
Comparing the Usability of the Web-Based 24-h Dietary Recall R24W and ASA24-Canada-2018 among French-Speaking Adults from Québec

Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Study Design
2.3. Dietary Recalls Tools
2.4. Outcome Measurements
2.4.1. Usability
2.4.2. Dietary Intakes
2.4.3. Health Literacy
2.4.4. Socio-Demographic Characteristics
2.5. Sample Size Estimation
2.6. Statistical Analyses
3. Results
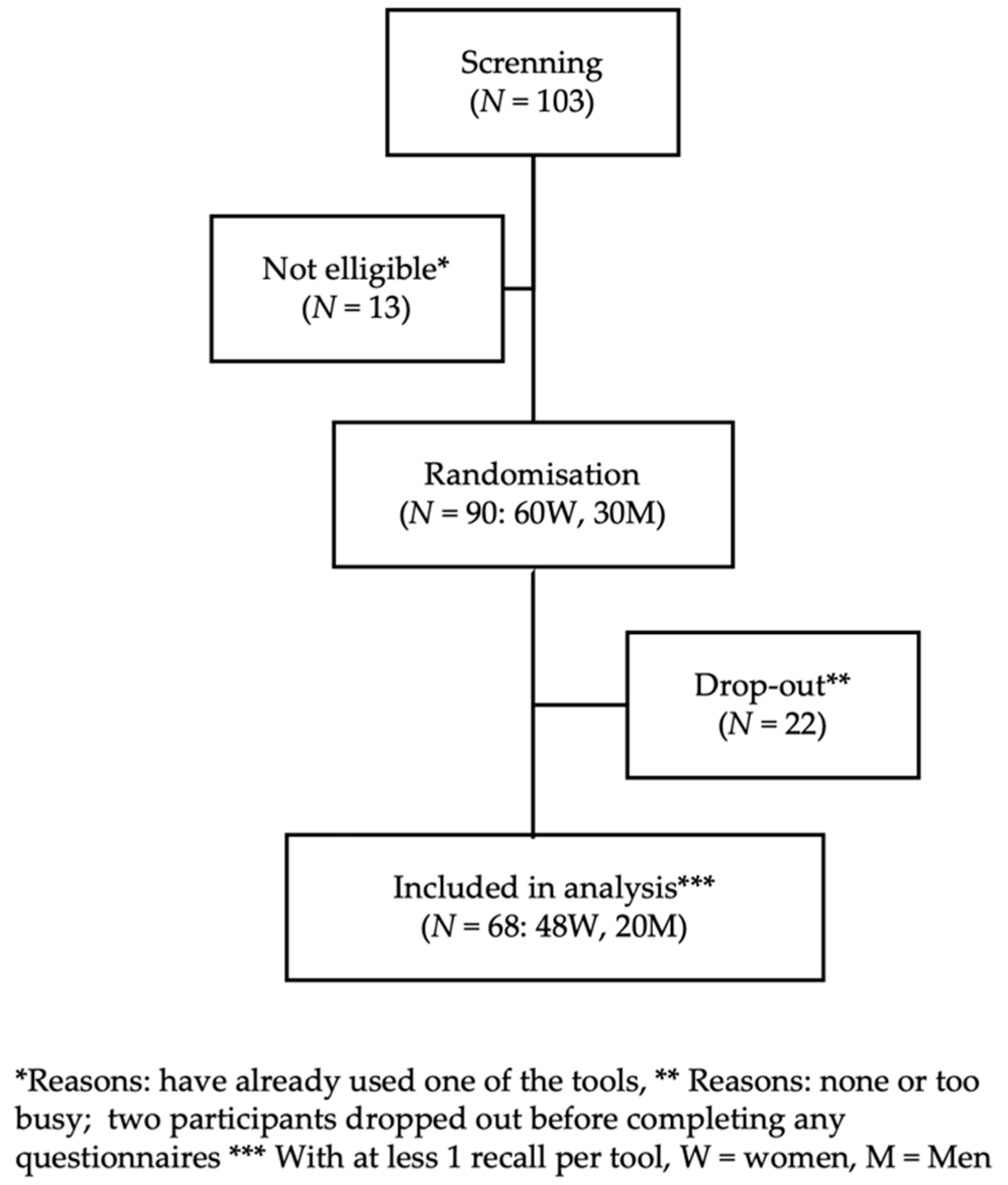
3.1. Participant Characteristics
3.2. Usability
3.3. Dietary Intakes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Schatzkin, A.; Kipnis, V.; Carroll, R.J.; Midthune, D.; Subar, A.F.; Bingham, S.; Schoeller, D.A.; Troiano, R.P.; Freedman, L.S. A comparison of a food frequency questionnaire with a 24-hour recall for use in an epidemiological cohort study: Results from the biomarker-based Observing Protein and Energy Nutrition (OPEN) study. Int. J. Epidemiol. 2003, 32, 1054–1062. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Freedman, L.S.; Commins, J.M.; Moler, J.E.; Willett, W.; Tinker, L.F.; Subar, A.F.; Spiegelman, D.; Rhodes, D.; Potischman, N.; Neuhouser, M.L.; et al. Pooled results from 5 validation studies of dietary self-report instruments using recovery biomarkers for potassium and sodium intake. Am. J. Epidemiol. 2015, 181, 473–487. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Subar, A.F.; Kipnis, V.; Troiano, R.P.; Midthune, D.; Schoeller, D.A.; Bingham, S.; Sharbaugh, C.O.; Trabulsi, J.; Runswick, S.; Ballard-Barbash, R.; et al. Using intake biomarkers to evaluate the extent of dietary misreporting in a large sample of adults: The OPEN study. Am. J. Epidemiol. 2003, 158, 1–13. [Google Scholar] [CrossRef]
- Illner, A.K.; Freisling, H.; Boeing, H.; Huybrechts, I.; Crispim, S.P.; Slimani, N. Review and evaluation of innovative technologies for measuring diet in nutritional epidemiology. Int. J. Epidemiol. 2012, 41, 1187–1203. [Google Scholar] [CrossRef] [Green Version]
- Timon, C.M.; van den Barg, R.; Blain, R.J.; Kehoe, L.; Evans, K.; Walton, J.; Flynn, A.; Gibney, E.R. A review of the design and validation of web- and computer-based 24-h dietary recall tools. Nutr. Res. Rev. 2016, 29, 268–280. [Google Scholar] [CrossRef] [PubMed]
- Eldridge, A.L.; Piernas, C.; Illner, A.K.; Gibney, M.J.; Gurinovic, M.A.; de Vries, J.H.M.; Cade, J.E. Evaluation of New Technology-Based Tools for Dietary Intake Assessment-An ILSI Europe Dietary Intake and Exposure Task Force Evaluation. Nutrients 2018, 11, 55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gazan, R.; Vieux, F.; Mora, S.; Havard, S.; Dubuisson, C. Potential of existing online 24-h dietary recall tools for national dietary surveys. Public Health Nutr. 2021, 24, 5361–5386. [Google Scholar] [CrossRef] [PubMed]
- Jacques, S.; Lemieux, S.; Lamarche, B.; Laramee, C.; Corneau, L.; Lapointe, A.; Tessier-Grenier, M.; Robitaille, J. Development of a Web-Based 24-h Dietary Recall for a French-Canadian Population. Nutrients 2016, 8, 724. [Google Scholar] [CrossRef] [Green Version]
- Subar, A.F.; Kirkpatrick, S.I.; Mittl, B.; Zimmerman, T.P.; Thompson, F.E.; Bingley, C.; Willis, G.; Islam, N.G.; Baranowski, T.; McNutt, S.; et al. The Automated Self-Administered 24-hour dietary recall (ASA24): A resource for researchers, clinicians, and educators from the National Cancer Institute. J. Acad. Nutr. Diet. 2012, 112, 1134–1137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raper, N.; Perloff, B.; Ingwersen, L.; Steinfeldt, L.; Anand, J. An overview of USDA’s Dietary Intake Data System. J. Food Compos. Anal. 2004, 17, 545–555. [Google Scholar] [CrossRef]
- National Cancer Institute. ASA24® Respondent Website Methodology|EGRP/DCCPS/NCI/NIH. Available online: https://epi.grants.cancer.gov/asa24/respondent/methodology.html (accessed on 19 October 2022).
- Lafrenière, J.; Lamarche, B.; Laramee, C.; Robitaille, J.; Lemieux, S. Validation of a newly automated web-based 24-hour dietary recall using fully controlled feeding studies. BMC Nutr. 2017, 3, 34. [Google Scholar] [CrossRef] [Green Version]
- Kirkpatrick, S.I.; Subar, A.F.; Douglass, D.; Zimmerman, T.P.; Thompson, F.E.; Kahle, L.L.; George, S.M.; Dodd, K.W.; Potischman, N. Performance of the Automated Self-Administered 24-hour Recall relative to a measure of true intakes and to an interviewer-administered 24-h recall. Am. J. Clin. Nutr. 2014, 100, 233–240. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- International Organization for Standardization. ISO—ISO 9241-11:2018—Ergonomics of Human-System Interaction—Part 11: Usability: Definitions and Concepts. Available online: https://www.iso.org/standard/63500.html (accessed on 22 July 2022).
- Maramba, I.; Chatterjee, A.; Newman, C. Methods of usability testing in the development of eHealth applications: A scoping review. Int. J. Med. Inform. 2019, 126, 95–104. [Google Scholar] [CrossRef] [PubMed]
- Grossman, T.; Fitzmaurice, G.; Attar, R. A survey of software learnability: Metrics, methodologies and guidelines. In Proceedings of the Sigchi Conference on Human Factors in Computing Systems, Boston, MA, USA, 4–9 April 2009; pp. 649–658. [Google Scholar]
- National Cancer Institute. Examining the Association between Diet as an INDEPENDENT Variable & a Dependent Variable|Dietary Assessment Primer. Available online: https://dietassessmentprimer.cancer.gov/approach/independent.html (accessed on 25 July 2022).
- Brooke, J. SUS-A quick and dirty usability scale. In Usability Evaluation in Industry; Jordan, P.W., Thomas, B., Weerdmeester, B.A., McClelland, I.L., Eds.; Taylor and Francis: London, UK, 1996; pp. 189–194. [Google Scholar]
- Peres, S.C.; Pham, T.; Phillips, R. Validation of the System Usability Scale (SUS) SUS in the Wild. Proc. Hum. Factors Ergon. Soc. Annu. Meet. 2013, 57, 192–196. [Google Scholar] [CrossRef]
- Mansfield, E.D.; Wahba, R.; Gillis, D.E.; Weiss, B.D.; L’Abbe, M. Canadian adaptation of the Newest Vital Sign(c), a health literacy assessment tool. Public Health Nutr. 2018, 21, 2038–2045. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weiss, B.D.; Mays, M.Z.; Martz, W.; Castro, K.M.; DeWalt, D.A.; Pignone, M.P.; Mockbee, J.; Hale, F.A. Quick assessment of literacy in primary care: The newest vital sign. Ann. Fam. Med. 2005, 3, 514–522. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gilsing, A.; Mayhew, A.J.; Payette, H.; Shatenstein, B.; Kirkpatrick, S.I.; Amog, K.; Wolfson, C.; Kirkland, S.; Griffith, L.E.; Raina, P. Validity and Reliability of a Short Diet Questionnaire to Estimate Dietary Intake in Older Adults in a Subsample of the Canadian Longitudinal Study on Aging. Nutrients 2018, 10, 1522. [Google Scholar] [CrossRef] [Green Version]
- Gianfrancesco, C.; Darwin, Z.; McGowan, L.; Smith, D.M.; Haddrill, R.; Carter, M.; Scott, E.M.; Alwan, N.A.; Morris, M.A.; Albar, S.A.; et al. Exploring the Feasibility of Use of An Online Dietary Assessment Tool (myfood24) in Women with Gestational Diabetes. Nutrients 2018, 10, 1147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bangor, A.; Kortum, P.; Miller, J. Determining what individual SUS scores mean: Adding an adjective rating scale. J. Usabil. Stud. 2009, 4, 114–123. [Google Scholar]
- Hopstock, L.A.; Medin, A.C.; Skeie, G.; Henriksen, A.; Lundblad, M.W. Evaluation of a Web-Based Dietary Assessment Tool (myfood24) in Norwegian Women and Men Aged 60–74 Years: Usability Study. JMIR Form. Res. 2022, 6, e35092. [Google Scholar] [CrossRef] [PubMed]
- Threapleton, D.E.; Beer, S.L.; Foley, D.J.; Gibson, L.E.; Trevillion, S.; Burke, D.; Wheatstone, P.; Gath, J.; Hex, N.; Setters, J.; et al. Usability of myfood24 Healthcare and Mathematical Diet Optimisation in Clinical Populations: A Pilot Feasibility Randomised Controlled Trial. Nutrients 2022, 14, 1768. [Google Scholar] [CrossRef] [PubMed]
- Albar, S.A.; Carter, M.C.; Alwan, N.A.; Evans, C.E.L.; Cade, J.E. Formative evaluation of the usability and acceptability of myfood24 among adolescents: A UK online dietary assessments tool. BMC Nutr. 2015, 1, 29. [Google Scholar] [CrossRef] [Green Version]
- Kupis, J.; Johnson, S.; Hallihan, G.; Olstad, D.L. Assessing the Usability of the Automated Self-Administered Dietary Assessment Tool (ASA24) among Low-Income Adults. Nutrients 2019, 11, 132. [Google Scholar] [CrossRef] [PubMed]
- National Cancer Institute. ASA24-2020|EGRP/DCCPS/NCI/NIH. Available online: https://epi.grants.cancer.gov/asa24/respondent/2020.html (accessed on 25 May 2022).
- National Cancer Institute. ASA24® Frequently Asked Questions|EGRP/DCCPS/NCI/NIH. Available online: https://epi.grants.cancer.gov/asa24/resources/faq.html (accessed on 6 June 2022).


{kind=link}
| R24W | ASA24-Canada-2018 | |
|---|---|---|
| Developer | Université Laval, Quebec, Canada | US National Cancer Institute, adapted by Health Canada’s Food Directorate |
| App languages | Developed in French and translated in English | Developed in English and translated in French |
| Tutorial | Mandatory video | Written instructions |
| Steps | Modified version of the Automated Multiple-Pass Method (AMPM)
| Modified version of the AMPM
|
| Food identification |
|
|
| Food list |
|
|
| Integrated food composition database |
|
|
| Portions sizes |
|
|
| Data Reports |
|
|
| Characteristics | Participants | Dropouts | p Values |
|---|---|---|---|
| % | |||
| Sex | |||
| Female | 71 | 60 | 0.37 |
| Male | 29 | 40 | |
| Age in years | |||
| 18–30 | 43 | 45 | 0.50 |
| 31–50 | 43 | 50 | |
| ≥51 | 15 | 5 | |
| BMI in kg/m2 | |||
| Normal weight, <25 | 63 | 50 | 0.38 |
| Overweight, 25.0–29.9 | 23 | 22 | |
| Obese, ≥30 | 14 | 27 | |
| Education | |||
| Trade school, high school, or no diploma | 7 | 5 | 0.78 |
| CEGEP | 37 | 45 | |
| University | 56 | 50 | |
| Annual gross household income in $ CAD | |||
| <30,000 | 15 | 35 | 0.24 |
| 30,000–59,999 | 26 | 25 | |
| 60,000–99,999 | 25 | 15 | |
| 100,000 and more | 33 | 25 | |
| Health literacy categories | |||
| High likelihood of low health literacy (score 0–1) | 0 | 5 | 0.04 |
| Possible low health literacy (score 2–3) | 0 | 5 | |
| Adequate health literacy (score 4–6) | 100 | 90 | |
| R24W | ASA24-Canada-2018 | p Values | |
|---|---|---|---|
| SUS score 1, points (/100) | 81 ± 2 | 58 ± 2 | <0.0001 |
| Completion time 2, min | 14 (9–19) | 25 (16–34) | <0.0001 |
| Favorite tool reported 3, % | 84 | 16 | <0.0001 |
| R24W | ASA24-Canada-2018 | |
|---|---|---|
| Most appreciated features |
|
|
| Least appreciated features |
|
|
| R24W | ASA24-Canada-2018 | Differences | p Values | |
|---|---|---|---|---|
| Energy, kcal | 2282 ± 87 | 2252 ± 87 | 30 | 0.69 |
| Vegetables and fruits, servings 1 | 5.5 ± 0.4 | 6.1 ± 0.4 | 0.6 | 0.07 |
| Grain products, servings 1 | 5.0 ± 0.3 | 5.2 ± 0.3 | 0.2 | 0.74 |
| Milk and alternatives, servings 1 | 2.0 ± 0.1 | 1.9 ± 0.1 | 0.8 | 0.38 |
| Meat and alternatives, servings 1 | 2.2 ± 0.2 | 2.1 ± 0.2 | 0.1 | 0.42 |
| Total Fat, g | 93 ± 5 | 94 ± 5 | 1 | 0.81 |
| Saturated Fat, g | 32 ± 2 | 31 ± 2 | 1 | 0.44 |
| Carbohydrate, g | 266 ± 13 | 262 ± 13 | 4 | 0.68 |
| Protein, g | 91 ± 3 | 86 ± 3 | 5 | 0.11 |
| Fibers, g | 23 ± 2 | 23 ± 2 | 0 | 0.52 |
| Sodium, mg | 3201 ± 152 | 3341 ± 152 | 140 | 0.41 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Laramée, C.; Lemieux, S.; Robitaille, J.; Lamarche, B. Comparing the Usability of the Web-Based 24-h Dietary Recall R24W and ASA24-Canada-2018 among French-Speaking Adults from Québec. Nutrients 2022, 14, 4543. https://doi.org/10.3390/nu14214543
Laramée C, Lemieux S, Robitaille J, Lamarche B. Comparing the Usability of the Web-Based 24-h Dietary Recall R24W and ASA24-Canada-2018 among French-Speaking Adults from Québec. Nutrients. 2022; 14(21):4543. https://doi.org/10.3390/nu14214543
Chicago/Turabian StyleLaramée, Catherine, Simone Lemieux, Julie Robitaille, and Benoît Lamarche. 2022. "Comparing the Usability of the Web-Based 24-h Dietary Recall R24W and ASA24-Canada-2018 among French-Speaking Adults from Québec" Nutrients 14, no. 21: 4543. https://doi.org/10.3390/nu14214543