
Combined Plasma DHA-Containing Phosphatidylcholine PCaa C38:6 and Tetradecanoyl-Carnitine as an Early Biomarker for Assessing the Mortality Risk among Sarcopenic Patients
 , , , , , ,
, , , , , ,  ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population and Study Design
2.2. Assessment of Sarcopenia and Muscle Mass and Physical Functions
2.3. Targeted Metabolomic Analysis of Plasma
2.4. Chemometric and Statistical Analyses
3. Results
3.1. Demographics
3.2. Metabolomic Analysis of the Plasma of Sarcopenic Patients
3.3. Plasma Metabolites Associated with the Mortality of Sarcopenic Patients
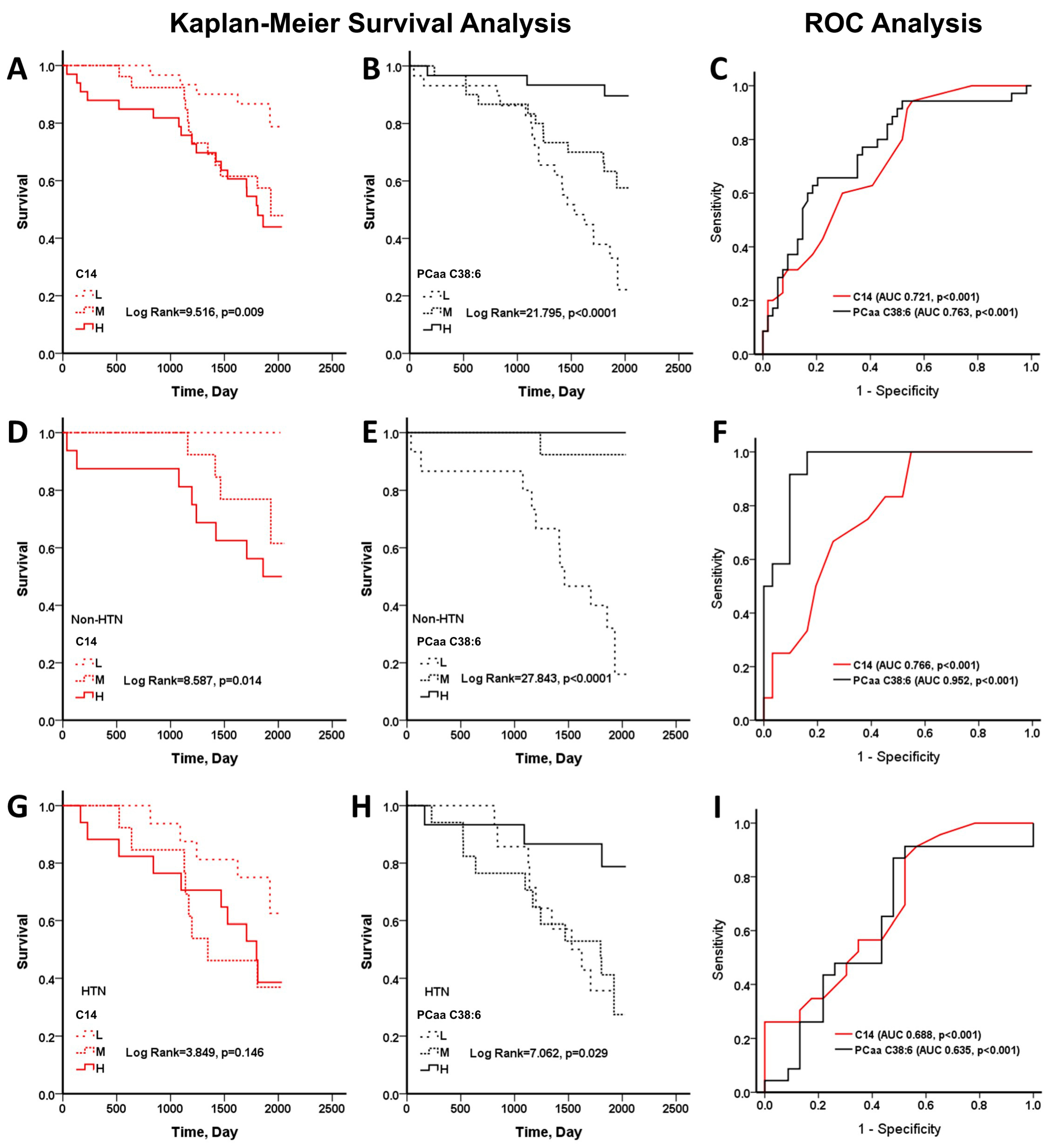
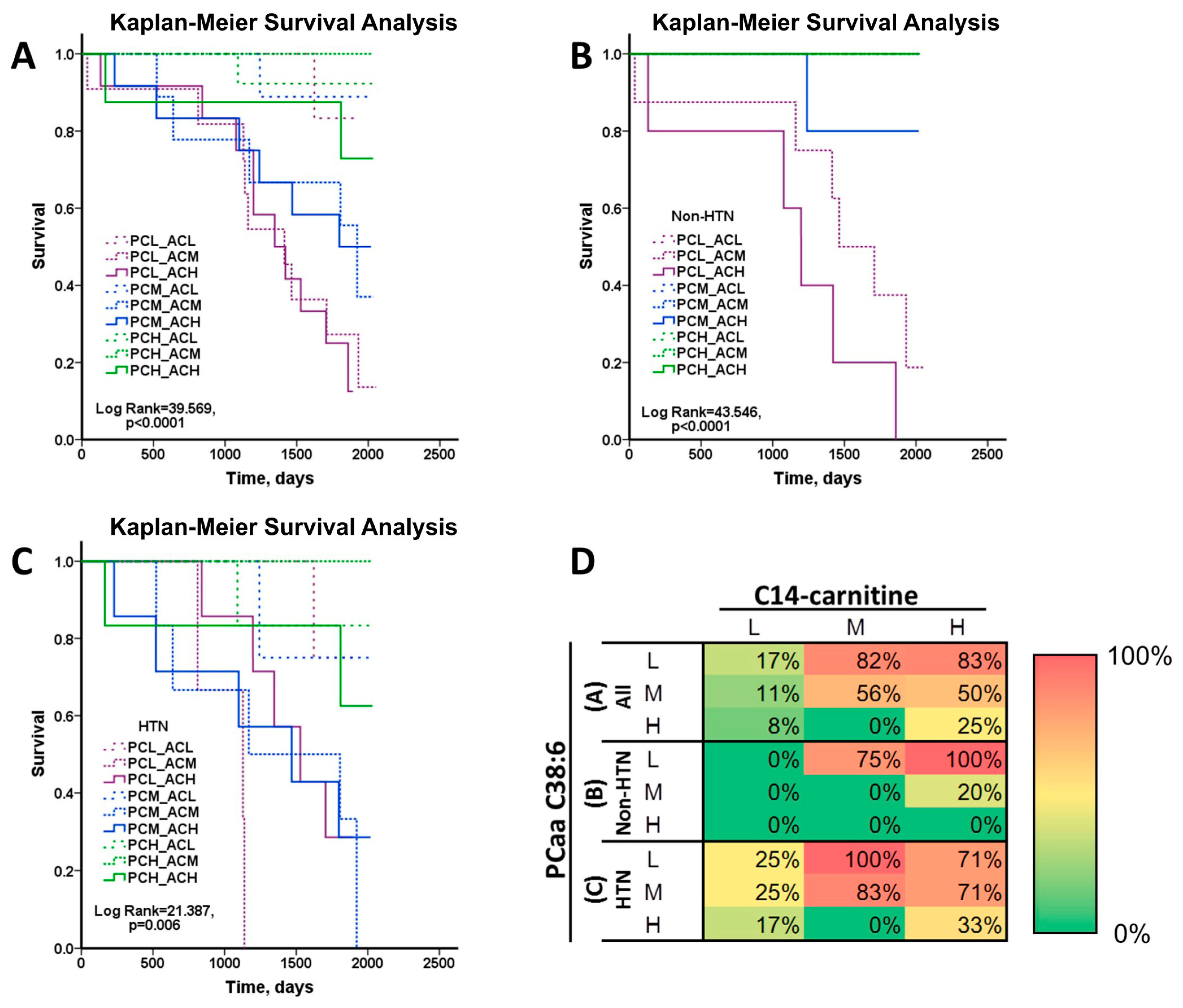
3.4. C14-Carnitine and PCaa C38:6 as Predictor of Mortality
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyere, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef]
- Morley, J.E.; Abbatecola, A.M.; Argiles, J.M.; Baracos, V.; Bauer, J.; Bhasin, S.; Cederholm, T.; Coats, A.J.; Cummings, S.R.; Evans, W.J.; et al. Sarcopenia with limited mobility: An international consensus. J. Am. Med. Dir. Assoc. 2011, 12, 403–409. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Sayer, A.A. Sarcopenia. Lancet 2019, 393, 2636–2646. [Google Scholar] [CrossRef]
- Mayhew, A.J.; Amog, K.; Phillips, S.; Parise, G.; McNicholas, P.D.; de Souza, R.J.; Thabane, L.; Raina, P. The prevalence of sarcopenia in community-dwelling older adults, an exploration of differences between studies and within definitions: A systematic review and meta-analyses. Age Ageing 2019, 48, 48–56. [Google Scholar] [CrossRef]
- Chen, L.K.; Liu, L.K.; Woo, J.; Assantachai, P.; Auyeung, T.W.; Bahyah, K.S.; Chou, M.Y.; Chen, L.Y.; Hsu, P.S.; Krairit, O.; et al. Sarcopenia in Asia: Consensus report of the Asian Working Group for Sarcopenia. J. Am. Med. Dir. Assoc. 2014, 15, 95–101. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.K.; Woo, J.; Assantachai, P.; Auyeung, T.W.; Chou, M.Y.; Iijima, K.; Jang, H.C.; Kang, L.; Kim, M.; Kim, S.; et al. Asian Working Group for Sarcopenia: 2019 Consensus Update on Sarcopenia Diagnosis and Treatment. J. Am. Med. Dir. Assoc. 2020, 21, 300–307.e302. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.; Won, C.W. Sarcopenia in Korean Community-Dwelling Adults Aged 70 Years and Older: Application of Screening and Diagnostic Tools from the Asian Working Group for Sarcopenia 2019 Update. J. Am. Med. Dir. Assoc. 2020, 21, 752–758. [Google Scholar] [CrossRef] [PubMed]
- Hunter, G.R.; Singh, H.; Carter, S.J.; Bryan, D.R.; Fisher, G. Sarcopenia and Its Implications for Metabolic Health. J. Obes. 2019, 2019, 8031705. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Jentoft, A.J.; Baeyens, J.P.; Bauer, J.M.; Boirie, Y.; Cederholm, T.; Landi, F.; Martin, F.C.; Michel, J.P.; Rolland, Y.; Schneider, S.M.; et al. Sarcopenia: European consensus on definition and diagnosis: Report of the European Working Group on Sarcopenia in Older People. Age Ageing 2010, 39, 412–423. [Google Scholar] [CrossRef] [PubMed]
- Pourhassan, M.; Norman, K.; Muller, M.J.; Dziewas, R.; Wirth, R. Impact of Sarcopenia on One-Year Mortality among Older Hospitalized Patients with Impaired Mobility. J. Frailty Aging 2018, 7, 40–46. [Google Scholar] [CrossRef] [PubMed]
- Snyder, C.K.; Lapidus, J.A.; Cawthon, P.M.; Dam, T.T.; Sakai, L.Y.; Marshall, L.M.; Osteoporotic Fractures in Men Research, G. Serum albumin in relation to change in muscle mass, muscle strength, and muscle power in older men. J. Am. Geriatr. Soc. 2012, 60, 1663–1672. [Google Scholar] [CrossRef] [PubMed]
- Uemura, K.; Doi, T.; Lee, S.; Shimada, H. Sarcopenia and Low Serum Albumin Level Synergistically Increase the Risk of Incident Disability in Older Adults. J. Am. Med. Dir. Assoc. 2019, 20, 90–93. [Google Scholar] [CrossRef] [PubMed]
- Wagatsuma, A.; Sakuma, K. Vitamin D signaling in myogenesis: Potential for treatment of sarcopenia. Biomed. Res. Int. 2014, 2014, 121254. [Google Scholar] [CrossRef] [PubMed]
- Remelli, F.; Vitali, A.; Zurlo, A.; Volpato, S. Vitamin D Deficiency and Sarcopenia in Older Persons. Nutrients 2019, 11, 2861. [Google Scholar] [CrossRef] [PubMed]
- Jang, I.Y.; Jung, H.W.; Park, J.H.; Kim, J.H.; Lee, S.; Lee, E.; Lee, J.Y.; Park, S.J.; Kim, D.A.; Kim, S.J.; et al. Lower Serum n-3 Fatty Acid Level in Older Adults with Sarcopenia. Nutrients 2020, 12, 2959. [Google Scholar] [CrossRef]
- Giovannini, S.; Brau, F.; Forino, R.; Berti, A.; D’Ignazio, F.; Loreti, C.; Bellieni, A.; D’Angelo, E.; Di Caro, F.; Biscotti, L.; et al. Sarcopenia: Diagnosis and Management, State of the Art and Contribution of Ultrasound. J. Clin. Med. 2021, 10, 5552. [Google Scholar] [CrossRef]
- Kalinkovich, A.; Livshits, G. Sarcopenia—The search for emerging biomarkers. Ageing Res. Rev. 2015, 22, 58–71. [Google Scholar] [CrossRef]
- Dent, E.; Morley, J.E.; Cruz-Jentoft, A.J.; Arai, H.; Kritchevsky, S.B.; Guralnik, J.; Bauer, J.M.; Pahor, M.; Clark, B.C.; Cesari, M.; et al. International Clinical Practice Guidelines for Sarcopenia (ICFSR): Screening, Diagnosis and Management. J. Nutr. Health Aging 2018, 22, 1148–1161. [Google Scholar] [CrossRef]
- Di Girolamo, F.G.; Situlin, R.; Mazzucco, S.; Valentini, R.; Toigo, G.; Biolo, G. Omega-3 fatty acids and protein metabolism: Enhancement of anabolic interventions for sarcopenia. Curr. Opin. Clin. Nutr. Metab. Care 2014, 17, 145–150. [Google Scholar] [CrossRef]
- Goyens, P.L.; Spilker, M.E.; Zock, P.L.; Katan, M.B.; Mensink, R.P. Compartmental modeling to quantify alpha-linolenic acid conversion after longer term intake of multiple tracer boluses. J. Lipid Res. 2005, 46, 1474–1483. [Google Scholar] [CrossRef]
- Calder, P.C. Docosahexaenoic Acid. Ann. Nutr. Metab. 2016, 69 (Suppl. S1), 7–21. [Google Scholar] [CrossRef]
- Khan, I.; Hussain, M.; Jiang, B.; Zheng, L.; Pan, Y.; Hu, J.; Khan, A.; Ashraf, A.; Zou, X. Omega-3 long-chain polyunsaturated fatty acids: Metabolism and health implications. Prog. Lipid Res. 2023, 92, 101255. [Google Scholar] [CrossRef]
- Longo, N.; Frigeni, M.; Pasquali, M. Carnitine transport and fatty acid oxidation. Biochim. Biophys. Acta 2016, 1863, 2422–2435. [Google Scholar] [CrossRef]
- Reuter, S.E.; Evans, A.M. Carnitine and acylcarnitines: Pharmacokinetic, pharmacological and clinical aspects. Clin. Pharmacokinet. 2012, 51, 553–572. [Google Scholar] [CrossRef]
- Ruiz, M.; Labarthe, F.; Fortier, A.; Bouchard, B.; Thompson Legault, J.; Bolduc, V.; Rigal, O.; Chen, J.; Ducharme, A.; Crawford, P.A.; et al. Circulating acylcarnitine profile in human heart failure: A surrogate of fatty acid metabolic dysregulation in mitochondria and beyond. Am. J. Physiol. Heart Circ. Physiol. 2017, 313, H768–H781. [Google Scholar] [CrossRef]
- Guasch-Ferre, M.; Zheng, Y.; Ruiz-Canela, M.; Hruby, A.; Martinez-Gonzalez, M.A.; Clish, C.B.; Corella, D.; Estruch, R.; Ros, E.; Fito, M.; et al. Plasma acylcarnitines and risk of cardiovascular disease: Effect of Mediterranean diet interventions. Am. J. Clin. Nutr. 2016, 103, 1408–1416. [Google Scholar] [CrossRef]
- Guasch-Ferre, M.; Ruiz-Canela, M.; Li, J.; Zheng, Y.; Bullo, M.; Wang, D.D.; Toledo, E.; Clish, C.; Corella, D.; Estruch, R.; et al. Plasma Acylcarnitines and Risk of Type 2 Diabetes in a Mediterranean Population at High Cardiovascular Risk. J. Clin. Endocrinol. Metab. 2019, 104, 1508–1519. [Google Scholar] [CrossRef] [PubMed]
- Xia, F.Y.; Zhu, L.; Xu, C.; Wu, Q.Q.; Chen, W.J.; Zeng, R.; Deng, Y.Y. Plasma acylcarnitines could predict prognosis and evaluate treatment of IgA nephropathy. Nutr. Metab. 2019, 16, 2. [Google Scholar] [CrossRef]
- Lo, C.J.; Lin, C.M.; Fan, C.M.; Tang, H.Y.; Liu, H.F.; Ho, H.Y.; Cheng, M.L. Plasma acylcarnitine in elderly Taiwanese: As biomarkers of possible sarcopenia and sarcopenia. BMC Geriatr. 2023, 23, 769. [Google Scholar] [CrossRef]
- Caballero, F.F.; Struijk, E.A.; Lana, A.; Buno, A.; Rodriguez-Artalejo, F.; Lopez-Garcia, E. Plasma acylcarnitines and risk of lower-extremity functional impairment in older adults: A nested case-control study. Sci. Rep. 2021, 11, 3350. [Google Scholar] [CrossRef]
- Moaddel, R.; Fabbri, E.; Khadeer, M.A.; Carlson, O.D.; Gonzalez-Freire, M.; Zhang, P.; Semba, R.D.; Ferrucci, L. Plasma Biomarkers of Poor Muscle Quality in Older Men and Women from the Baltimore Longitudinal Study of Aging. J. Gerontol. A Biol. Sci. Med. Sci. 2016, 71, 1266–1272. [Google Scholar] [CrossRef] [PubMed]
- Korostishevsky, M.; Steves, C.J.; Malkin, I.; Spector, T.; Williams, F.M.; Livshits, G. Genomics and metabolomics of muscular mass in a community-based sample of UK females. Eur. J. Hum. Genet. 2016, 24, 277–283. [Google Scholar] [CrossRef]
- Lustgarten, M.S.; Price, L.L.; Chale, A.; Phillips, E.M.; Fielding, R.A. Branched chain amino acids are associated with muscle mass in functionally limited older adults. J. Gerontol. A Biol. Sci. Med. Sci. 2014, 69, 717–724. [Google Scholar] [CrossRef] [PubMed]
- Lustgarten, M.S.; Price, L.L.; Chale, A.; Fielding, R.A. Metabolites related to gut bacterial metabolism, peroxisome proliferator-activated receptor-alpha activation, and insulin sensitivity are associated with physical function in functionally-limited older adults. Aging Cell 2014, 13, 918–925. [Google Scholar] [CrossRef]
- Da Boit, M.; Tommasi, S.; Elliot, D.; Zinellu, A.; Sotgia, S.; Sibson, R.; Meakin, J.R.; Aspden, R.M.; Carru, C.; Mangoni, A.A.; et al. Sex Differences in the Associations between L-Arginine Pathway Metabolites, Skeletal Muscle Mass and Function, and their Responses to Resistance Exercise, in Old Age. J. Nutr. Health Aging 2018, 22, 534–540. [Google Scholar] [CrossRef]
- Fazelzadeh, P.; Hangelbroek, R.W.; Tieland, M.; de Groot, L.C.; Verdijk, L.B.; van Loon, L.J.; Smilde, A.K.; Alves, R.D.; Vervoort, J.; Muller, M.; et al. The Muscle Metabolome Differs between Healthy and Frail Older Adults. J. Proteome Res. 2016, 15, 499–509. [Google Scholar] [CrossRef]
- Zhao, Q.; Shen, H.; Su, K.J.; Tian, Q.; Zhao, L.J.; Qiu, C.; Garrett, T.J.; Liu, J.; Kakhniashvili, D.; Deng, H.W. A joint analysis of metabolomic profiles associated with muscle mass and strength in Caucasian women. Aging 2018, 10, 2624–2635. [Google Scholar] [CrossRef]
- Murphy, R.A.; Moore, S.C.; Playdon, M.; Meirelles, O.; Newman, A.B.; Milijkovic, I.; Kritchevsky, S.B.; Schwartz, A.; Goodpaster, B.H.; Sampson, J.; et al. Metabolites Associated with Lean Mass and Adiposity in Older Black Men. J. Gerontol. A Biol. Sci. Med. Sci. 2017, 72, 1352–1359. [Google Scholar] [CrossRef]
- Lu, Y.; Karagounis, L.G.; Ng, T.P.; Carre, C.; Narang, V.; Wong, G.; Tan, C.T.Y.; Zin Nyunt, M.S.; Gao, Q.; Abel, B.; et al. Systemic and Metabolic Signature of Sarcopenia in Community-Dwelling Older Adults. J. Gerontol. A Biol. Sci. Med. Sci. 2020, 75, 309–317. [Google Scholar] [CrossRef]
- Karpman, C.; Lebrasseur, N.K.; Depew, Z.S.; Novotny, P.J.; Benzo, R.P. Measuring gait speed in the out-patient clinic: Methodology and feasibility. Respir. Care 2014, 59, 531–537. [Google Scholar] [CrossRef] [PubMed]
- Cheng, M.L.; Wang, C.H.; Shiao, M.S.; Liu, M.H.; Huang, Y.Y.; Huang, C.Y.; Mao, C.T.; Lin, J.F.; Ho, H.Y.; Yang, N.I. Metabolic disturbances identified in plasma are associated with outcomes in patients with heart failure: Diagnostic and prognostic value of metabolomics. J. Am. Coll. Cardiol. 2015, 65, 1509–1520. [Google Scholar] [CrossRef] [PubMed]
- Lo, C.J.; Tang, H.Y.; Huang, C.Y.; Lin, C.M.; Ho, H.Y.; Shiao, M.S.; Cheng, M.L. Metabolic Signature Differentiated Diabetes Mellitus from Lipid Disorder in Elderly Taiwanese. J. Clin. Med. 2018, 8, 13. [Google Scholar] [CrossRef]
- Tsai, H.I.; Lo, C.J.; Zheng, C.W.; Lee, C.W.; Lee, W.C.; Lin, J.R.; Shiao, M.S.; Cheng, M.L.; Yu, H.P. A Lipidomics Study Reveals Lipid Signatures Associated with Early Allograft Dysfunction in Living Donor Liver Transplantation. J. Clin. Med. 2018, 8, 30. [Google Scholar] [CrossRef] [PubMed]
- Pang, Z.; Chong, J.; Zhou, G.; de Lima Morais, D.A.; Chang, L.; Barrette, M.; Gauthier, C.; Jacques, P.E.; Li, S.; Xia, J. MetaboAnalyst 5.0: Narrowing the gap between raw spectra and functional insights. Nucleic Acids Res. 2021, 49, W388–W396. [Google Scholar] [CrossRef] [PubMed]
- Bai, T.; Fang, F.; Li, F.; Ren, Y.; Hu, J.; Cao, J. Sarcopenia is associated with hypertension in older adults: A systematic review and meta-analysis. BMC Geriatr. 2020, 20, 279. [Google Scholar] [CrossRef] [PubMed]
- Srivastava, S. The Mitochondrial Basis of Aging and Age-Related Disorders. Genes 2017, 8, 398. [Google Scholar] [CrossRef] [PubMed]
- Guo, Y.; Guan, T.; Shafiq, K.; Yu, Q.; Jiao, X.; Na, D.; Li, M.; Zhang, G.; Kong, J. Mitochondrial dysfunction in aging. Ageing Res. Rev. 2023, 88, 101955. [Google Scholar] [CrossRef] [PubMed]
- McGill, M.R.; Li, F.; Sharpe, M.R.; Williams, C.D.; Curry, S.C.; Ma, X.; Jaeschke, H. Circulating acylcarnitines as biomarkers of mitochondrial dysfunction after acetaminophen overdose in mice and humans. Arch. Toxicol. 2014, 88, 391–401. [Google Scholar] [CrossRef]
- Gu, X.; Wang, W.; Yang, Y.; Lei, Y.; Liu, D.; Wang, X.; Wu, T. The Effect of Metabolites on Mitochondrial Functions in the Pathogenesis of Skeletal Muscle Aging. Clin. Interv. Aging 2022, 17, 1275–1295. [Google Scholar] [CrossRef]
- Jarrell, Z.R.; Smith, M.R.; Hu, X.; Orr, M.; Liu, K.H.; Quyyumi, A.A.; Jones, D.P.; Go, Y.M. Plasma acylcarnitine levels increase with healthy aging. Aging 2020, 12, 13555–13570. [Google Scholar] [CrossRef]
- McCoin, C.S.; Knotts, T.A.; Ono-Moore, K.D.; Oort, P.J.; Adams, S.H. Long-chain acylcarnitines activate cell stress and myokine release in C2C12 myotubes: Calcium-dependent and -independent effects. Am. J. Physiol. Endocrinol. Metab. 2015, 308, E990–E1000. [Google Scholar] [CrossRef]
- Rutkowsky, J.M.; Knotts, T.A.; Ono-Moore, K.D.; McCoin, C.S.; Huang, S.; Schneider, D.; Singh, S.; Adams, S.H.; Hwang, D.H. Acylcarnitines activate proinflammatory signaling pathways. Am. J. Physiol. Endocrinol. Metab. 2014, 306, E1378–E1387. [Google Scholar] [CrossRef]
- Ferrucci, L.; Fabbri, E. Inflammageing: Chronic inflammation in ageing, cardiovascular disease, and frailty. Nat. Rev. Cardiol. 2018, 15, 505–522. [Google Scholar] [CrossRef]
- Chung, H.Y.; Cesari, M.; Anton, S.; Marzetti, E.; Giovannini, S.; Seo, A.Y.; Carter, C.; Yu, B.P.; Leeuwenburgh, C. Molecular inflammation: Underpinnings of aging and age-related diseases. Ageing Res. Rev. 2009, 8, 18–30. [Google Scholar] [CrossRef]
- Harris, W.S. The omega-3 index: From biomarker to risk marker to risk factor. Curr. Atheroscler. Rep. 2009, 11, 411–417. [Google Scholar] [CrossRef]
- McGlory, C.; Calder, P.C.; Nunes, E.A. The Influence of Omega-3 Fatty Acids on Skeletal Muscle Protein Turnover in Health, Disuse, and Disease. Front. Nutr. 2019, 6, 144. [Google Scholar] [CrossRef]
- Jeromson, S.; Gallagher, I.J.; Galloway, S.D.; Hamilton, D.L. Omega-3 Fatty Acids and Skeletal Muscle Health. Mar. Drugs 2015, 13, 6977–7004. [Google Scholar] [CrossRef]
- Okamura, T.; Hashimoto, Y.; Miki, A.; Kaji, A.; Sakai, R.; Iwai, K.; Osaka, T.; Ushigome, E.; Hamaguchi, M.; Yamazaki, M.; et al. Reduced dietary omega-3 fatty acids intake is associated with sarcopenia in elderly patients with type 2 diabetes: A cross-sectional study of KAMOGAWA-DM cohort study. J. Clin. Biochem. Nutr. 2020, 66, 233–237. [Google Scholar] [CrossRef] [PubMed]
- Wahlin-Larsson, B.; Carnac, G.; Kadi, F. The influence of systemic inflammation on skeletal muscle in physically active elderly women. Age 2014, 36, 9718. [Google Scholar] [CrossRef] [PubMed]
- Oppedisano, F.; Macri, R.; Gliozzi, M.; Musolino, V.; Carresi, C.; Maiuolo, J.; Bosco, F.; Nucera, S.; Caterina Zito, M.; Guarnieri, L.; et al. The Anti-Inflammatory and Antioxidant Properties of n-3 PUFAs: Their Role in Cardiovascular Protection. Biomedicines 2020, 8, 306. [Google Scholar] [CrossRef] [PubMed]
- Back, M. Omega-3 fatty acids in atherosclerosis and coronary artery disease. Future Sci. OA 2017, 3, FSO236. [Google Scholar] [CrossRef]
- Bhullar, A.S.; Putman, C.T.; Mazurak, V.C. Potential Role of Omega-3 Fatty Acids on the Myogenic Program of Satellite Cells. Nutr. Metab. Insights 2016, 9, NMI-S27481. [Google Scholar] [CrossRef] [PubMed]
- Briolay, A.; Jaafar, R.; Nemoz, G.; Bessueille, L. Myogenic differentiation and lipid-raft composition of L6 skeletal muscle cells are modulated by PUFAs. Biochim. Biophys. Acta 2013, 1828, 602–613. [Google Scholar] [CrossRef] [PubMed]
- Lewis, E.J.; Radonic, P.W.; Wolever, T.M.; Wells, G.D. 21 days of mammalian omega-3 fatty acid supplementation improves aspects of neuromuscular function and performance in male athletes compared to olive oil placebo. J. Int. Soc. Sports Nutr. 2015, 12, 28. [Google Scholar] [CrossRef] [PubMed]
- Markworth, J.F.; Brown, L.A.; Lim, E.; Floyd, C.; Larouche, J.; Castor-Macias, J.A.; Sugg, K.B.; Sarver, D.C.; Macpherson, P.C.; Davis, C.; et al. Resolvin D1 supports skeletal myofiber regeneration via actions on myeloid and muscle stem cells. JCI Insight 2020, 5, e137713. [Google Scholar] [CrossRef] [PubMed]
- Tachtsis, B.; Camera, D.; Lacham-Kaplan, O. Potential Roles of n-3 PUFAs during Skeletal Muscle Growth and Regeneration. Nutrients 2018, 10, 309. [Google Scholar] [CrossRef] [PubMed]
- Kamolrat, T.; Gray, S.R. The effect of eicosapentaenoic and docosahexaenoic acid on protein synthesis and breakdown in murine C2C12 myotubes. Biochem. Biophys. Res. Commun. 2013, 432, 593–598. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Jeon, J.H.; Lee, M.J. Docosahexaenoic Acid, a Potential Treatment for Sarcopenia, Modulates the Ubiquitin-Proteasome and the Autophagy-Lysosome Systems. Nutrients 2020, 12, 2597. [Google Scholar] [CrossRef]
- Jain, A.P.; Aggarwal, K.K.; Zhang, P.Y. Omega-3 fatty acids and cardiovascular disease. Eur. Rev. Med. Pharmacol. Sci. 2015, 19, 441–445. [Google Scholar]
- DiNicolantonio, J.J.; O’Keefe, J.H. The Benefits of Omega-3 Fats for Stabilizing and Remodeling Atherosclerosis. Mo. Med. 2020, 117, 65–69. [Google Scholar]
- Dyall, S.C. Long-chain omega-3 fatty acids and the brain: A review of the independent and shared effects of EPA, DPA and DHA. Front. Aging Neurosci. 2015, 7, 52. [Google Scholar] [CrossRef]
- Wang, H.; Li, Q.; Zhu, Y.; Zhang, X. Omega-3 Polyunsaturated Fatty Acids: Versatile Roles in Blood Pressure Regulation. Antioxid. Redox Signal. 2021, 34, 800–810. [Google Scholar] [CrossRef] [PubMed]
- Yagi, S.; Fukuda, D.; Aihara, K.I.; Akaike, M.; Shimabukuro, M.; Sata, M. n-3 Polyunsaturated Fatty Acids: Promising Nutrients for Preventing Cardiovascular Disease. J. Atheroscler. Thromb. 2017, 24, 999–1010. [Google Scholar] [CrossRef] [PubMed]
- Yu, M.D.; Zhang, H.Z.; Zhang, Y.; Yang, S.P.; Lin, M.; Zhang, Y.M.; Wu, J.B.; Hong, F.Y.; Chen, W.X. Relationship between chronic kidney disease and sarcopenia. Sci. Rep. 2021, 11, 20523. [Google Scholar] [CrossRef] [PubMed]
- Baechle, J.J.; Chen, N.; Makhijani, P.; Winer, S.; Furman, D.; Winer, D.A. Chronic inflammation and the hallmarks of aging. Mol. Metab. 2023, 74, 101755. [Google Scholar] [CrossRef]
- Pugh, D.; Dhaun, N. Hypertension and Vascular Inflammation: Another Piece of the Genetic Puzzle. Hypertension 2021, 77, 190–192. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Non-Sarcopenic | Sarcopenic | |||||
|---|---|---|---|---|---|---|
| Parameter | Alive, N = 106 | Dead, N = 10 | p-Value 1 | Alive, N = 54 | Dead, N = 35 | p-Value 1 |
| Age & body index, and physical function | ||||||
| Age (years) | 79.4 ± 7.3 | 81.2 ± 7.3 | 0.4603 | 82.8 ± 5.7 | 87.8 ± 4.1 | <0.0001 |
| Sex (% male) | 25% | 40% | 0.4537 | 44% | 89% | <0.0001 |
| ASMI (kg/m2) | 6.2 ± 0.8 | 6.7 ± 0.6 | 0.0491 | 5.5 ± 0.9 | 6.0 ± 0.7 | 0.0053 |
| HGS (kg) | 19.0 ± 7.5 | 21.8 ± 8.9 | 0.2683 | 17.7 ± 7.1 | 18.5 ± 4.7 | 0.5356 |
| GS (m/s) | 1.1 ± 0.3 | 0.9 ± 0.3 | 0.0413 | 1.1 ± 0.3 | 0.8 ± 0.3 | <0.0001 |
| BMI (kg/m2) | 24.2 ± 3.0 | 26.5 ± 3.7 | 0.0270 | 21.2 ± 2.5 | 22.7 ± 3.1 | 0.0152 |
| Complete blood count | ||||||
| WBC (103/μL) | 5.5 ± 1.5 | 5.6 ± 1.1 | 0.7260 | 5.5 ± 1.3 | 5.7 ± 1.3 | 0.3403 |
| Segment (%) | 56.5 ± 8.8 | 57.9 ± 10.1 | 0.6231 | 58.5 ± 8.1 | 59.8 ± 10.4 | 0.5110 |
| Lymphocyte (%) | 33.9 ± 8.4 | 33.0 ± 9.7 | 0.7259 | 31.6 ± 7.2 | 29.6 ± 9.5 | 0.2709 |
| Monocyte (%) | 6.2 ± 1.6 | 5.4 ± 1.1 | 0.1637 | 6.4 ± 1.5 | 5.9 ± 1.4 | 0.1161 |
| Eosinophil (%) | 2.9 ± 2.1 | 3.3 ± 2.0 | 0.5753 | 3.0 ± 2.5 | 4.1 ± 3.6 | 0.1215 |
| Basophil (%) | 0.6 ± 0.4 | 0.4 ± 0.2 | 0.0813 | 0.6 ± 0.4 | 0.5 ± 0.3 | 0.7907 |
| RBC (106/μL) | 4.3 ± 0.5 | 4.7 ± 0.5 | 0.0558 | 4.3 ± 0.4 | 4.1 ± 0.5 | 0.0362 |
| Hemoglobin (g/dL) | 13.1 ± 1.6 | 13.7 ± 0.9 | 0.2337 | 13.3 ± 1.3 | 12.4 ± 1.8 | 0.0097 |
| Hematocrit (%) | 39.5 ± 4.2 | 40.8 ± 2.2 | 0.1087 | 39.8 ± 3.6 | 37.2 ± 4.7 | 0.0049 |
| MCV (fL) | 91.3 ± 5.8 | 88.4 ± 8.8 | 0.3349 | 92.1 ± 3.8 | 90.5 ± 5.2 | 0.1237 |
| MCH (pg/cell) | 30.4 ± 2.4 | 29.7 ± 3.3 | 0.4540 | 30.8 ± 1.3 | 30.0 ± 2.6 | 0.1267 |
| MCHC (gHb/dL) | 33.2 ± 1.0 | 33.6 ± 0.7 | 0.2672 | 33.4 ± 0.7 | 33.1 ± 1.5 | 0.2942 |
| RDW (%) | 13.6 ± 1.5 | 14.1 ± 1.9 | 0.3019 | 13.4 ± 0.6 | 13.9 ± 1.6 | 0.0873 |
| Platelets (103/μL) | 203.6 ± 49.0 | 176.7 ± 43.2 | 0.0962 | 193.4 ± 49.8 | 192.9 ± 45.6 | 0.9647 |
| Biochemical test | ||||||
| Cholesterol (mg/dL) | 184.2 ± 36.7 | 185.1 ± 55.7 | 0.9614 | 180.1 ± 31.8 | 168.3 ± 38.1 | 0.1180 |
| Triglyceride (mg/dL) | 109.5 ± 58.0 | 96.6 ± 45.9 | 0.4971 | 88.2 ± 33.7 | 88.3 ± 51.7 | 0.9927 |
| LDLC (mg/dL) | 108.3 ± 32.6 | 111.9 ± 45.2 | 0.7471 | 104.5 ± 26.0 | 100.1 ± 31.1 | 0.4647 |
| HDLC (mg/dL) | 53.3 ± 11.9 | 53.9 ± 10.0 | 0.8799 | 57.4 ± 14.3 | 49.7 ± 12.2 | 0.0104 |
| Insulin (μlU/mL) | 6.7 ± 8.6 | 6.1 ± 3.7 | 0.6510 | 4.9 ± 7.5 | 4.7 ± 3.7 | 0.8697 |
| Glucose (mg/dL) | 97.2 ± 15.4 | 100.2 ± 15.8 | 0.5540 | 97.6 ± 22.2 | 101.3 ± 22.8 | 0.4611 |
| HbA1c (%) | 5.8 ± 0.5 | 5.9 ± 0.6 | 0.8402 | 5.9 ± 0.7 | 5.9 ± 0.8 | 0.7032 |
| HOMA-IR | 1.7 ± 2.1 | 1.6 ± 1.3 | 0.8948 | 1.2 ± 1.7 | 1.2 ± 1.0 | 0.9367 |
| Albumin (g/dL) | 4.4 ± 0.3 | 4.2 ± 0.2 | 0.0561 | 4.4 ± 0.2 | 4.2 ± 0.3 | 0.0008 |
| Total protein (g/dL) | 7.0 ± 0.4 | 6.9 ± 0.3 | 0.4134 | 7.0 ± 0.4 | 6.9 ± 0.4 | 0.1557 |
| BUN (mg/dL) | 17.4 ± 8.8 | 15.0 ± 2.3 | 0.0358 | 16.3 ± 4.3 | 24.8 ± 12.4 | 0.0004 |
| Creatinine (mg/dL) | 0.9 ± 0.9 | 0.8 ± 0.2 | 0.5016 | 0.8 ± 0.3 | 1.3 ± 0.9 | 0.0024 |
| AST/GOT (U/L) | 26.9 ± 9.9 | 32.4 ± 14.3 | 0.1117 | 28.7 ± 8.9 | 25.1 ± 8.4 | 0.0567 |
| ALT/GPT (U/L) | 20.3 ± 18.9 | 25.0 ± 9.9 | 0.2163 | 19.7 ± 12.7 | 16.5 ± 8.6 | 0.1534 |
| ALKP (U/L) | 67.4 ± 18.7 | 72.9 ± 35.0 | 0.6356 | 59.6 ± 15.5 | 64.7 ± 24.3 | 0.2718 |
| Total bilirubin (mg/dL) | 0.7 ± 0.3 | 0.7 ± 0.2 | 0.9267 | 0.8 ± 0.5 | 0.8 ± 0.5 | 0.8682 |
| TSH (μIU/mL) | 2.7 ± 2.2 | 2.6 ± 2.5 | 0.9643 | 2.4 ± 2.2 | 2.6 ± 1.8 | 0.6058 |
| Uric acid (mg/dL) | 5.5 ± 1.4 | 5.9 ± 2.2 | 0.6608 | 5.5 ± 1.2 | 6.7 ± 2.1 | 0.0018 |
| T4 (μg/dL) | 8.1 ± 1.7 | 9.0 ± 1.5 | 0.1570 | 8.2 ± 1.5 | 7.9 ± 1.9 | 0.3987 |
| Cortisol (μg/dL) | 13.6 ± 4.6 | 10.2 ± 5.4 | 0.0292 | 14.0 ± 4.5 | 16.3 ± 5.5 | 0.0352 |
| Vitamin B12 (pg/mL) | 762.4 ± 578.8 | 729.4 ± 361.6 | 0.8601 | 758.2 ± 632.6 | 789.8 ± 500.8 | 0.8039 |
| Comorbidities (%) | ||||||
| HTN | 58% | 60% | 1.0000 | 43% | 66% | 0.0501 |
| Diabetes | 21% | 30% | 0.4472 | 31% | 17% | 0.1466 |
| Hyperlipidemia | 38% | 40% | 1.0000 | 31% | 23% | 0.4716 |
| CAD | 8% | 0% | 1.0000 | 9% | 11% | 0.7341 |
| Stroke | 4% | 10% | 0.3682 | 6% | 17% | 0.1462 |
| CKD | 8% | 10% | 1.0000 | 13% | 29% | 0.0971 |
| COPD | 15% | 10% | 1.0000 | 31% | 37% | 0.6490 |
| Osteoporosis | 26% | 20% | 1.0000 | 37% | 34% | 0.8249 |
| Non-Sarcopenic | Sarcopenic | ||||||
|---|---|---|---|---|---|---|---|
| Metabolite, μM | Alive, N = 106 | Dead, N = 10 | p-Value 1 | Alive, N = 54 | Dead, N = 35 | p-Value 1 | PFDR |
| PCaa C40:6 | 32.839 ± 9.150 | 33.620 ± 14.030 | 0.8664 | 30.774 ± 7.525 | 23.278 ± 7.337 | 1.2 × 10−5 | 0.0022 |
| PCaa C38:6 | 88.734 ± 23.968 | 92.170 ± 32.817 | 0.6759 | 85.576 ± 22.647 | 66.229 ± 20.437 | 9.7 × 10−5 | 0.0058 |
| C14 | 0.035 ± 0.006 | 0.036 ± 0.003 | 0.5532 | 0.035 ± 0.006 | 0.040 ± 0.006 | 0.0002 | 0.0072 |
| C3-DC (C4-OH) | 0.062 ± 0.027 | 0.061 ± 0.016 | 0.9229 | 0.058 ± 0.018 | 0.073 ± 0.023 | 0.0005 | 0.0140 |
| PCae C38:0 | 1.754 ± 0.678 | 1.732 ± 0.728 | 0.9230 | 1.688 ± 0.540 | 1.298 ± 0.530 | 0.0012 | 0.0266 |
| PCae C40:1 | 1.030 ± 0.280 | 0.986 ± 0.294 | 0.6317 | 1.073 ± 0.283 | 0.833 ± 0.246 | 8.9 × 10−5 | 0.0080 |
| SM (OH) 22:1 | 49.325 ± 10.752 | 51.520 ± 13.016 | 0.5456 | 49.841 ± 9.998 | 41.783 ± 8.431 | 0.0002 | 0.0058 |
| SM (OH) 22:2 | 52.066 ± 12.564 | 55.070 ± 11.672 | 0.4689 | 52.750 ± 9.190 | 44.994 ± 10.906 | 0.0005 | 0.0153 |
| SDMA | 0.760 ± 0.417 | 0.799 ± 0.180 | 0.5866 | 0.789 ± 0.257 | 1.120 ± 0.538 | 0.0014 | 0.0288 |
| Model 1 | Model 2 | |||
|---|---|---|---|---|
| Variables | HR (95% CI) | p Value | HR (95% CI) | p Value |
| Sex | 16.635 (2.449–113.005) | 0.004 | 12.132 (1.663–88.494) | 0.014 |
| HTN | 5.314 (1.639–17.228) | 0.005 | 6.194 (1.813–21.189) | 0.004 |
| C14, nM | 1.099 (1.015–1.190) | 0.020 | 1.097 (1.013–1.186) | 0.022 |
| PCaa C38:6, μM 1 | 0.962 (0.929–0.996) | 0.030 | ||
| PCaa C40:6, μM 2 | 0.875 (0.789–0.971) | 0.012 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ho, H.-Y.; Chen, Y.-H.; Lo, C.-J.; Tang, H.-Y.; Chang, S.-W.; Fan, C.-M.; Ho, Y.-H.; Lin, G.; Chiu, C.-Y.; Lin, C.-M.; et al. Combined Plasma DHA-Containing Phosphatidylcholine PCaa C38:6 and Tetradecanoyl-Carnitine as an Early Biomarker for Assessing the Mortality Risk among Sarcopenic Patients. Nutrients 2024, 16, 611. https://doi.org/10.3390/nu16050611
Ho H-Y, Chen Y-H, Lo C-J, Tang H-Y, Chang S-W, Fan C-M, Ho Y-H, Lin G, Chiu C-Y, Lin C-M, et al. Combined Plasma DHA-Containing Phosphatidylcholine PCaa C38:6 and Tetradecanoyl-Carnitine as an Early Biomarker for Assessing the Mortality Risk among Sarcopenic Patients. Nutrients. 2024; 16(5):611. https://doi.org/10.3390/nu16050611
Chicago/Turabian StyleHo, Hung-Yao, Yuan-Ho Chen, Chi-Jen Lo, Hsiang-Yu Tang, Su-Wei Chang, Chun-Ming Fan, Yu-Hsuan Ho, Gigin Lin, Chih-Yung Chiu, Chih-Ming Lin, and et al. 2024. "Combined Plasma DHA-Containing Phosphatidylcholine PCaa C38:6 and Tetradecanoyl-Carnitine as an Early Biomarker for Assessing the Mortality Risk among Sarcopenic Patients" Nutrients 16, no. 5: 611. https://doi.org/10.3390/nu16050611