
High Mortality and Graft Loss after Infective Endocarditis in Kidney Transplant Recipients: A Case-Controlled Study from Two Centers

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Material and Methods
2.1. Study Design, Setting, and Participants
2.2. Clinical Data and Definitions
- Medical history: presence of a heart disease at high risk of IE heart (prosthetic valves, congenital cyanotic heart disease, or history of infective endocarditis), a history intravenous drug use, pre-transplant diabetes or new onset diabetes after transplantation (NODAT).
- Kidney transplantation (KT) history: the most recent estimated glomerular filtration rate (eGFR, MDRD formula) considered as stable before IE onset, induction and maintenance immunosuppressive treatments before and at the time of the infectious episode, the presence of high levels of calcineurin inhibitors or antimetabolites prior to the infectious episode (trough level > 10 ng/mL for tacrolimus or >150 ng/mL for cyclosporine, mycophenolate mofetil area under the curve (MMF AUC) > 60 mg.h/L), the treated episodes of rejection and viral infections (BK virus and cytomegalovirus, CMV) between transplantation and the IE episode.
- The characteristics of the IE with the time to onset after KT, bacteriological documentation, infectious gateway, ultrasonography features, type of valve, vascular (embolization, intracranial hemorrhages, mycotic aneurysms) and immunological (glomerulonephritis) complications, and the presence of an indication for surgery according to the European Society of Cardiology [5],
- IE therapeutic management: antibiotic therapy used, treatment duration and surgical management
- Outcome: patient and renal graft survival one year after the IE were collected. For controls, the delay between the IE diagnosis in the corresponding case and the event (death, loss of graft function, loss to follow-up, or end of the study) was considered for the survival analysis. The end of the study was 31 December 2019.
2.3. Statistical Analysis
3. Ethics
4. Results
4.1. Population and Incidence of IE
4.2. Clinical Presentation and Microbiological Epidemiology of IE
5. Analysis of Risk Factors
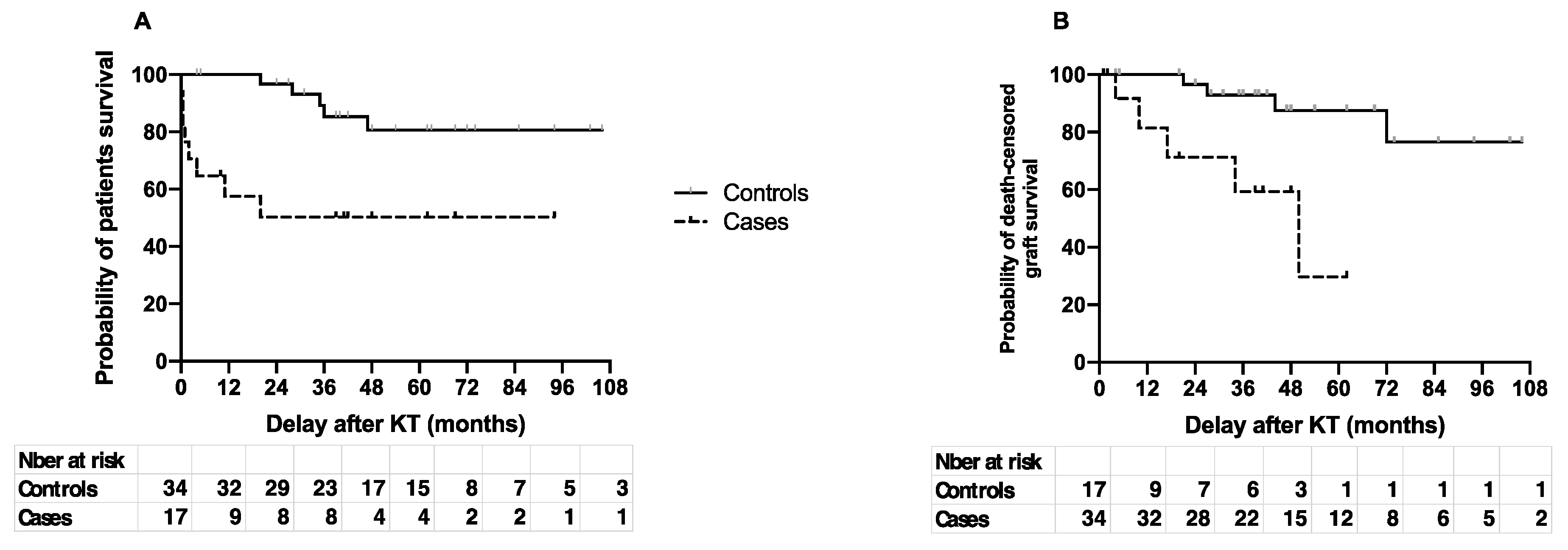
6. Patient and Graft Survival
7. Discussion
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
Ethics Approval
References
- Cahill, T.J.; Prendergast, B.D. Infective endocarditis. Lancet 2016, 387, 882–893. [Google Scholar] [CrossRef] [Green Version]
- Center for Diseases Control and Prevention. Chronic Kidney Disease in the United States, 2019. 2019. Available online: https://www.cdc.gov/kidneydisease/publications-resources/2019-national-facts.html (accessed on 3 November 2020).
- Fishman, J.A. Infection in Organ Transplantation. Am. J. Transplant. 2017, 17, 856–879. [Google Scholar] [CrossRef] [Green Version]
- Li, J.S.; Sexton, D.J.; Mick, N.; Nettles, R.; Fowler, V.G., Jr.; Ryan, T.; Bashore, T.; Corey, G.R. Proposed Modifications to the Duke Criteria for the Diagnosis of Infective Endocarditis. Clin. Infect. Dis. 2000, 30, 633–638. [Google Scholar] [CrossRef]
- Habib, G.; Lancellotti, P.; Antunes, M.J.; Bongiorni, M.G.; Casalta, J.P.; Del Zotti, F.; Dulgheru, R.; El Khoury, G.; Erba, P.A.; Iung, B.; et al. 2015 ESC Guidelines for the management of infective endocarditisThe Task Force for the Management of Infective Endocarditis of the European Society of Cardiology (ESC)Endorsed by: European Association for Cardio-Thoracic Surgery (EACTS), the European Association of Nuclear Medicine (EANM). Eur. Heart J. 2015, 36, 3075–3128. [Google Scholar]
- Selton-Suty, C.; Célard, M.; Le Moing, V.; Doco-Lecompte, T.; Chirouze, C.; Iung, B.; Strady, C.; Revest, M.; Vandenesch, F.; Bouvet, A.; et al. Preeminence of Staphylococcus aureus in infective endocarditis: A 1-year population-based survey. Clin. Infect. Dis. 2012, 54, 1230–1239. [Google Scholar] [CrossRef] [Green Version]
- Sunder, S.; Grammatico-Guillon, L.; Lemaignen, A.; Lacasse, M.; Gaborit, C.; Boutoille, D.; Tattevin, P.; Denes, E.; Guimard, T.; Dupont, M.; et al. Incidence, characteristics, and mortality of infective endocarditis in France in 2011. PLoS ONE 2019, 14, e0223857. [Google Scholar] [CrossRef] [Green Version]
- Iung, B. Endocardite infectieuse. Épidémiologie, physiopathologie et anatomopathologie. Presse Médicale 2019, 48, 513–521. [Google Scholar] [CrossRef]
- Toyoda, N.; Chikwe, J.; Itagaki, S.; Gelijns, A.C.; Adams, D.H.; Egorova, N.N. Trends in Infective Endocarditis in California and New York State, 1998–2013. JAMA 2017, 317, 1652–1660. [Google Scholar] [CrossRef] [PubMed]
- Hoen, B. Infective endocarditis: A frequent disease in dialysis patients. Nephrol. Dial. Transplant. 2004, 19, 1360–1362. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoen, B.; Alla, F.; Selton-Suty, C.; Béguinot, I.; Bouvet, A.; Briançon, S.; Casalta, J.P.; Danchin, N.; Delahaye, F.; Etienne, J.; et al. Changing profile of infective endocarditis: Results of a 1-year survey in France. JAMA 2002, 288, 75–81. [Google Scholar] [CrossRef] [PubMed]
- Sadeghi, M.; Behdad, S.; Shahsanaei, F. Infective Endocarditis and Its Short and Long-Term Prognosis in Hemodialysis Patients: A Systematic Review and Meta-analysis. Curr. Probl. Cardiol. 2020, 46, 100680. [Google Scholar] [CrossRef] [PubMed]
- Nucifora, G.; Badano, L.P.; Viale, P.; Gianfagna, P.; Allocca, G.; Montanaro, D.; Livi, U.; Fioretti, P.M. Infective endocarditis in chronic haemodialysis patients: An increasing clinical challenge. Eur. Heart J. 2007, 28, 2307–2312. [Google Scholar] [CrossRef] [PubMed]
- Nardi Agmon, I.; Goldberg, E.; Cohen, E.; Krause, I. Infective endocarditis in the setting of renal transplantation: Case report and review of the literature. Transpl. Infect. Dis. Off. J. Transplant. Soc. 2017, 19, e12786. [Google Scholar] [CrossRef]
- McHenry, M.C.; Braun, W.E.; Popowniak, K.L.; Banowsky, L.H.; Deodhar, S.D. Septicemia in renal transplant recipients. Urol. Clin. N. Am. 1976, 3, 647–666. [Google Scholar] [CrossRef]
- Paula, F.J.D.; Neves, P.D.M.D.M.; Bridi, R.A.; Song, A.T.W.; David-Neto, E. First Report of Granulicatella sp. Endocarditis in a Kidney Transplant Patient. Braz. J. Nephrol. 2017, 39, 341–344. [Google Scholar] [CrossRef] [PubMed]
- Ruttmann, E.; Bonatti, H.; Legit, C.; Ulmer, H.; Stelzmueller, I.; Antretter, H.; Margreiter, R.; Laufer, G.; Mueller, L.C. Severe endocarditis in transplant recipients—An epidemiologic study. Transpl. Int. 2005, 18, 690–696. [Google Scholar] [CrossRef] [PubMed]
- George, S.; Varghese, J.; Chandrasekhar, S.; Perumalla, R.; Reddy, M.S.; Jayanthi, V.; Rela, M. Gram-negative bacteria causing infective endocarditis: Rare cardiac complication after liver transplantation. World J. Hepatol. 2013, 5, 296–297. [Google Scholar] [CrossRef] [Green Version]
- Pour-Reza-Gholi, F.; Farrokhi, F.; Einollahi, B.; Nemati, E. Successful treatment of infective endocarditis in four kidney transplant recipients. Iran. J. Kidney Dis. 2007, 1, 43–45. [Google Scholar] [PubMed]
- Farahani, M.M.; Rostami, Z.; Einollahi, B.; Khosravi, A.; Nemati, E.; Pezeshki, M.L.; Pourfarziani, V.; Joneidi, N.; Hosseini, M.J.; Ghorbani, G.A. Infective Endocarditis after Renal Transplantation. Nephro Urol. Mon. 2014, 6. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3968955/ (accessed on 2 November 2020).
- Chuang, S.; Shrestha, N.K.; Brizendine, K.D. Matched retrospective study of infective endocarditis among solid organ transplant recipients compared to non-transplant: Seven-year experience in a US Referral Center. Transpl. Infect. Dis. 2020, 22, e13368. [Google Scholar] [CrossRef]
- Fricke, W.F.; Maddox, C.; Song, Y.; Bromberg, J.S. Human Microbiota Characterization in the Course of Renal Transplantation. Am. J. Transplant. 2014, 14, 416–427. [Google Scholar] [CrossRef]
- Lee, J.R.; Muthukumar, T.; Dadhania, D.; Toussaint, N.C.; Ling, L.; Pamer, E.; Suthanthiran, M. Gut Microbial Community Structure and Complications Following Kidney Transplantation: A Pilot Study. Transplantation 2014, 98, 697–705. [Google Scholar]
- Bhat, M.; Pasini, E.; Copeland, J.; Angeli, M.; Husain, S.; Kumar, D.; Renner, E.; Teterina, A.; Allard, J.; Guttman, D.S.; et al. Impact of Immunosuppression on the Metagenomic Composition of the Intestinal Microbiome: A Systems Biology Approach to Post-Transplant Diabetes. Sci. Rep. 2017, 7. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5578994/ (accessed on 2 November 2020). [CrossRef]
- Tourret, J.; Willing, B.P.; Dion, S.; MacPherson, J.; Denamur, E.; Finlay, B.B. Immunosuppressive Treatment Alters Secretion of Ileal Antimicrobial Peptides and Gut Microbiota, and Favors Subsequent Colonization by Uropathogenic Escherichia coli. Transplantation 2017, 101, 74–82. [Google Scholar] [CrossRef] [PubMed]
- Paterson, D.L.; Dominguez, E.A.; Chang, F.-Y.; Snydman, D.R.; Singh, N. Infective Endocarditis in Solid Organ Transplant Recipients. Clin. Infect. Dis. 1998, 26, 689–694. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bishara, J.; Robenshtok, E.; Weinberger, M.; Yeshurun, M.; Sagie, A.; Pitlik, S. Infective endocarditis in renal transplant recipients. Transpl. Infect. Dis. 1999, 1, 138–143. [Google Scholar] [CrossRef]
- Einollahi, B.; Lessan-Pezeshki, M.; Pourfarziani, V.; Nemati, E.; Nafar, M.; Pour-Reza-Gholi, F.; Ghadyani, M.H.; Farahani, M.M. Does CMV infection increase the incidence of infective endocarditis following kidney transplantation? Ann. Transplant. 2009, 14, 32–37. [Google Scholar] [PubMed]
- White, C.A.; Huang, D.; Akbari, A.; Garland, J.; Knoll, G.A. Performance of creatinine-based estimates of GFR in kidney transplant recipients: A systematic review. Am. J. Kidney Dis. Off. J. Natl. Kidney Found 2008, 51, 1005–1015. [Google Scholar] [CrossRef] [PubMed]
- Von Tokarski, F.; Lemaignen, A.; Portais, A.; Fauchier, L.; Hennekinne, F.; Sautenet, B.; Halimi, J.M.; Legras, A.; Patat, F.; Bourguignon, T.; et al. Risk factors and outcomes of early acute kidney injury in infective endocarditis: A retrospective cohort study. Int. J. Infect. Dis. 2020, 99, 421–427. [Google Scholar] [CrossRef]


{kind=link}
| Cases, N = 17 * n (%) or Mean ± SD | Controls, N = 34 * n (%) or Mean ± SD | p Value | |
|---|---|---|---|
| Demographics | |||
| Age (years) | 63.8 ± 13.4 | 55.6 ± 11.7 | 0.03 |
| Sex (male) | 11 (64.7) | 19 (55.9) | 0.54 |
| Comorbidities | |||
| Intravenous drug use | 0 (0) | 0 (0) | 1 |
| Heart prosthetic valve | 3 (17.6) | 2 (5.9) | 0.32 |
| Diabetes | 7 (41) | 7 (20.6) | 0.2 |
| 4 (23.5) | 4 (11.8) | 0.21 |
| 3 (17.6) | 3 (8.8) | 0.35 |
| Initial nephropathy | <0.01 | ||
| Vascular/Hypertension | 5 (29.4) | 2 (5.9) | |
| Diabetes | 3 (17.6) | 5 (14.7) | |
| PKD | 3 (17.6) | 4 (11.8) | |
| IgA nephropathy | 2 (11.8) | 2 (5.9) | |
| Glomerulonephritis | 2 (11.8) | 3 (8.8) | |
| aHUS | 2 (11.8) | 0 | |
| Undetermined | 0 | 7 (20.6) | |
| Other | 0 | 11 (32.4) | |
| Transplant features | |||
| First transplantation | 17 (100) | 30 (88.2) | 0.29 |
| CMV infection | 9 (52.9) | 11 (32.3) | 0.26 |
| BK virus infection | 1 (5.9) | 8 (23.5) | 0.24 |
| Treatment of acute rejection | 2 (11.8) | 3 (8.8) | 1 |
| Induction therapy | |||
| ATG | 13 (76.5) | 24 (70.6) | 1 |
| Basiliximab | 4 (23.5) | 10 (29.4) | 1 |
| Maintenance therapy | |||
| Steroids | 15 (88.2) | 29 (85.3) | 1 |
| MMF | 16 (94.1) | 30 (88.2) | 0.65 |
| CNI | 17 (100) | 34 (100) | 1 |
| Other | 1 (5.9) | 3 (8.8) | 1 |
| Drug monitoring | |||
| AUC MMF > 60 mg·h/L | 1/6 (16) | 0/10 (0) | 0.36 |
| Elevated CNI trough level ** | 5/14 (35.7) | 2/22 (9.1) | 0.08 |
| IE features | |||
| Time for onset after KT (months) | 77.8 ± 82.3 | NA | 1 |
| Last available eGFR before IE (mL/min/1.73 m2) | 43.6 ± 21.9 | 52.3 ± 24.0 | 0.14 |
| Characteristics | N = 17, n (%) Unless Otherwise Specified |
|---|---|
| Definite IE | 12 (70.6) |
| Possible IE | 5 (29.4) |
| Valve | |
| Native | 14 (82.4) |
| Prosthetic | 3 (17.6) |
| Aortic IE | 5 (39.4) |
| Mitral IE | 7 (41.2) |
| Mitral and aortic | 4 (23.5) |
| Echocardiography data | |
| No vegetation | 2 (11.8) |
| Ring abscess and/or severe valve leakage | 6 (35.3) |
| Vascular complications | 6 (36.3) |
| Microbiology | |
| Enterococci | 6 (35.3) |
| Streptococcus gallolyticus | 3 (17.6) |
| Staphylococcus aureus | 3 (17.6) |
| Coagulase-negative Staphylococci | 3 (17.6) |
| Escherichia coli | 1 (5.9) |
| No documentation | 1 (5.9) |
| Probable origin of the causative bacterium | |
| Digestive | 10 (58.8) |
| Cutaneous | 7 (41.2) |
| Unknown | 1 (5.9) |
| Treatment | |
| Antibiotic treatment duration (weeks), mean ± SD | 5.9 ± 0.5 |
| Aminoglycoside use | 12 (70.6) |
| Indication for surgery | 7 (41.2) |
| Surgery | 3 (17.6) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tamzali, Y.; Danthu, C.; Aubry, A.; Brousse, R.; Faucher, J.-F.; El Ouafi, Z.; Rufat, P.; Essig, M.; Barrou, B.; Toure, F.; et al. High Mortality and Graft Loss after Infective Endocarditis in Kidney Transplant Recipients: A Case-Controlled Study from Two Centers. Pathogens 2021, 10, 1023. https://doi.org/10.3390/pathogens10081023
Tamzali Y, Danthu C, Aubry A, Brousse R, Faucher J-F, El Ouafi Z, Rufat P, Essig M, Barrou B, Toure F, et al. High Mortality and Graft Loss after Infective Endocarditis in Kidney Transplant Recipients: A Case-Controlled Study from Two Centers. Pathogens. 2021; 10(8):1023. https://doi.org/10.3390/pathogens10081023
Chicago/Turabian StyleTamzali, Yanis, Clément Danthu, Alexandra Aubry, Romain Brousse, Jean-François Faucher, Zhour El Ouafi, Pierre Rufat, Marie Essig, Benoit Barrou, Fatouma Toure, and et al. 2021. "High Mortality and Graft Loss after Infective Endocarditis in Kidney Transplant Recipients: A Case-Controlled Study from Two Centers" Pathogens 10, no. 8: 1023. https://doi.org/10.3390/pathogens10081023