The Role of Omega-3 Fatty Acids in Acute Pancreatitis: A Meta-Analysis of Randomized Controlled Trials

Abstract
:1. Introduction
2. Methods
2.1. Literature Search
2.2. Study Selection
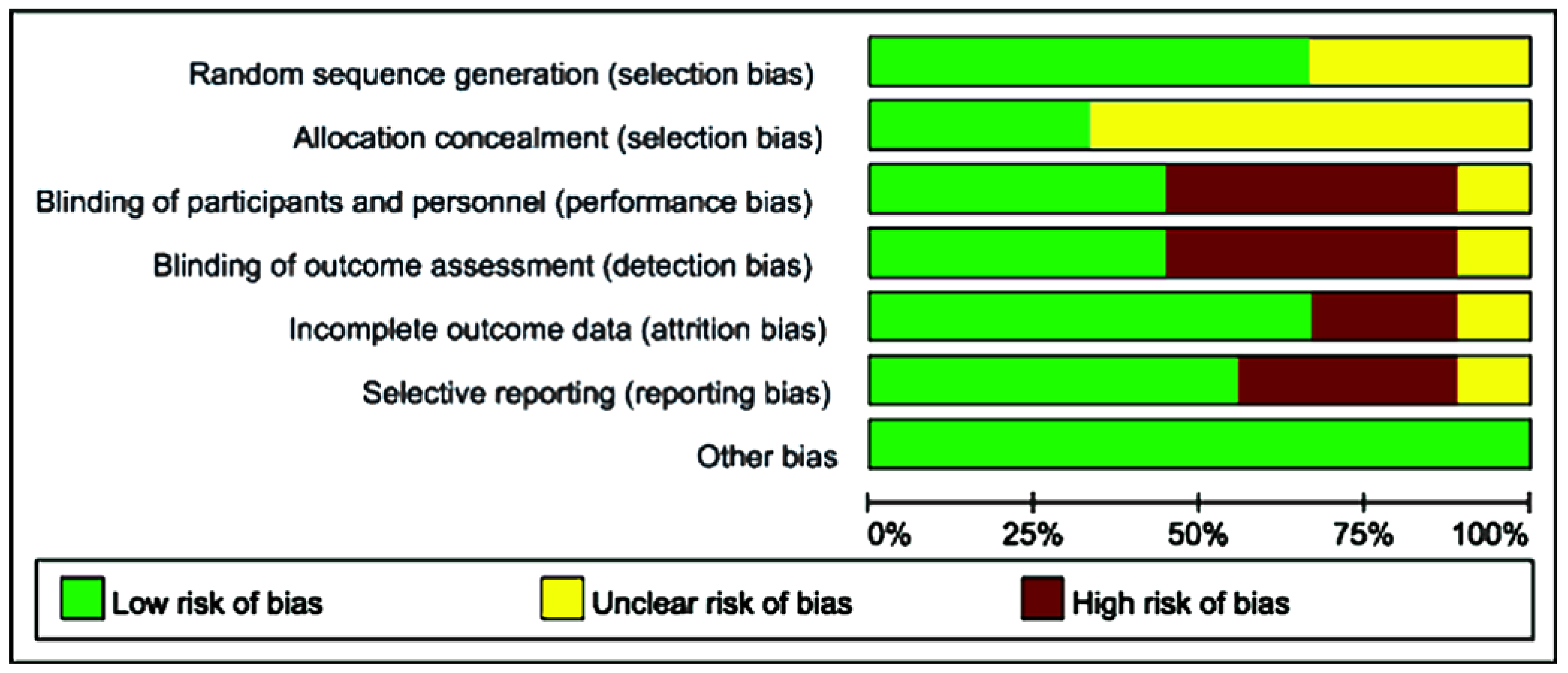
2.3. Quality Assessment
2.4. Statistical Analysis
3. Results
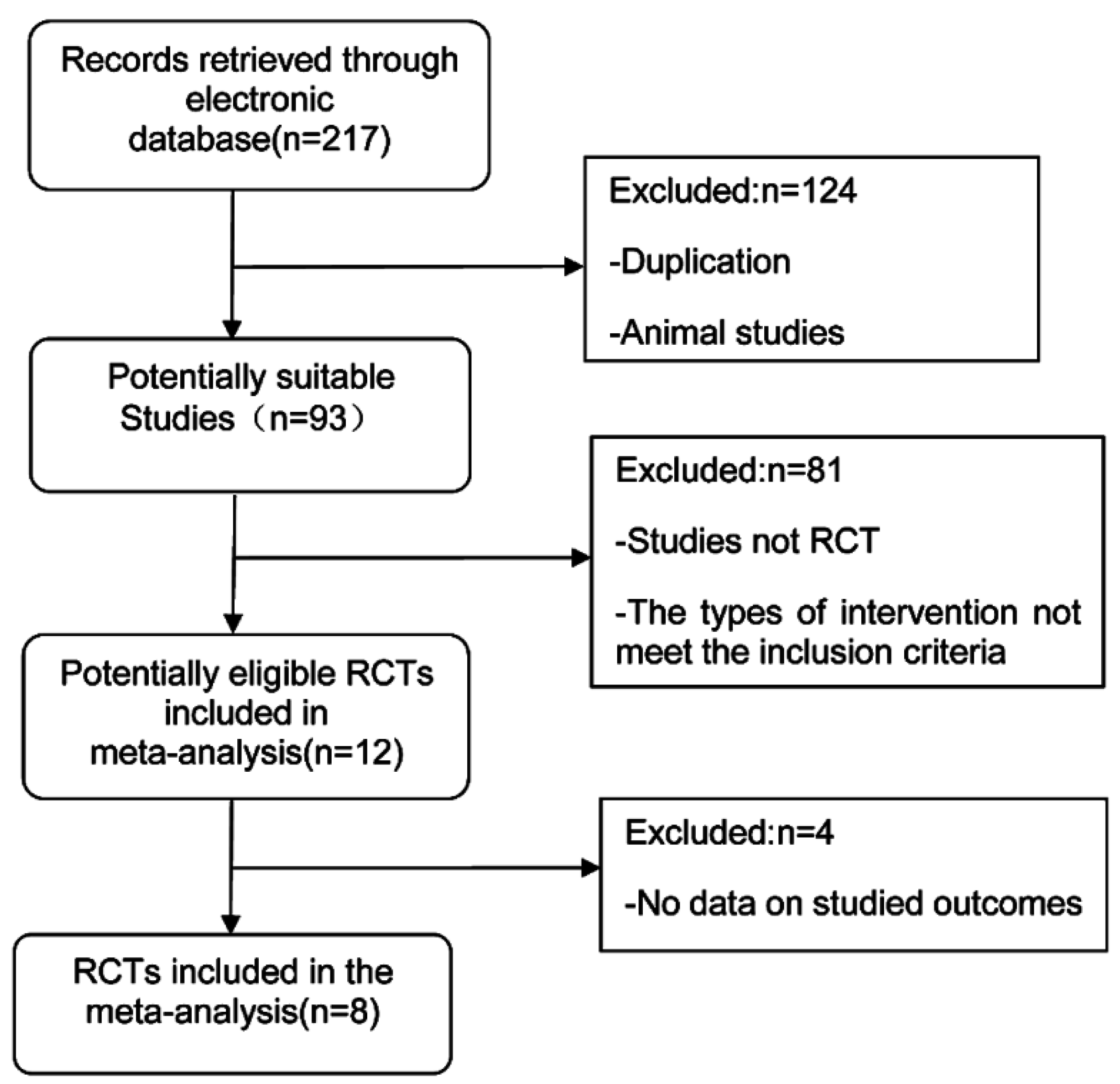
3.1. Search Results and Study Characteristics
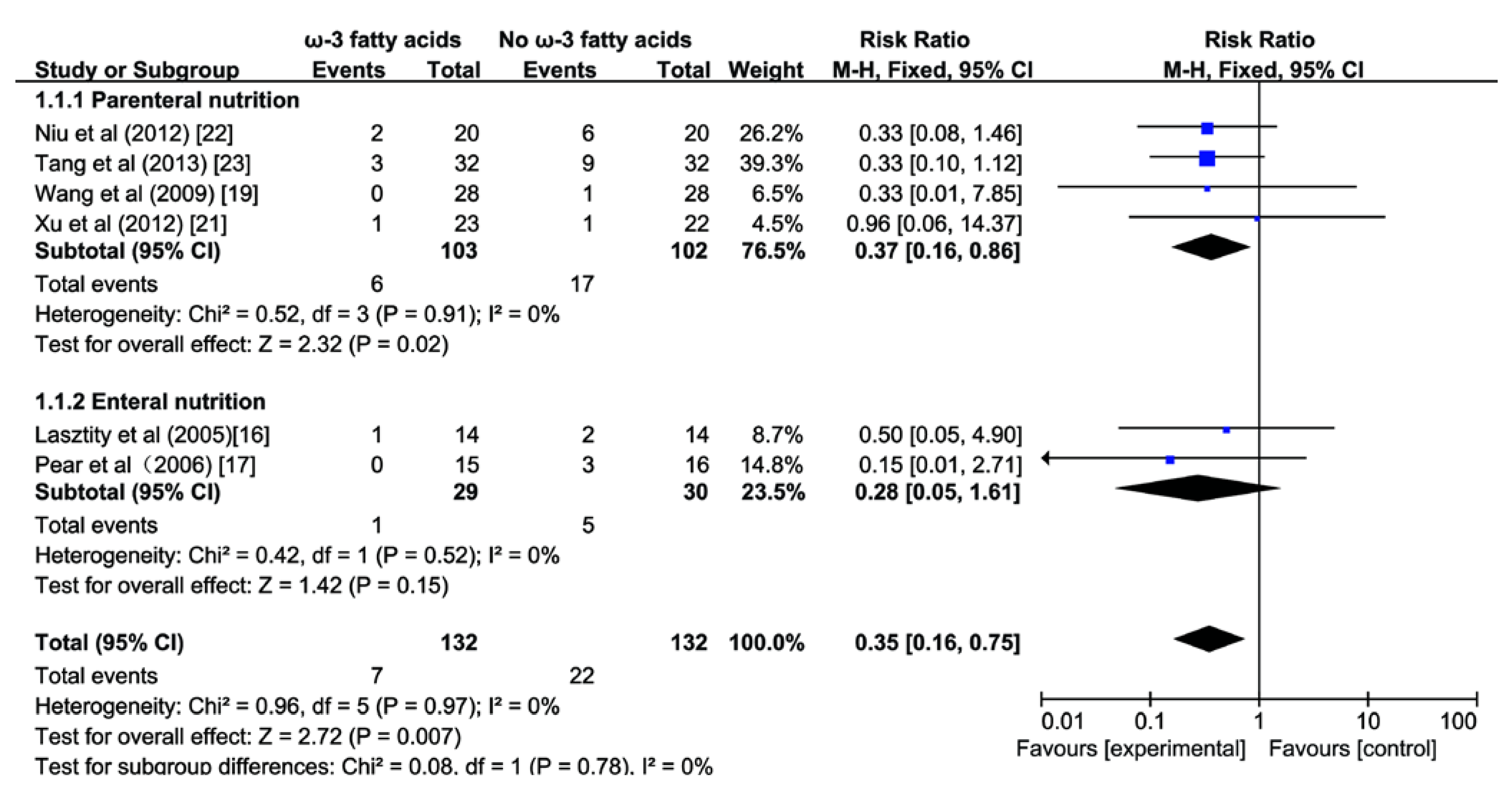
3.2. Effect of ω-3 FA on Mortality


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Country | Year | Type | No. of Patients | Patients (ω-3/con) | Mean age (ω-3/con) | Male/ Female | Severity Criteria of Used | Intervention | Route of Nutrition | Dose | Duration of Intervention |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Lasztity et al. [16] | Hungary | 2005 | RCTFull text | 28 | 14/14 | 56.1/55.9 | 16/12 | APACHE II score ≥ 5 | ω-3 FA alone | EN | 2.84 g day−1a | 5–7 days |
| Pearce et al. [17] | UK | 2006 | RCT DBFull text | 31 | 15/16 | 63.2/73.2 | 18/13 | APACHE II score ≥ 8 | ω-3 FA composite | EN | NR | 3–15 days |
| Wang et al. [18] | China | 2008 | RCTFull text | 40 | 20/20 | 37/40 | 28/12 | Mean APACHE II score = 12.5 | ω-3 FA alone | PN | 0.15–0.2g (kg day)−1b | 5 days |
| Wang et al. [19] | China | 2009 | RCTFull text | 56 | 28/28 | 40/42 | 39/17 | Mean APACHE II score = 14 | ω-3 FA alone | PN | 0.15–0.2g (kg day)−1b | 5 days |
| Xiong et al. [20] | China | 2009 | RCTFull text | 60 | 30/30 | 41.2/42.7 | 36/24 | APACHE-II ≥ 8; Ranson's score ≥ 3; Balthazar CT severity score > 6 | ω-3 FA alone | PN | 0.2 g (kg day)−1b | 2 weeks |
| Xu et al. [21] | China | 2012 | RCTFull text | 45 | 22/23 | 50.5/51.7 | 30/15 | APACHE II score > 8; Ranson score > 3 | ω-3 FA alone | PN | 0.2 g (kg day)−1 b | 2 weeks |
| Niu et al. [22] | China | 2012 | RCTFull text | 40 | 20/20 | Mean 50 | 25/15 | APACHE II score ≥ 8 | ω-3 FA alone | PN | NR | 5 days |
| Tang et al. [23] | China | 2013 | RCTFull text | 64 | 32/32 | Mean 37.5 | 50/24 | APACHE II score ≥ 8; Ranson’s score ≥ 3 | ω-3 FA alone | PN | NR | 5 days |


3.3. Effect of ω-3 FA on Infectious Complications

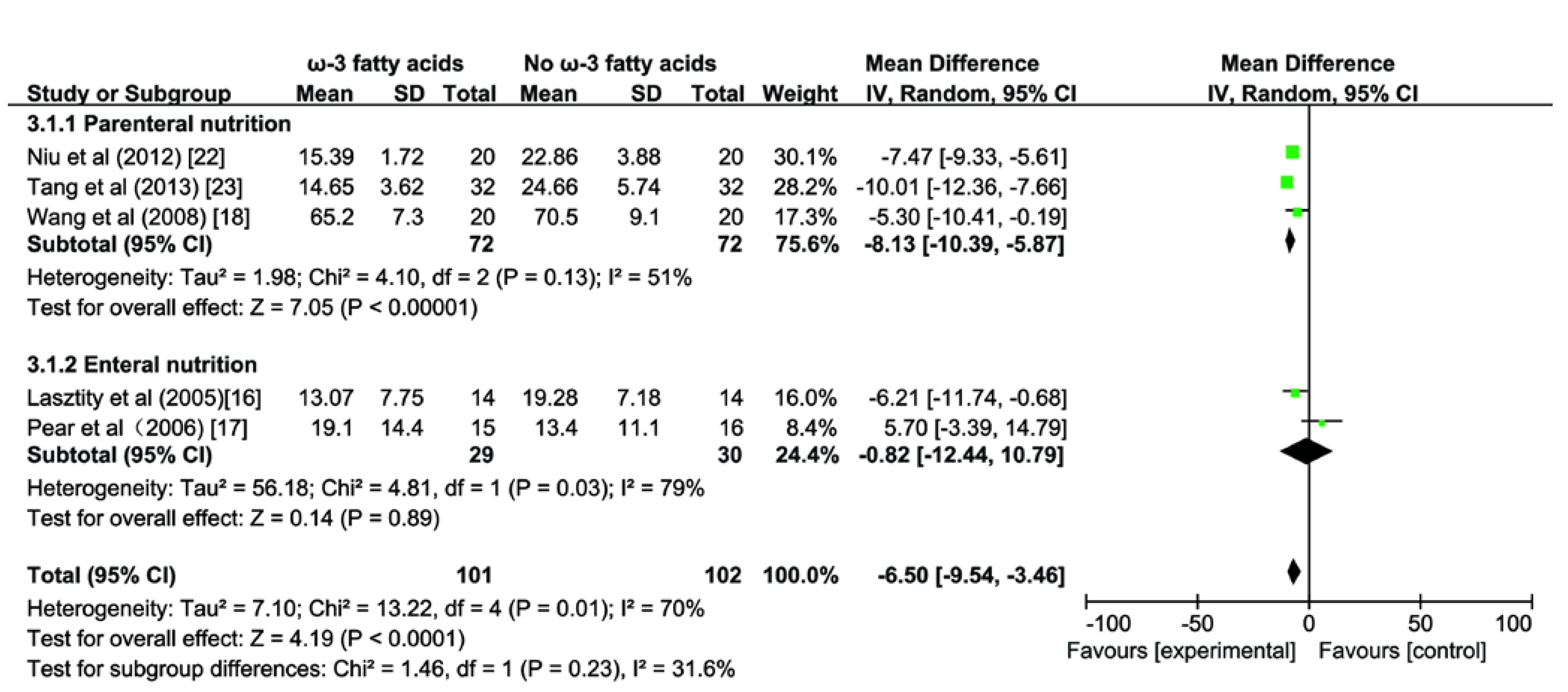
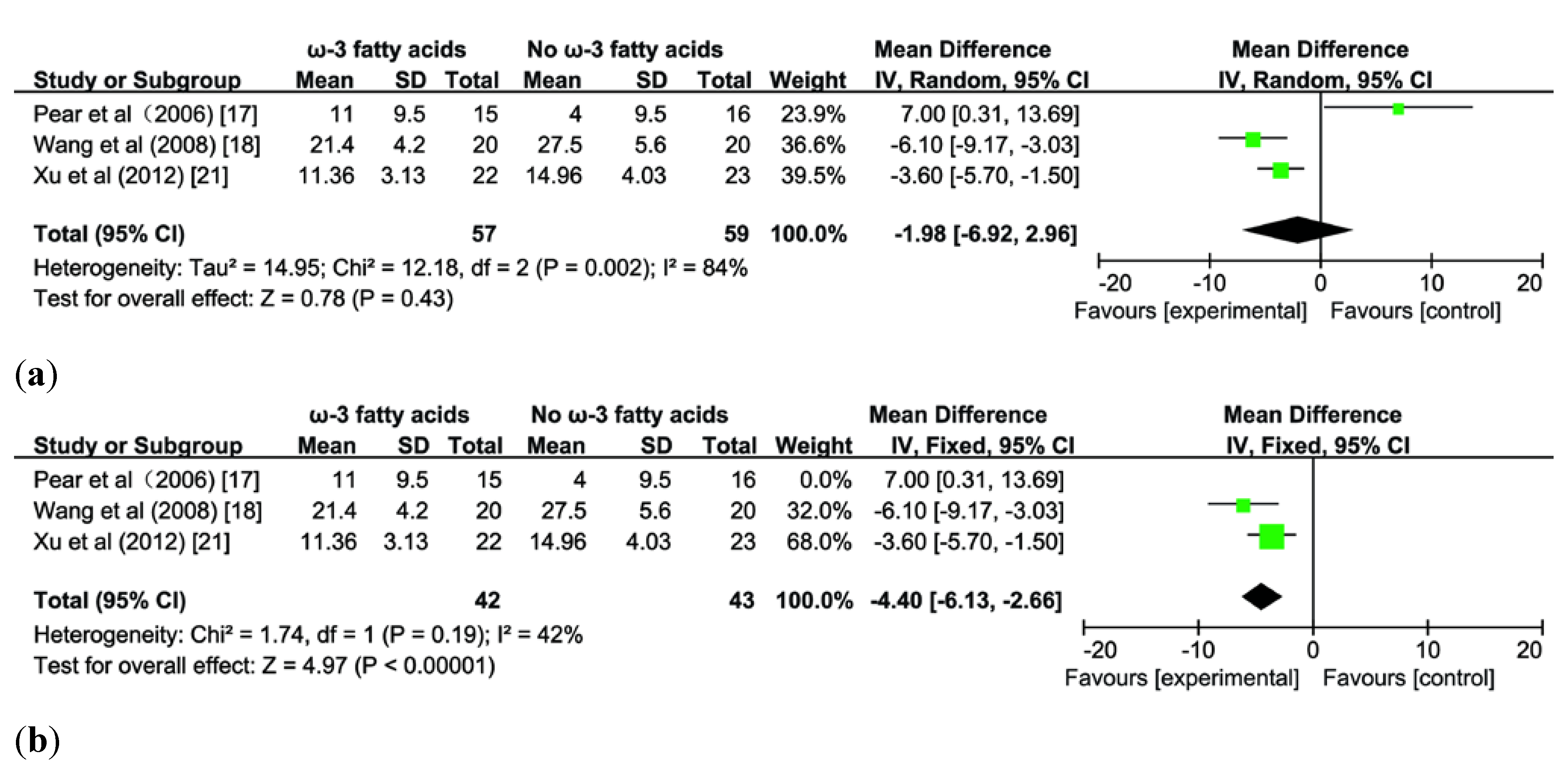
3.4. Effect of ω-3 FA on Length of Hospital Stay
3.5. Effect of ω-3 FA on Length of ICU Stay


4. Discussion
5. Conclusions
Author Contributions
Conflicts of Interest
References
- UK Working Party on Acute Pancreatitis. UK guidelines for the management of acute pancreatitis. Gut 2005, 54, 1–9. [Google Scholar]
- Winslet, M.; Hall, C.; London, N.J.; Neoptolemos, J.P. Relation of diagnostic serum amylase levels to aetiology and severity of acute pancreatitis. Gut 1992, 33, 982–986. [Google Scholar] [CrossRef] [PubMed]
- Meier, R. Enteral fish oil in acute pancreatitis. Clin. Nutr. 2005, 24, 169–171. [Google Scholar] [CrossRef] [PubMed]
- Jha, R.K.; Ma, Q.; Sha, H.; Palikhe, M. Acute pancreatitis: A literature review. Med. Sci. Monit. 2009, 15, 147–156. [Google Scholar]
- Bhatia, M. Acute pancreatitis as a model of SIRS. Front. Biosci. 2008, 14, 2042–2050. [Google Scholar]
- Mishra, G.; Pineau, B.C. Infectious complications of pancreatitis: Diagnosis and management. Curr. Gastroenterol. Rep. 2004, 6, 280–286. [Google Scholar]
- Kingsnorth, A.N.; Galloway, S.W.; Formela, L.J. Randomized, double-blind phase II trial of Lexipafant, a platelet-activating factor antagonist, in human acute pancreatitis. Br. J. Surg. 1995, 82, 1414–1420. [Google Scholar] [CrossRef] [PubMed]
- Mayer, K.; Meyer, S.; Reinholz-Muhly, M.; Maus, U.; Merfels, M.; Lohmeyer, J.; Grimminger, F.; Seeger, W. Short-time infusion of fish oil based lipid emulsions, approved for parenteral nutrition, reduces monocyte proinflammatory cytokine generation and adhesive interaction with endothelium in humans. J. Immunol. 2003, 171, 4837–4843. [Google Scholar] [CrossRef] [PubMed]
- Mori, T.A.; Beilin, L.J. Omega-3 fatty acids and inflammation. Curr. Atheroscler. Rep. 2004, 6, 461–467. [Google Scholar] [CrossRef] [PubMed]
- Weiss, G.; Meyer, F.; Matthies, B.; Pross, M.; Koenig, W.; Lippert, H. Immunomodulation by perioperative administration of n-3 fatty acids. Br. J. Nutr. 2002, 87, 89–94. [Google Scholar] [CrossRef]
- Marik, P.E. What is the best way to feed patients with pancreatitis? Curr. Opin. Crit. Care 2009, 15, 131–138. [Google Scholar] [CrossRef] [PubMed]
- Petrov, M.S.; Pylypchuk, R.D.; Emelyanov, N.V. Systematic review: Nutritional support in acute pancreatitis. Aliment. Pharmacol. Ther. 2008, 28, 704–712. [Google Scholar] [CrossRef] [PubMed]
- Petrov, M.S.; Atduev, V.A.; Zagainov, V.E. Advanced enteral therapy in acute pancreatitis: Is there a room for immunonutrition? A meta-analysis. Int. J. Surg. 2008, 6, 119–124. [Google Scholar] [CrossRef] [PubMed]
- Jafari, T.; Feizi, A.; Askari, G.; Fallah, A.A. Parenteral immunonutrition in patients with acute pancreatitis: A systematic review and meta-analysis. Clin. Nutr. 2014, 34, 35–43. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomized trials. BMJ 2011, 343. [Google Scholar] [CrossRef] [Green Version]
- Lasztity, N.; Hamvas, J.; Biró, L.; Németh, E.; Marosvölgyi, T.; Decsi, T.; Pap, A.; Antal, M. Effect of enterally administered n-3 polyunsaturated fatty acids in acute pancreatitis—A prospective randomized clinical trial. Clin. Nutr. 2005, 24, 198–205. [Google Scholar] [CrossRef] [PubMed]
- Pearce, C.B.; Sadek, S.A.; Walters, A.M.; Goggin, P.M.; Somers, S.S.; Toh, S.K.; Johns, T.; Duncan, H.D. A double-blind, randomized, controlled trial to study the effects of an enteral feed supplemented with glutamine, arginine, and omega-3 fatty acid in predicted acute severe pancreatitis. J. Pancreas. 2006, 7, 361–371. [Google Scholar]
- Wang, X.; Li, W.; Li, N.; Li, J. ω-3 Fatty acids-supplemented parenteral nutrition decreases hyperinflammatory response and attenuates systemic disease sequelae in severe acute pancreatitis: A Randomized and Controlled Study. J. Parenter. Enteral. Nutr. 2008, 32, 236–241. [Google Scholar] [CrossRef]
- Wang, X.; Li, W.; Zhang, F.; Pan, L.; Li, N.; Li, J. Fish oil-supplemented parenteral nutrition in severe acute pancreatitis patients and effects on immune function and infectious risk: A randomized controlled trial. Inflammation 2009, 32, 304–309. [Google Scholar] [CrossRef] [PubMed]
- Xiong, J.; Zhu, S.; Zhou, Y.; Wu, H.; Wang, C. Regulation of ω-3 fish oil emulsion on the SIRS during the initial stage of severe acute pancreatitis. J. Huazhong. Univ. Sci. Technol. Med. Sci. 2009, 29, 35–38. (in Chinese). [Google Scholar] [CrossRef] [PubMed]
- Xu, Q.H.; Cai, G.L.; Lü, X.C.; Hu, C.B.; Chen, J.; Yan, J. The effects of ω-3 fish oil lipid emulsion on inflammation-immune response and organ function in patients with severe acute pancreatitis. Chin. J. Intern. Med. 2012, 51, 962–965. (in Chinese). [Google Scholar]
- Niu, G.H.; Cao, Y.R.; Wang, Y.; Ma, L. The clinical therapeutic effect of omega-3 fish oil emulsion injection on patients with severe acute pancreatitis. Chin. J. Clin. 2012, 6, 1047–1048. (in Chinese). [Google Scholar]
- Tang, B.B.; Hu, D.G. The effects of ω-3 fish oil emulsion injection on patients with sever acute pancreatitis. Chongqing Yixue 2013, 42, 1092–1094. (in Chinese). [Google Scholar]
- Manzanares, W.; Dhaliwal, R.; Jurewitsch, B.; Stapleton, R.D.; Jeejeebhoy, K.N.; Heyland, D.K. Parenteral Fish Oil Lipid Emulsions in the Critically Ill A Systematic Review and Meta-Analysis. J. Parenter. Enter. Nutr. 2014, 38, 20–28. [Google Scholar] [CrossRef]
- Palmer, A.J.; Ho, C.K.; Ajibola, O.; Avenell, A. The role of ω-3 fatty acid supplemented parenteral nutrition in critical illness in adults: A systematic review and meta-analysis. Crit. Care. Med. 2013, 41, 307–316. [Google Scholar] [CrossRef] [PubMed]
- Rice, T.W.; Wheeler, A.P.; Thompson, B.T.; deBoisblanc, B.P.; Steingrub, J.; Rock, P.; NIH NHLBI. Acute Respiratory Distress Syndrome Network of Investigators. Enteral omega-3 fatty acid, γ-linolenic acid, and antioxidant supplementation in acute lung injury. J. Am. Med. Assoc. 2011, 306, 1574–1581. [Google Scholar] [CrossRef]
- Rangel Huerta, O.D.; Aguilera, C.M.; Mesa, M.D.; Gil, A. Omega-3 long-chain polyunsaturated fatty acids supplementation on inflammatory biomakers: A systematic review of randomized clinical trials. Br. J. Nutr. 2012, 107, S159–S170. [Google Scholar] [CrossRef] [PubMed]
- Singer, P.; Shapiro, H.; Theilla, M.; Anbar, R.; Singer, J.; Cohen, J. Anti-inflammatory properties of omega-3 fatty acids in critical illness: Novel mechanisms and an integrative perspective. Intensive Care. Med. 2008, 34, 1580–1592. [Google Scholar] [CrossRef] [PubMed]
- Mayer, K.; Schaefer, M.B.; Seeger, W. Fish oil in the critically ill: from experimental to clinical data. Curr. Opin. Clin. Nutr. Metab. Care 2006, 9, 140–148. [Google Scholar] [CrossRef] [PubMed]
- Cao, S.; Ren, J.; Sun, L.; Gu, G.; Yuan, Y.; Li, J. Fish oil-supplemented parenteral nutrition prolongs survival while beneficially altering phospholipids’ fatty acid composition and modulating immune function in rat sepsis. Shock 2011, 36, 184–190. [Google Scholar] [CrossRef] [PubMed]
- Daly, J.M.; Lieberman, M.D.; Goldfine, J.; Shou, J.; Weintraub, F.; Rosato, E.F.; Lavin, P. Enteral nutrition with supplemental arginine, RNA, and omega-3 fatty acids in patients after operation: Immunologic, metabolic, and clinical outcome. Surgery 1992, 112, 56–67. [Google Scholar] [PubMed]
- Kemen, M.; Senkal, M.; Homann, H.H.; Mumme, A.; Dauphin, A.K.; Baier, J.; Windeler, J.; Neumann, H.; Zumtobel, V. Early postoperative enteral nutrition with arginine-omega-3 fatty acids and ribonucleic acid-supplemented diet versus placebo in cancer patients: An immunologic evaluation of Impact Registered Trademark. Crit. Care Med. 1995, 23, 652–659. [Google Scholar] [CrossRef] [PubMed]
- Bower, R.H.; Cerra, F.B.; Bershadsky, B.; Licari, J.J.; Hoyt, D.B.; Jensen, G.L.; van Buren, C.T.; Rothkopf, M.M.; Daly, J.M.; Adelsberg, B.R. Early enteral administration of a formula (Impact Registered Trademark) supplemented with arginine, nucleotides, and fish oil in intensive care unit patients: Results of a multicenter, prospective, randomized, clinical trial. Crit. Care Med. 1995, 23, 436–449. [Google Scholar] [CrossRef] [PubMed]
- Eckerwall, G.E.; Axelsson, J.B.; Andersson, R.G. Early nasogastric feeding in predicted severe acute pancreatitis: A clinical, randomized study. Ann. Surg. 2006, 244, 959–965. [Google Scholar] [CrossRef] [PubMed]
- Powell, J.J.; Murchison, J.T.; Fearon, K.C.; Ross, J.A.; Siriwardena, A.K. Randomized controlled trial of the effect of early enteral nutrition on markers of the inflammatory response in predicted severe acute pancreatitis. Br. J. Surg. 2000, 87, 1375–1381. [Google Scholar] [CrossRef] [PubMed]
- Heller, A.R.; Rössler, S.; Litz, R.J.; Stehr, S.N.; Heller, S.C.; Koch, R.; Koch, T. Omega-3 fatty acids improve the diagnosis-related clinical outcome. Crit. Care Med. 2006, 34, 972–979. [Google Scholar] [CrossRef] [PubMed]
- Tappy, L.; Berger, M.M.; Schwarz, J.M.; Schneiter, P.; Kim, S.; Revelly, J.P.; Chioléro, R. Metabolic effects of parenteral nutrition enriched with n-3 polyunsaturated fatty acids in critically ill patients. Clin. Nutr. 2006, 25, 588–595. [Google Scholar] [CrossRef] [PubMed]
- Gura, K.M.; Lee, S.; Valim, C.; Zhou, J.; Kim, S.; Modi, B.P.; Arsenault, D.A.; Strijbosch, R.A.; Lopes, S.; Duggan, C.; et al. Safety and efficacy of a fish-oil-based fat emulsion in the treatment of parenteral nutrition-associated liver disease. Pediatrics 2008, 121, e678–e686. [Google Scholar] [CrossRef] [PubMed]
- Martin, J.M.; Stapleton, R.D. Omega-3 fatty acids in critical illness. Nutr. Rev. 2010, 68, 531–541. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lei, Q.C.; Wang, X.Y.; Xia, X.F.; Zheng, H.Z.; Bi, J.C.; Tian, F.; Li, N. The Role of Omega-3 Fatty Acids in Acute Pancreatitis: A Meta-Analysis of Randomized Controlled Trials. Nutrients 2015, 7, 2261-2273. https://doi.org/10.3390/nu7042261
Lei QC, Wang XY, Xia XF, Zheng HZ, Bi JC, Tian F, Li N. The Role of Omega-3 Fatty Acids in Acute Pancreatitis: A Meta-Analysis of Randomized Controlled Trials. Nutrients. 2015; 7(4):2261-2273. https://doi.org/10.3390/nu7042261
Chicago/Turabian StyleLei, Qiu Cheng, Xin Ying Wang, Xian Feng Xia, Hua Zhen Zheng, Jing Cheng Bi, Feng Tian, and Ning Li. 2015. "The Role of Omega-3 Fatty Acids in Acute Pancreatitis: A Meta-Analysis of Randomized Controlled Trials" Nutrients 7, no. 4: 2261-2273. https://doi.org/10.3390/nu7042261