
Assessment of a Nano-Docetaxel Combined Treatment for Head and Neck Cancer

 , ,
, ,
Abstract
:1. Introduction
2. Results
2.1. Cell Death Effects of LANT Monotreatment
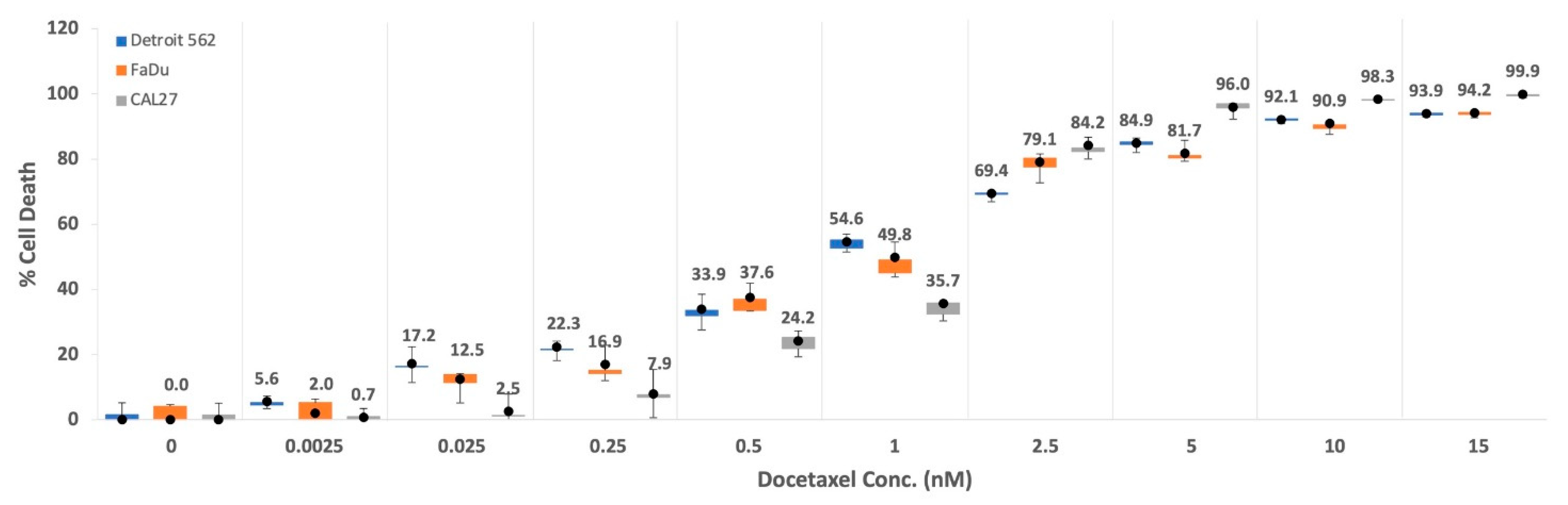
2.2. Cell Death Effects of DTX Monotreatment
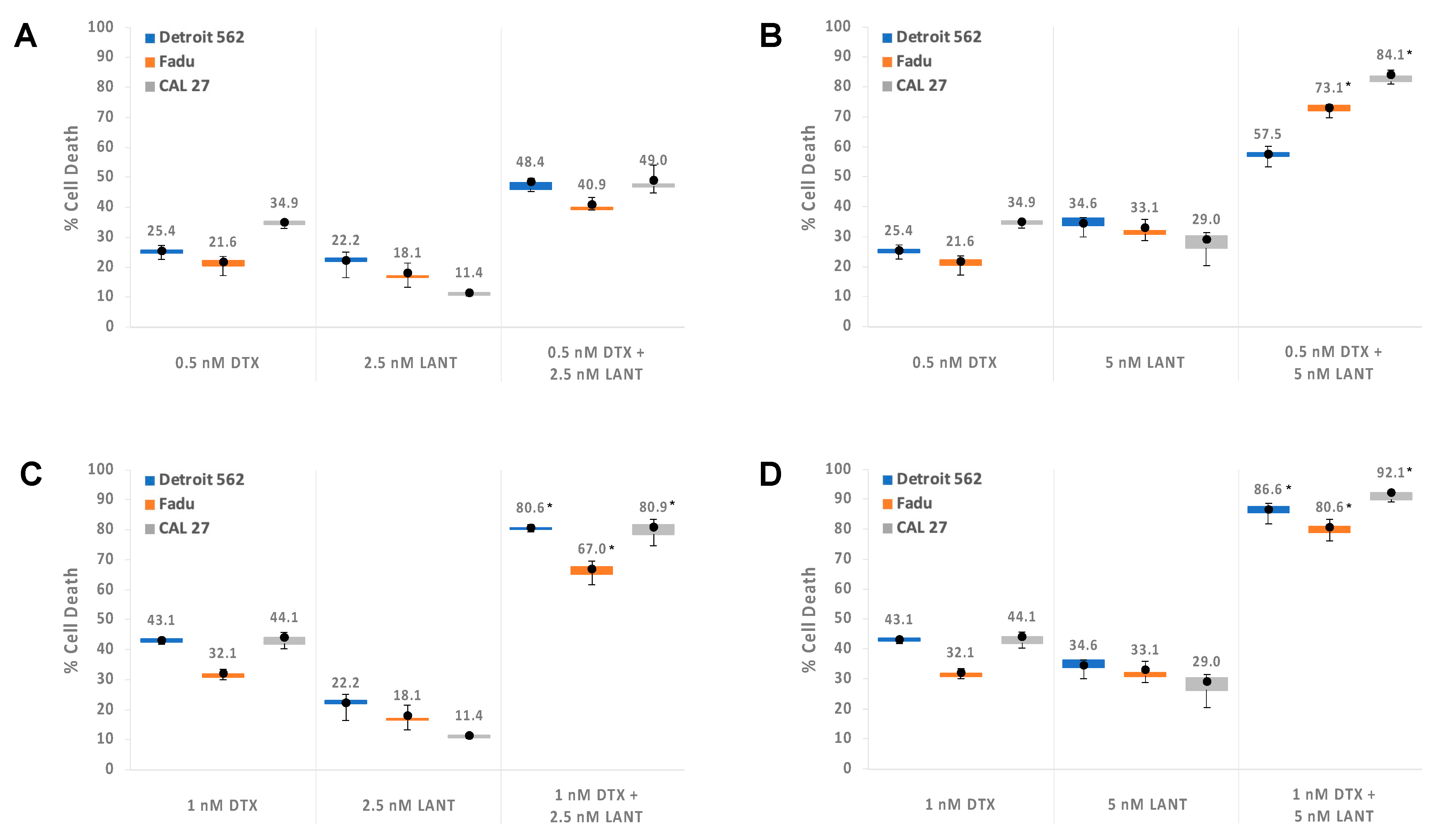
2.3. Combination of DTX and LANT Treatments, Synergy, and Dose Reduction
2.4. Summary Statistics and Linear Mixed Model (LMM) Regression Post Hoc Results
3. Discussion
4. Materials and Methods
4.1. Materials
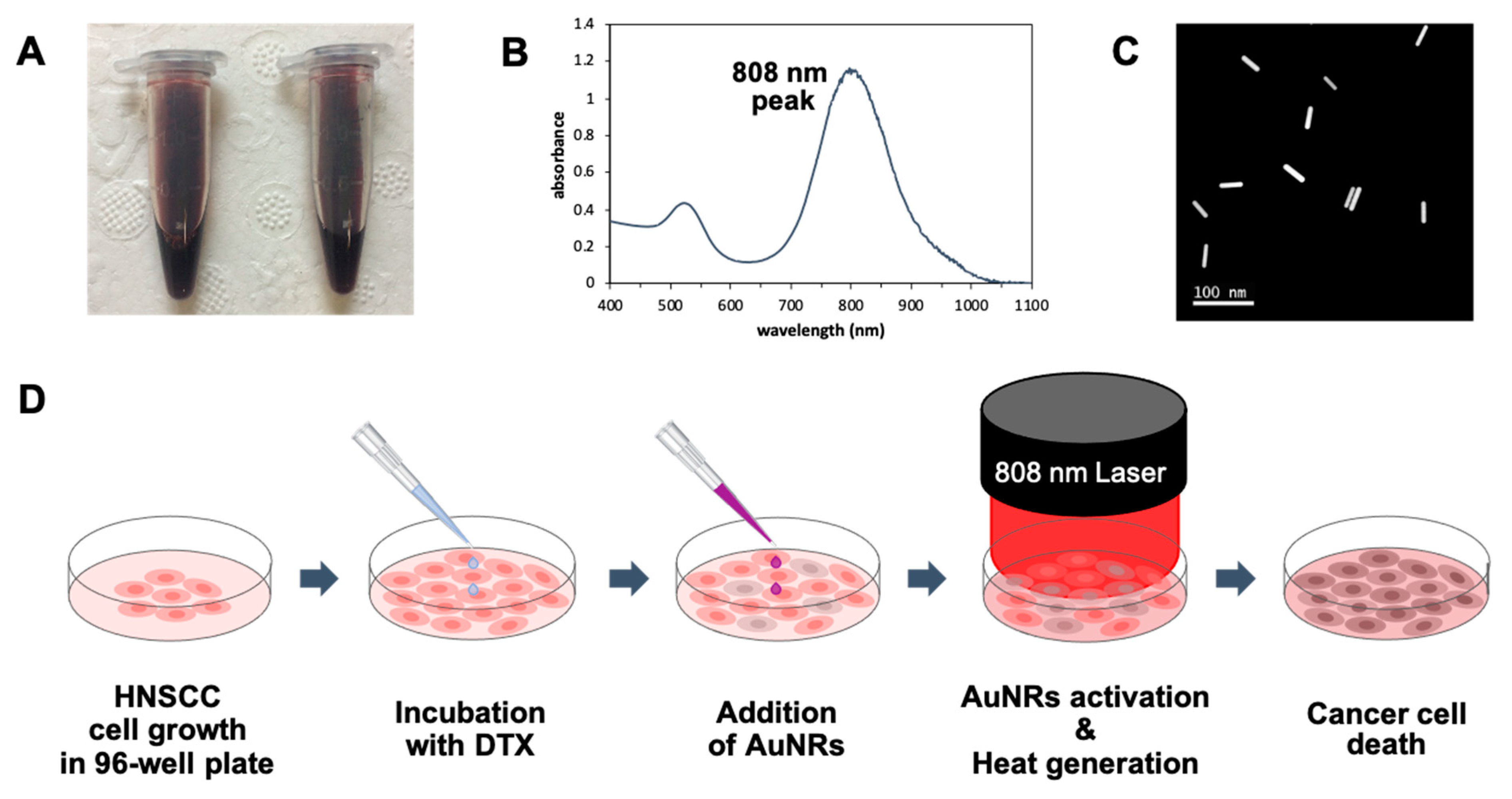
4.2. Preparation of AuNRs
4.3. Cell Lines
4.4. Cell Death by LANT and DTX Monotreatments
4.5. Combination of DTX and LANT In Vitro
4.6. Statistical Power and Analysis
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Siegel, R.; Naishadham, D.; Jemal, A. Cancer statistics, 2013. CA Cancer J. Clin. 2013, 63, 11–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bray, F.; Ferlay, J.; Soerjomataram, I. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [Green Version]
- Blanchard, P.; Baujat, B.; Holostenco, V.; Bourredjem, A.; Baey, C.; Bourhis, J.; Pignon, J.-P. MACH-CH Collaborative group. Meta-analysis of chemotherapy in head and neck cancer (Mach-Nc): A comprehensive analysis by tumour site. Radiother. Oncol. 2011, 100, 33–40. [Google Scholar] [CrossRef]
- Vigneswaran, N.; Williams, M.D. Epidemiologic trends in head and neck cancer and aids in diagnosis. Oral Maxillofac. Surg. Clin. N. Am. 2014, 26, 123–141. [Google Scholar] [CrossRef] [PubMed]
- Marur, S.; Forastiere, A.A. Head and neck squamous cell carcinoma: Update on epidemiology, diagnosis, and treatment. Mayo Clin. Proc. 2016, 91, 386–396. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alsahafi, E.; Begg, K.; Amelio, I.; Raulf, N.; Lucarelli, P.; Sauter, T.; Tavassoli, M. Clinical update on head and neck cancer: Molecular biology and ongoing challenges. Cell Death Dis. 2019, 10, 1–17. [Google Scholar] [CrossRef] [Green Version]
- Docetaxel—National Cancer Institute. Published 10 May 2006. Available online: https://www.cancer.gov/about-cancer/treatment/drugs/docetaxel (accessed on 2 March 2021).
- Lyseng-Williamson, K.A.; Fenton, C. Docetaxel: A review of its use in metastatic breast cancer. Drugs 2005, 65, 2513–2531. [Google Scholar] [CrossRef]
- McKeage, K. Docetaxel: A review of its use for the first-line treatment of advanced castration-resistant prostate cancer. Drugs 2012, 72, 1559–1577. [Google Scholar] [CrossRef] [PubMed]
- Ho, M.Y.; Mackey, J.R. Presentation and management of docetaxel-related adverse effects in patients with breast cancer. Cancer Manag. Res. 2014, 6, 253–259. [Google Scholar] [CrossRef]
- Valero, V. Docetaxel as single-agent therapy in metastatic breast cancer: Clinical efficacy. Semin. Oncol. 1997, 24 (Suppl. S13), S13-11–S13-18. [Google Scholar]
- Catimel, G.; Verweij, J.; Mattijssen, V.; Hanauske, A.; Piccart, M.; Wanders, J.; Franklin, H.; Le Bail, N.; Clavel, M.; Kaye, S.B.; et al. Docetaxel (Taxotere®): An active drug for the treatment of patients with advanced squamous cell carcinoma of the head and neck. Ann. Oncol. 1994, 5, 533–537. [Google Scholar] [CrossRef] [PubMed]
- Colevas, A.D.; Posner, M.R. Docetaxel in head and neck cancer: A review. Am. J. Clin. Oncol. 1998, 21, 482–486. [Google Scholar] [CrossRef]
- Couteau, C.; Chouaki, N.; Leyvraz, S.; Oulid-Aissa, D.; Lebecq, A.; Domenge, C.; Groult, V.; Bordessoule, S.; Janot, F.; De Forni, M.; et al. A phase II study of docetaxel in patients with metastatic squamous cell carcinoma of the head and neck. Br. J. Cancer 1999, 81, 457–462. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernandes, K.A.; Felix, P.A. Persistent docetaxel-induced supravenous erythematous eruption. An. Bras. Dermatol. 2015, 90, 728–730. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cortes, J.E.; Pazdur, R. Docetaxel. J. Clin. Oncol. 1995, 13, 2643–2655. [Google Scholar] [CrossRef]
- Trudeau, M.E. Docetaxel: A review of its pharmacology and clinical activity. Can. J. Oncol. 1996, 6, 443–457. [Google Scholar]
- Bernier, J.; Vrieling, C. Docetaxel in the management of patients with head and neck squamous cell carcinoma. Expert Rev. Anticancer Ther. 2008, 8, 1023–1032. [Google Scholar] [CrossRef]
- Haddad, R.; Posner, M.; Hitt, R.; Cohen, E.; Schulten, J.; Lefebvre, J.-L.; Vermorken, J. Induction chemotherapy in locally advanced squamous cell carcinoma of the head and neck: Role, controversy, and future directions. Ann. Oncol. 2018, 29, 1130–1140. [Google Scholar] [CrossRef]
- DailyMed—DOCETAXEL Injection, Solution. Available online: https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=3104aab1-cd6e-4ad2-8e0a-286a0c5d1940#S5.1 (accessed on 2 March 2021).
- Albers, A.E.; Grabow, R.; Qian, X.; Jumah, M.D.; Hofmann, V.M.; Krannich, A.; Pecher, G. Efficacy and toxicity of docetaxel combination chemotherapy for advanced squamous cell cancer of the head and neck. Mol. Clin. Oncol. 2017, 7, 151–157. [Google Scholar] [CrossRef] [Green Version]
- Galletti, E.; Magnani, M.; Renzulli, M.L.; Botta, M. Paclitaxel And Docetaxel Resistance: Molecular Mechanisms and Development of New Generation Taxanes. ChemMedChem 2007, 2, 920–942. [Google Scholar] [CrossRef] [PubMed]
- Bannister, A.H.; Bromma, K.; Sung, W.; Monica, M.; Cicon, L.; Howard, P.; Chow, R.L.; Schuemann, J.; Chithrani, D.B. Modulation of nanoparticle uptake, intracellular distribution, and retention with docetaxel to enhance radiotherapy. Br. J. Radiol. 2020, 93, 20190742. [Google Scholar] [CrossRef] [PubMed]
- Tran, P.; Duan, W.; Lee, B.-J.; Tran, T.T. Nanogels for Skin Cancer Therapy via Transdermal Delivery: Current Designs. Curr. Drug Metab. 2019, 20, 575–582. [Google Scholar] [CrossRef]
- Her, S.; Jaffray, D.A.; Allen, C. Gold nanoparticles for applications in cancer radiotherapy: Mechanisms and recent advancements. Adv. Drug Deliv. Rev. 2017, 109, 84–101. [Google Scholar] [CrossRef]
- Essawy, M.M.; El-Sheikh, S.M.; Raslan, H.S.; Ramadan, H.S.; Kang, B.; Talaat, I.M.; Afifi, M.M. Function of gold nanoparticles in oral cancer beyond drug delivery: Implications in cell apoptosis. Oral Dis. 2021, 27, 251–265. [Google Scholar] [CrossRef]
- Choi, Y.J.; Kim, Y.J.; Lee, J.W.; Lee, Y.; Lee, S.; Lim, Y.-B.; Chung, H.W. Cytotoxicity and genotoxicity induced by photothermal effects of colloidal gold nanorods. J. Nanosci. Nanotechnol. 2013, 13, 4437–4445. [Google Scholar] [CrossRef]
- Zhou, B.; Song, J.; Wang, M.; Wang, X.; Wang, J.; Howard, E.W.; Zhou, F.; Qu, J.; Chen, W.R. BSA-bioinspired gold nanorods loaded with immunoadjuvant for the treatment of melanoma by combined photothermal therapy and immunotherapy. Nanoscale 2018, 10, 21640–21647. [Google Scholar] [CrossRef]
- Hijaz, M.; Das, S.; Mert, I.; Gupta, A.; Al-Wahab, Z.; Tebbe, C.; Dar, S.; Chhina, J.; Giri, S.; Munkarah, A.; et al. Folic acid tagged nanoceria as a novel therapeutic agent in ovarian cancer. BMC Cancer 2016, 16, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Li, H.; Qu, X.; Qian, W.; Song, Y.; Wang, C.; Liu, W. Andrographolide-loaded solid lipid nanoparticles enhance anti-cancer activity against head and neck cancer and precancerous cells. Oral Dis. 2020. [Google Scholar] [CrossRef] [PubMed]
- Sun, B.; Feng, S.S. Trastuzumab-functionalized nanoparticles of biodegradable copolymers for targeted delivery of docetaxel. Nanomedicine 2009, 4, 431–445. [Google Scholar] [CrossRef]
- Tang, X.; Wang, G.; Shi, R.; Jiang, K.; Meng, L.; Ren, H.; Wu, J.; Hu, Y. Enhanced tolerance and antitumor efficacy by docetaxel-loaded albumin nanoparticles. Drug Deliv. 2015, 23, 2686–2696. [Google Scholar] [CrossRef] [PubMed]
- Bowerman, C.J.; Byrne, J.D.; Chu, K.S.; Schorzman, A.N.; Keeler, A.W.; Sherwood, C.A.; Perry, J.L.; Luft, J.C.; Darr, D.B.; Deal, A.M.; et al. Docetaxel-Loaded PLGA Nanoparticles Improve Efficacy in Taxane-Resistant Triple-Negative Breast Cancer. Nano Lett. 2017, 17, 242–248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choudhury, H.; Gorain, B.; Pandey, M.; Kumbhar, S.A.; Tekade, R.K.; Iyer, A.K.; Kesharwani, P. Recent advances in TPGS-based nanoparticles of docetaxel for improved chemotherapy. Int. J. Pharm. 2017, 529, 506–522. [Google Scholar] [CrossRef] [PubMed]
- Wan, J.; Ma, X.; Xu, D.; Yang, B.; Yang, S.; Han, S. Docetaxel-decorated anticancer drug and gold nanoparticles encapsulated apatite carrier for the treatment of liver cancer. J. Photochem. Photobiol. B Biol. 2018, 185, 73–79. [Google Scholar] [CrossRef]
- Chi, C.; Li, F.; Liu, H.; Feng, S.; Zhang, Y.; Zhou, D.; Zhang, R. Docetaxel-loaded biomimetic nanoparticles for targeted lung cancer therapy in vivo. J. Nanoparticle Res. 2019, 21, 144. [Google Scholar] [CrossRef]
- Ahmad, T.; Sarwar, R.; Iqbal, A.; Bashir, U.; Farooq, U.; Halim, S.A.; Khan, A.; Al-Harrasi, A. Recent advances in combinatorial cancer therapy via multifunctionalized gold nanoparticles. Nanomedicine 2020, 15, 1221–1237. [Google Scholar] [CrossRef]
- Popp, M.K.; Oubou, I.; Shepherd, C.; Nager, Z.; Anderson, C.; Pagliaro, L. Photothermal Therapy Using Gold Nanorods and Near-Infrared Light in a Murine Melanoma Model Increases Survival and Decreases Tumor Volume. J. Nanomater. 2014, 2014, 1–8. [Google Scholar] [CrossRef]
- Green, H.; Crockett, S.; Martyshkin, D.; Singh, K.; Grizzle, W.; Rosenthal, E.; Mirov, S. A histological evaluation and in vivo assessment of intratumoral near infrared photothermal nanotherapy-induced tumor regression. Int. J. Nanomed. 2014, 9, 5093–5102. [Google Scholar] [CrossRef] [Green Version]
- Green, H.N.; Martyshkin, D.V.; Rosenthal, E.L.; Mirov, S.B. A Minimally Invasive Multifunctional Nanoscale System for Selective Targeting, Imaging, and NIR Photothermal Therapy of Malignant Tumors; Achilefu, S., Raghavachari, R., Eds.; SPIE BiOs (Proceeding): San Francisco, CA, USA, 10 February 2011; p. 79100B. [Google Scholar] [CrossRef]
- Lee, G.Y.; Mubasher, M.; Pollack, B.P.; McKenzie, T.; Cothran, M.B.; Green, H.N. Combination paclitaxel and Laser-Activated NanoTherapy for inducing cell death in head and neck squamous cell carcinoma. J. Nanomed. Nanotech. 2021, 12, 557. [Google Scholar]
- Lee, G.Y.; Perez, S.M.; Singh, K.P.; Green, H.N. Cisplatin combined with laser-activated nanotherapy as an adjuvant therapy for head and neck cancer. Int. J. Oncol. 2020, 57, 1169–1178. [Google Scholar] [CrossRef]
- Sebaugh, J.L. Guidelines for accurate EC50/IC50 estimation. Pharm. Stat. 2011, 10, 128–134. [Google Scholar] [CrossRef]
- Long, J.S. Regression Models for Categorical and Limited Dependent Variables; Advanced quantitative techniques in the social sciences; Sage Publications: Thousand Oaks, CA, USA, 1997. [Google Scholar]
- Figgitt, D.P.; Wiseman, L.R. Docetaxel: An update of its use in advanced breast cancer. Drugs 2000, 59, 621–651. [Google Scholar] [CrossRef]
- Yao, M.; Galanopoulos, N.; Lavertu, P.; Fu, P.; Gibson, M.; Argiris, A.; Rezaee, R.; Zender, C.; Wasman, J.; Machtay, M.; et al. Phase II study of bevacizumab in combination with docetaxel and radiation in locally advanced squamous cell carcinoma of the head and neck. Head Neck 2014, 37, 1665–1671. [Google Scholar] [CrossRef] [Green Version]
- Elbehi, A.M.; Anu, R.; Ekine-Afolabi, B.; Cash, E. Emerging role of immune checkpoint inhibitors and predictive biomarkers in head and neck cancers. Oral Oncol. 2020, 109, 104977. [Google Scholar] [CrossRef] [PubMed]
- Adkins, D.; Ley, J.; Atiq, O.; Powell, S.; Spanos, W.C.; Gitau, M.; Rigden, C.; Palka, K.; Liu, J.; Oppelt, P. Nanoparticle albumin-bound paclitaxel with cetuximab and carboplatin as first-line therapy for recurrent or metastatic head and neck cancer: A single-arm, multicenter, phase 2 trial. Oral Oncol. 2021, 115, 105173. [Google Scholar] [CrossRef]
- Marcazzan, S.; Varoni, E.M.; Blanco, E.; Lodi, G.; Ferrari, M. Nanomedicine, an emerging therapeutic strategy for oral cancer therapy. Oral Oncol. 2018, 76, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Link, S.; El-Sayed, M.A. Simulation of the optical absorption spectra of gold nanorods as a function of their aspect ratio and the effect of the medium dielectric constant. J. Phys. Chem. B 2005, 109, 10531–10532. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| EC50 | Cell Lines | ||
|---|---|---|---|
| Detroit 562 | FaDu | CAL 27 | |
| LANT (nM) | 8.08 | 11.03 | 6.68 |
| DTX (nM) | 1.09 | 0.90 | 1.24 |
| Cell Line | Outcome | Treatment Combination | |||
|---|---|---|---|---|---|
| 0.5 nM DTX + 2.5 nM LANT | 0.5 nM DTX + 5 nM LANT | 1 nM DTX + 2.5 nM LANT | 1 nM DTX + 5 nM LANT | ||
| Detroit 562 | Cell death (%) in combo | 48.4 | 57.5 | 81.3 | 86.6 |
| Est. conc. (nM) of DTX mono to obtain the same % cell death | 0.9 | 1.3 | 4.4 | 6.5 | |
| DTX dose reduction (%) | 43.0 | 61.7 | 77.2 | 84.6 a | |
| FaDu | Cell death (%) in combo | 40.9 | 73.1 | 67.0 | 80.6 |
| Est. conc. (nM) of DTX mono to obtain the same % cell death | 0.6 | 2.3 | 1.7 | 3.5 | |
| DTX dose reduction (%) | 22.7 | 78.2 a | 42.2 | 71.5 | |
| CAL 27 | Cell death (%) in combo | 49.0 | 84.1 | 80.9 | 92.1 |
| Est. conc. (nM) of DTX mono to obtain the same % cell death | 1.2 | 2.8 | 2.6 | 4.2 | |
| DTX dose reduction (%) | 57.0 | 82.4 a | 60.8 | 76.0 | |
| Treatment Group Comparison a (First Column vs. Second Column) | Detroit 562 | FaDu | CAL 27 | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Mean Diff. b | Unadj. p-Value c | Adj. p-Value d | Mean Diff. b | Unadj. p-Value c | Adj. p-Value d | Mean Diff. b | Unadj. p-Value c | Adj. p-Value d | ||
| 0.5 nM DTX + 2.5 nM LANT | 0.5 nM DTX | 23.0 | <0.0001 * | <0.0001 * | 19.3 | <0.0001 * | <0.0001 * | 14.2 | <0.0001 * | <0.0001 * |
| 0.5 nM DTX + 5 nM LANT | 0.5 nM DTX | 32.1 | <0.0001 * | <0.0001 * | 51.5 | <0.0001 * | <0.0001 * | 49.2 | <0.0001 * | <0.0001 * |
| 1 nM DTX + 2.5 nM LANT | 0.5 nM DTX | 55.2 | <0.0001 * | <0.0001 * | 45.3 | <0.0001 * | <0.0001 * | 46.1 | <0.0001 * | <0.0001 * |
| 1 nM DTX + 5 nM LANT | 0.5 nM DTX | 61.1 | <0.0001 * | <0.0001 * | 59.0 | <0.0001 * | <0.0001 * | 57.3 | <0.0001 * | <0.0001 * |
| 0.5 nM DTX + 2.5 nM LANT | 1 nM DTX | 5.3 | 0.0219 | 0.3285 | 8.8 | 0.0002 § | 0.0036 § | 4.9 | 0.0306 | 0.4595 |
| 0.5 nM DTX + 5 nM LANT | 1 nM DTX | 14.4 | <0.0001 * | <0.0001 * | 41.0 | <0.0001 * | <0.0001 * | 40.0 | <0.0001 * | <0.0001 * |
| 1 nM DTX + 2.5 nM LANT | 1 nM DTX | 37.5 | <0.0001 * | <0.0001 * | 34.8 | <0.0001 * | <0.0001 * | 36.9 | <0.0001 * | <0.0001 * |
| 1 nM DTX + 5 nM LANT | 1 nM DTX | 43.4 | <0.0001 * | <0.0001 * | 48.5 | <0.0001 * | <0.0001 * | 48.1 | <0.0001 * | <0.0001 * |
| 1 nM DTX | 0.5 nM DTX | 17.7 | <0.0001 * | <0.0001 * | 10.5 | <0.0001 * | 0.0003 | 9.2 | 0.0001 § | 0.0019 § |
| 0.5 nM DTX + 5 nM LANT | 0.5 nM DTX + 2.5 nM LANT | 9.1 | 0.0001 § | 0.0021 § | 32.2 | <0.0001 * | <0.0001 * | 35.0 | <0.0001 * | <0.0001 * |
| 1 nM DTX + 2.5 nM LANT | 0.5 nM DTX + 2.5 nM LANT | 32.2 | <0.0001 * | <0.0001 * | 26.0 | <0.0001 * | <0.0001 * | 31.9 | <0.0001* | <0.0001 * |
| 1 nM DTX + 5 nM LANT | 0.5 nM DTX + 2.5 nM LANT | 38.2 | <0.0001 * | <0.0001 * | 39.7 | <0.0001 * | <0.0001 * | 43.1 | <0.0001 * | <0.0001 * |
| 1 nM DTX + 2.5 nM LANT | 0.5 nM DTX + 5 nM LANT | 23.1 | <0.0001 * | <0.0001 * | −6.2 | 0.0077 | 0.1157 | −3.1 | 0.1658 | 0.999 |
| 1 nM DTX + 5 nM LANT | 0.5 nM DTX + 5 nM LANT | 29.0 | <0.0001 * | <0.0001 * | 7.5 | 0.0014 † | 0.0204 † | 8.1 | 0.0006 † | 0.0097 † |
| 1 nM DTX + 5 nM LANT | 1 nM DTX + 2.5 nM LANT | 5.9 | 0.0101 | 0.1522 | 13.7 | <0.0001 * | <0.0001 * | 11.2 | <0.0001 * | <0.0001 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, G.Y.; Mubasher, M.; McKenzie, T.S.; Schmitt, N.C.; Sebelik, M.E.; Flanagan, C.E.; Osta, B.E.; Cothran, M.B.; Green, H.-N. Assessment of a Nano-Docetaxel Combined Treatment for Head and Neck Cancer. Onco 2021, 1, 83-94. https://doi.org/10.3390/onco1020007
Lee GY, Mubasher M, McKenzie TS, Schmitt NC, Sebelik ME, Flanagan CE, Osta BE, Cothran MB, Green H-N. Assessment of a Nano-Docetaxel Combined Treatment for Head and Neck Cancer. Onco. 2021; 1(2):83-94. https://doi.org/10.3390/onco1020007
Chicago/Turabian StyleLee, Gee Young, Mohamed Mubasher, Tamra S. McKenzie, Nicole C. Schmitt, Merry E. Sebelik, Carrie E. Flanagan, Badi El Osta, Maya B. Cothran, and Hadiyah-Nicole Green. 2021. "Assessment of a Nano-Docetaxel Combined Treatment for Head and Neck Cancer" Onco 1, no. 2: 83-94. https://doi.org/10.3390/onco1020007