
Alveolar Echinococcosis of the Parotid Gland—An Ultra Rare Location Reported from Western Europe


Abstract
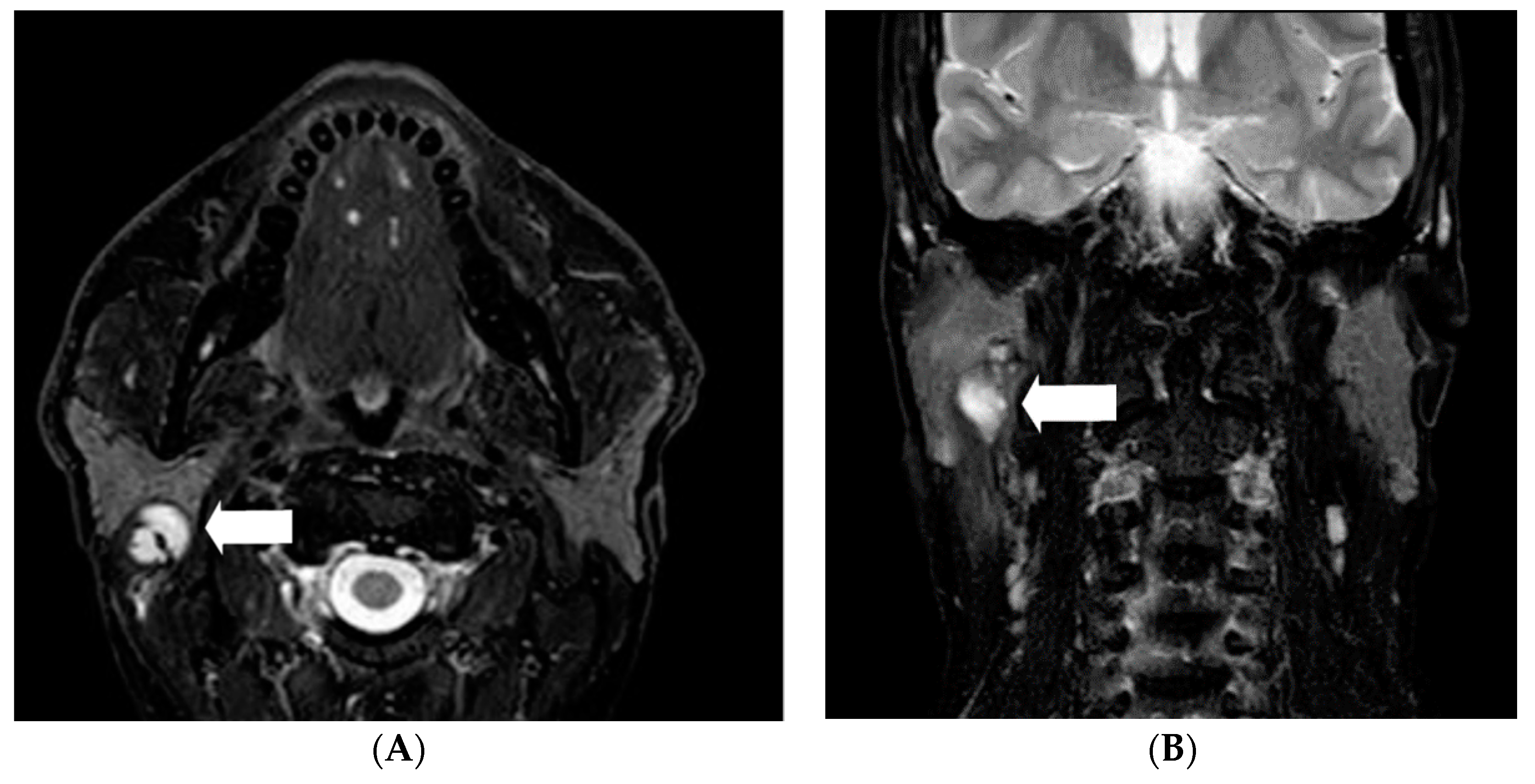
:1. Introduction
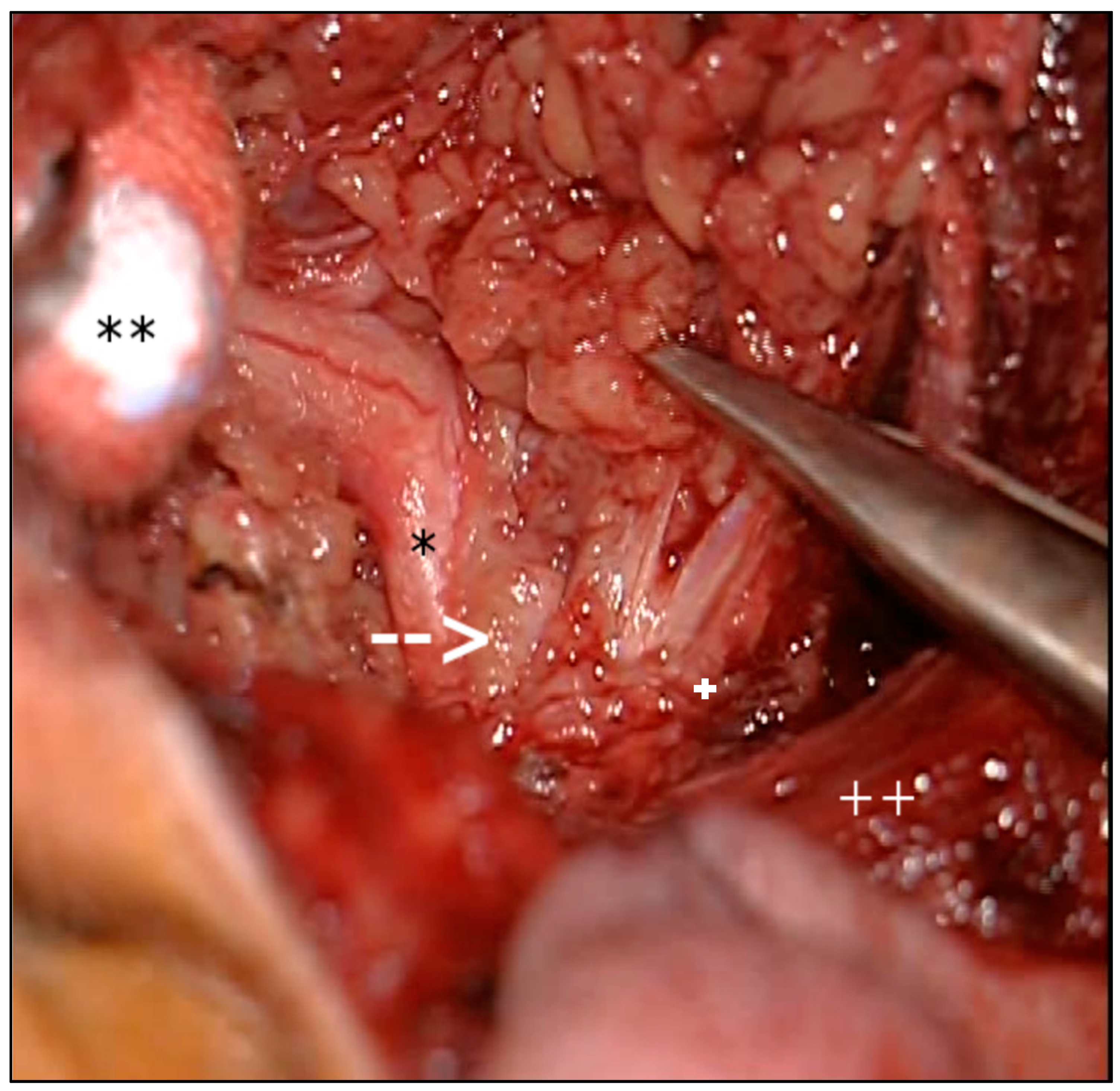
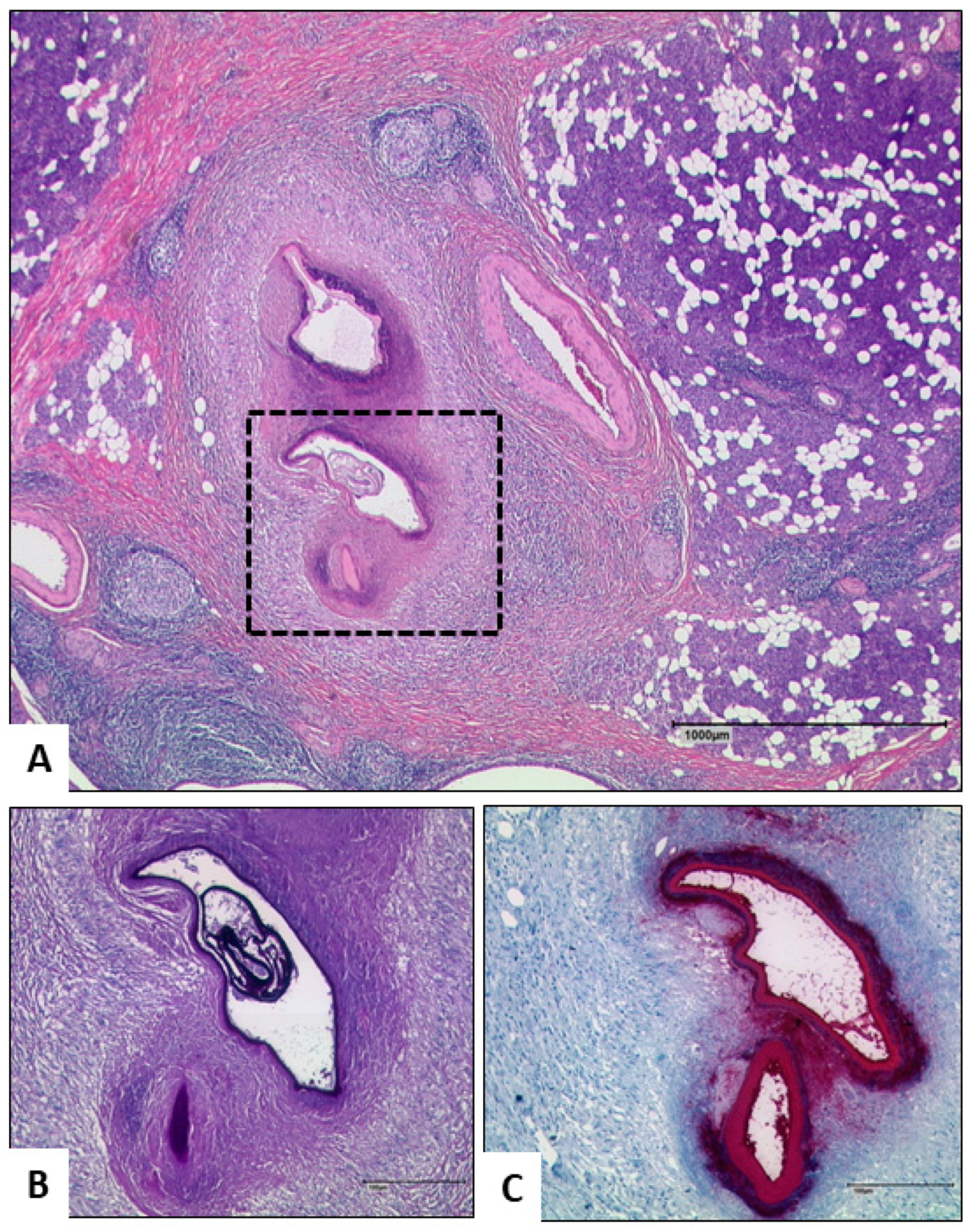
2. Results
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AE | Alveolar echinococcosis |
| CE | Cystic Echinococcosis |
| E. multilocularis | Echinococcus multilocularis |
| ELISA | Enzyme-linked Immunosorbent Assay |
| FFPE | Formalin fixed paraffin-embedded |
| IgG | Immunoglobulin G |
| MRI | Magnetic resonance imaging |
| PAS | Periodic acid-Schiff reaction staining |
| PCR | Polymerase chain reaction |
| Spems | Small particles of E. multilocularis |
References
- Deplazes, P.; Rinaldi, L.; Rojas, C.A.; Torgerson, P.; Harandi, M.; Romig, T.; Antolova, D.; Schurer, J.; Lahmar, S.; Cringoli, G.; et al. Global Distribution of Alveolar and Cystic Echinococcosis. Adv. Parasitol. 2017, 95, 315–493. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higuita, N.I.A.; Brunetti, E.; McCloskey, C. Cystic Echinococcosis. J. Clin. Microbiol. 2016, 54, 518–523. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eckert, J.; Deplazes, P. Biological, Epidemiological, and Clinical Aspects of Echinococcosis, a Zoonosis of Increasing Concern. Clin. Microbiol. Rev. 2004, 17, 107–135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baumann, S.; Shi, R.; Liu, W.; Bao, H.; Schmidberger, J.; Kratzer, W.; Li, W. Worldwide literature on epidemiology of human alveolar echinococcosis: A systematic review of research published in the twenty-first century. Infection 2019, 47, 703–727. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Casulli, A.; Barth, T.F.; Tamarozzi, F. Echinococcus multilocularis. Trends Parasitol. 2019, 35, 738–739. [Google Scholar] [CrossRef] [PubMed]
- Barth, T.; Herrmann, T.S.; Tappe, D.; Stark, L.; Grüner, B.; Buttenschoen, K.; Hillenbrand, A.; Juchems, M.; Henne-Bruns, R.; Kern, P.; et al. Sensitive and Specific Immunohistochemical Diagnosis of Human Alveolar Echinococcosis with the Monoclonal Antibody Em2G11. PLoS Negl. Trop. Dis. 2012, 6, e1877. [Google Scholar] [CrossRef] [PubMed]
- Grimm, J.; Krickl, J.; Beck, A.; Nell, J.; Bergmann, M.; Tappe, D.; Grüner, B.; Barth, T.F.; Brehm, K. Establishing and evaluation of a polymerase chain reaction for the detection of Echinococcus multilocularis in human tissue. PLoS Negl. Trop. Dis. 2021, 15, e0009155. [Google Scholar] [CrossRef] [PubMed]
- Kowalczyk, M.; Kurpiewski, W.; Zieliński, E.; Zadrożny, D.; Klepacki, Ł.; Juśkiewicz, W.; Lasocki, J.; Dyśko, Ł.; Batia, K.; Pesta, W. A rare case of the simultaneous location of Echinococcus multilocularis in the liver and the head of the pancreas: Case report analysis and review of literature. BMC Infect. Dis. 2019, 19, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Darabi, M.; Varedi, P.; Mohebi, A.R.; Mahmoodi, S.; Varedi, P.; Nabavizadeh, S.A.; Erfan, A.; Makhmalbaf, A.O.; Saedi, D.; Mostafavi, S.R.S.; et al. Hydatid cyst of the parotid gland. Oral Maxillofac. Surg. 2008, 13, 33–35. [Google Scholar] [CrossRef] [PubMed]
- Kara, T.; Arpaci, R.B.; Vayisoglu, Y.; Serinsöz, E.; Gürsoy, D.; Ozgur, A.; Apaydın, D.; Ozcan, C. Hydatid cyst of parotid gland: An unusual case diagnosed by fine needle aspiration biopsy. Turk. J. Pathol. 2017, 33, 171–174. [Google Scholar] [CrossRef] [PubMed]
- El Bousaadani, A.; Abada, R.; Rouadi, S.; Roubal, M.; Mahtar, M.; Kadiri, F. Localisations cervico-faciales du kyste hydatique: Série de 17 cas. Rev. Stomatol. Chir. Maxillo-Faciale Chir. Orale 2016, 117, 127–130. [Google Scholar] [CrossRef] [PubMed]
- Just, B.; Kern, P.; Luthardt, R.; Rudolph, H.; Grüner, B.; Wahlers, K. Echinococcus cysts affecting oromaxillofacial structures—A systematic review. Oral Dis. 2014, 20, 756–761. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Author | Cases | E. multilocularis (EM) E. granulosus (EG) | Additional Organs Involved | Region | Age in Years |
|---|---|---|---|---|---|
| Erdur O et al., 2018 | 1 | EG | No | Turkey | 26 |
| Kara T et al., 2017 | 1 | EG | No | Turkey | 54 |
| Arora V K et al., 2016 | 1 | EG | No | India | 13 |
| Diwan R et al., 2015 | 1 | EG | No | India | 35 |
| Du Plessis J et al., 2012 | 1 | EG | No | South Africa | 20 |
| Zouita B et al., 2011 | 1 | EG | No | Morocco | 10 |
| Darabi M et al., 2008 | 1 | EG | No | Iran | 23 |
| Safiolias M et al., 2007 | 1 | EG | No | Greece | 40 |
| Karahatay S et al., 2006 | 1 | EG | No | Turkey | - |
| Oudidi A et al., 2006 | 6 | assumed EG | No | Morocco | - |
| Divisi D et al., 2006 | 1 | EG | Lung | Italy | 81 |
| Akhan O et al., 2002 | 1 | assumed EG | - | Turkey | - |
| Develoux M et al., 1985 | 1 | assumed EG | No | Niger | - |
| Kalovidouris A et al., 1985 | 1 | assumed EG | Fossa infratemporalis | Greece | - |
| Saxena S K et al., 1983 | 1 | EG | No | Lebanon | 45 |
| REVIEWS/SERIES | |||||
| El Bousaadani A et al., 2016 | 6 | assumed EG | - | Morocco | Av. 35 |
| Just B A et al., 2014 | 32 | assumed EG | - | - | Av. 22 |
| Belcadhi M et al., 2011 | 2 | - | - | - | Av. 27 |
| Bellil S et al., 2009 | 1 | - | - | Tunisia | Av. 38.7 |
| Cooney R et al., 2004 | 3 | assumed EG | - | Kenya | Av. 27 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Koppen, T.; Barth, T.F.E.; Eichhorn, K.W.; Gabrielpillai, J.; Kader, R.; Bootz, F.; Send, T. Alveolar Echinococcosis of the Parotid Gland—An Ultra Rare Location Reported from Western Europe. Pathogens 2021, 10, 426. https://doi.org/10.3390/pathogens10040426
Koppen T, Barth TFE, Eichhorn KW, Gabrielpillai J, Kader R, Bootz F, Send T. Alveolar Echinococcosis of the Parotid Gland—An Ultra Rare Location Reported from Western Europe. Pathogens. 2021; 10(4):426. https://doi.org/10.3390/pathogens10040426
Chicago/Turabian StyleKoppen, Tim, Thomas F. E. Barth, Klaus W. Eichhorn, Jennis Gabrielpillai, Ralph Kader, Friedrich Bootz, and Thorsten Send. 2021. "Alveolar Echinococcosis of the Parotid Gland—An Ultra Rare Location Reported from Western Europe" Pathogens 10, no. 4: 426. https://doi.org/10.3390/pathogens10040426