
Dietary Habits and Lifestyle, Including Cardiovascular Risk among Vegetarians and Omnivores during the COVID-19 Pandemic in the Polish Population


Abstract
:1. Introduction
2. Materials and Methods
2.1. Diet and Lifestyle Behaviours Questionnaire
- Primary data of respondents/socio-demographic data (number of questions = 9 for OMN, 11 for VEGE, the difference is due to additional questions about a vegetarian diet).
- Information on cardiovascular risk factors (number of questions = 16).
- Changes caused by the epidemic situation, taking into account the quality of life (number of questions = 13).
- Changes in eating habits during the pandemic (number of questions = 19 for OMN and 18 for VEGE (the difference is due to an additional question about meat consumption in the OMN group)).
2.2. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Cardiovascular Risk Factors of the Respondents
3.3. Changes in Diets and Quality of Life Caused by the Epidemic Situation
3.3.1. Quality Life Change
- “I feel bad because of the need to isolate and maintain social distancing.”
- “Powerlessness, helplessness.”
- “Anger.”
- The highest number of responses was obtained for “the level of physical activity was at an average level, and during the pandemic, physical activity decreased” (22.7% OMN vs. 20.2% VEGE).
- The answer “the level of physical activity was at an average level and remained at this level” was indicated by 18.4% of OMN vs. 18.8% VEGE.
- The answer “the level of physical activity was at a low level and remained so” was chosen by 20% of people on a mixed diet and 18.5% of vegetarians.
- “I sleep longer”—29% OMN vs. 30.1% VEGE.
- “I wake up later”—22% OMN vs. 18% VEGE.
- “I go to sleep later”—21.1% OMN vs. 16.7% VEGE.
- “I go to bed at less regular times”—18% OMN vs. 16.1% VEGE.
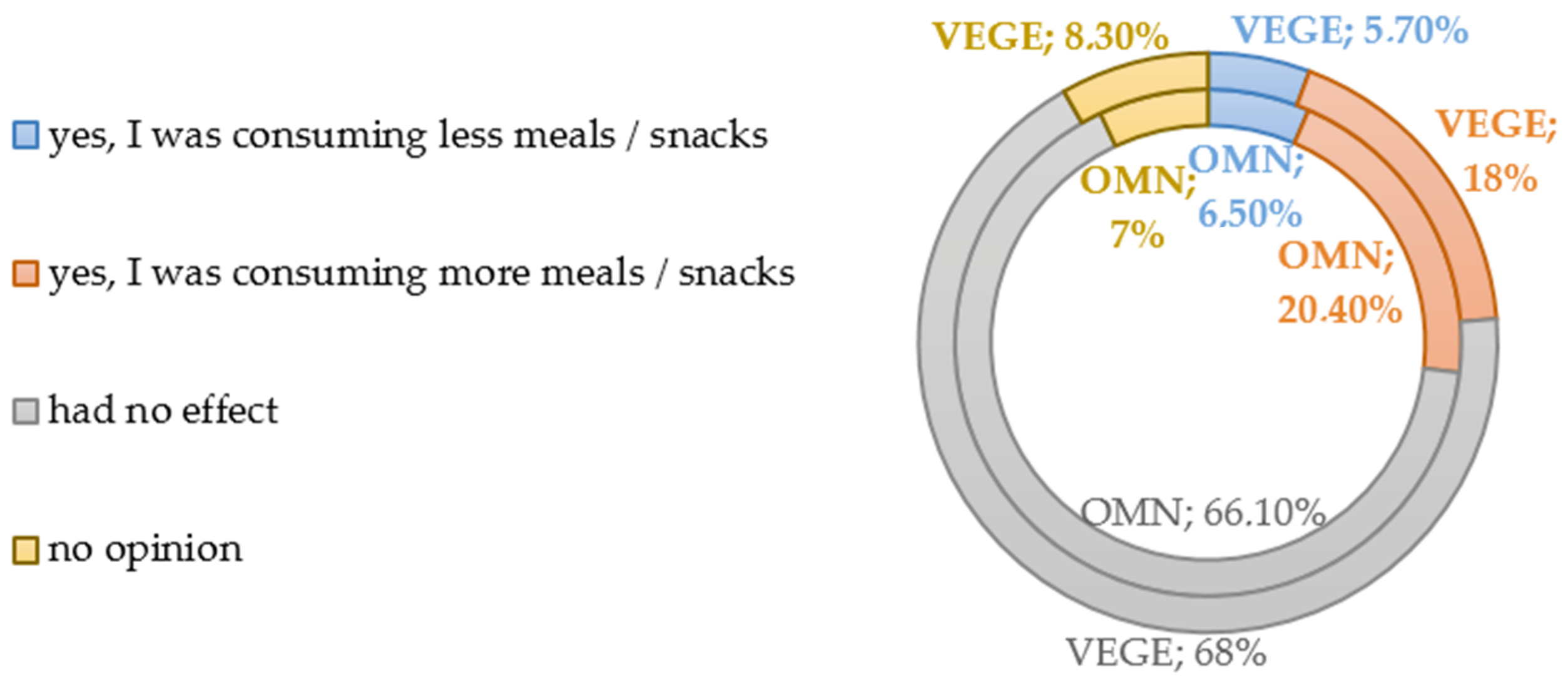
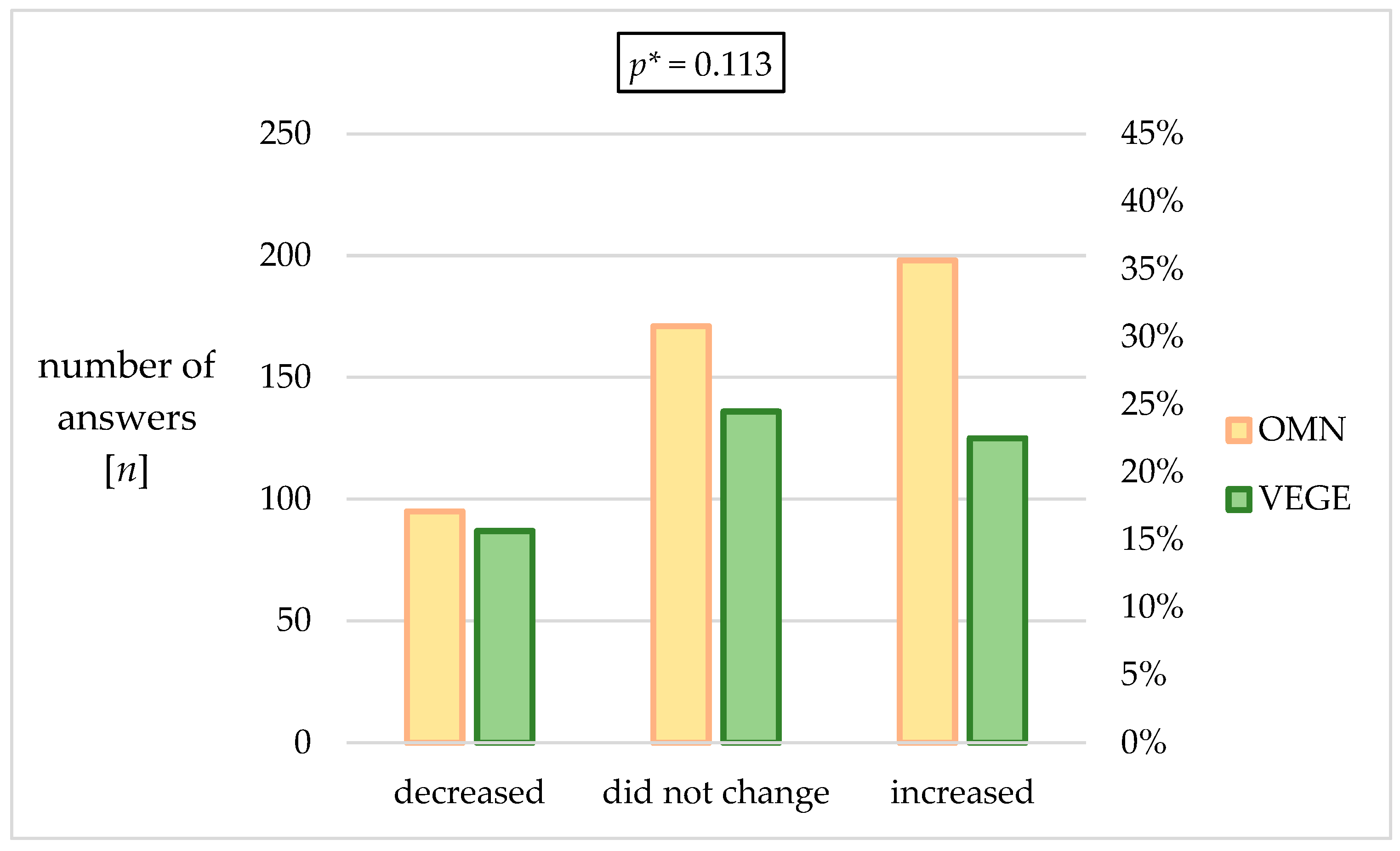
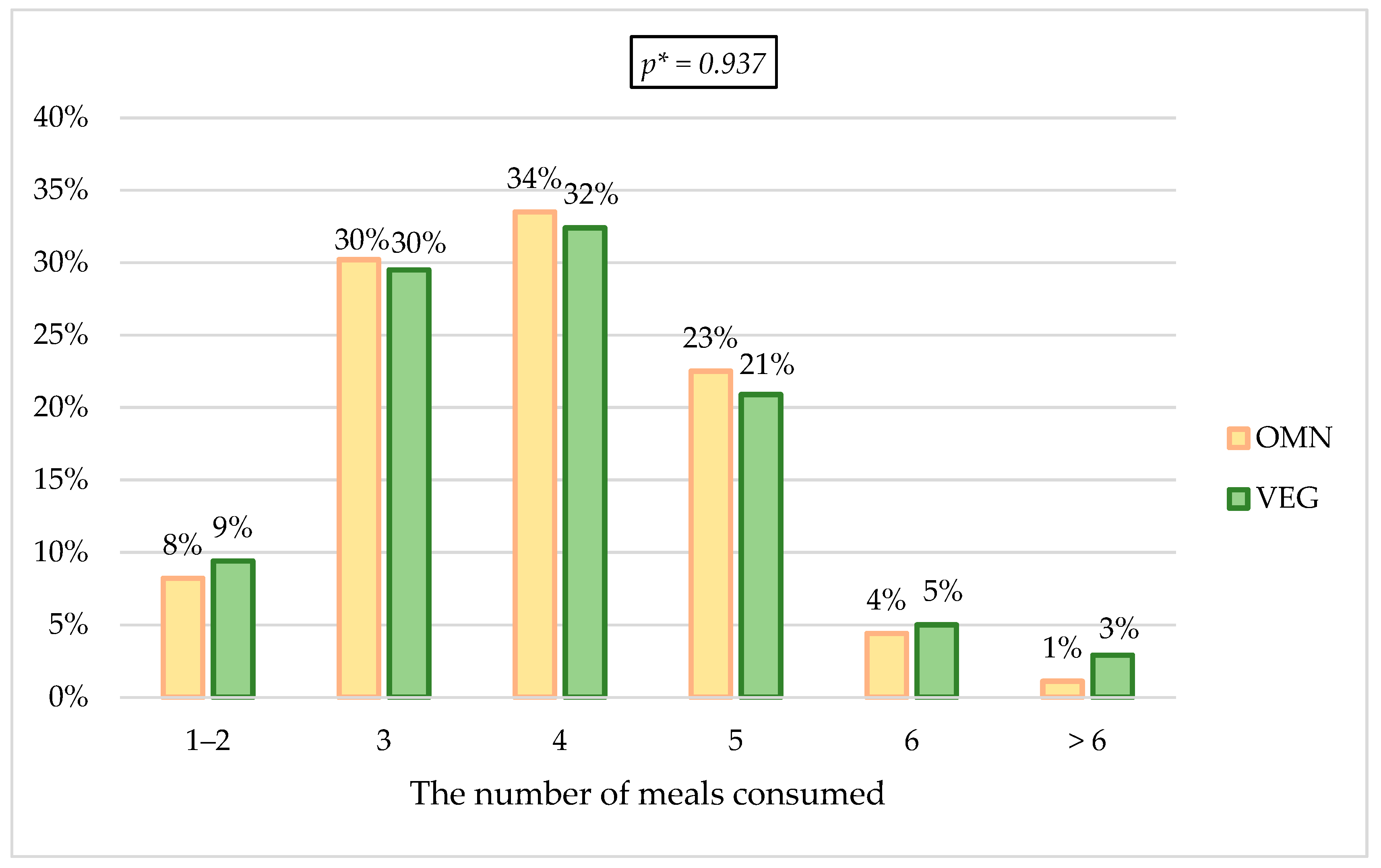
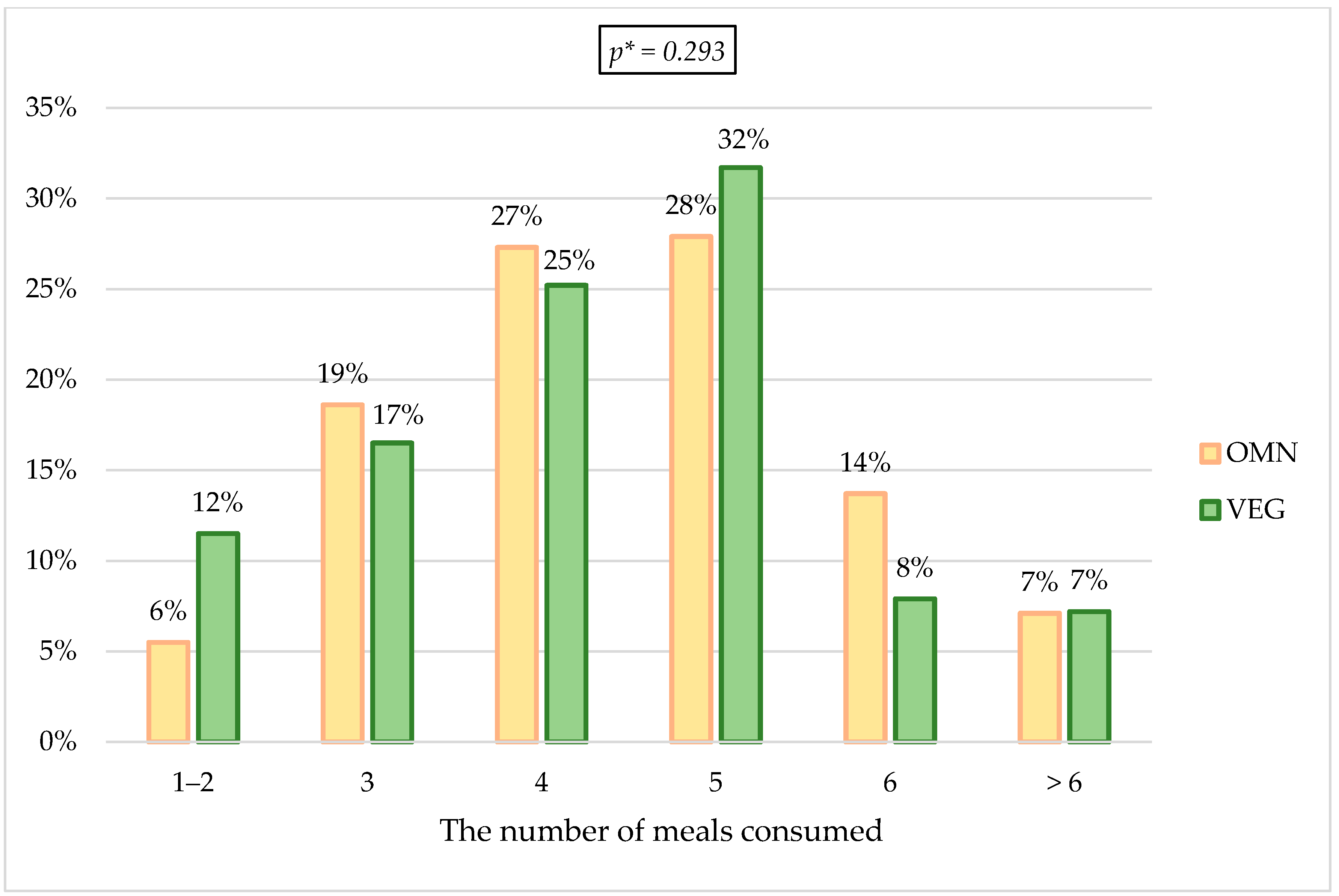
3.3.2. Changes Related to the Number of Meals Eaten, Dietary Preferences, and Body Weight Value
3.4. Dietary Changes during a Pandemic—Refer to 60% of Responders Declaring Such Changes
- More time for snacks/snacking—48.9% OMN vs. 38.8% VEGE.
- More time to prepare meals—35.8% OMN vs. 34.5% VEGE.
- I wanted to take better care of my health in this particular period—31.6% OMN vs. 33.5% VEGE.
- Stress, fear, negative emotions—29.8% OMN vs. 28.2% VEGE.
4. Discussion
4.1. Risk Factors of Cardiovascular Diseases among the Respondents (Characteristics of the Study Group)
4.1.1. Classification by BMI Value
4.1.2. Disease Burden—Cardiovascular Risk
4.1.3. Nutritional Factors Important in Estimating Cardiovascular Risk
4.2. Changes in the Quality of Life Caused by an Epidemic Situation
4.2.1. Changes in the Quality of Life—Physical Activity
4.2.2. Changes in Quality of Life—Sleeping
4.2.3. Changes in Quality of Life—General Eating Behavior
4.2.4. Changes in Quality of Life—Effects on Body Weight
4.3. Additional Detailed Observations Regarding Changes in Eating Habits during the Pandemic—Concerns about 60% of Respondents Who Confirmed the Existence of Differences
4.3.1. Changes in Food Intake
4.3.2. Changes in the Number of Meals Eaten
4.3.3. Changes in the Regularity of Meals Eaten
4.3.4. Changes to the Way Food Is Prepared
4.3.5. Changes in Nutritional Behavior (Favorable or Unfavorable)
4.3.6. Pandemic Impact—Summary of Changes in the Nutrition Quality
4.4. Strengths and Limitations
4.4.1. Strengths
- The study participants did not show any differences concerning average age, which proves reliable samples. The division of the study participants into age categories was primarily planned, but due to the above, such a division was abandoned. The similar age in groups may be due to the place of recruitment, social media, which young adults or adults mainly use.
- The results obtained in this study enrich the current positive reports on the vegetarian diet showing that even under a situation that has never happened before (the pandemic), people who follow such a diet show more correct eating behavior, which can have a positive effect on health.
4.4.2. Limitations
- The measurement was not previously validated in the literature.
- A narrow age group does not give a complete cross-section of possible outcomes.
- The data were collected through an online-based questionnaire; the possibility of selection bias should be taken into account, as it is possible that people who completed our form were interested in a healthy lifestyle.
- Since a survey was performed during the lockdown, the possibilities of checking the nutritional status were limited. Moreover, most of the available studies comparing groups of vegetarians and non-vegetarians also took into account the BMI indicator in question, so it was concluded that its use might constitute a valuable reference. However, it should be noted that the limitations of BMI are being increasingly emphasized; therefore, it should not be considered a perfect tool [49,130].
- Respondents may have been tempted to report increased consumption of commonly considered “healthy” foods and consumption of “unhealthy” food as lower than it is.
- The fact that the questionnaire was web-based and self-reported could have negatively influenced data quality.
- This study was based on univariate analysis.
5. Conclusions
5.1. Information on Cardiovascular Risk Factors
5.2. Information on Changes in Quality of Life
5.3. Changes in Eating Habits during the Pandemic
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19—11 March 2020. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-COVID-19---11-march-2020 (accessed on 12 October 2022).
- Decree of the Minister of Health of 20 March 2020 Regarding the Announcement of the State of the Epidemic in the Territory of the Republic of Poland. Available online: https://isap.sejm.gov.pl/isap.nsf/DocDetails.xsp?id=WDU20200000491 (accessed on 12 October 2022). (In Polish)
- Bennett, G.; Young, E.; Butler, I.; Coe, S. The Impact of Lockdown During the COVID-19 Outbreak on Dietary Habits in Various Population Groups: A Scoping Review. Front. Nutr. 2021, 8, 626432. [Google Scholar] [CrossRef] [PubMed]
- Al Hourani, H.; Alkhatib, B.; Abdullah, M. Impact of COVID-19 Lockdown on Body Weight, Eating Habits, and Physical Activity of Jordanian Children and Adolescents. Disaster Med. Public Health Prep. 2021, 16, 1855–1863. [Google Scholar] [CrossRef] [PubMed]
- Deschasaux-Tanguy, M.; Druesne-Pecollo, N.; Esseddik, Y.; de Edelenyi, F.S.; Allès, B.; Andreeva, V.A.; Baudry, J.; Charreire, H.; Deschamps, V.; Egnell, M.; et al. Diet and Physical Activity during the Coronavirus Disease 2019 (COVID-19) Lockdown (March–May 2020): Results from the French NutriNet-Santé Cohort Study. Am. J. Clin. Nutr. 2021, 113, 924–938. [Google Scholar] [CrossRef] [PubMed]
- Robinson, E.; Boyland, E.; Chisholm, A.; Harrold, J.; Maloney, N.G.; Marty, L.; Mead, B.R.; Noonan, R.; Hardman, C.A. Obesity, Eating Behavior and Physical Activity during COVID-19 Lockdown: A Study of UK Adults. Appetite 2021, 156, 104853. [Google Scholar] [CrossRef] [PubMed]
- Błaszczyk-Bębenek, E.; Jagielski, P.; Bolesławska, I.; Jagielska, A.; Nitsch-Osuch, A.; Kawalec, P. Nutrition Behaviors in Polish Adults before and during COVID-19 Lockdown. Nutrients 2020, 12, 3084. [Google Scholar] [CrossRef]
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The Psychological Impact of Quarantine and How to Reduce It: Rapid Review of the Evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef] [Green Version]
- Yoon, M.-K.; Kim, S.-Y.; Ko, H.-S.; Lee, M.-S. System Effectiveness of Detection, Brief Intervention and Refer to Treatment for the People with Post-Traumatic Emotional Distress by MERS: A Case Report of Community-Based Proactive Intervention in South Korea. Int. J. Ment. Health Syst. 2016, 10, 51. [Google Scholar] [CrossRef] [Green Version]
- Hawryluck, L.; Gold, W.L.; Robinson, S.; Pogorski, S.; Galea, S.; Styra, R. SARS Control and Psychological Effects of Quarantine, Toronto, Canada. Emerg. Infect. Dis 2004, 10, 1206–1212. [Google Scholar] [CrossRef]
- Mihashi, M.; Otsubo, Y.; Yinjuan, X.; Nagatomi, K.; Hoshiko, M.; Ishitake, T. Predictive Factors of Psychological Disorder Development during Recovery Following SARS Outbreak. Health Psychol. 2009, 28, 91–100. [Google Scholar] [CrossRef]
- Marjanovic, Z.; Greenglass, E.R.; Coffey, S. The Relevance of Psychosocial Variables and Working Conditions in Predicting Nurses’ Coping Strategies during the SARS Crisis: An Online Questionnaire Survey. Int. J. Nurs. Stud. 2007, 44, 991–998. [Google Scholar] [CrossRef]
- Reynolds, D.L.; Garay, J.R.; Deamond, S.L.; Moran, M.K.; Gold, W.; Styra, R. Understanding, Compliance and Psychological Impact of the SARS Quarantine Experience. Epidemiol. Infect. 2008, 136, 997–1007. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Moreno, D.V.; Vazquez, S.; Cheslack-Postava, K.; Xu, G.; Cycowicz, Y.M. Changes in Appetite during Quarantine and Their Association with Pre-COVID-19 Mental and Physical Health. Appetite 2022, 176, 106104. [Google Scholar] [CrossRef] [PubMed]
- Fürtjes, S.; King, J.A.; Goeke, C.; Seidel, M.; Goschke, T.; Horstmann, A.; Ehrlich, S. Automatic and Controlled Processing: Implications for Eating Behavior. Nutrients 2020, 12, 1097. [Google Scholar] [CrossRef] [Green Version]
- Kabir, A.; Miah, S.; Islam, A. Factors Influencing Eating Behavior and Dietary Intake among Resident Students in a Public University in Bangladesh: A Qualitative Study. PLoS ONE 2018, 13, e0198801. [Google Scholar] [CrossRef] [Green Version]
- Razzoli, M.; Bartolomucci, A. The Dichotomous Effect of Chronic Stress on Obesity. Trends Endocrinol. Metab. 2016, 27, 504–515. [Google Scholar] [CrossRef] [Green Version]
- Maniscalco, J.W.; Rinaman, L. Interoceptive Modulation of Neuroendocrine, Emotional, and Hypophagic Responses to Stress. Physiol. Behav. 2017, 176, 195–206. [Google Scholar] [CrossRef]
- Gasmi, A.; Noor, S.; Tippairote, T.; Dadar, M.; Menzel, A.; Bjørklund, G. Individual Risk Management Strategy and Potential Therapeutic Options for the COVID-19 Pandemic. Clin. Immunol. 2020, 215, 108409. [Google Scholar] [CrossRef] [PubMed]
- Bracale, R.; Vaccaro, C.M. Changes in Food Choice Following Restrictive Measures Due to COVID-19. Nutr. Metab. Cardiovasc. Dis. 2020, 30, 1423–1426. [Google Scholar] [CrossRef] [PubMed]
- Husain, W.; Ashkanani, F. Does COVID-19 Change Dietary Habits and Lifestyle Behaviours in Kuwait: A Community-Based Cross-Sectional Study. Environ. Health Prev. Med. 2020, 25, 61. [Google Scholar] [CrossRef]
- Bhutani, S.; Cooper, J.A.; vanDellen, M.R. Self-Reported Changes in Energy Balance Behaviors during COVID-19-Related Home Confinement: A Cross-Sectional Study. Am. J. Health Behav. 2021, 45, 756–770. [Google Scholar] [CrossRef]
- Di Renzo, L.; Gualtieri, P.; Pivari, F.; Soldati, L.; Attinà, A.; Cinelli, G.; Leggeri, C.; Caparello, G.; Barrea, L.; Scerbo, F.; et al. Eating Habits and Lifestyle Changes during COVID-19 Lockdown: An Italian Survey. J. Transl. Med. 2020, 18, 229. [Google Scholar] [CrossRef] [PubMed]
- Pietrobelli, A.; Pecoraro, L.; Ferruzzi, A.; Heo, M.; Faith, M.; Zoller, T.; Antoniazzi, F.; Piacentini, G.; Fearnbach, S.N.; Heymsfield, S.B. Effects of COVID-19 Lockdown on Lifestyle Behaviors in Children with Obesity Living in Verona, Italy: A Longitudinal Study. Obesity 2020, 28, 1382–1385. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Pérez, C.; Molina-Montes, E.; Verardo, V.; Artacho, R.; García-Villanova, B.; Guerra-Hernández, E.J.; Ruíz-López, M.D. Changes in Dietary Behaviours during the COVID-19 Outbreak Confinement in the Spanish COVIDiet Study. Nutrients 2020, 12, 1730. [Google Scholar] [CrossRef] [PubMed]
- Navarro-Pérez, C.F.; Fernández-Aparicio, Á.; González-Jiménez, E.; Montero-Alonso, M.Á.; Schmidt-RioValle, J. Effects of COVID-19 Lockdown on the Dietary Habits and Lifestyle in a Population in Southern Spain: A Cross-Sectional Questionnaire. Eur. J. Clin. Nutr. 2022, 76, 883–890. [Google Scholar] [CrossRef] [PubMed]
- Cheikh Ismail, L.; Hashim, M.; Mohamad, M.N.; Hassan, H.; Ajab, A.; Stojanovska, L.; Jarrar, A.H.; Hasan, H.; Abu Jamous, D.O.; Saleh, S.T.; et al. Dietary Habits and Lifestyle During Coronavirus Pandemic Lockdown: Experience From Lebanon. Front. Nutr. 2021, 8, 730425. [Google Scholar] [CrossRef] [PubMed]
- Ammar, A.; Brach, M.; Trabelsi, K.; Chtourou, H.; Boukhris, O.; Masmoudi, L.; Bouaziz, B.; Bentlage, E.; How, D.; Ahmed, M.; et al. Effects of COVID-19 Home Confinement on Eating Behaviour and Physical Activity: Results of the ECLB-COVID-19 International Online Survey. Nutrients 2020, 12, 1583. [Google Scholar] [CrossRef]
- Gallo, L.A.; Gallo, T.F.; Young, S.L.; Moritz, K.M.; Akison, L.K. The Impact of Isolation Measures Due to COVID-19 on Energy Intake and Physical Activity Levels in Australian University Students. Nutrients 2020, 12, 1865. [Google Scholar] [CrossRef]
- Matsungo, T.M.; Chopera, P. Effect of the COVID-19-Induced Lockdown on Nutrition, Health and Lifestyle Patterns among Adults in Zimbabwe. BMJ Nutr. Prev. Health 2020, 3, 205–212. [Google Scholar] [CrossRef]
- Mehta, V. The Impact of COVID-19 on the Dietary Habits of Middle-Class Population in Mulund, Mumbai, India. Available online: https://preprints.aijr.org/index.php/ap/preprint/view/82 (accessed on 17 August 2022).
- Pellegrini, M.; Ponzo, V.; Rosato, R.; Scumaci, E.; Goitre, I.; Benso, A.; Belcastro, S.; Crespi, C.; De Michieli, F.; Ghigo, E.; et al. Changes in Weight and Nutritional Habits in Adults with Obesity during the “Lockdown” Period Caused by the COVID-19 Virus Emergency. Nutrients 2020, 12, 2016. [Google Scholar] [CrossRef]
- Zachary, Z.; Brianna, F.; Brianna, L.; Garrett, P.; Jade, W.; Alyssa, D.; Mikayla, K. Self-Quarantine and Weight Gain Related Risk Factors during the COVID-19 Pandemic. Obes. Res. Clin. Pr. 2020, 14, 210–216. [Google Scholar] [CrossRef]
- Sidebottom, C.; Ullevig, S.; Cheever, K.; Zhang, T. Effects of COVID-19 Pandemic and Quarantine Period on Physical Activity and Dietary Habits of College-Aged Students. Sport. Med. Health Sci. 2021, 3, 228–235. [Google Scholar] [CrossRef] [PubMed]
- Global, Regional, and National Comparative Risk Assessment of 79 Behavioural, Environmental and Occupational, and Metabolic Risks or Clusters of Risks, 1990–2015: A Systematic Analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1659–1724. [CrossRef] [Green Version]
- Noncommunicable Diseases. Available online: https://www.who.int/news-room/fact-sheets/detail/noncommunicable-diseases (accessed on 12 October 2022).
- World Health Organization. Regional Office for Europe European Health Report 2018: More than Numbers—Evidence for All: Highlights; World Health Organization. Regional Office for Europe: København, Denmark, 2018; ISBN 978-92-890-5344-0. [Google Scholar]
- GBD 2019 Diseases and Injuries Collaborators Global Burden of 369 Diseases and Injuries in 204 Countries and Territories, 1990-2019: A Systematic Analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1204–1222. [CrossRef] [PubMed]
- Willett, W.; Rockström, J.; Loken, B.; Springmann, M.; Lang, T.; Vermeulen, S.; Garnett, T.; Tilman, D.; DeClerck, F.; Wood, A.; et al. Food in the Anthropocene: The EAT-Lancet Commission on Healthy Diets from Sustainable Food Systems. Lancet 2019, 393, 447–492. [Google Scholar] [CrossRef] [PubMed]
- Visseren, F.L.J.; Mach, F.; Smulders, Y.M.; Carballo, D.; Koskinas, K.C.; Bäck, M.; Benetos, A.; Biffi, A.; Boavida, J.-M.; Capodanno, D.; et al. 2021 ESC Guidelines on Cardiovascular Disease Prevention in Clinical Practice. Eur. Heart J. 2021, 42, 3227–3337. [Google Scholar] [CrossRef] [PubMed]
- Urgent Health Challenges for the Next Decade. Available online: https://www.who.int/news-room/photo-story/photo-story-detail/urgent-health-challenges-for-the-next-decade (accessed on 12 October 2022).
- History of Vegetarianism—Extracts from Some Journals 1843-48. Available online: https://ivu.org/history/vegetarian.html (accessed on 30 September 2022).
- Definition of Veganism. Available online: https://www.vegansociety.com/go-vegan/definition-veganism (accessed on 30 September 2022).
- Leitzmann, C. Vegetarian Nutrition: Past, Present, Future. Am. J Clin. Nutr. 2014, 100 (Suppl. 1), 496S–502S. [Google Scholar] [CrossRef] [Green Version]
- Melina, V.; Craig, W.; Levin, S. Position of the Academy of Nutrition and Dietetics: Vegetarian Diets. J. Acad. Nutr. Diet. 2016, 116, 1970–1980. [Google Scholar] [CrossRef]
- Rizzo, G.; Laganà, A.S.; Rapisarda, A.M.C.; La Ferrera, G.M.G.; Buscema, M.; Rossetti, P.; Nigro, A.; Muscia, V.; Valenti, G.; Sapia, F.; et al. Vitamin B12 among Vegetarians: Status, Assessment and Supplementation. Nutrients 2016, 8, 767. [Google Scholar] [CrossRef] [Green Version]
- Craig, W.J.; Mangels, A.R. American Dietetic Association Position of the American Dietetic Association: Vegetarian Diets. J. Am. Diet. Assoc. 2009, 109, 1266–1282. [Google Scholar] [CrossRef]
- Agnoli, C.; Baroni, L.; Bertini, I.; Ciappellano, S.; Fabbri, A.; Papa, M.; Pellegrini, N.; Sbarbati, R.; Scarino, M.L.; Siani, V.; et al. Position Paper on Vegetarian Diets from the Working Group of the Italian Society of Human Nutrition. Nutr. Metab. Cardiovasc. Dis. 2017, 27, 1037–1052. [Google Scholar] [CrossRef]
- Bradbury, K.E.; Crowe, F.L.; Appleby, P.N.; Schmidt, J.A.; Travis, R.C.; Key, T.J. Serum Concentrations of Cholesterol, Apolipoprotein A-I and Apolipoprotein B in a Total of 1694 Meat-Eaters, Fish-Eaters, Vegetarians and Vegans. Eur. J. Clin. Nutr. 2014, 68, 178–183. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, T.; Yang, B.; Zheng, J.; Li, G.; Wahlqvist, M.L.; Li, D. Cardiovascular Disease Mortality and Cancer Incidence in Vegetarians: A Meta-Analysis and Systematic Review. Ann. Nutr. Metab. 2012, 60, 233–240. [Google Scholar] [CrossRef]
- Tonstad, S.; Stewart, K.; Oda, K.; Batech, M.; Herring, R.P.; Fraser, G.E. Vegetarian Diets and Incidence of Diabetes in the Adventist Health Study-2. Nutr. Metab. Cardiovasc. Dis. 2013, 23, 292–299. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Orlich, M.J.; Singh, P.N.; Sabaté, J.; Jaceldo-Siegl, K.; Fan, J.; Knutsen, S.; Beeson, W.L.; Fraser, G.E. Vegetarian Dietary Patterns and Mortality in Adventist Health Study 2. JAMA Intern. Med. 2013, 173, 1230–1238. [Google Scholar] [CrossRef] [PubMed]
- Yokoyama, Y.; Nishimura, K.; Barnard, N.D.; Takegami, M.; Watanabe, M.; Sekikawa, A.; Okamura, T.; Miyamoto, Y. Vegetarian Diets and Blood Pressure: A Meta-Analysis. JAMA Intern. Med. 2014, 174, 577–587. [Google Scholar] [CrossRef] [PubMed]
- Rosi, A.; Mena, P.; Pellegrini, N.; Turroni, S.; Neviani, E.; Ferrocino, I.; Di Cagno, R.; Ruini, L.; Ciati, R.; Angelino, D.; et al. Environmental Impact of Omnivorous, Ovo-Lacto-Vegetarian, and Vegan Diet. Sci. Rep. 2017, 7, 6105. [Google Scholar] [CrossRef] [Green Version]
- Appleby, P.N.; Key, T.J. The Long-Term Health of Vegetarians and Vegans. Proc. Nutr. Soc. 2016, 75, 287–293. [Google Scholar] [CrossRef] [Green Version]
- Najjar, R.S.; Moore, C.E.; Montgomery, B.D. Consumption of a Defined, Plant-Based Diet Reduces Lipoprotein(a), Inflammation, and Other Atherogenic Lipoproteins and Particles within 4 Weeks. Clin. Cardiol. 2018, 41, 1062–1068. [Google Scholar] [CrossRef] [Green Version]
- Kahleova, H.; Petersen, K.F.; Shulman, G.I.; Alwarith, J.; Rembert, E.; Tura, A.; Hill, M.; Holubkov, R.; Barnard, N.D. Effect of a Low-Fat Vegan Diet on Body Weight, Insulin Sensitivity, Postprandial Metabolism, and Intramyocellular and Hepatocellular Lipid Levels in Overweight Adults: A Randomized Clinical Trial. JAMA Netw. Open. 2020, 3, e2025454. [Google Scholar] [CrossRef]
- Wright, N.; Wilson, L.; Smith, M.; Duncan, B.; McHugh, P. The BROAD Study: A Randomised Controlled Trial Using a Whole Food Plant-Based Diet in the Community for Obesity, Ischaemic Heart Disease or Diabetes. Nutr. Diabetes 2017, 7, e256. [Google Scholar] [CrossRef]
- Jakše, B.; Pinter, S.; Jakše, B.; Bučar Pajek, M.; Pajek, J. Effects of an Ad Libitum Consumed Low-Fat Plant-Based Diet Supplemented with Plant-Based Meal Replacements on Body Composition Indices. BioMed Res. Int. 2017, 2017, 9626390. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dorard, G.; Mathieu, S. Vegetarian and Omnivorous Diets: A Cross-Sectional Study of Motivation, Eating Disorders, and Body Shape Perception. Appetite 2021, 156, 104972. [Google Scholar] [CrossRef] [PubMed]
- Lavallee, K.; Zhang, X.C.; Michalak, J.; Schneider, S.; Margraf, J. Vegetarian Diet and Mental Health: Cross-Sectional and Longitudinal Analyses in Culturally Diverse Samples. J. Affect. Disord. 2019, 248, 147–154. [Google Scholar] [CrossRef] [PubMed]
- Rosenfeld, D.L.; Burrow, A.L. The Unified Model of Vegetarian Identity: A Conceptual Framework for Understanding Plant-Based Food Choices. Appetite 2017, 112, 78–95. [Google Scholar] [CrossRef]
- Rosenfeld, D.L.; Burrow, A.L. Vegetarian on Purpose: Understanding the Motivations of Plant-Based Dieters. Appetite 2017, 116, 456–463. [Google Scholar] [CrossRef]
- Derbyshire, E.J. Flexitarian Diets and Health: A Review of the Evidence-Based Literature. Front. Nutr. 2017, 3, 55. [Google Scholar] [CrossRef] [Green Version]
- Forestell, C.A.; Nezlek, J.B. Vegetarianism, Depression, and the Five Factor Model of Personality. Ecol. Food Nutr. 2018, 57, 246–259. [Google Scholar] [CrossRef] [Green Version]
- Mathieu, S.; Dorard, G. Vegetarianism and veganism lifestyle: Motivation and psychological dimensions associated with selective diet. Presse Med. 2016, 45, 726–733. [Google Scholar] [CrossRef]
- Rosenfeld, D.L. The Psychology of Vegetarianism: Recent Advances and Future Directions. Appetite 2018, 131, 125–138. [Google Scholar] [CrossRef]
- Rothgerber, H. Efforts to Overcome Vegetarian-Induced Dissonance among Meat Eaters. Appetite 2014, 79, 32–41. [Google Scholar] [CrossRef]
- Ruby, M.B.; Alvarenga, M.S.; Rozin, P.; Kirby, T.A.; Richer, E.; Rutsztein, G. Attitudes toward Beef and Vegetarians in Argentina, Brazil, France, and the USA. Appetite 2016, 96, 546–554. [Google Scholar] [CrossRef] [PubMed]
- Zuromski, K.L.; Witte, T.K.; Smith, A.R.; Goodwin, N.; Bodell, L.P.; Bartlett, M.; Siegfried, N. Increased Prevalence of Vegetarianism among Women with Eating Pathology. Eat. Behav. 2015, 19, 24–27. [Google Scholar] [CrossRef] [PubMed]
- Rosenfeld, D.L.; Burrow, A.L. Development and Validation of the Dietarian Identity Questionnaire: Assessing Self-Perceptions of Animal-Product Consumption. Appetite 2018, 127, 182–194. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, S.R.; Stallings, S.F.; Bessinger, R.C.; Brooks, G.T. Differences between Health and Ethical Vegetarians. Strength of Conviction, Nutrition Knowledge, Dietary Restriction, and Duration of Adherence. Appetite 2013, 65, 139–144. [Google Scholar] [CrossRef]
- Torna, E.; Smith, E.; Lamothe, M.; Langkamp-Henken, B.; Andrade, J.M. Comparison of Diet Quality of US Adults Based on Primary Motivation for Following a Vegetarian Diet: A Cross-Sectional Online Study. Nutr. Res. 2021, 90, 13–23. [Google Scholar] [CrossRef] [PubMed]
- Hopwood, C.J.; Bleidorn, W.; Schwaba, T.; Chen, S. Health, Environmental, and Animal Rights Motives for Vegetarian Eating. PLoS ONE 2020, 15, e0230609. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hargreaves, S.M.; Nakano, E.Y.; Zandonadi, R.P. Brazilian Vegetarian Population-Influence of Type of Diet, Motivation and Sociodemographic Variables on Quality of Life Measured by Specific Tool (VEGQOL). Nutrients 2020, 12, 1406. [Google Scholar] [CrossRef]
- Khan, M.A.; Menon, P.; Govender, R.; Abu Samra, A.M.; Allaham, K.K.; Nauman, J.; Östlundh, L.; Mustafa, H.; Smith, J.E.M.; AlKaabi, J.M. Systematic Review of the Effects of Pandemic Confinements on Body Weight and Their Determinants. Br. J. Nutr. 2022, 127, 298–317. [Google Scholar] [CrossRef]
- The Jamovi Project 2021. Available online: https://www.jamovi.org (accessed on 30 September 2022).
- SPSS Statistics—Overview. Available online: https://www.ibm.com/products/spss-statistics (accessed on 30 December 2022).
- Clarys, P.; Deliens, T.; Huybrechts, I.; Deriemaeker, P.; Vanaelst, B.; De Keyzer, W.; Hebbelinck, M.; Mullie, P. Comparison of Nutritional Quality of the Vegan, Vegetarian, Semi-Vegetarian, Pesco-Vegetarian and Omnivorous Diet. Nutrients 2014, 6, 1318–1332. [Google Scholar] [CrossRef]
- Fontes, T.; Rodrigues, L.M.; Ferreira-Pêgo, C. Comparison between Different Groups of Vegetarianism and Its Associations with Body Composition: A Literature Review from 2015 to 2021. Nutrients 2022, 14, 1853. [Google Scholar] [CrossRef]
- Saintila, J.; Lozano López, T.E.; Ruiz Mamani, P.G.; White, M.; Huancahuire-Vega, S. Health-Related Quality of Life, Blood Pressure, and Biochemical and Anthropometric Profile in Vegetarians and Nonvegetarians. J. Nutr. Metab. 2020, 2020, 3629742. [Google Scholar] [CrossRef] [PubMed]
- Brytek-Matera, A. Interaction between Vegetarian Versus Omnivorous Diet and Unhealthy Eating Patterns (Orthorexia Nervosa, Cognitive Restraint) and Body Mass Index in Adults. Nutrients 2020, 12, 646. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jaceldo-Siegl, K.; Estevez, D.; Fraser, G.E.; Hayes-Bautista, D.E.; Flores, H.; Jordan, M.; Singh, P.N. Plant-Based Diets in Hispanic/Latino Adult Adventists in the United States and Their Association With Body Mass Index. Am. J. Health Promot. 2019, 33, 869–875. [Google Scholar] [CrossRef] [PubMed]
- Vanacore, D.; Messina, G.; Lama, S.; Bitti, G.; Ambrosio, P.; Tenore, G.; Messina, A.; Monda, V.; Zappavigna, S.; Boccellino, M.; et al. Effect of Restriction Vegan Diet’s on Muscle Mass, Oxidative Status, and Myocytes Differentiation: A Pilot Study. J. Cell. Physiol. 2018, 233, 9345–9353. [Google Scholar] [CrossRef] [PubMed]
- Kwiatkowska, I.; Olszak, J.; Formanowicz, P.; Formanowicz, D. Nutritional Status and Habits among People on Vegan, Lacto/Ovo-Vegetarian, Pescatarian and Traditional Diets. Nutrients 2022, 14, 4591. [Google Scholar] [CrossRef]
- Roth, G.A.; Mensah, G.A.; Johnson, C.O.; Addolorato, G.; Ammirati, E.; Baddour, L.M.; Barengo, N.C.; Beaton, A.Z.; Benjamin, E.J.; Benziger, C.P.; et al. Global Burden of Cardiovascular Diseases and Risk Factors, 1990-2019: Update From the GBD 2019 Study. J. Am. Coll. Cardiol. 2020, 76, 2982–3021. [Google Scholar] [CrossRef]
- Jóźwiak, J.J.; Studziński, K.; Tomasik, T.; Windak, A.; Mastej, M.; Catapano, A.L.; Ray, K.K.; Mikhailidis, D.P.; Toth, P.P.; Howard, G.; et al. The Prevalence of Cardiovascular Risk Factors and Cardiovascular Disease among Primary Care Patients in Poland: Results from the LIPIDOGRAM2015 Study. Atheroscler. Suppl. 2020, 42, e15–e24. [Google Scholar] [CrossRef]
- GUS Sytuacja demograficzna Polski do 2020 roku. Zgony i Umieralność. Available online: https://stat.gov.pl/obszary-tematyczne/ludnosc/ludnosc/sytuacja-demograficzna-polski-do-2020-roku-zgony-i-umieralnosc,40,1.html (accessed on 20 December 2022). (In Polish)
- Leong, D.P.; Joseph, P.G.; McKee, M.; Anand, S.S.; Teo, K.K.; Schwalm, J.-D.; Yusuf, S. Reducing the Global Burden of Cardiovascular Disease, Part 2: Prevention and Treatment of Cardiovascular Disease. Circ. Res. 2017, 121, 695–710. [Google Scholar] [CrossRef]
- Nations, U. LIFESTYLE DISEASES: An Economic Burden on the Health Services. Available online: https://www.un.org/en/chronicle/article/lifestyle-diseases-economic-burden-health-services (accessed on 1 December 2022).
- Livingstone, K.M.; Abbott, G.; Ward, J.; Bowe, S.J. Unhealthy Lifestyle, Genetics and Risk of Cardiovascular Disease and Mortality in 76,958 Individuals from the UK Biobank Cohort Study. Nutrients 2021, 13, 4283. [Google Scholar] [CrossRef]
- Lin, C.-L.; Wang, J.-H.; Chang, C.-C.; Chiu, T.H.T.; Lin, M.-N. Vegetarian Diets and Medical Expenditure in Taiwan—A Matched Cohort Study. Nutrients 2019, 11, 2688. [Google Scholar] [CrossRef]
- Jakše, B.; Jakše, B.; Godnov, U.; Pinter, S. Nutritional, Cardiovascular Health and Lifestyle Status of ‘Health Conscious’ Adult Vegans and Non-Vegans from Slovenia: A Cross-Sectional Self-Reported Survey. Int. J. Environ. Res. Public Health 2021, 18, 5968. [Google Scholar] [CrossRef] [PubMed]
- Battaglia Richi, E.; Baumer, B.; Conrad, B.; Darioli, R.; Schmid, A.; Keller, U. Health Risks Associated with Meat Consumption: A Review of Epidemiological Studies. Int. J. Vitam. Nutr. Res. 2015, 85, 70–78. [Google Scholar] [CrossRef] [PubMed]
- Zhong, V.W.; Van Horn, L.; Greenland, P.; Carnethon, M.R.; Ning, H.; Wilkins, J.T.; Lloyd-Jones, D.M.; Allen, N.B. Associations of Processed Meat, Unprocessed Red Meat, Poultry, or Fish Intake With Incident Cardiovascular Disease and All-Cause Mortality. JAMA Intern. Med. 2020, 180, 503–512. [Google Scholar] [CrossRef] [PubMed]
- Larsson, S.C.; Orsini, N. Red Meat and Processed Meat Consumption and All-Cause Mortality: A Meta-Analysis. Am. J. Epidemiol. 2014, 179, 282–289. [Google Scholar] [CrossRef] [Green Version]
- Abete, I.; Romaguera, D.; Vieira, A.R.; Lopez de Munain, A.; Norat, T. Association between Total, Processed, Red and White Meat Consumption and All-Cause, CVD and IHD Mortality: A Meta-Analysis of Cohort Studies. Br. J. Nutr. 2014, 112, 762–775. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.; Pan, L.; Sun, C.; Xi, Y.; Wang, L.; Li, D. Red Meat Consumption and the Risk of Stroke: A Dose-Response Meta-Analysis of Prospective Cohort Studies. J. Stroke Cereb. Dis. 2016, 25, 1177–1186. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, X.; Lin, X.; Ouyang, Y.Y.; Liu, J.; Zhao, G.; Pan, A.; Hu, F.B. Red and Processed Meat Consumption and Mortality: Dose-Response Meta-Analysis of Prospective Cohort Studies. Public Health Nutr. 2016, 19, 893–905. [Google Scholar] [CrossRef] [Green Version]
- Micha, R.; Michas, G.; Mozaffarian, D. Unprocessed Red and Processed Meats and Risk of Coronary Artery Disease and Type 2 Diabetes--an Updated Review of the Evidence. Curr. Atheroscler. Rep. 2012, 14, 515–524. [Google Scholar] [CrossRef] [Green Version]
- Cui, K.; Liu, Y.; Zhu, L.; Mei, X.; Jin, P.; Luo, Y. Association between Intake of Red and Processed Meat and the Risk of Heart Failure: A Meta-Analysis. BMC Public Health 2019, 19, 354. [Google Scholar] [CrossRef] [Green Version]
- Etemadi, A.; Sinha, R.; Ward, M.H.; Graubard, B.I.; Inoue-Choi, M.; Dawsey, S.M.; Abnet, C.C. Mortality from Different Causes Associated with Meat, Heme Iron, Nitrates, and Nitrites in the NIH-AARP Diet and Health Study: Population Based Cohort Study. BMJ 2017, 357, j1957. [Google Scholar] [CrossRef]
- Burlingame, B.; Nishida, C.; Uauy, R.; Weisell, R. (Eds.) Fats and Fatty Acids in Human Nutrition. Report of an Expert Consultation; FAO Food and Nutrition Paper; S. Karger: Basel, Switzerland, 2010; Volume 91, pp. 1–166. [Google Scholar]
- Li, J.; Sun, Q. Consumption of Saturated Fatty Acids and Coronary Heart Disease Risk. Int. J. Cardiol. 2019, 279, 27–28. [Google Scholar] [CrossRef] [PubMed]
- Trans Fatty Acids and Lipid Profile: A Serious Risk Factor to Cardiovascular Disease, Cancer and Diabetes. Diabetes Metab. Syndr. Clin. Res. Rev. 2019, 13, 1643–1647. [CrossRef] [PubMed]
- de Souza, R.J.; Mente, A.; Maroleanu, A.; Cozma, A.I.; Ha, V.; Kishibe, T.; Uleryk, E.; Budylowski, P.; Schünemann, H.; Beyene, J.; et al. Intake of Saturated and Trans Unsaturated Fatty Acids and Risk of All Cause Mortality, Cardiovascular Disease, and Type 2 Diabetes: Systematic Review and Meta-Analysis of Observational Studies. BMJ 2015, 351, h3978. [Google Scholar] [CrossRef] [Green Version]
- U.S. Department of Health and Human Services; U.S. Department of Agriculture. 2015–2020 Dietary Guidelines for Americans, 8th ed.; U.S. Department of Health and Human Services: Washington, DC, USA, 2015. Available online: https://health.gov/our-work/nutrition-physical-activity/dietary-guidelines/previous-dietary-guidelines/2015 (accessed on 12 October 2022).
- Healthy Diet. Available online: https://www.who.int/news-room/fact-sheets/detail/healthy-diet (accessed on 12 October 2022).
- Nochaiwong, S.; Ruengorn, C.; Thavorn, K.; Hutton, B.; Awiphan, R.; Phosuya, C.; Ruanta, Y.; Wongpakaran, N.; Wongpakaran, T. Global Prevalence of Mental Health Issues among the General Population during the Coronavirus Disease-2019 Pandemic: A Systematic Review and Meta-Analysis. Sci. Rep. 2021, 11, 10173. [Google Scholar] [CrossRef] [PubMed]
- Allabadi, H.; Dabis, J.; Aghabekian, V.; Khader, A.; Khammash, U. Impact of COVID-19 lockdown on dietary and lifestyle behaviours among adolescents in Palestine. Dyn. Hum. Health 2020, 2020, 7. [Google Scholar]
- Almughamis, N.; Alasfour, S.; Mehmood, S. Poor Eating Habits and Predictors of Weight Gain During the COVID-19 Quarantine Measures in Kuwait: A Cross Sectional Study; Research Square. F1000 Res. 2020, 9, 914. [Google Scholar] [CrossRef]
- Phillipou, A.; Meyer, D.; Neill, E.; Tan, E.J.; Toh, W.L.; Van Rheenen, T.E.; Rossell, S.L. Eating and Exercise Behaviors in Eating Disorders and the General Population during the COVID-19 Pandemic in Australia: Initial Results from the COLLATE Project. Int. J. Eat. Disord. 2020, 53, 1158–1165. [Google Scholar] [CrossRef]
- Yücel, Ü.; Kömbeci, K.; Tuğrul, G.; Uçar, A.; Yüksel, S. Changes in Diet, Lifestyle and Orthorexia Nervosa Attitudes of Vegetarian, Vegan and Omnivorous Individuals in COVID-19 Pandemic. Int. J. Nutr. Sci. 2021, 6, 74–80. [Google Scholar] [CrossRef]
- Marelli, S.; Castelnuovo, A.; Somma, A.; Castronovo, V.; Mombelli, S.; Bottoni, D.; Leitner, C.; Fossati, A.; Ferini-Strambi, L. Impact of COVID-19 Lockdown on Sleep Quality in University Students and Administration Staff. J. Neurol 2021, 268, 8–15. [Google Scholar] [CrossRef]
- Piekarska, M.; Pszczółka, M.; Parol, D.; Szewczyk, P.; Śliż, D.; Mamcarz, A. Sleeping Disorders in Healthy Individuals with Different Dietary Patterns and BMI, Questionnaire Assessment. Int. J. Environ. Res. Public Health 2021, 18, 12285. [Google Scholar] [CrossRef]
- Cellini, N.; Canale, N.; Mioni, G.; Costa, S. Changes in Sleep Pattern, Sense of Time and Digital Media Use during COVID-19 Lockdown in Italy. J. Sleep Res. 2020, 29, e13074. [Google Scholar] [CrossRef] [PubMed]
- Papazisis, Z.; Nikolaidis, P.T.; Trakada, G. Sleep, Physical Activity, and Diet of Adults during the Second Lockdown of the COVID-19 Pandemic in Greece. Int. J. Environ. Res. Public Health 2021, 18, 7292. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Roso, M.B.; de Carvalho Padilha, P.; Mantilla-Escalante, D.C.; Ulloa, N.; Brun, P.; Acevedo-Correa, D.; Arantes Ferreira Peres, W.; Martorell, M.; Aires, M.T.; de Oliveira Cardoso, L.; et al. COVID-19 Confinement and Changes of Adolescent’s Dietary Trends in Italy, Spain, Chile, Colombia and Brazil. Nutrients 2020, 12, 1807. [Google Scholar] [CrossRef] [PubMed]
- Scarmozzino, F.; Visioli, F. COVID-19 and the Subsequent Lockdown Modified Dietary Habits of Almost Half the Population in an Italian Sample. Foods 2020, 9, 675. [Google Scholar] [CrossRef]
- Sidor, A.; Rzymski, P. Dietary Choices and Habits during COVID-19 Lockdown: Experience from Poland. Nutrients 2020, 12, 1657. [Google Scholar] [CrossRef]
- Dondi, A.; Candela, E.; Morigi, F.; Lenzi, J.; Pierantoni, L.; Lanari, M. Parents’ Perception of Food Insecurity and of Its Effects on Their Children in Italy Six Months after the COVID-19 Pandemic Outbreak. Nutrients 2020, 13, 121. [Google Scholar] [CrossRef]
- Drywień, M.E.; Hamulka, J.; Zielinska-Pukos, M.A.; Jeruszka-Bielak, M.; Górnicka, M. The COVID-19 Pandemic Lockdowns and Changes in Body Weight among Polish Women. A Cross-Sectional Online Survey PLifeCOVID-19 Study. Sustainability 2020, 12, 7768. [Google Scholar] [CrossRef]
- Bhutani, S.; Cooper, J.A. COVID-19-Related Home Confinement in Adults: Weight Gain Risks and Opportunities. Obesity 2020, 28, 1576–1577. [Google Scholar] [CrossRef]
- Marchitelli, S.; Mazza, C.; Lenzi, A.; Ricci, E.; Gnessi, L.; Roma, P. Weight Gain in a Sample of Patients Affected by Overweight/Obesity with and without a Psychiatric Diagnosis during the COVID-19 Lockdown. Nutrients 2020, 12, 3525. [Google Scholar] [CrossRef]
- Food-Based Dietary Guidelines—Poland. Available online: http://www.fao.org/nutrition/education/food-dietary-guidelines/regions/poland/en/ (accessed on 7 August 2022).
- Górska, P.; Górna, I.; Miechowicz, I.; Przysławski, J. Changes in Eating Behaviour during SARS-CoV-2 Pandemic among the Inhabitants of Five European Countries. Foods 2021, 10, 1624. [Google Scholar] [CrossRef]
- Durán-Agüero, S.; Albornoz, P.; Morejón, Y.; Barrientos, C.; Mardones, M.J.; García-Milla, P.; Torres, X.; Landaeta-Díaz, L. Consumption of Pulses among Chilean Vegetarians and Non-Vegetarians during the COVID-19 Pandemic. J. Am. Nutr. Assoc. 2022, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Barnard, N.D.; Levin, S.M.; Yokoyama, Y. A Systematic Review and Meta-Analysis of Changes in Body Weight in Clinical Trials of Vegetarian Diets. J. Acad. Nutr. Diet. 2015, 115, 954–969. [Google Scholar] [CrossRef]
- Merino, J.; Joshi, A.D.; Nguyen, L.H.; Leeming, E.R.; Mazidi, M.; Drew, D.A.; Gibson, R.; Graham, M.S.; Lo, C.-H.; Capdevila, J.; et al. Diet Quality and Risk and Severity of COVID-19: A Prospective Cohort Study. Gut 2021, 70, 2096–2104. [Google Scholar] [CrossRef] [PubMed]
- Chrysant, S.G.; Chrysant, G.S. The Single Use of Body Mass Index for the Obesity Paradox Is Misleading and Should Be Used in Conjunction with Other Obesity Indices. Postgrad. Med. 2019, 131, 96–102. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics n = 861 | OMN | VEGE |
|---|---|---|
| n (%) * | ||
| The gender division, p *1 = 0.009 | ||
| Participants | 489 (56.8) | 372 (43.2) |
| Female | 420 (85.9) | 341 (91.7) |
| Male | 69 (14.1) | 31 (8.3) |
| Educational level, p *1 = 0.025 | ||
| University or university college level | 440 (90.9) | 315 (84.9) |
| Secondary education | 36 (7.4) | 39 (10.5) |
| Vocational education | 5 (1.0) | 10 (2.7) |
| Primary education | 3 (0.6) | 7 (1.9) |
| Place of residence, p *1 = 0.001 | ||
| Inhabiting a city The following responses were considered: a city with up to 50,000/100,000/250,000 residents; a city with more than 250,000 residents. | 384 (78.5) | 324 (87.1) |
| Rural area | 105 (21.5) | 48 (12.9) |
| Age, years, p *2 = 0.744 | mean ± SD | |
| all groups | 28.6 ± 7.60 | 29.2 ± 8.68 |
| Female | 29.0 ± 7.49 | 29.1 ± 8.77 |
| Male | 26.6 ± 7.99 | 30.6 ± 7.72 |
| Possible Answer | Cardiovascular Diseases, i.e., Heart Disease, Heart Attack, Stroke, Arterial Hypertension, Thrombosis | Abnormal Values of the Lipid Profile (Total Cholesterol, Triglycerides, HDL Cholesterol, LDL Cholesterol) | Fasting Glucose Abnormalities/ Diabetes/Insulin Resistance | ||||
|---|---|---|---|---|---|---|---|
| Groups | |||||||
| n * | % * | n * | % * | n * | % * | ||
| Yes | |||||||
| OMN | 243 | 49.69 | 256 | 52.35 | 167 | 34.15 | |
| VEGE | 175 | 47.04 | 175 | 47.04 | 133 | 35.75 | |
| No | |||||||
| OMN | 225 | 46.01 | 157 | 32.11 | 293 | 59.92 | |
| VEGE | 178 | 47.85 | 116 | 31.18 | 210 | 56.45 | |
| I don’t know | |||||||
| OMN | 21 | 4.29 | 76 | 15.54 | 29 | 5.93 | |
| VEGE | 19 | 5.11 | 81 | 21.77 | 29 | 7.80 | |
| p *2 | 0.684 | 0.057 | 0.431 | ||||
| Possible Answer | Cardiovascular Diseases, i.e., Heart Disease, Heart Attack, Stroke, Arterial Hypertension, Thrombosis | Abnormal Values of the Lipid Profile (Total Cholesterol, Triglycerides, HDL Cholesterol, LDL Cholesterol) | Fasting Glucose Abnormalities/ Diabetes/Insulin Resistance | ||||
|---|---|---|---|---|---|---|---|
| Groups | |||||||
| n * | % * | n * | % * | n * | % * | ||
| Yes | |||||||
| OMN | 31 | 6.3 | 57 | 11.7 | 64 | 13.1 | |
| VEGE | 24 | 6.5 | 40 | 10.8 | 25 | 6.7 | |
| No | |||||||
| OMN | 444 | 90.8 | 361 | 73.8 | 390 | 79.8 | |
| VEGE | 334 | 89.8 | 283 | 76.1 | 318 | 85.8 | |
| I don’t know | |||||||
| OMN | 14 | 2.9 | 71 | 14.5 | 35 | 7.2 | |
| VEGE | 14 | 3.8 | 49 | 13.2 | 28 | 7.5 | |
| p *2 | 0.758 | 0.751 | 0.010 | ||||
| CD Risk Factors: | The Blood Pressure Characteristic p = 0.864 *1 | Tobacco Smoking p = 0.003 *2 | Alcohol Consumption p = 0.448 *3 | ||||
|---|---|---|---|---|---|---|---|
| Studied Groups: | n * | % * | n * | % * | n * | % * | |
| I don’t know | Yes, occasionally | High consumption (daily or 3–5 x week) | |||||
| OMN | 52 | 10.6 | 40 | 8.18 | 19 | 3.9 | |
| VEGE | 52 | 14.0 | 46 | 12.37 | 25 | 6.7 | |
| I do not measure | Yes, regularly | Medium consumption (1–2 x week) | |||||
| OMN | 70 | 14.3 | 28 | 5.73 | 48 | 9.8 | |
| VEGE | 60 | 16.1 | 34 | 9.14 | 32 | 8.6 | |
| <120/60 mmHg | No | Low consumption (once a month or less, several times a month) | |||||
| OMN | 146 | 29.9 | 421 | 86.09 | 334 | 68.3 | |
| VEGE | 127 | 34.1 | 292 | 78.49 | 241 | 64.8 | |
| 140/80–120/60 mmHg | None | ||||||
| OMN | 201 | 41.1 | 86 | 17.6 | |||
| VEGE | 118 | 31.7 | 73 | 19.6 | |||
| >140/80 mmHg | No answer | ||||||
| OMN | 20 | 4.1 | 2 | 0.4 | |||
| VEGE | 15 | 4.0 | 1 | 0.3 | |||
| Categorization | OMN BMI [kg/m2] Mean ± SD | VEGE BMI [kg/m2] Mean ± SD | ||
|---|---|---|---|---|
| all groups p * < 0.001 | 23.5 ± 4.89 | 21.8 ± 3.57 | ||
| by gender | Female | Male | Female | Male |
| 23.3 ± 5.01 | 24.7 ± 3.94 | 21.6 ± 3.53 | 23.6 ± 3.54 | |
| BMI Classification p < 0.001 *2 | Group | n * | % * |
|---|---|---|---|
| Underweight (<18.5 kg/m2) | OMN | 32 | 6.6 |
| VEGE | 49 | 13.2 | |
| Normal weight (18.5 to <25.0 kg/m2) | OMN | 325 | 66.9 |
| VEGE | 263 | 70.7 | |
| Overweight (≥25.0 to <30.0 kg/m2) | OMN | 95 | 19.5 |
| VEGE | 51 | 13.7 | |
| Obesity (≥30 kg/m2) | OMN | 34 | 7.0 |
| VEGE | 9 | 2.4 |
| Responses | OMN | VEGE | p * |
|---|---|---|---|
| deep fried meals | 2.28 | 2 | <0.001 |
| meals with the addition of a large amount of fat (fast-food, pizza, ready meals) | 2.55 | 2.47 | 0.324 |
| addition to meals, e.g., butter or cream (or vegetable substitutes for these products) | 3.16 | 2.55 | <0.001 |
| oil addition to meals (rapeseed, sunflower, olive oil, linseed oil, etc.) | 4.04 | 4.19 | 0.006 |
| Health State of the Studied Groups | OMN | VEGE | ||
|---|---|---|---|---|
| n | % | n | % | |
| With risk factors for cardiovascular diseases (smoking regularly and/or medium/high alcohol consumption) | 95 | 19.4 | 91 | 24.46 |
| With risk factors for cardiovascular diseases (dyslipidemias and/or dysfunction of carbohydrate metabolism) | 125 | 25.5 | 66 | 17.74 |
| With cardiovascular diseases | 31 | 6.34 | 24 | 6.45 |
| With hypertension (>140/80 mmHg) | 20 | 4.1 | 15 | 4.0 |
| With obesity (BMI ≥ 30 kg/m2) | 36 | 7.4 | 9 | 2.4 |
| Responses p * = 0.360 | OMN | VEGE |
|---|---|---|
| % | ||
| My dietary habits did not change. | 41.8 | 40.3 |
| Yes, I consumed more healthy products, such as fruits, vegetables, nuts, and whole grain products. | 27.3 | 31.7 |
| Yes, I consumed more sweets. | 31.1 | 25.8 |
| Yes, I consumed more savory snacks. | 20.3 | 21.9 |
| Yes, I ate more unhealthy meals/snacks, such as ready-made products, instant soups, dishes, and chips. | 19.2 | 17.8 |
| Category of Products | % of Respondents Declaring Product Consumption Increase | Increase Consumption Measure [Mean ± SD] | p *2 | |
|---|---|---|---|---|
| The Most Frequently Indicated Number of Servings | ||||
| OMN | VEGE | |||
| Vegetables (1 portion = a glass of vegetables or half a glass of vegetable juice) | 36.5% | 43.4% | OMN < VEGE * 0.481 ± 0.695 vs. 0.652 ± 0.815 | 0.029 |
| 1–2 portion(s) (44.9%) 3 portions (26.5%) 4–6 portions (13.9%) | 1–2 portion(s) (27.9%) 3 portions (29.7%) 4–6 portions (28.8%) | |||
| Fruits (1 portion = 1 medium piece or half glass of fruit juice) | 34.2% | 35.9% | OMN < VEGE * 0.430 ± 0.651 vs. 0.491 ± 0.718 | 0.476 |
| <1 portion (16.7%) 1–2 portion(s) (51.5%) 3 portions (22.2%) 4–6 portions (6.5%) | <1 portion (15.2%) 1–2 portion(s) (49.3%) 3 portions (20.7%) 4–6 portions (9.7%) | |||
| Legumes (1 portion = half a cup of legumes) | 23.5% | 44.1% | OMN < VEGE * 0.256 ± 0.482 vs. 0.545 ± 0.678 | <0.001 |
| <1 portion (69.8%) 1–2 portion(s) (18.4%) 3 portions (3.5%) | <1 portion (36.7%) 1–2 portion(s) (40.4%) 3 portions (13.3%) | |||
| Whole grain products (1 portion = 1 slice of bread or a half cup of groats | 34.4% | 34.7% | OMN > VEGE * 0.381 ± 0.559 vs. 0.379 ± 0.548 | 0.977 |
| <1 portion (19.6%) 1–2 portion(s) (37.8%) 3 portions (23%) | <1 portion (19.2%) 1–2 portion(s) (35.5%) 3 portions (23.8%) | |||
| Dairy products or plant-based substitutes 1 portion = glass of milk | 42.3% | 57.5% | OMN < VEGE * 0.515 ± 0.660 vs. 0.676 ± 0.650 | 0.002 |
| <1 portion (24.2%) 1–2 portion(s) (44.7%) 3 portions (21.8%) | <1 portion (15.5%) 1–2 portion(s) (40.2%) 3 portions (27.4%) | |||
| Nuts, seeds 1 portion = ¼ cup of nuts | 32.7% | 29.6% | OMN > VEGE * 0.372 ± 0.569 vs. 0.350 ± 0.581 | 0.512 |
| <1 portion (52.9%) 1–2 portion(s) (33.3%) 3 portions (7.2%) | <1 portion (52.8%) 1–2 portion(s) (33.2%) 3 portions (7.9%) | |||
| Meat (only in the OMN group) 1 portion= 1 slice of ham or ½ chicken breast | 22.1% | – | – | – |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kwiatkowska, I.; Olszak, J.; Formanowicz, P.; Formanowicz, D. Dietary Habits and Lifestyle, Including Cardiovascular Risk among Vegetarians and Omnivores during the COVID-19 Pandemic in the Polish Population. Nutrients 2023, 15, 442. https://doi.org/10.3390/nu15020442
Kwiatkowska I, Olszak J, Formanowicz P, Formanowicz D. Dietary Habits and Lifestyle, Including Cardiovascular Risk among Vegetarians and Omnivores during the COVID-19 Pandemic in the Polish Population. Nutrients. 2023; 15(2):442. https://doi.org/10.3390/nu15020442
Chicago/Turabian StyleKwiatkowska, Izabela, Jakub Olszak, Piotr Formanowicz, and Dorota Formanowicz. 2023. "Dietary Habits and Lifestyle, Including Cardiovascular Risk among Vegetarians and Omnivores during the COVID-19 Pandemic in the Polish Population" Nutrients 15, no. 2: 442. https://doi.org/10.3390/nu15020442