
Creatine Supplementation to Improve Sarcopenia in Chronic Liver Disease: Facts and Perspectives
 , and
, and 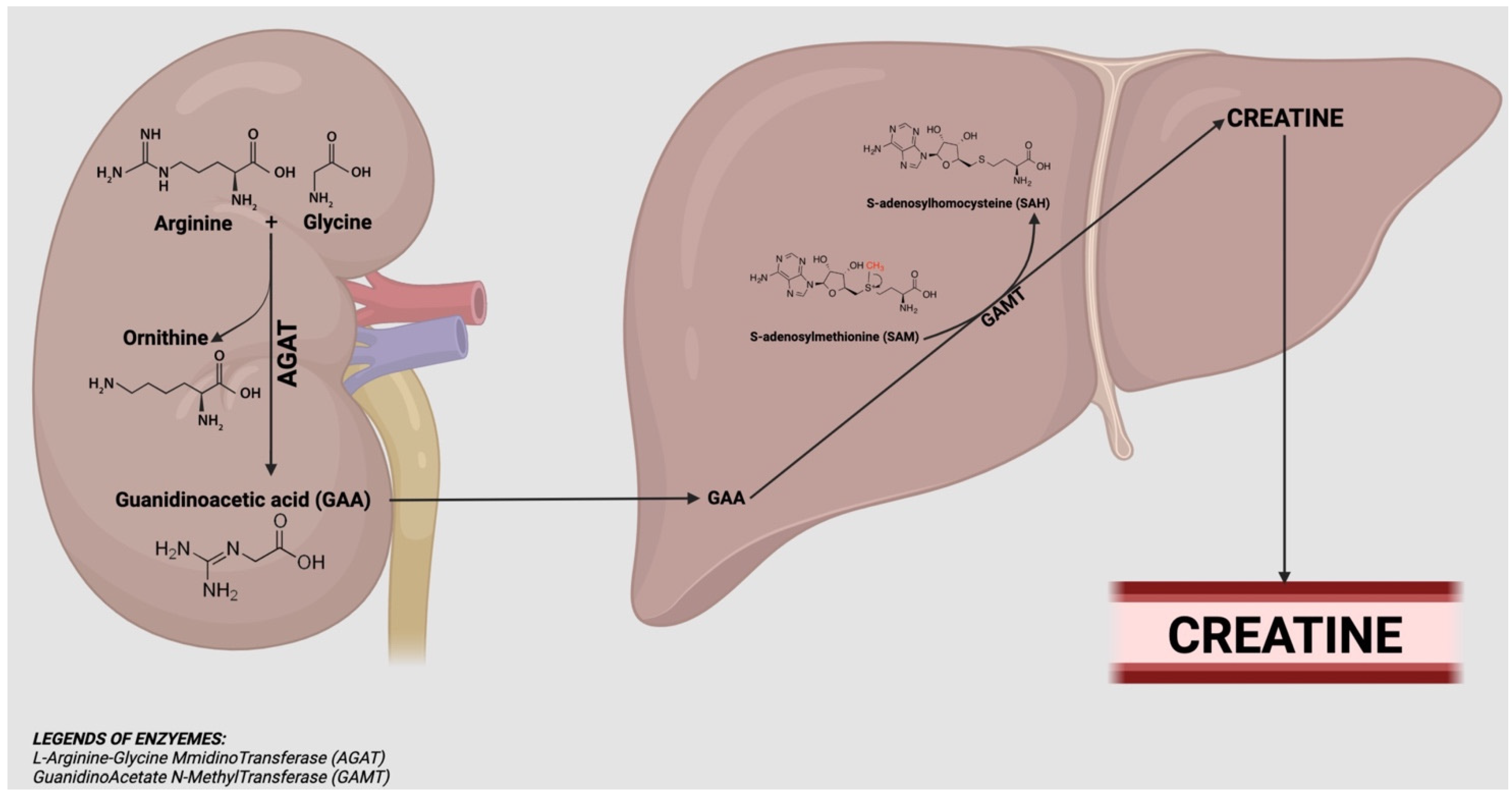{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Data Sources and Searches
3. Creatine: Instruction for Use
3.1. Definition
3.2. Biosynthesis and Metabolism
3.3. Dosage, Formulation and Method of Administration
3.4. Creatine Safety
4. Creatine: Role in Health and Disease
4.1. Creatine in Healthy Young and Elderly with and without Resistance Training
4.2. Creatine as a New Treatment for Improving Health and Quality of Life for Patients with Chronic Kidney Disease
4.3. Creatine in Other Disease Conditions
5. Creatine and Liver
5.1. Creatine and Chronic Liver Diseases
5.2. Creatine and Hyperammonaemia in Advanced Chronic Liver Disease
5.3. Creatine and Sarcopenia in Advanced Chronic Liver Disease
5.4. Rational for Creatine Supplementation in Advanced Chronic Liver Disease
6. Future Perspective of Creatine in Liver Diseases
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kreider, R.B.; Stout, J.R. Creatine in Health and Disease. Nutrients 2021, 13, 447. [Google Scholar] [CrossRef]
- Kreider, R.B.; Kalman, D.S.; Antonio, J.; Ziegenfuss, T.N.; Wildman, R.; Collins, R.; Candow, D.G.; Kleiner, S.M.; Almada, A.L.; Lopez, H.L. International Society of Sports Nutrition Position Stand: Safety and Efficacy of Creatine Supplementation in Exercise, Sport, and Medicine. J. Int. Soc. Sports Nutr. 2017, 14, 18. [Google Scholar] [CrossRef] [PubMed]
- Barcelos, R.P.; Stefanello, S.T.; Mauriz, J.L.; Gonzalez-Gallego, J.; Soares, F.A.A. Creatine and the Liver: Metabolism and Possible Interactions. MRMC 2015, 16, 12–18. [Google Scholar] [CrossRef] [PubMed]
- Cannataro, R.; Carbone, L.; Petro, J.L.; Cione, E.; Vargas, S.; Angulo, H.; Forero, D.A.; Odriozola-Martínez, A.; Kreider, R.B.; Bonilla, D.A. Sarcopenia: Etiology, Nutritional Approaches, and MiRNAs. IJMS 2021, 22, 9724. [Google Scholar] [CrossRef] [PubMed]
- Smith, R.N.; Agharkar, A.S.; Gonzales, E.B. A Review of Creatine Supplementation in Age-Related Diseases: More than a Supplement for Athletes. F1000Res 2014, 3, 222. [Google Scholar] [CrossRef]
- Joncquel-Chevalier Curt, M.; Voicu, P.-M.; Fontaine, M.; Dessein, A.-F.; Porchet, N.; Mention-Mulliez, K.; Dobbelaere, D.; Soto-Ares, G.; Cheillan, D.; Vamecq, J. Creatine Biosynthesis and Transport in Health and Disease. Biochimie 2015, 119, 146–165. [Google Scholar] [CrossRef]
- Lehninger, A.L.; Nelson, D.L.; Cox, M.M. Lehninger Principles of Biochemistry, 5th ed.; W.H. Freeman: New York, NY, USA, 2008; ISBN 978-0-7167-7108-1. [Google Scholar]
- Bonilla, D.A.; Kreider, R.B.; Stout, J.R.; Forero, D.A.; Kerksick, C.M.; Roberts, M.D.; Rawson, E.S. Metabolic Basis of Creatine in Health and Disease: A Bioinformatics-Assisted Review. Nutrients 2021, 13, 1238. [Google Scholar] [CrossRef]
- Candow, D.G.; Forbes, S.C.; Chilibeck, P.D.; Cornish, S.M.; Antonio, J.; Kreider, R.B. Effectiveness of Creatine Supplementation on Aging Muscle and Bone: Focus on Falls Prevention and Inflammation. JCM 2019, 8, 488. [Google Scholar] [CrossRef]
- Da Silva, R.P.; Nissim, I.; Brosnan, M.E.; Brosnan, J.T. Creatine Synthesis: Hepatic Metabolism of Guanidinoacetate and Creatine in the Rat in Vitro and in Vivo. Am. J. Physiol. Endocrinol. Metab. 2009, 296, E256–E261. [Google Scholar] [CrossRef]
- Askenasy, N.; Koretsky, A.P. Differential Effects of Creatine Kinase Isoenzymes and Substrates on Regeneration in Livers of Transgenic Mice. Am. J. Physiol. 1997, 273, C741–C746. [Google Scholar] [CrossRef]
- Alsever, R.N.; Georg, R.H.; Sussman, K.E. Stimulation of Insulin Secretion by Guanidinoacetic Acid and Other Guanidine Derivatives. Endocrinology 1970, 86, 332–336. [Google Scholar] [CrossRef]
- Ambrosio, G.; Zweier, J.L.; Flaherty, J.T. The Relationship between Oxygen Radical Generation and Impairment of Myocardial Energy Metabolism Following Post-Ischemic Reperfusion. J. Mol. Cell. Cardiol. 1991, 23, 1359–1374. [Google Scholar] [CrossRef]
- Kazak, L.; Cohen, P. Creatine Metabolism: Energy Homeostasis, Immunity and Cancer Biology. Nat. Rev. Endocrinol. 2020, 16, 421–436. [Google Scholar] [CrossRef]
- Santacruz, L.; Jacobs, D.O. Structural Correlates of the Creatine Transporter Function Regulation: The Undiscovered Country. Amino Acids 2016, 48, 2049–2055. [Google Scholar] [CrossRef]
- Schulze, A. Creatine Deficiency Syndromes. Handb. Clin. Neurol. 2013, 113, 1837–1843. [Google Scholar] [CrossRef]
- Wallimann, T.; Riek, U.; Möddel, M. Intradialytic Creatine Supplementation: A Scientific Rationale for Improving the Health and Quality of Life of Dialysis Patients. Med. Hypotheses 2017, 99, 1–14. [Google Scholar] [CrossRef]
- Antonio, J.; Candow, D.G.; Forbes, S.C.; Gualano, B.; Jagim, A.R.; Kreider, R.B.; Rawson, E.S.; Smith-Ryan, A.E.; VanDusseldorp, T.A.; Willoughby, D.S.; et al. Common Questions and Misconceptions about Creatine Supplementation: What Does the Scientific Evidence Really Show? J. Int. Soc. Sports Nutr. 2021, 18, 13. [Google Scholar] [CrossRef]
- Ostojic, S.M.; Ahmetovic, Z. Gastrointestinal Distress after Creatine Supplementation in Athletes: Are Side Effects Dose Dependent? Res. Sports Med. 2008, 16, 15–22. [Google Scholar] [CrossRef]
- Kreider, R.B.; Melton, C.; Rasmussen, C.J.; Greenwood, M.; Lancaster, S.; Cantler, E.C.; Milnor, P.; Almada, A.L. Long-Term Creatine Supplementation Does Not Significantly Affect Clinical Markers of Health in Athletes. Mol. Cell Biochem. 2003, 244, 95–104. [Google Scholar] [CrossRef]
- Antonio, J. International Society of Sport Nutrition. Essentials of Sports Nutrition and Supplements; Humana Press: Totowa, NJ, USA, 2008; ISBN 978-1-58829-611-5. [Google Scholar]
- Steenge, G.R.; Lambourne, J.; Casey, A.; Macdonald, I.A.; Greenhaff, P.L. Stimulatory Effect of Insulin on Creatine Accumulation in Human Skeletal Muscle. Am. J. Physiol. Endocrinol. Metab. 1998, 275, E974–E979. [Google Scholar] [CrossRef]
- Powers, M.E.; Arnold, B.L.; Weltman, A.L.; Perrin, D.H.; Mistry, D.; Kahler, D.M.; Kraemer, W.; Volek, J. Creatine Supplementation Increases Total Body Water Without Altering Fluid Distribution. J. Athl. Train. 2003, 38, 44–50. [Google Scholar] [PubMed]
- Bender, A.; Klopstock, T. Creatine for Neuroprotection in Neurodegenerative Disease: End of Story? Amino Acids 2016, 48, 1929–1940. [Google Scholar] [CrossRef] [PubMed]
- Klivenyi, P.; Ferrante, R.J.; Matthews, R.T.; Bogdanov, M.B.; Klein, A.M.; Andreassen, O.A.; Mueller, G.; Wermer, M.; Kaddurah-Daouk, R.; Beal, M.F. Neuroprotective Effects of Creatine in a Transgenic Animal Model of Amyotrophic Lateral Sclerosis. Nat. Med. 1999, 5, 347–350. [Google Scholar] [CrossRef] [PubMed]
- Matthews, R.T.; Yang, L.; Jenkins, B.G.; Ferrante, R.J.; Rosen, B.R.; Kaddurah-Daouk, R.; Beal, M.F. Neuroprotective Effects of Creatine and Cyclocreatine in Animal Models of Huntington’s Disease. J. Neurosci. 1998, 18, 156–163. [Google Scholar] [CrossRef] [PubMed]
- Araújo, M.B.; Moura, L.P.; Junior, R.C.V.; Junior, M.C.; Dalia, R.A.; Sponton, A.C.; Ribeiro, C.; Mello, M.A.R. Creatine Supplementation and Oxidative Stress in Rat Liver. J. Int. Soc. Sports. Nutr. 2013, 10, 54. [Google Scholar] [CrossRef]
- Stefani, G.P.; Nunes, R.B.; Dornelles, A.Z.; Alves, J.P.; Piva, M.O.; Domenico, M.D.; Rhoden, C.R.; Lago, P.D. Effects of Creatine Supplementation Associated with Resistance Training on Oxidative Stress in Different Tissues of Rats. J. Int. Soc. Sports Nutr. 2014, 11, 11. [Google Scholar] [CrossRef]
- Souza, W.M.; Heck, T.G.; Wronski, E.C.; Ulbrich, A.Z.; Boff, E. Effects of Creatine Supplementation on Biomarkers of Hepatic and Renal Function in Young Trained Rats. Toxicol. Mech. Methods 2013, 23, 697–701. [Google Scholar] [CrossRef]
- Aljobaily, N.; Viereckl, M.J.; Hydock, D.S.; Aljobaily, H.; Wu, T.-Y.; Busekrus, R.; Jones, B.; Alberson, J.; Han, Y. Creatine Alleviates Doxorubicin-Induced Liver Damage by Inhibiting Liver Fibrosis, Inflammation, Oxidative Stress, and Cellular Senescence. Nutrients 2020, 13, 41. [Google Scholar] [CrossRef]
- Marinello, P.C.; Cella, P.S.; Testa, M.T.J.; Guirro, P.B.; Brito, W.A.S.; Borges, F.H.; Cecchini, R.; Cecchini, A.L.; Duarte, J.A.; Deminice, R. Creatine Supplementation Exacerbates Ethanol-Induced Hepatic Damage in Mice. Nutrition 2019, 66, 122–130. [Google Scholar] [CrossRef]
- Farquhar, W.B.; Zambraski, E.J. Effects of Creatine Use on the Athlete’s Kidney. Curr. Sports Med. Rep. 2002, 1, 103–106. [Google Scholar] [CrossRef]
- Twycross-Lewis, R.; Kilduff, L.P.; Wang, G.; Pitsiladis, Y.P. The Effects of Creatine Supplementation on Thermoregulation and Physical (Cognitive) Performance: A Review and Future Prospects. Amino Acids 2016, 48, 1843–1855. [Google Scholar] [CrossRef]
- Stares, A.; Bains, M. The Additive Effects of Creatine Supplementation and Exercise Training in an Aging Population: A Systematic Review of Randomized Controlled Trials. J. Geriatr. Phys. Ther. 2020, 43, 99–112. [Google Scholar] [CrossRef]
- Forbes, S.C.; Candow, D.G.; Ostojic, S.M.; Roberts, M.D.; Chilibeck, P.D. Meta-Analysis Examining the Importance of Creatine Ingestion Strategies on Lean Tissue Mass and Strength in Older Adults. Nutrients 2021, 13, 1912. [Google Scholar] [CrossRef]
- Moon, A.; Heywood, L.; Rutherford, S.; Cobbold, C. Creatine Supplementation: Can It Improve Quality of Life in the Elderly without Associated Resistance Training? Curr. Aging Sci. 2013, 6, 251–257. [Google Scholar] [CrossRef]
- Stout, J.R.; Sue Graves, B.; Cramer, J.T.; Goldstein, E.R.; Costa, P.B.; Smith, A.E.; Walter, A.A. Effects of Creatine Supplementation on the Onset of Neuromuscular Fatigue Threshold and Muscle Strength in Elderly Men and Women (64–86 Years). J. Nutr. Health Aging 2007, 11, 459–464. [Google Scholar]
- Rawson, E.S.; Wehnert, M.L.; Clarkson, P.M. Effects of 30 Days of Creatine Ingestion in Older Men. Eur. J. Appl. Physiol. Occup. Physiol. 1999, 80, 139–144. [Google Scholar] [CrossRef]
- Gotshalk, L.A.; Volek, J.S.; Staron, R.S.; Denegar, C.R.; Hagerman, F.C.; Kraemer, W.J. Creatine Supplementation Improves Muscular Performance in Older Men. Med. Sci. Sports Exerc. 2002, 34, 537–543. [Google Scholar] [CrossRef]
- Gotshalk, L.A.; Kraemer, W.J.; Mendonca, M.A.G.; Vingren, J.L.; Kenny, A.M.; Spiering, B.A.; Hatfield, D.L.; Fragala, M.S.; Volek, J.S. Creatine Supplementation Improves Muscular Performance in Older Women. Eur. J. Appl. Physiol. 2008, 102, 223–231. [Google Scholar] [CrossRef]
- Chami, J.; Candow, D.G. Effect of Creatine Supplementation Dosing Strategies on Aging Muscle Performance. J. Nutr. Health Aging 2019, 23, 281–285. [Google Scholar] [CrossRef]
- Lobo, D.M.; Tritto, A.C.; da Silva, L.R.; de Oliveira, P.B.; Benatti, F.B.; Roschel, H.; Nieß, B.; Gualano, B.; Pereira, R.M.R. Effects of Long-Term Low-Dose Dietary Creatine Supplementation in Older Women. Exp. Gerontol. 2015, 70, 97–104. [Google Scholar] [CrossRef]
- Baker, T.P.; Candow, D.G.; Farthing, J.P. Effect of Preexercise Creatine Ingestion on Muscle Performance in Healthy Aging Males. J. Strength Cond. Res. 2016, 30, 1763–1766. [Google Scholar] [CrossRef] [PubMed]
- Cañete, S.; San Juan, A.F.; Pérez, M.; Gómez-Gallego, F.; López-Mojares, L.M.; Earnest, C.P.; Fleck, S.J.; Lucia, A. Does Creatine Supplementation Improve Functional Capacity in Elderly Women? J. Strength Cond. Res. 2006, 20, 22–28. [Google Scholar] [CrossRef] [PubMed]
- Rawson, E.S.; Clarkson, P.M. Acute Creatine Supplementation in Older Men. Int. J. Sports Med. 2000, 21, 71–75. [Google Scholar] [CrossRef] [PubMed]
- Bermon, S.; Venembre, P.; Sachet, C.; Valour, S.; Dolisi, C. Effects of Creatine Monohydrate Ingestion in Sedentary and Weight-Trained Older Adults. Acta Physiol. Scand. 1998, 164, 147–155. [Google Scholar] [CrossRef]
- De Deyn, P.P.; Marescau, B.; Swartz, R.D.; Hogaerth, R.; Possemiers, I.; Lowenthal, A. Serum Guanidino Compound Levels and Clearances in Uremic Patients Treated with Continuous Ambulatory Peritoneal Dialysis. Nephron 1990, 54, 307–312. [Google Scholar] [CrossRef] [PubMed]
- Dolder, M.; Walzel, B.; Speer, O.; Schlattner, U.; Wallimann, T. Inhibition of the Mitochondrial Permeability Transition by Creatine Kinase Substrates. Requirement for Microcompartmentation. J. Biol. Chem. 2003, 278, 17760–17766. [Google Scholar] [CrossRef]
- Caretti, A.; Bianciardi, P.; Sala, G.; Terruzzi, C.; Lucchina, F.; Samaja, M. Supplementation of Creatine and Ribose Prevents Apoptosis in Ischemic Cardiomyocytes. Cell Physiol. Biochem. 2010, 26, 831–838. [Google Scholar] [CrossRef]
- Gualano, B.; Novaes, R.B.; Artioli, G.G.; Freire, T.O.; Coelho, D.F.; Scagliusi, F.B.; Rogeri, P.S.; Roschel, H.; Ugrinowitsch, C.; Lancha, A.H. Effects of Creatine Supplementation on Glucose Tolerance and Insulin Sensitivity in Sedentary Healthy Males Undergoing Aerobic Training. Amino Acids 2008, 34, 245–250. [Google Scholar] [CrossRef]
- Gualano, B.; DE Salles Painneli, V.; Roschel, H.; Artioli, G.G.; Neves, M.; De Sá Pinto, A.L.; Da Silva, M.E.R.; Cunha, M.R.; Otaduy, M.C.G.; Leite, C.D.C.; et al. Creatine in Type 2 Diabetes: A Randomized, Double-Blind, Placebo-Controlled Trial. Med. Sci. Sports Exerc. 2011, 43, 770–778. [Google Scholar] [CrossRef]
- Deminice, R.; de Castro, G.S.; Brosnan, M.E.; Brosnan, J.T. Creatine Supplementation as a Possible New Therapeutic Approach for Fatty Liver Disease: Early Findings. Amino Acids 2016, 48, 1983–1991. [Google Scholar] [CrossRef]
- Earnest, C.P.; Almada, A.L.; Mitchell, T.L. High-Performance Capillary Electrophoresis-Pure Creatine Monohydrate Reduces Blood Lipids in Men and Women. Clin. Sci. 1996, 91, 113–118. [Google Scholar] [CrossRef]
- Riesberg, L.A.; Weed, S.A.; McDonald, T.L.; Eckerson, J.M.; Drescher, K.M. Beyond Muscles: The Untapped Potential of Creatine. Int. Immunopharmacol. 2016, 37, 31–42. [Google Scholar] [CrossRef]
- Glover, L.E.; Bowers, B.E.; Saeedi, B.; Ehrentraut, S.F.; Campbell, E.L.; Bayless, A.J.; Dobrinskikh, E.; Kendrick, A.A.; Kelly, C.J.; Burgess, A.; et al. Control of Creatine Metabolism by HIF Is an Endogenous Mechanism of Barrier Regulation in Colitis. Proc. Natl. Acad. Sci. USA 2013, 110, 19820–19825. [Google Scholar] [CrossRef]
- Jakobi, J.M.; Rice, C.L.; Curtin, S.V.; Marsh, G.D. Neuromuscular Properties and Fatigue in Older Men Following Acute Creatine Supplementation. Eur. J. Appl. Physiol. 2001, 84, 321–328. [Google Scholar] [CrossRef]
- Rae, C.; Digney, A.L.; McEwan, S.R.; Bates, T.C. Oral Creatine Monohydrate Supplementation Improves Brain Performance: A Double-Blind, Placebo-Controlled, Cross-over Trial. Proc. Biol. Sci. 2003, 270, 2147–2150. [Google Scholar] [CrossRef]
- McMorris, T.; Mielcarz, G.; Harris, R.C.; Swain, J.P.; Howard, A. Creatine Supplementation and Cognitive Performance in Elderly Individuals. Neuropsychol. Dev. Cogn. B Aging Neuropsychol. Cogn. 2007, 14, 517–528. [Google Scholar] [CrossRef]
- McMorris, T.; Harris, R.C.; Howard, A.N.; Langridge, G.; Hall, B.; Corbett, J.; Dicks, M.; Hodgson, C. Creatine Supplementation, Sleep Deprivation, Cortisol, Melatonin and Behavior. Physiol. Behav. 2007, 90, 21–28. [Google Scholar] [CrossRef]
- Deminice, R.; de Castro, G.S.F.; Francisco, L.V.; da Silva, L.E.C.M.; Cardoso, J.F.R.; Frajacomo, F.T.T.; Teodoro, B.G.; Dos Reis Silveira, L.; Jordao, A.A. Creatine Supplementation Prevents Fatty Liver in Rats Fed Choline-Deficient Diet: A Burden of One-Carbon and Fatty Acid Metabolism. J. Nutr. Biochem. 2015, 26, 391–397. [Google Scholar] [CrossRef]
- Deminice, R.; da Silva, R.P.; Lamarre, S.G.; Brown, C.; Furey, G.N.; McCarter, S.A.; Jordao, A.A.; Kelly, K.B.; King-Jones, K.; Jacobs, R.L.; et al. Creatine Supplementation Prevents the Accumulation of Fat in the Livers of Rats Fed a High-Fat Diet. J. Nutr. 2011, 141, 1799–1804. [Google Scholar] [CrossRef]
- Wyss, M.; Schulze, A. Health Implications of Creatine: Can Oral Creatine Supplementation Protect against Neurological and Atherosclerotic Disease? Neuroscience 2002, 112, 243–260. [Google Scholar] [CrossRef]
- Da Silva, R.P.; Leonard, K.-A.; Jacobs, R.L. Dietary Creatine Supplementation Lowers Hepatic Triacylglycerol by Increasing Lipoprotein Secretion in Rats Fed High-Fat Diet. J. Nutr. Biochem. 2017, 50, 46–53. [Google Scholar] [CrossRef] [PubMed]
- Ganesan, M.; Feng, D.; Barton, R.W.; Thomes, P.G.; McVicker, B.L.; Tuma, D.J.; Osna, N.A.; Kharbanda, K.K. Creatine Supplementation Does Not Prevent the Development of Alcoholic Steatosis. Alcohol. Clin. Exp. Res. 2016, 40, 2312–2319. [Google Scholar] [CrossRef] [PubMed]
- Kharbanda, K.K.; Todero, S.L.; Moats, J.C.; Harris, R.M.; Osna, N.A.; Thomes, P.G.; Tuma, D.J. Alcohol Consumption Decreases Rat Hepatic Creatine Biosynthesis via Altered Guanidinoacetate Methyltransferase Activity. Alcohol. Clin. Exp. Res. 2014, 38, 641–648. [Google Scholar] [CrossRef] [PubMed]
- Braissant, O.; Henry, H.; Villard, A.-M.; Zurich, M.-G.; Loup, M.; Eilers, B.; Parlascino, G.; Matter, E.; Boulat, O.; Honegger, P.; et al. Ammonium-Induced Impairment of Axonal Growth Is Prevented through Glial Creatine. J. Neurosci. 2002, 22, 9810–9820. [Google Scholar] [CrossRef] [PubMed]
- Xu, S.; Zhu, W.; Wan, Y.; Wang, J.; Chen, X.; Pi, L.; Lobo, M.K.; Ren, B.; Ying, Z.; Morris, M.; et al. Decreased Taurine and Creatine in the Thalamus May Relate to Behavioral Impairments in Ethanol-Fed Mice: A Pilot Study of Proton Magnetic Resonance Spectroscopy. Mol. Imaging 2018, 17, 1536012117749051. [Google Scholar] [CrossRef]
- Wallimann, T.; Wyss, M.; Brdiczka, D.; Nicolay, K.; Eppenberger, H.M. Intracellular Compartmentation, Structure and Function of Creatine Kinase Isoenzymes in Tissues with High and Fluctuating Energy Demands: The “phosphocreatine Circuit” for Cellular Energy Homeostasis. Biochem. J. 1992, 281, 21–40. [Google Scholar] [CrossRef]
- Greenhaff, P.L.; Casey, A.; Short, A.H.; Harris, R.; Soderlund, K.; Hultman, E. Influence of Oral Creatine Supplementation of Muscle Torque during Repeated Bouts of Maximal Voluntary Exercise in Man. Clin. Sci. 1993, 84, 565–571. [Google Scholar] [CrossRef]
- Deminice, R.; Portari, G.V.; Vannucchi, H.; Jordao, A.A. Effects of Creatine Supplementation on Homocysteine Levels and Lipid Peroxidation in Rats. Br. J. Nutr. 2009, 102, 110–116. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European Consensus on Definition and Diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef]
- Ebadi, M.; Bhanji, R.A.; Mazurak, V.C.; Montano-Loza, A.J. Sarcopenia in Cirrhosis: From Pathogenesis to Interventions. J. Gastroenterol. 2019, 54, 845–859. [Google Scholar] [CrossRef]
- DiMartini, A.; Cruz, R.J.; Dew, M.A.; Myaskovsky, L.; Goodpaster, B.; Fox, K.; Kim, K.H.; Fontes, P. Muscle Mass Predicts Outcomes Following Liver Transplantation. Liver Transpl. 2013, 19, 1172–1180. [Google Scholar] [CrossRef] [Green Version]
- Montano-Loza, A.J.; Duarte-Rojo, A.; Meza-Junco, J.; Baracos, V.E.; Sawyer, M.B.; Pang, J.X.Q.; Beaumont, C.; Esfandiari, N.; Myers, R.P. Inclusion of Sarcopenia Within MELD (MELD-Sarcopenia) and the Prediction of Mortality in Patients With Cirrhosis. Clin. Transl. Gastroenterol. 2015, 6, e102. [Google Scholar] [CrossRef]
- Durand, F.; Buyse, S.; Francoz, C.; Laouénan, C.; Bruno, O.; Belghiti, J.; Moreau, R.; Vilgrain, V.; Valla, D. Prognostic Value of Muscle Atrophy in Cirrhosis Using Psoas Muscle Thickness on Computed Tomography. J. Hepatol. 2014, 60, 1151–1157. [Google Scholar] [CrossRef]
- Kaido, T.; Ogawa, K.; Fujimoto, Y.; Ogura, Y.; Hata, K.; Ito, T.; Tomiyama, K.; Yagi, S.; Mori, A.; Uemoto, S. Impact of Sarcopenia on Survival in Patients Undergoing Living Donor Liver Transplantation. Am. J. Transpl. 2013, 13, 1549–1556. [Google Scholar] [CrossRef]
- Masuda, T.; Shirabe, K.; Ikegami, T.; Harimoto, N.; Yoshizumi, T.; Soejima, Y.; Uchiyama, H.; Ikeda, T.; Baba, H.; Maehara, Y. Sarcopenia Is a Prognostic Factor in Living Donor Liver Transplantation. Liver Transpl. 2014, 20, 401–407. [Google Scholar] [CrossRef]
- Montano-Loza, A.J.; Meza-Junco, J.; Baracos, V.E.; Prado, C.M.M.; Ma, M.; Meeberg, G.; Beaumont, C.; Tandon, P.; Esfandiari, N.; Sawyer, M.B.; et al. Severe Muscle Depletion Predicts Postoperative Length of Stay but Is Not Associated with Survival after Liver Transplantation. Liver Transpl. 2014, 20, 640–648. [Google Scholar] [CrossRef]
- Krell, R.W.; Kaul, D.R.; Martin, A.R.; Englesbe, M.J.; Sonnenday, C.J.; Cai, S.; Malani, P.N. Association between Sarcopenia and the Risk of Serious Infection among Adults Undergoing Liver Transplantation. Liver Transpl. 2013, 19, 1396–1402. [Google Scholar] [CrossRef]
- Norman, K.; Kirchner, H.; Lochs, H.; Pirlich, M. Malnutrition Affects Quality of Life in Gastroenterology Patients. World J. Gastroenterol. 2006, 12, 3380–3385. [Google Scholar] [CrossRef]
- Bhanji, R.A.; Moctezuma-Velazquez, C.; Duarte-Rojo, A.; Ebadi, M.; Ghosh, S.; Rose, C.; Montano-Loza, A.J. Myosteatosis and Sarcopenia Are Associated with Hepatic Encephalopathy in Patients with Cirrhosis. Hepatol. Int. 2018, 12, 377–386. [Google Scholar] [CrossRef]
- van Vugt, J.L.A.; Buettner, S.; Alferink, L.J.M.; Bossche, N.; de Bruin, R.W.F.; Darwish Murad, S.; Polak, W.G.; Metselaar, H.J.; IJzermans, J.N.M. Low Skeletal Muscle Mass is Associated with Increased Hospital Costs in Patients with Cirrhosis Listed for Liver Transplantation-a Retrospective Study. Transpl. Int. 2018, 31, 165–174. [Google Scholar] [CrossRef]
- Ha, Y.; Kim, D.; Han, S.; Chon, Y.E.; Lee, Y.B.; Kim, M.N.; Lee, J.H.; Park, H.; Rim, K.S.; Hwang, S.G. Sarcopenia Predicts Prognosis in Patients with Newly Diagnosed Hepatocellular Carcinoma, Independent of Tumor Stage and Liver Function. Cancer Res. Treat. 2018, 50, 843–851. [Google Scholar] [CrossRef] [PubMed]
- Marasco, G.; Dajti, E.; Ravaioli, F.; Brocchi, S.; Rossini, B.; Alemanni, L.V.; Peta, G.; Bartalena, L.; Golfieri, R.; Festi, D.; et al. Clinical Impact of Sarcopenia Assessment in Patients with Liver Cirrhosis. Expert. Rev. Gastroenterol. Hepatol. 2021, 15, 377–388. [Google Scholar] [CrossRef] [PubMed]
- Marasco, G.; Dajti, E.; Serenari, M.; Alemanni, L.V.; Ravaioli, F.; Ravaioli, M.; Vestito, A.; Vara, G.; Festi, D.; Golfieri, R.; et al. Sarcopenia Predicts Major Complications after Resection for Primary Hepatocellular Carcinoma in Compensated Cirrhosis. Cancers 2022, 14, 1935. [Google Scholar] [CrossRef] [PubMed]
- Marasco, G.; Serenari, M.; Renzulli, M.; Alemanni, L.V.; Rossini, B.; Pettinari, I.; Dajti, E.; Ravaioli, F.; Golfieri, R.; Cescon, M.; et al. Clinical Impact of Sarcopenia Assessment in Patients with Hepatocellular Carcinoma Undergoing Treatments. J. Gastroenterol. 2020, 55, 927–943. [Google Scholar] [CrossRef] [PubMed]
- Dajti, E.; Renzulli, M.; Ravaioli, F.; Marasco, G.; Vara, G.; Brandi, N.; Rossini, B.; Colecchia, L.; Alemanni, L.V.; Ferrarese, A.; et al. The Interplay between Sarcopenia and Portal Hypertension Predicts Ascites and Mortality in Cirrhosis. Dig. Liver Dis. 2022, S1590-8658(22)00789-7. [Google Scholar] [CrossRef]
- Dolz, C.; Raurich, J.M.; Ibáñez, J.; Obrador, A.; Marsé, P.; Gayá, J. Ascites Increases the Resting Energy Expenditure in Liver Cirrhosis. Gastroenterology 1991, 100, 738–744. [Google Scholar] [CrossRef]
- Hayashi, F.; Matsumoto, Y.; Momoki, C.; Yuikawa, M.; Okada, G.; Hamakawa, E.; Kawamura, E.; Hagihara, A.; Toyama, M.; Fujii, H.; et al. Physical Inactivity and Insufficient Dietary Intake Are Associated with the Frequency of Sarcopenia in Patients with Compensated Viral Liver Cirrhosis. Hepatol. Res. 2013, 43, 1264–1275. [Google Scholar] [CrossRef]
- Chang, W.K.; Chao, Y.C.; Tang, H.S.; Lang, H.F.; Hsu, C.T. Effects of Extra-Carbohydrate Supplementation in the Late Evening on Energy Expenditure and Substrate Oxidation in Patients with Liver Cirrhosis. JPEN J. Parenter Enteral. Nutr. 1997, 21, 96–99. [Google Scholar] [CrossRef]
- Davuluri, G.; Allawy, A.; Thapaliya, S.; Rennison, J.H.; Singh, D.; Kumar, A.; Sandlers, Y.; Van Wagoner, D.R.; Flask, C.A.; Hoppel, C.; et al. Hyperammonaemia-Induced Skeletal Muscle Mitochondrial Dysfunction Results in Cataplerosis and Oxidative Stress. J. Physiol. 2016, 594, 7341–7360. [Google Scholar] [CrossRef]
- Dam, G.; Ott, P.; Aagaard, N.K.; Vilstrup, H. Branched-Chain Amino Acids and Muscle Ammonia Detoxification in Cirrhosis. Metab. Brain Dis. 2013, 28, 217–220. [Google Scholar] [CrossRef]
- Qiu, J.; Thapaliya, S.; Runkana, A.; Yang, Y.; Tsien, C.; Mohan, M.L.; Narayanan, A.; Eghtesad, B.; Mozdziak, P.E.; McDonald, C.; et al. Hyperammonemia in Cirrhosis Induces Transcriptional Regulation of Myostatin by an NF-ΚB-Mediated Mechanism. Proc. Natl. Acad. Sci. USA 2013, 110, 18162–18167. [Google Scholar] [CrossRef] [Green Version]
- Ábrigo, J.; Elorza, A.A.; Riedel, C.A.; Vilos, C.; Simon, F.; Cabrera, D.; Estrada, L.; Cabello-Verrugio, C. Role of Oxidative Stress as Key Regulator of Muscle Wasting during Cachexia. Oxid. Med. Cell Longev. 2018, 2018, 2063179. [Google Scholar] [CrossRef]
- Wang, Q.; McPherron, A.C. Myostatin Inhibition Induces Muscle Fibre Hypertrophy Prior to Satellite Cell Activation. J. Physiol. 2012, 590, 2151–2165. [Google Scholar] [CrossRef]
- Nishikawa, H.; Enomoto, H.; Ishii, A.; Iwata, Y.; Miyamoto, Y.; Ishii, N.; Yuri, Y.; Hasegawa, K.; Nakano, C.; Nishimura, T.; et al. Elevated Serum Myostatin Level Is Associated with Worse Survival in Patients with Liver Cirrhosis. J. Cachexia Sarcopenia Muscle 2017, 8, 915–925. [Google Scholar] [CrossRef]
- Lee, J.H.; Jun, H.-S. Role of Myokines in Regulating Skeletal Muscle Mass and Function. Front. Physiol. 2019, 10, 42. [Google Scholar] [CrossRef]
- Jacobsen, E.B.; Hamberg, O.; Quistorff, B.; Ott, P. Reduced Mitochondrial Adenosine Triphosphate Synthesis in Skeletal Muscle in Patients with Child-Pugh Class B and C Cirrhosis. Hepatology 2001, 34, 7–12. [Google Scholar] [CrossRef]
- Sestili, P.; Ambrogini, P.; Barbieri, E.; Sartini, S.; Fimognari, C.; Calcabrini, C.; Diaz, A.R.; Guescini, M.; Polidori, E.; Luchetti, F.; et al. New Insights into the Trophic and Cytoprotective Effects of Creatine in in Vitro and in Vivo Models of Cell Maturation. Amino Acids 2016, 48, 1897–1911. [Google Scholar] [CrossRef]
- Sestili, P.; Martinelli, C.; Colombo, E.; Barbieri, E.; Potenza, L.; Sartini, S.; Fimognari, C. Creatine as an Antioxidant. Amino Acids 2011, 40, 1385–1396. [Google Scholar] [CrossRef]
- Meyer, L.E.; Machado, L.B.; Santiago, A.P.S.A.; da-Silva, W.S.; De Felice, F.G.; Holub, O.; Oliveira, M.F.; Galina, A. Mitochondrial Creatine Kinase Activity Prevents Reactive Oxygen Species Generation: Antioxidant Role of Mitochondrial Kinase-Dependent ADP Re-Cycling Activity. J. Biol. Chem. 2006, 281, 37361–37371. [Google Scholar] [CrossRef]
- Kay, L.; Nicolay, K.; Wieringa, B.; Saks, V.; Wallimann, T. Direct Evidence for the Control of Mitochondrial Respiration by Mitochondrial Creatine Kinase in Oxidative Muscle Cells in Situ. J. Biol. Chem. 2000, 275, 6937–6944. [Google Scholar] [CrossRef]
- Farshidfar, F.; Pinder, M.A.; Myrie, S.B. Creatine Supplementation and Skeletal Muscle Metabolism for Building Muscle Mass- Review of the Potential Mechanisms of Action. Curr. Protein Pept. Sci. 2017, 18, 1273–1287. [Google Scholar] [CrossRef] [PubMed]
- Häussinger, D.; Lang, F.; Gerok, W. Regulation of Cell Function by the Cellular Hydration State. Am. J. Physiol. 1994, 267, E343–E355. [Google Scholar] [CrossRef] [PubMed]
- Häussinger, D. The Role of Cellular Hydration in the Regulation of Cell Function. Biochem. J. 1996, 313, 697–710. [Google Scholar] [CrossRef] [PubMed]
- VAN Cutsem, J.; Roelands, B.; Pluym, B.; Tassignon, B.; Verschueren, J.O.; DE Pauw, K.; Meeusen, R. Can Creatine Combat the Mental Fatigue-Associated Decrease in Visuomotor Skills? Med. Sci. Sports Exerc. 2020, 52, 120–130. [Google Scholar] [CrossRef]
- Avgerinos, K.I.; Spyrou, N.; Bougioukas, K.I.; Kapogiannis, D. Effects of Creatine Supplementation on Cognitive Function of Healthy Individuals: A Systematic Review of Randomized Controlled Trials. Exp. Gerontol. 2018, 108, 166–173. [Google Scholar] [CrossRef]
- Benton, D.; Donohoe, R. The Influence of Creatine Supplementation on the Cognitive Functioning of Vegetarians and Omnivores. Br. J. Nutr. 2011, 105, 1100–1105. [Google Scholar] [CrossRef]
- Satoh, S.; Tanaka, A.; Hatano, E.; Inomoto, T.; Iwata, S.; Kitai, T.; Shinohara, H.; Tsunekawa, S.; Chance, B.; Yamaoka, Y. Energy Metabolism and Regeneration in Transgenic Mouse Liver Expressing Creatine Kinase after Major Hepatectomy. Gastroenterology 1996, 110, 1166–1174. [Google Scholar] [CrossRef]
- Kanazawa, A.; Tanaka, A.; Iwata, S.; Satoh, S.; Hatano, E.; Shinohara, H.; Kitai, T.; Tsunekawa, S.; Ikai, I.; Yamamoto, M.; et al. The Beneficial Effect of Phosphocreatine Accumulation in the Creatine Kinase Transgenic Mouse Liver in Endotoxin-Induced Hepatic Cell Death. J. Surg. Res. 1998, 80, 229–235. [Google Scholar] [CrossRef] [Green Version]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Casciola, R.; Leoni, L.; Cuffari, B.; Pecchini, M.; Menozzi, R.; Colecchia, A.; Ravaioli, F. Creatine Supplementation to Improve Sarcopenia in Chronic Liver Disease: Facts and Perspectives. Nutrients 2023, 15, 863. https://doi.org/10.3390/nu15040863
Casciola R, Leoni L, Cuffari B, Pecchini M, Menozzi R, Colecchia A, Ravaioli F. Creatine Supplementation to Improve Sarcopenia in Chronic Liver Disease: Facts and Perspectives. Nutrients. 2023; 15(4):863. https://doi.org/10.3390/nu15040863
Chicago/Turabian StyleCasciola, Riccardo, Laura Leoni, Biagio Cuffari, Maddalena Pecchini, Renata Menozzi, Antonio Colecchia, and Federico Ravaioli. 2023. "Creatine Supplementation to Improve Sarcopenia in Chronic Liver Disease: Facts and Perspectives" Nutrients 15, no. 4: 863. https://doi.org/10.3390/nu15040863