
Waist Circumference Trajectories in Relation to Blood Pressure and the Risk of Hypertension in Chinese Adults
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Participants
2.3. Measurement of Variables
2.4. Measurement of Covariates
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics
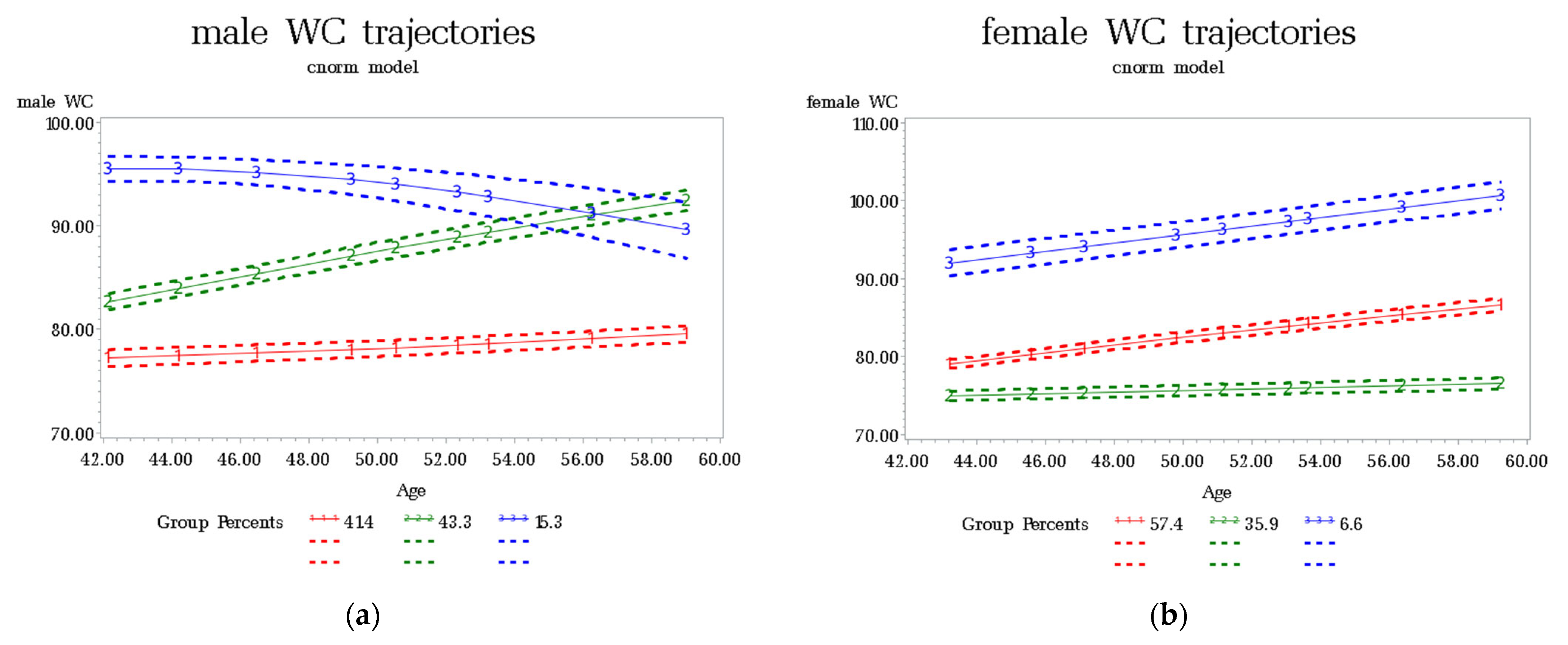
3.2. Trajectories of WC
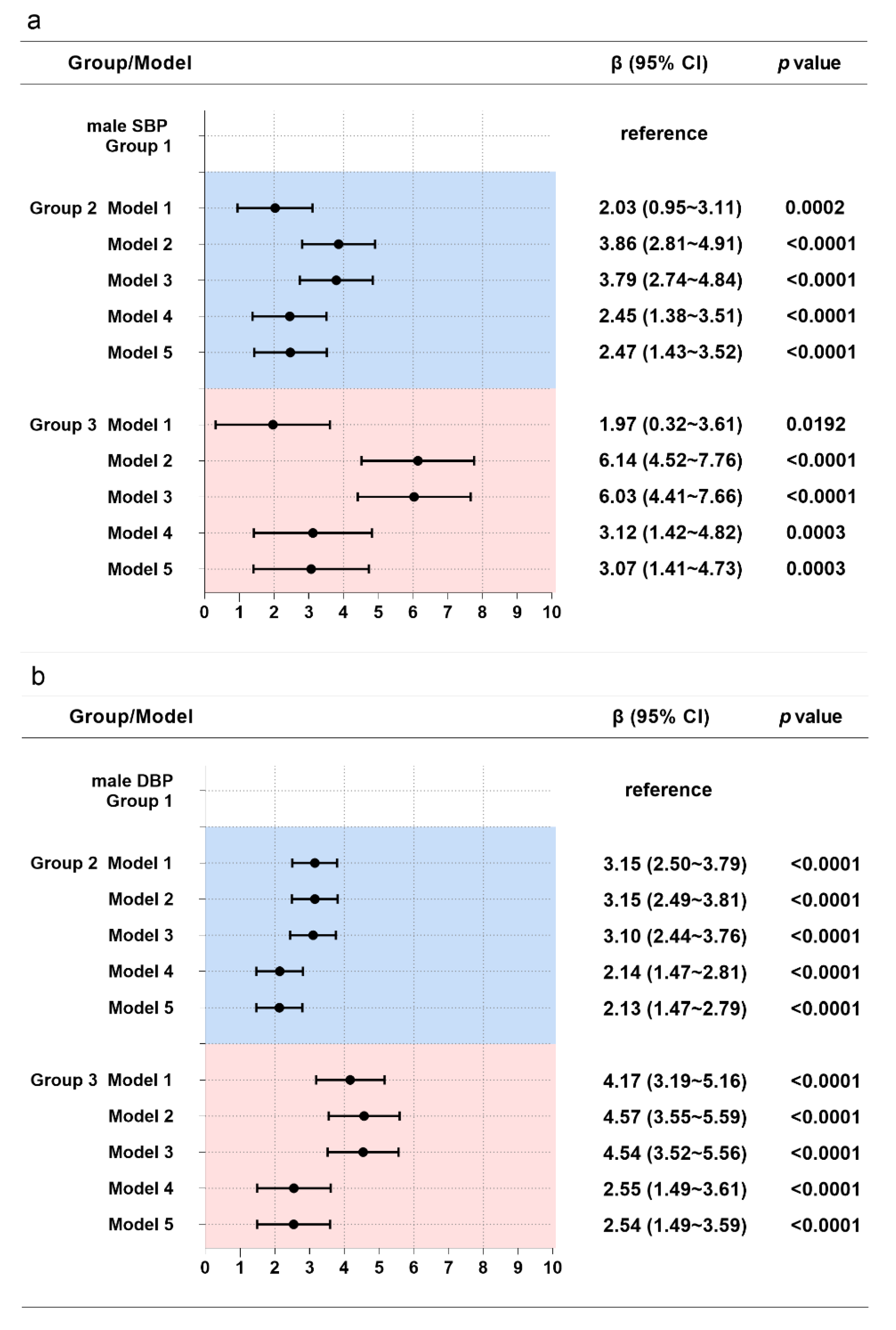
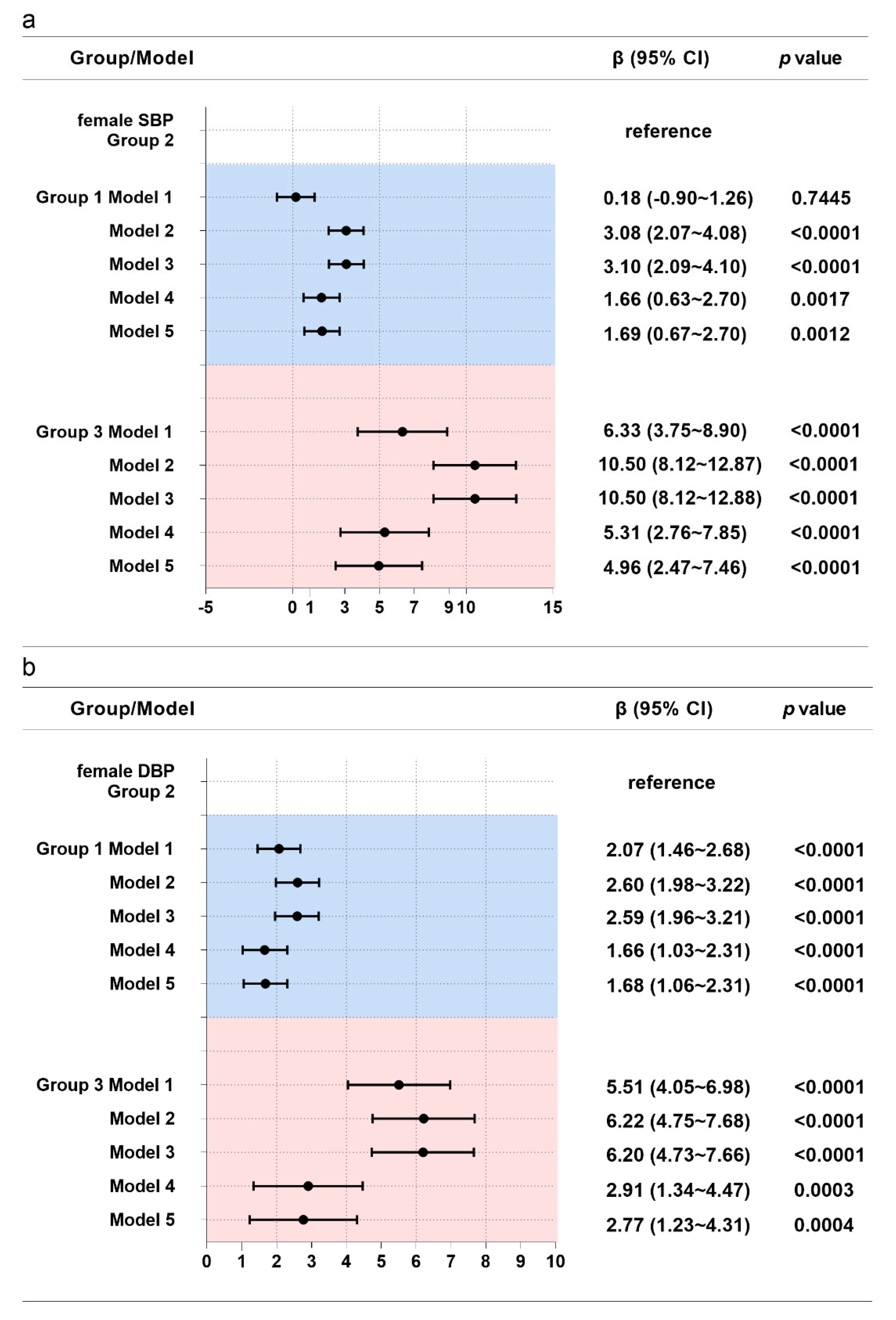
3.3. Associations between WC Trajectories and Blood Pressure
3.4. Associations between WC Trajectories and Hypertension
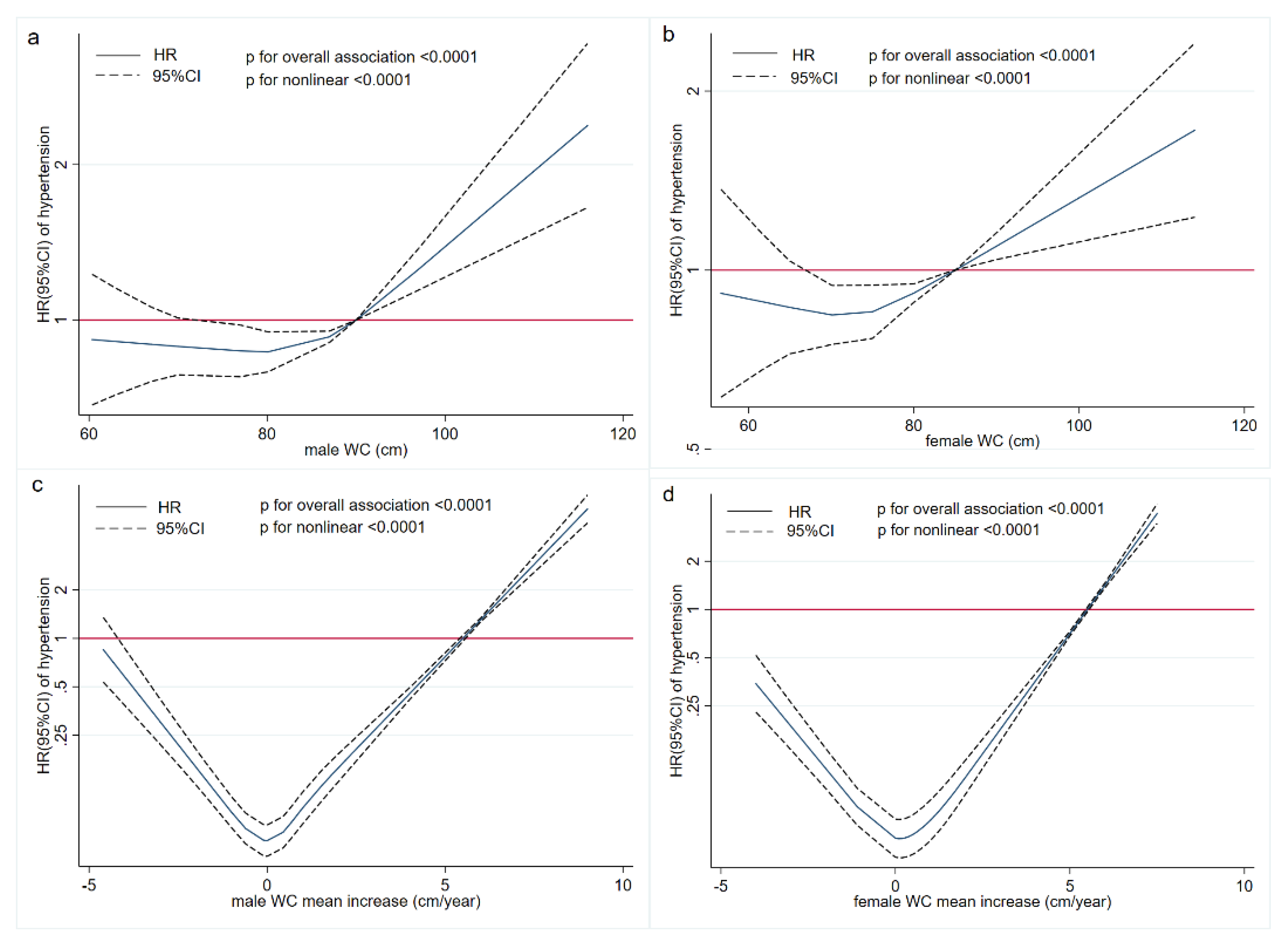
3.5. Exposure-Response Relationships between WC and Hypertension
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization (WHO). Hypertension. 2021. Available online: https://www.who.int/news-room/fact-sheets/detail/hypertension (accessed on 9 August 2022).
- Report on Nutrition and Chronic Diseases in China; Acta Nutrimenta Sinica: Beijing, China, 2020.
- Stanaway, J.D.; Afshin, A.; Gakidou, S.L.S.E.; Abate, D.; Abate, K.H. Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1923–1994. [Google Scholar]
- Wu, X.; Li, B.; Lin, W.; Huang, L.; Wang, X.; Fu, L.; Li, B.; Wang, P. The association between obesity indices and hypertension: Which index is the most notable indicator of hypertension in different age groups stratified by sex? Clin. Exp. Hypertens. 2019, 41, 373–380. [Google Scholar] [CrossRef] [PubMed]
- Nurdiantami, Y.; Watanabe, K.; Tanaka, E.; Pradono, J.; Anme, T. Association of general and central obesity with hypertension. Clin. Nutr. 2018, 37, 1259–1263. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klein, S.; Allison, D.B.; Heymsfield, S.B.; Kelley, D.E.; Leibel, R.L.; Nonas, C.; Kahn, A.R. Waist circumference and cardiometabolic risk: A consensus statement from Shaping America’s Health: Association for Weight Management and Obesity Prevention; NAASO, The Obesity Society; the American Society for Nutrition; and the American Diabetes Association. Am. J. Clin. Nutr. 2007, 85, 1197–1202. [Google Scholar]
- Zhang, X.; Yao, S.; Sun, G.; Yu, S.; Sun, Z.; Zheng, L.; Xu, C.; Li, J.; Sun, Y. Total and abdominal obesity among rural Chinese women and the association with hypertension. Nutrition 2012, 28, 46–52. [Google Scholar] [CrossRef]
- Foulds, H.J.A.; Bredin, S.S.D.; Warburton, D.E.R. The relationship between hypertension and obesity across different ethnicities. J. Hypertens. 2012, 30, 359–367. [Google Scholar] [CrossRef]
- Shrestha, R.; Upadhyay, S.K.; Khatri, B.; Bhattarai, J.R.; Kayastha, M.; Upadhyay, M.P. BMI, waist to height ratio and waist circumference as a screening tool for hypertension in hospital outpatients: A cross-sectional, non-inferiority study. BMJ Open 2021, 11, e50096. [Google Scholar] [CrossRef]
- Wildman, R.P.; Gu, D.; Reynolds, K.; Duan, X.; Wu, X.; He, J. Are waist circumference and body mass index independently associated with cardiovascular disease risk in Chinese adults. Am. J. Clin. Nutr. 2005, 82, 1195–1202. [Google Scholar] [CrossRef] [Green Version]
- Luo, W.; Guo, Z.; Hu, X.; Zhou, Z.; Ming, W.; Zhang, L.; Liu, J. A prospective study on association between 2 years change of waist circumference and incident hypertension in Han Chinese. Int. J. Cardiol. 2012, 167, 2781–2785. [Google Scholar] [CrossRef]
- Zhao, Y.; Zhang, M.; Luo, X.; Wang, C.; Li, L.; Zhang, L.; Wang, B.; Ren, Y.; Zhou, J.; Han, C.; et al. Association of 6-year waist circumference gain and incident hypertension. Heart 2017, 103, 1347–1352. [Google Scholar] [CrossRef]
- Sun, H.; Zheng, M.; Wu, S.; Chen, M.; Cai, J.; Yang, X. Waist circumference and incidence of hypertension in Chinese adults. Herz 2017, 42, 677–683. [Google Scholar] [CrossRef] [PubMed]
- Adegbija, O.; Hoy, W.; Wang, Z. Prediction of cardiovascular disease risk using waist circumference among Aboriginals in a remote Australian community. BMC Public Health 2015, 15, 57. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Hoy, W. Waist circumference, body mass index, hip circumference and waist-to-hip ratio as predictors of cardiovascular disease in Aboriginal people. Eur. J. Clin. Nutr. 2004, 58, 888–893. [Google Scholar] [CrossRef] [Green Version]
- Cheng, C.; Li, Y.; Ma, W.; Jia, C. Trajectories of waist circumference during young adulthood and incident hypertension: The China Health and Nutrition Survey. J. Hum. Hypertens. 2021, 36, 767–774. [Google Scholar] [CrossRef] [PubMed]
- Ahanchi, N.S.; Tamehri Zadeh, S.S.; Khalili, D.; Azizi, F.; Hadaegh, F. Sex specific trajectories of central adiposity, lipid indices, and glucose level with incident hypertension: 12 years Follow-up in Tehran lipid and glucose study. J. Transl. Med. 2021, 19, 84. [Google Scholar] [CrossRef]
- Wang, L.; Lee, Y.; Wu, Y.; Zhang, X.; Jin, C.; Huang, Z.; Wang, Y.; Wang, Z.; Kris-Etherton, P.; Wu, S.; et al. A prospective study of waist circumference trajectories and incident cardiovascular disease in China: The Kailuan Cohort Study. Am. J. Clin. Nutr. 2021, 113, 338–347. [Google Scholar] [CrossRef]
- Zhang, B.; Zhai, F.Y.; Du, S.F.; Popkin, B.M. The China Health and Nutrition Survey, 1989–2011. Obes. Rev. 2014, 15, 2–7. [Google Scholar] [CrossRef] [Green Version]
- Popkin, B.M.; Du, S.; Zhai, F.; Zhang, B. Cohort Profile: The China Health and Nutrition Survey--monitoring and understanding socio-economic and health change in China, 1989–2011. Int. J. Epidemiol. 2010, 39, 1435–1440. [Google Scholar] [CrossRef] [Green Version]
- WS/T 428-2013; Criteria of Weight for Adults. Standards Press of China: Beijing, China, 2013.
- Writing Group of Chinese Guidelines for the Management of Hypertension. 2018 Chinese guidelines for the management of hypertension. Chin. J. Cardiovasc. Med. 2019, 24, 24–56. [Google Scholar]
- Roeder, B.L.J.D. A SAS Procedure Based on Mixture Models for Estimating Developmental Trajectories. Soc. Methods Res. 2001, 29, 374–393. [Google Scholar]
- Proust-Lima, C.; Letenneur, L.; Jacqmin-Gadda, H. A nonlinear latent class model for joint analysis of multivariate longitudinal data and a binary outcome. Stat. Med. 2007, 26, 2229–2245. [Google Scholar] [CrossRef] [PubMed]
- Jones, B.L.; Nagin, D.S. Advances in Group-Based Trajectory Modeling and an SAS Procedure for Estimating Them. Soc. Methods Res. 2007, 35, 542–571. [Google Scholar] [CrossRef] [Green Version]
- van der Nest, G.; Passos, V.L.; Candel, M.J.; van Breukelen, G.J.P. An overview of mixture modelling for latent evolutions inlongitudinal data: Modelling approaches, fit statistics and software. Adv. Life Course Res. 2020, 43, 100323. [Google Scholar] [CrossRef]
- Nagin, D.S.; Odgers, C.L. Group-based trajectory modeling in clinical research. Annu. Rev. Clin. Psychol. 2010, 6, 109–138. [Google Scholar] [CrossRef]
- Nagin, D.S. Group-Based Trajectory Modeling: An Overview. Ann. Nutr. Metab. 2014, 65, 205–210. [Google Scholar] [CrossRef]
- Qu, Y.; Niu, H.; Li, L.; Li, M.; Yan, S.; Li, M.; Jiang, S.; Ma, X.; Li, B.; Wu, H. Analysis of Dose-response Relationship between BMI and Hypertension in Northeastern China Using Restricted Cubic Spline Functions. Sci. Rep. 2019, 9, 18208. [Google Scholar] [CrossRef] [Green Version]
- Frank, B.; Hu, M.J.S.E. Dietary Fat and Coronary Heart Disease: A Comparison of Approaches for Adjusting for Total Energy Intake and Modeling Repeated Dietary Measurements. Am. J. Epidemiol. 1999, 149, 531–540. [Google Scholar]
- Mikkelsen, B.; Williams, J.; Rakovac, I.; Wickramasinghe, K.; Hennis, A.; Shin, H.; Farmer, M.; Weber, M.; Berdzuli, N.; Borges, C.; et al. Life course approach to prevention and control of non-communicable diseases. BMJ 2019, 364, l257. [Google Scholar] [CrossRef] [Green Version]
- Lynch, J.; Smith, G.D. A life course approach to chronic disease epidemiology. Annu. Rev. Public Health 2005, 26, 1–35. [Google Scholar] [CrossRef] [Green Version]
- Ben-Shlomo, Y.; Kuh, D. A life course approach to chronic disease epidemiology: Conceptual models, empirical challenges and interdisciplinary perspectives. Int. J. Epidemiol. 2002, 31, 285–293. [Google Scholar] [CrossRef]
- Dzudie, A.; Njedock, N.; Boombhi, J.; Ba, H.; Amougou, S.N.; Kamdem, F.; Barche, B.; Nzali, A.; Njomou, A.; Ngwasiri, C.; et al. Association between measures of adiposity and blood pressure levels in adult Cameroonians. Health Sci. Rep. 2021, 4, e259. [Google Scholar] [CrossRef] [PubMed]
- Sun, J.Y.; Ma, Y.X.; Liu, H.L.; Qu, Q.; Cheng, C.; Kong, X.Q.; Huang, W.J.; Sun, W. High waist circumference is a risk factor of new-onset hypertension: Evidence from the China Health and Retirement Longitudinal Study. J. Clin. Hypertens. 2022, 24, 320–328. [Google Scholar] [CrossRef] [PubMed]
- Araujo, J.; Barros, H.; Ramos, E.; Li, L. Trajectories of total and central adiposity throughout adolescence and cardiometabolic factors in early adulthood. Int. J. Obes. 2016, 40, 1899–1905. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stevens, J.; Katz, E.G.; Huxley, R.R. Associations between gender, age and waist circumference. Eur. J. Clin. Nutr. 2010, 64, 6–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mathur, P.; Ostadal, B.; Romeo, F.; Mehta, J.L. Gender-Related Differences in Atherosclerosis. Cardiovasc. Drugs Ther. 2015, 29, 319–327. [Google Scholar] [CrossRef] [PubMed]
- Fu, W.; Cao, S.; Liu, B.; Li, H.; Song, F.; Gan, Y.; Li, W.; Opoku, S.; Yan, S.; Yue, W.; et al. Association of general and central adiposity with blood pressure among Chinese adults. J. Hypertens. 2018, 36, 2406–2413. [Google Scholar] [CrossRef] [Green Version]
- Fan, H.; Zhang, X. Body mass index trajectory across childhood and subsequent risk of elevated blood pressure. J. Clin. Hypertens. 2020, 22, 1902–1907. [Google Scholar] [CrossRef]
- Lu, Y.K.; Dong, J.; Sun, Y.; Hu, L.K.; Liu, Y.H.; Chu, X.; Yan, Y.X. Gender-specific predictive ability for the risk of hypertension incidence related to baseline level or trajectories of adiposity indices: A cohort study of functional community. Int. J. Obes. 2022, 46, 1036–1043. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Baseline Characteristics | Male (n = 5686) | Female (n = 6199) | Overall (n = 11,885) |
|---|---|---|---|
| Age, year (mean [SD]) | 42.72 (14.15) | 43.58 (13.66) | 43.17 (13.91) |
| Follow-up time, year (mean [SD]) | 14.45 (6.39) | 14.55 (6.60) | 14.50 (6.50) |
| Education level, n (%) | |||
| Primary school and below | 2086 (36.69) | 3264 (52.65) | 5350 (45.01) |
| Middle school | 2028 (35.67) | 1665 (26.86) | 3693 (31.07) |
| High school and above | 1572 (27.64) | 1270 (20.49) | 2842 (23.92) |
| Geographic region, n (%) | |||
| Rural | 3798 (66.80) | 4019 (64.83) | 7817 (65.77) |
| Urban | 1888 (33.20) | 2180 (35.17) | 4068 (34.23) |
| annual household income per capita, yuan/year (median [IQR]) | 2292.96 (976.43~5375.76) | 2349.88 (962.75~5703.42) | 2328.40 (969.98~5558.36) |
| Physical activity, METs/wk (median [IQR]) | 169.55 (81.03~315.00) | 189.72 (93.88~347.11) | 180.33 (86.63~332.30) |
| Smoking, n (%) | |||
| Nonsmoker | 2193 (38.57) | 5939 (95.81) | 8132 (68.42) |
| Current smoker | 3493 (61.43) | 260 (4.19) | 3753 (31.58) |
| drinking, n (%) | |||
| Nondrinker | 2050 (36.05) | 5518 (89.01) | 7568 (63.68) |
| Current drinker | 3636 (63.95) | 681 (10.99) | 4317 (36.32) |
| K intake, mg/d (median [IQR]) | 1746.27 (1405.66~2144.02) | 1535.64 (1232.71~1925.30) | 1628.76 (1303.43~2041.04) |
| Na intake, mg/d (median [IQR]) | 5805.78 (3806.58~8637.20) | 5025.20 (3272.47~7416.11) | 5386.81 (3516.91~7981.71) |
| BMI, kg/m2 (mean [SD]) | 22.56 (3.06) | 22.85 (3.36) | 22.71 (3.22) |
| WC, cm (mean [SD]) | 80.16 (10.02) | 77.45 (9.70) | 78.75 (9.95) |
| SBP, mmHg (mean [SD]) | 120.02 (15.41) | 116.22 (17.49) | 118.04 (16.64) |
| DBP, mmHg (mean [SD]) | 78.39 (10.33) | 75.56 (10.74) | 76.92 (10.64) |
| Gender | Model | Trajectory Groups | ||||
|---|---|---|---|---|---|---|
| Male | Group 1 (n = 1929) | Group 2 (n = 2046) | Group 3 (n = 517) | |||
| HR | HR (95% CI) | p | HR (95% CI) | p | ||
| Model 1 | 1 | 1.11 (1.02~1.21) | 0.017 | 1.48 (1.29~1.69) | <0.0001 | |
| Model 2 | 1 | 1.38 (1.26~1.51) | <0.0001 | 1.78 (1.54~2.06) | <0.0001 | |
| Model 3 | 1 | 1.37 (1.25~1.50) | <0.0001 | 1.75 (1.51~2.02) | <0.0001 | |
| Model 4 | 1 | 1.16 (1.05~1.27) | 0.003 | 1.26 (1.08~1.47) | 0.003 | |
| Model 5 | 1 | 1.16 (1.06~1.28) | 0.002 | 1.29 (1.10~1.50) | 0.001 | |
| Female | Group 2 (n = 1548) | Group 1 (n = 3398) | Group 3 (n = 213) | |||
| HR | HR (95% CI) | p | HR (95% CI) | p | ||
| Model 1 | 1 | 1.07 (0.98~1.17) | 0.137 | 1.72 (1.42~2.09) | <0.0001 | |
| Model 2 | 1 | 1.41 (1.28~1.55) | <0.0001 | 2.83 (2.31~3.46) | <0.0001 | |
| Model 3 | 1 | 1.41 (1.31~1.59) | <0.0001 | 2.85 (2.33~3.49) | <0.0001 | |
| Model 4 | 1 | 1.14 (1.03~1.26) | 0.011 | 1.55 (1.24~1.93) | <0.0001 | |
| Model 5 | 1 | 1.14 (1.03~1.26) | 0.012 | 1.47 (1.17~1.84) | 0.001 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, Q.; Song, X.; Du, S.; Du, W.; Su, C.; Zhang, J.; Zhang, X.; Zhang, B.; Wang, H. Waist Circumference Trajectories in Relation to Blood Pressure and the Risk of Hypertension in Chinese Adults. Nutrients 2022, 14, 5260. https://doi.org/10.3390/nu14245260
Wang Q, Song X, Du S, Du W, Su C, Zhang J, Zhang X, Zhang B, Wang H. Waist Circumference Trajectories in Relation to Blood Pressure and the Risk of Hypertension in Chinese Adults. Nutrients. 2022; 14(24):5260. https://doi.org/10.3390/nu14245260
Chicago/Turabian StyleWang, Qi, Xiaoyun Song, Shufa Du, Wenwen Du, Chang Su, Jiguo Zhang, Xiaofan Zhang, Bing Zhang, and Huijun Wang. 2022. "Waist Circumference Trajectories in Relation to Blood Pressure and the Risk of Hypertension in Chinese Adults" Nutrients 14, no. 24: 5260. https://doi.org/10.3390/nu14245260