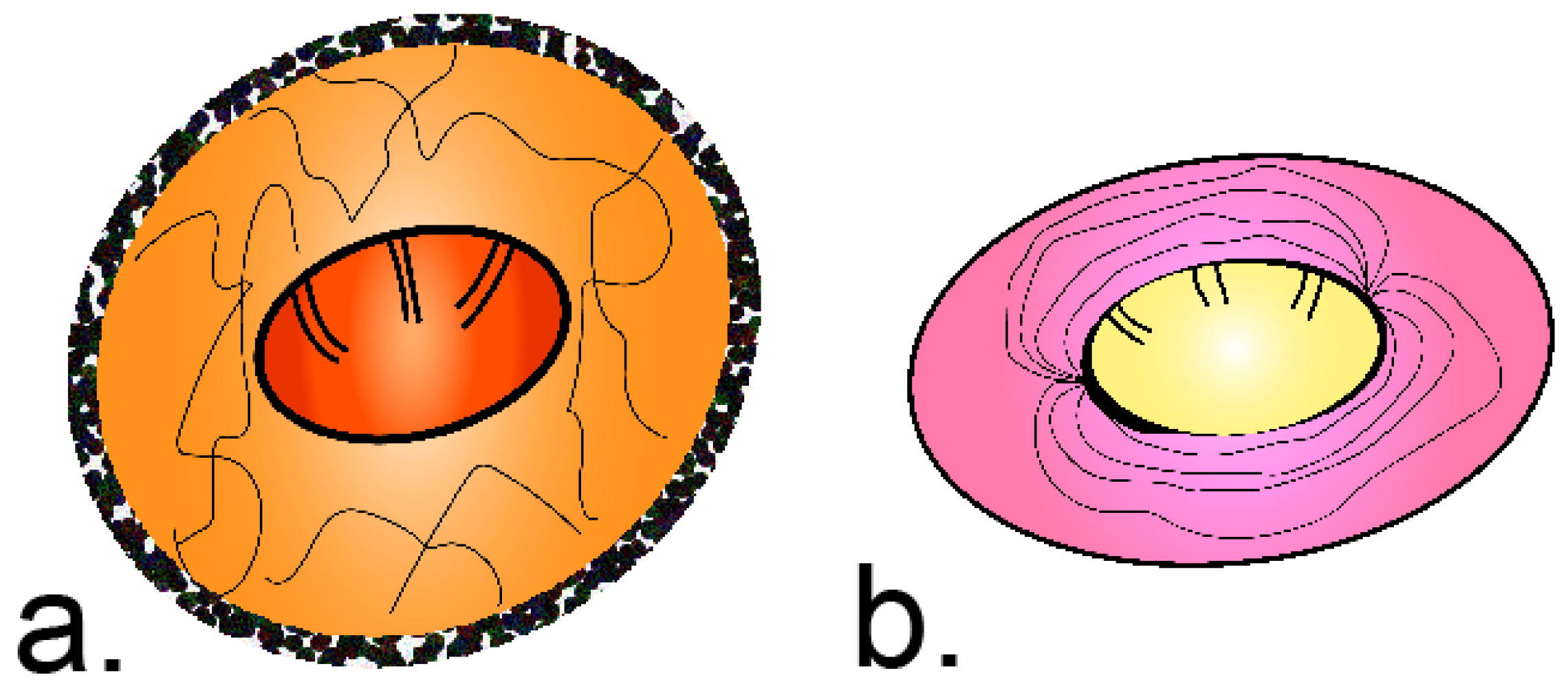
Figure 1.
The morphology difference between H. diminuta and H. nana eggs. (a) Egg of H. diminuta—round or slightly oval, with a size of approx. 70 µm × 80 µm, with a thick striated outer membrane and a thin inner membrane; the oncosphere has 6 central hooks (hexacanth). (b) Egg of H. nana—oval or subspherical, with a smaller size of approx. 40 µm × 30 µm; the inner membrane has two poles, from which 4 to 8 polar filaments spread out between the membranes; the oncosphere also has 6 central hooks (hexacanth).
Figure 1.
The morphology difference between H. diminuta and H. nana eggs. (a) Egg of H. diminuta—round or slightly oval, with a size of approx. 70 µm × 80 µm, with a thick striated outer membrane and a thin inner membrane; the oncosphere has 6 central hooks (hexacanth). (b) Egg of H. nana—oval or subspherical, with a smaller size of approx. 40 µm × 30 µm; the inner membrane has two poles, from which 4 to 8 polar filaments spread out between the membranes; the oncosphere also has 6 central hooks (hexacanth).

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Galoș, F.; Anghel, M.; Ioan, A.; Ieșanu, M.-I.; Boboc, C.; Boboc, A.A. Hymenolepis diminuta Infection in a Romanian Child from an Urban Area. Pathogens 2022, 11, 322. https://doi.org/10.3390/pathogens11030322
AMA Style
Galoș F, Anghel M, Ioan A, Ieșanu M-I, Boboc C, Boboc AA. Hymenolepis diminuta Infection in a Romanian Child from an Urban Area. Pathogens. 2022; 11(3):322. https://doi.org/10.3390/pathogens11030322
Chicago/Turabian StyleGaloș, Felicia, Mălina Anghel, Andreea Ioan, Mara-Ioana Ieșanu, Cătălin Boboc, and Anca Andreea Boboc. 2022. "Hymenolepis diminuta Infection in a Romanian Child from an Urban Area" Pathogens 11, no. 3: 322. https://doi.org/10.3390/pathogens11030322
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.