

Impact of Reducing Intake of Red and Processed Meat on Colorectal Cancer Incidence in Germany 2020 to 2050—A Simulation Study

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Red and Processed Meat Intake
2.2. Expected Numbers of CRC Cases without Intervention
2.3. Risk Estimates
2.4. Statistical Analysis
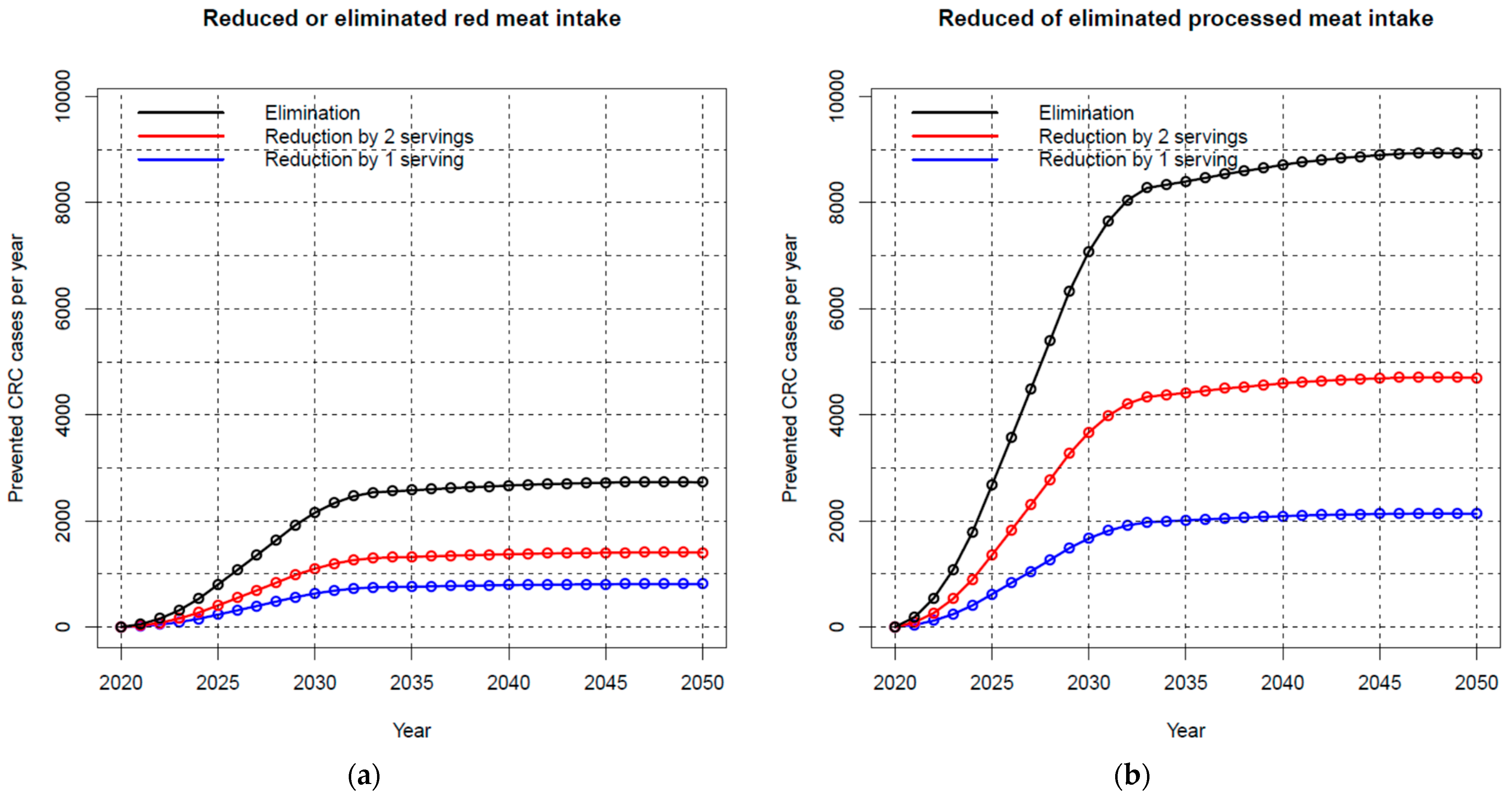
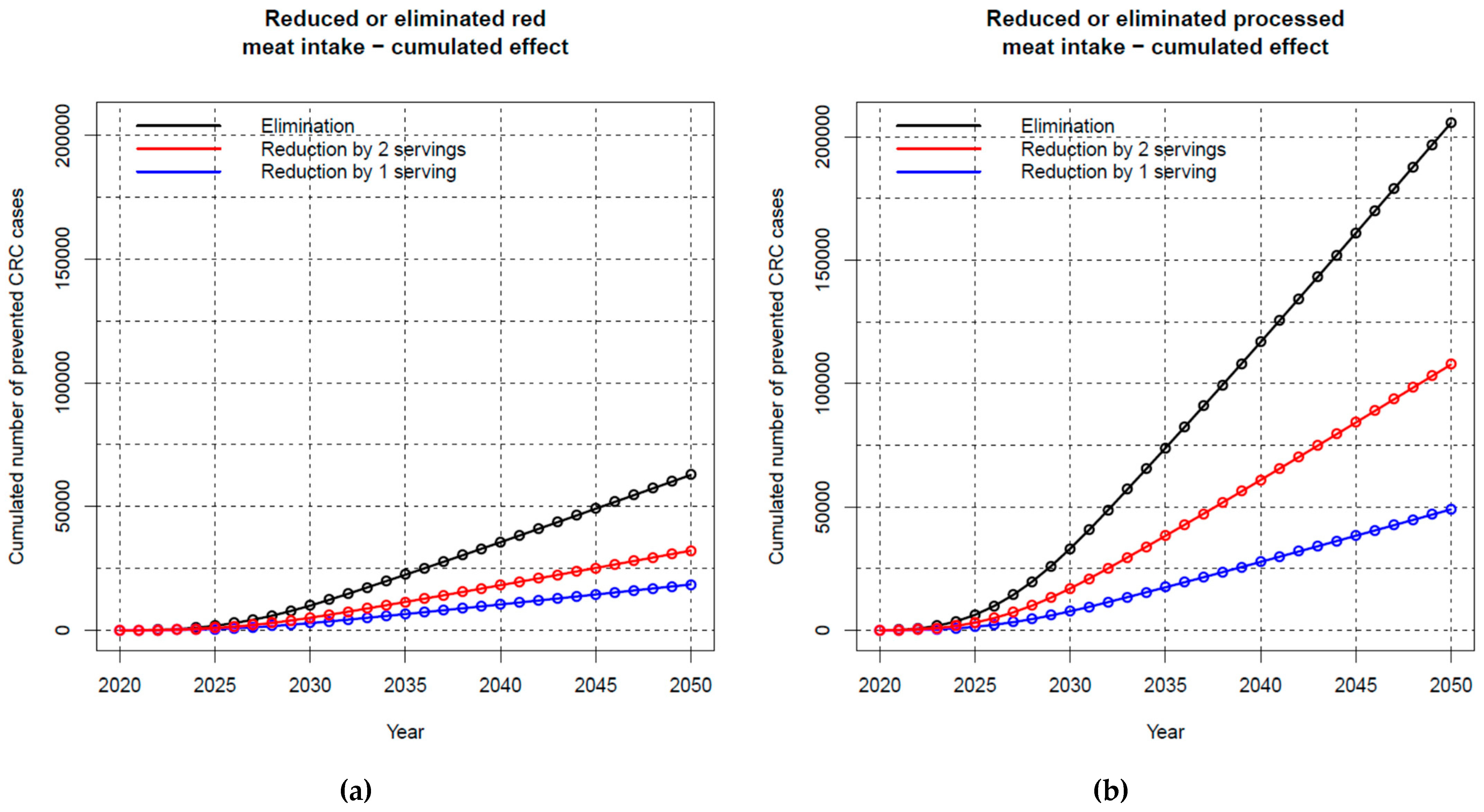
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ferlay, J.; Soerjomataram, I.; Ervik, M.; Dikshit, R.; Eser, S.; Mathers, C.; Rebelo, M.; Parkin, D.M.; Forman, D.; Bray, F. International Agency for Research on Cancer; GLOBOCAN: Lyon, France; Available online: https://gco.iarc.fr/ (accessed on 25 April 2022).
- Heisser, T.; Simon, A.; Hapfelmeier, J.; Hoffmeister, M.; Brenner, H. Treatment Costs of Colorectal Cancer by Sex and Age: Population-Based Study on Health Insurance Data from Germany. Cancers 2022, 14, 3836. [Google Scholar] [CrossRef] [PubMed]
- Bouvard, V.; Loomis, D.; Guyton, K.Z.; Grosse, Y.; El Ghissassi, F.; Benbrahim-Tallaa, L.; Guha, N.; Mattock, H.; Straif, K.; Corpet, D. Carcinogenicity of consumption of red and processed meat. Lancet Oncol. 2015, 16, 1599–1600. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kamtsiuris, P.; Lange, M.; Hoffmann, R.; Rosario, A.S.; Dahm, S.; Kuhnert, R.; Kurth, B.M. Die erste Welle der Studie zur Gesundheit Erwachsener in Deutschland (DEGS1) [The first wave of the German Health Interview and Examination Survey for Adults]. Bundesgesundheitsblatt Gesundh. Gesundh. 2013, 56, 620–630. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Cancer Research Fund; American Institute for Cancer Research. Continuous Update Project Expert Report 2018. Diet, Nutrition, Physical Activity and Colorectal Cancer. Available online: http://dietandcancerreport.org (accessed on 30 March 2022).
- Deutsche Gesellschaft für Ernährung e.V. Vollwertig Essen und Trinken Nach den 10 Regeln der DGE. Available online: https://www.dge.de/ernaehrungspraxis/vollwertige-ernaehrung/10-regeln-der-dge (accessed on 1 September 2022).
- Behrens, G.; Gredner, T.; Stock, C.; Leitzmann, M.F.; Brenner, H.; Mons, U. Cancers Due to Excess Weight, Low Physical Activity, and Unhealthy Diet. Dtsch. Arztebl. Int. 2018, 115, 578–585. [Google Scholar] [CrossRef] [PubMed]
- Barendregt, J.J.; Veerman, J.L. Categorical versus continuous risk factors and the calculation of potential impact fractions. J. Epidemiol. Community Health 2010, 64, 209–212. [Google Scholar] [CrossRef]
- Kuhn, D.-A. Entwicklung Eines Index zur Bewertung der Ernährungsqualität in der Studie zur Gesundheit Erwachsener in Deutschland (DEGS1); Robert Koch-Institut: Berlin, Germany, 2018. [Google Scholar]
- Robert Koch Institut. German Centre for Cancer Registry Data (ZfKD). Available online: http://www.krebsdaten.de (accessed on 17 June 2022).
- Federal Statistical Office (Destatis). Germany’s Population by 2060: Results of the 14th Coordinated Population Projection. Wiesbaden: Destatis. Available online: https://www.destatis.de/EN/Themes/Society-Environment/Population/Population-Projection/_node.html#sprg479856 (accessed on 22 April 2022).
- Soerjomataram, I.; de Vries, E.; Engholm, G.; Paludan-Müller, G.; Brønnum-Hansen, H.; Storm, H.H.; Barendregt, J.J. Impact of a smoking and alcohol intervention programme on lung and breast cancer incidence in Denmark: An example of dynamic modelling with Prevent. Eur. J. Cancer 2010, 46, 2617–2624. [Google Scholar] [CrossRef]
- Brenner, H.; Altenhofen, L.; Katalinic, A.; Lansdorp-Vogelaar, I.; Hoffmeister, M. Sojourn time of preclinical colorectal cancer by sex and age: Estimates from the German national screening colonoscopy database. Am. J. Epidemiol. 2011, 174, 1140–1146. [Google Scholar] [CrossRef]
- Haggar, F.A.; Boushey, R.P. Colorectal cancer epidemiology: Incidence, mortality, survival, and risk factors. Clin. Colon Rectal Surg. 2009, 22, 191–197. [Google Scholar] [CrossRef] [Green Version]
- De Jong, A.E.; Morreau, H.; Nagengast, F.M.; Mathus-Vliegen, E.M.; Kleibeuker, J.H.; Griffioen, G.; Cats, A.; Vasen, H.F. Prevalence of adenomas among young individuals at average risk for colorectal cancer. Off. J. Am. Coll. Gastroenterol. ACG 2005, 100, 139–143. [Google Scholar] [CrossRef]
- Davies, R.J.; Miller, R.; Coleman, N. Colorectal cancer screening: Prospects for molecular stool analysis. Nat. Rev. Cancer 2005, 5, 199–209. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2022; Available online: http://www.R-project.org/ (accessed on 28 April 2022).
- Kuhnle, G.G.; Bingham, S.A. Dietary meat, endogenous nitrosation and colorectal cancer. Biochem. Soc. Trans. 2007, 35, 1355–1357. [Google Scholar] [CrossRef] [PubMed]
- Van den Bussche, J.; Hemeryck, L.Y.; Van Hecke, T.; Kuhnle, G.G.; Pasmans, F.; Moore, S.A.; Van de Wiele, T.; De Smet, S.; Vanhaecke, L. O(6)-carboxymethylguanine DNA adduct formation and lipid peroxidation upon in vitro gastrointestinal digestion of haem-rich meat. Mol. Nutr. Food Res. 2014, 58, 1883–1896. [Google Scholar] [CrossRef] [PubMed]
- Willett, W.; Rockstrom, J.; Loken, B.; Springmann, M.; Lang, T.; Vermeulen, S.; Garnett, T.; Tilman, D.; DeClerck, F.; Wood, A.; et al. Food in the Anthropocene: The EAT-Lancet Commission on healthy diets from sustainable food systems. Lancet 2019, 393, 447–492. [Google Scholar] [CrossRef] [PubMed]
- Godfray, H.C.J.; Aveyard, P.; Garnett, T.; Hall, J.W.; Key, T.J.; Lorimer, J.; Pierrehumbert, R.T.; Scarborough, P.; Springmann, M.; Jebb, S.A. Meat consumption, health, and the environment. Science 2018, 361, eaam5324. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Vries, E.; Quintero, D.C.; Henriquez-Mendoza, G.; Herran, O.F. Population attributable fractions for colorectal cancer and red and processed meats in Colombia-a macro-simulation study. Colomb. Med. 2017, 48, 64–69. [Google Scholar]
- Lourenco, S.; Gunge, V.B.; Andersson, T.M.; Andersen, C.L.E.; Lund, A.Q.; Koster, B.; Hansen, G.L. Avoidable colorectal cancer cases in Denmark-The impact of red and processed meat. Cancer Epidemiol. 2018, 55, 1–7. [Google Scholar] [CrossRef]
- De Oliveira Mota, J.; Boue, G.; Guillou, S.; Pierre, F.; Membre, J.M. Estimation of the burden of disease attributable to red meat consumption in France: Influence on colorectal cancer and cardiovascular diseases. Food Chem. Toxicol. 2019, 130, 174–186. [Google Scholar] [CrossRef]
- Kim, D.D.; Wilde, P.E.; Michaud, D.S.; Liu, J.; Lizewski, L.; Onopa, J.; Mozaffarian, D.; Zhang, F.F.; Wong, J.B. Cost Effectiveness of Nutrition Policies on Processed Meat: Implications for Cancer Burden in the U.S. Am. J. Prev. Med. 2019, 57, e143–e152. [Google Scholar] [CrossRef]
- Ruan, Y.; Poirier, A.E.; Hebert, L.A.; Grevers, X.; Walter, S.D.; Villeneuve, P.J.; Brenner, D.R.; Friedenreich, C.M.; Com, P.S.T. Estimates of the current and future burden of cancer attributable to red and processed meat consumption in Canada. Prev. Med. 2019, 122, 31–39. [Google Scholar] [CrossRef]
- Gredner, T.; Niedermaier, T.; Brenner, H.; Mons, U. Impact of Tobacco Control Policies on Smoking-Related Cancer Incidence in Germany 2020 to 2050-A Simulation Study. Cancer Epidemiol. Biomark. Prev. 2020, 29, 1413–1422. [Google Scholar] [CrossRef]
- Gredner, T.; Niedermaier, T.; Brenner, H.; Mons, U. Impact of reducing alcohol consumption through price-based policies on cancer incidence in Germany 2020–2050—A simulation study. Addiction 2021, 116, 1677–1688. [Google Scholar] [CrossRef] [PubMed]
- Zhong, V.W.; Van Horn, L.; Greenland, P.; Carnethon, M.R.; Ning, H.; Wilkins, J.T.; Lloyd-Jones, D.M.; Allen, N.B. Associations of Processed Meat, Unprocessed Red Meat, Poultry, or Fish Intake With Incident Cardiovascular Disease and All-Cause Mortality. JAMA Intern. Med. 2020, 180, 503–512. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Lin, X.; Ouyang, Y.Y.; Liu, J.; Zhao, G.; Pan, A.; Hu, F.B. Red and processed meat consumption and mortality: Dose-response meta-analysis of prospective cohort studies. Public Health Nutr. 2016, 19, 893–905. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iqbal, R.; Dehghan, M.; Mente, A.; Rangarajan, S.; Wielgosz, A.; Avezum, A.; Seron, P.; AlHabib, K.F.; Lopez-Jaramillo, P.; Swaminathan, S.; et al. Associations of unprocessed and processed meat intake with mortality and cardiovascular disease in 21 countries [Prospective Urban Rural Epidemiology (PURE) Study]: A prospective cohort study. Am. J. Clin. Nutr. 2021, 114, 1049–1058. [Google Scholar] [CrossRef]
- International Agency for Research on Cancer. European Code Against Cancer—12 Ways to Reduce Your Cancer Risk. Available online: https://cancer-code-europe.iarc.fr/index.php/en/ (accessed on 25 May 2022).
- Schröck, R. Analyse der Preiselastizitäten der Nachfrage nach Biolebensmitteln unter Berücksichtigung Nicht Direkt Preisrelevanten Verhaltens der Verbraucher (Analysis of Price Elasticities for Organic Food Products in Consideration of Not Price-Related Consumer Behaviour); BÖLN-Bundesprogramm Ökologischer Landbau und Andere Formen Nachhaltiger Landwirtschaft: 2013. Available online: https://orgprints.org/id/eprint/22414/ (accessed on 25 April 2022).
- Volpp, K.G.; Asch, D.A. Make the healthy choice the easy choice: Using behavioral economics to advance a culture of health. QJM 2017, 110, 271–275. [Google Scholar] [CrossRef] [Green Version]
- Tran, K.B.; Lang, J.J.; Compton, K.; Xu, R.; Acheson, A.R.; Henrikson, H.J.; Kocarnik, J.M.; Penberthy, L.; Aali, A.; Abbas, Q.; et al. The global burden of cancer attributable to risk factors, 2010–19: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2022, 400, 563–591. [Google Scholar] [CrossRef]
- Ahrens, S. Fleischverbrauch in Deutschland pro Kopf in den Jahren 1991 bis 2020. Available online: https://de.statista.com/statistik/daten/studie/36573/umfrage/pro-kopf-verbrauch-von-fleisch-in-deutschland-seit-2000/ (accessed on 1 May 2022).
- Stintzing, S.; van Oostrum, I.; Pescott, C.P.; Ronga, P.; Heeg, B.; Heinemann, V. Cost-effectiveness of FOLFIRI + cetuximab vs FOLFIRI + bevacizumab in the first-line treatment of RAS wild-type metastatic colorectal cancer in Germany: Data from the FIRE-3 (AIO KRK-0306) study. J. Med. Econ. 2020, 23, 448–455. [Google Scholar] [CrossRef] [Green Version]
- Haug, U.; Engel, S.; Verheyen, F.; Linder, R. Estimating colorectal cancer treatment costs: A pragmatic approach exemplified by health insurance data from Germany. PLoS ONE 2014, 9, e88407. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Males | Females | Overall | 18–24 | 25–29 | 30–34 | 35–39 | 40–44 | 45–49 | 50–54 | 55–59 | 60–64 | 65–69 | 70–74 | 75–79 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Red meat intake | |||||||||||||||
| Minimum | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| 1st quartile | 11 | 11 | 11 | 11 | 11 | 11 | 13 | 11 | 11 | 11 | 11 | 11 | 11 | 11 | 11 |
| Median | 26 | 26 | 26 | 26 | 26 | 26 | 26 | 26 | 26 | 26 | 26 | 26 | 26 | 26 | 26 |
| Mean | 47 | 29 | 38 | 45 | 39 | 39 | 41 | 38 | 37 | 37 | 33 | 35 | 34 | 29 | 28 |
| 3rd quartile | 60 | 30 | 60 | 60 | 60 | 60 | 60 | 60 | 60 | 60 | 60 | 60 | 60 | 30 | 30 |
| 99th perc. | 240 | 120 | 189 | 240 | 240 | 240 | 240 | 120 | 120 | 120 | 120 | 120 | 120 | 120 | 120 |
| Processed meat intake | |||||||||||||||
| Minimum | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| 1st quartile | 24 | 11 | 16 | 19 | 16 | 18 | 19 | 17 | 17 | 17 | 17 | 14 | 14 | 15 | 12 |
| Median | 47 | 23 | 33 | 42 | 37 | 38 | 40 | 36 | 35 | 34 | 32 | 27 | 29 | 27 | 26 |
| Mean | 61 | 32 | 46 | 55 | 50 | 55 | 54 | 47 | 47 | 46 | 44 | 39 | 39 | 35 | 36 |
| 3rd quartile | 78 | 42 | 59 | 74 | 66 | 66 | 73 | 63 | 62 | 60 | 55 | 52 | 54 | 48 | 45 |
| 99th perc. | 242 | 169 | 220 | 239 | 199 | 219 | 244 | 213 | 236 | 199 | 511 | 169 | 172 | 147 | 171 |
| Red and processed meat intake | |||||||||||||||
| Minimum | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| 1st quartile | 54 | 28 | 37 | 41 | 35 | 39 | 44 | 40 | 41 | 40 | 37 | 36 | 35 | 35 | 32 |
| Median | 89 | 48 | 68 | 77 | 66 | 70 | 75 | 73 | 69 | 72 | 65 | 65 | 63 | 56 | 52 |
| Mean | 107 | 61 | 84 | 100 | 88 | 95 | 95 | 86 | 84 | 83 | 76 | 74 | 73 | 65 | 64 |
| 3rd quartile | 135 | 81 | 108 | 133 | 123 | 119 | 122 | 111 | 106 | 110 | 101 | 97 | 97 | 85 | 85 |
| 99th perc. | 415 | 233 | 340 | 478 | 410 | 341 | 378 | 309 | 356 | 323 | 275 | 231 | 278 | 203 | 235 |
| Expected Number of Cancer Cases in the Absence of Changes | Total (#) and Relative (%) Number of Prevented Colorectal Cancer Cases Per Scenario | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Sex Analysis | -1 Serving Red Meat Per Day | -2 Servings Red Meat Per Day | Elimination of Red Meat Intake | -1 Serving Processed Meat Per Day | -2 Servings Processed Meat Per Day | Elimination of Processed Meat Intake | |||||||
| # | % | # | % | # | % | # | % | # | % | # | % | ||
| Men | |||||||||||||
| Main analysis 1 | 1,208,329 | 10,890 | 0.9 | 19,292 | 1.6 | 39,178 | 3.2 | 28,633 | 2.4 | 60,721 | 5.0 | 145,291 | 12.0 |
| Lag time: 5 years | 11,718 | 1.0 | 20,763 | 1.7 | 42,183 | 3.5 | 30,809 | 2.5 | 65,334 | 5.4 | 156,403 | 12.9 | |
| Lag time: 15 years | 9611 | 0.8 | 17,019 | 1.4 | 34,541 | 2.9 | 25,268 | 2.1 | 53,586 | 4.4 | 128,182 | 10.6 | |
| Women | |||||||||||||
| Main analysis 1 | 939,932 | 7641 | 0.8 | 12,925 | 1.4 | 23,611 | 2.5 | 20,381 | 2.2 | 46,975 | 5.0 | 60,273 | 6.4 |
| Lag time: 5 years | 8224 | 0.9 | 13,927 | 1.5 | 25,446 | 2.7 | 21,960 | 2.3 | 50,607 | 5.4 | 64,978 | 6.9 | |
| Lag time: 15 years | 6732 | 0.7 | 11,387 | 1.2 | 20,800 | 2.2 | 17,989 | 1.9 | 41,401 | 4.4 | 53,073 | 5.6 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Niedermaier, T.; Gredner, T.; Hoffmeister, M.; Mons, U.; Brenner, H. Impact of Reducing Intake of Red and Processed Meat on Colorectal Cancer Incidence in Germany 2020 to 2050—A Simulation Study. Nutrients 2023, 15, 1020. https://doi.org/10.3390/nu15041020
Niedermaier T, Gredner T, Hoffmeister M, Mons U, Brenner H. Impact of Reducing Intake of Red and Processed Meat on Colorectal Cancer Incidence in Germany 2020 to 2050—A Simulation Study. Nutrients. 2023; 15(4):1020. https://doi.org/10.3390/nu15041020
Chicago/Turabian StyleNiedermaier, Tobias, Thomas Gredner, Michael Hoffmeister, Ute Mons, and Hermann Brenner. 2023. "Impact of Reducing Intake of Red and Processed Meat on Colorectal Cancer Incidence in Germany 2020 to 2050—A Simulation Study" Nutrients 15, no. 4: 1020. https://doi.org/10.3390/nu15041020