
The Association of Circulating Amino Acids and Dietary Inflammatory Potential with Muscle Health in Chinese Community-Dwelling Older People


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Participants
2.2. Demographic and Lifestyle Information
2.3. Dietary Assessment and Dietary Inflammatory Index (DII)
2.4. AA Assays
2.5. Assessment of Lean Muscle Mass
2.6. Assessment of Muscle Strength and Physical Performance
2.7. Statistical Analysis
3. Results
3.1. Association between DII and Baseline Serum AAs
3.2. Associations of DII and Serum AAs with Muscle Parameters at Baseline
3.3. Association of Baseline DII and Serum AAs with Change in Muscle Parameters over 4 Years
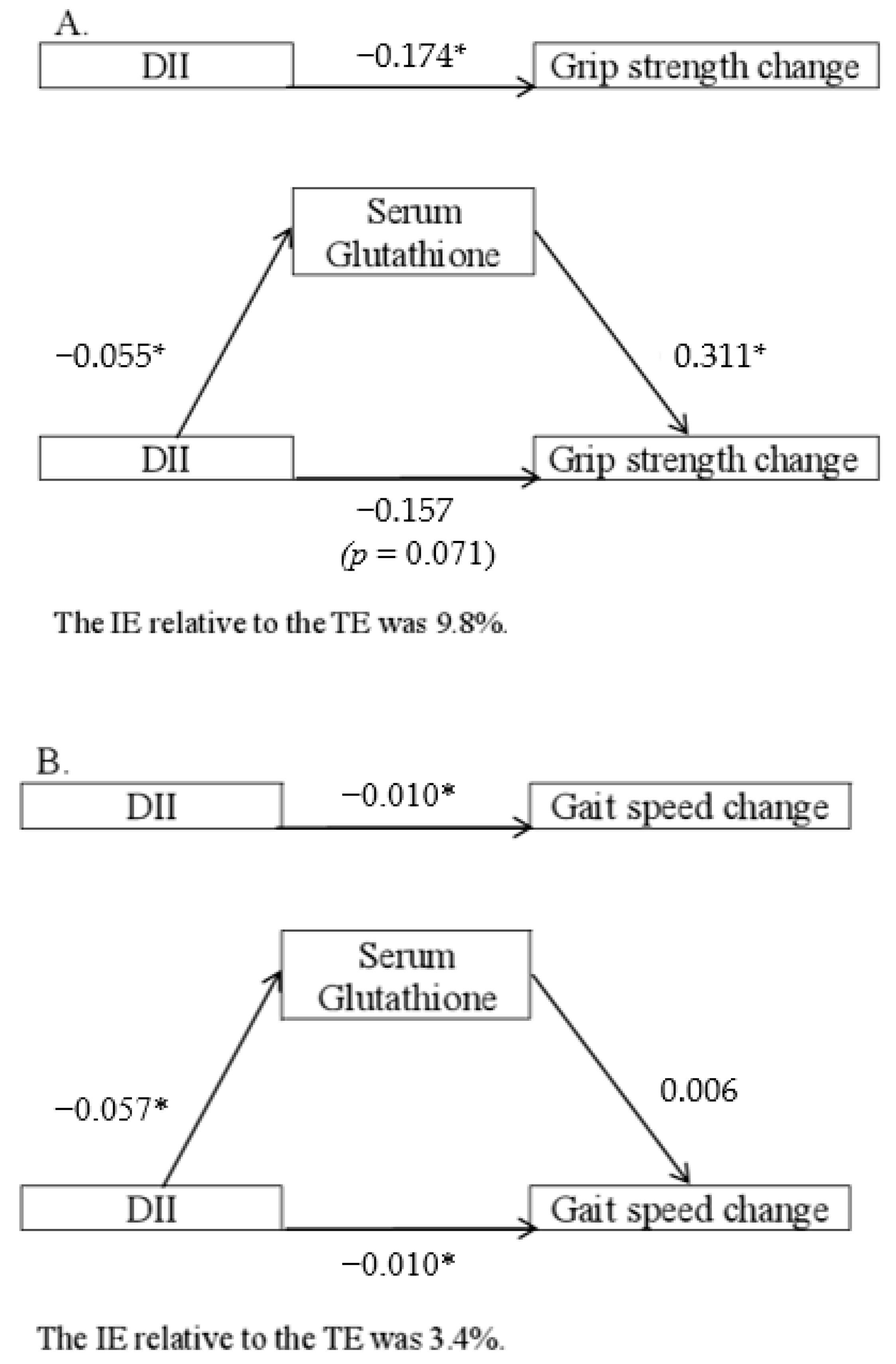
3.4. Mediation Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bianchi, L.; Ferrucci, L.; Cherubini, A.; Maggio, M.; Bandinelli, S.; Savino, E.; Brombo, G.; Zuliani, G.; Guralnik, J.M.; Landi, F.; et al. The Predictive Value of the EWGSOP Definition of Sarcopenia: Results from the InCHIANTI Study. J. Gerontol. A Biol. Sci. Med. Sci. 2016, 71, 259–264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kamei, Y.; Hatazawa, Y.; Uchitomi, R.; Yoshimura, R.; Miura, S. Regulation of Skeletal Muscle Function by Amino Acids. Nutrients 2020, 12, 261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jourdan, C.; Petersen, A.K.; Gieger, C.; Doring, A.; Illig, T.; Wang-Sattler, R.; Meisinger, C.; Peters, A.; Adamski, J.; Prehn, C.; et al. Body fat free mass is associated with the serum metabolite profile in a population-based study. PLoS ONE 2012, 7, e40009. [Google Scholar]
- Sayda, M.H.; Phillips, B.E.; Williams, J.P.; Greenhaff, P.L.; Wilkinson, D.J.; Smith, K.; Atherton, P.J. Associations between Plasma Branched Chain Amino Acids and Health Biomarkers in Response to Resistance Exercise Training Across Age. Nutrients 2020, 12, 3029. [Google Scholar] [CrossRef]
- Volpi, E.; Kobayashi, H.; Sheffield-Moore, M.; Mittendorfer, B.; Wolfe, R.R. Essential amino acids are primarily responsible for the amino acid stimulation of muscle protein anabolism in healthy elderly adults. Am. J. Clin. Nutr. 2003, 78, 250–258. [Google Scholar] [CrossRef]
- Fuchs, C.J.; Hermans, W.J.H.; Holwerda, A.M.; Smeets, J.S.J.; Senden, J.M.; van Kranenburg, J.; Gijsen, A.P.; Wodzig, W.; Schierbeek, H.; Verdijk, L.B.; et al. Branched-chain amino acid and branched-chain ketoacid ingestion increases muscle protein synthesis rates in vivo in older adults: A double-blind, randomized trial. Am. J. Clin. Nutr. 2019, 110, 862–872. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.K.; Suzuki, T.; Saito, K.; Yoshida, H.; Kobayashi, H.; Kato, H.; Katayama, M. Effects of exercise and amino acid supplementation on body composition and physical function in community-dwelling elderly Japanese sarcopenic women: A randomized controlled trial. J. Am. Geriatr. Soc. 2012, 60, 16–23. [Google Scholar] [CrossRef]
- Deutz, N.E.; Bauer, J.M.; Barazzoni, R.; Biolo, G.; Boirie, Y.; Bosy-Westphal, A.; Cederholm, T.; Cruz-Jentoft, A.; Krznaric, Z.; Nair, K.S.; et al. Protein intake and exercise for optimal muscle function with aging: Recommendations from the ESPEN Expert Group. Clin. Nutr. 2014, 33, 929–936. [Google Scholar] [CrossRef] [Green Version]
- Papet, I.; Rémond, D.; Dardevet, D.; Mosoni, L.; Polakof, S.; Peyron, M.-A.; Savary-Auzeloux, I. Sulfur Amino Acids and Skeletal Muscle. In Nutrition and Skeletal Muscle; Walrand, S., Ed.; Elsevier Inc.: Amsterdam, The Netherlands, 2019; pp. 335–363. [Google Scholar]
- Baldelli, S.; Ciccarone, F.; Limongi, D.; Checconi, P.; Palamara, A.T.; Ciriolo, M.R. Glutathione and Nitric Oxide: Key Team Players in Use and Disuse of Skeletal Muscle. Nutrients 2019, 11, 2318. [Google Scholar] [CrossRef] [Green Version]
- Aoi, W.; Ogaya, Y.; Takami, M.; Konishi, T.; Sauchi, Y.; Park, E.Y.; Wada, S.; Sato, K.; Higashi, A. Glutathione supplementation suppresses muscle fatigue induced by prolonged exercise via improved aerobic metabolism. J. Int. Soc. Sports Nutr. 2015, 12, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Dukes, A.; Davis, C.; El Refaey, M.; Upadhyay, S.; Mork, S.; Arounleut, P.; Johnson, M.H.; Hill, W.D.; Isales, C.M.; Hamrick, M.W. The aromatic amino acid tryptophan stimulates skeletal muscle IGF1/p70s6k/mTor signaling in vivo and the expression of myogenic genes in vitro. Nutrition 2015, 31, 1018–1024. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jo, E.; Lee, S.R.; Park, B.S.; Kim, J.S. Potential mechanisms underlying the role of chronic inflammation in age-related muscle wasting. Aging Clin. Exp. Res. 2012, 24, 412–422. [Google Scholar] [PubMed]
- Wang, J.; Leung, K.S.; Chow, S.K.; Cheung, W.H. Inflammation and age-associated skeletal muscle deterioration (sarcopaenia). J. Orthop. Translat. 2017, 10, 94–101. [Google Scholar] [CrossRef] [PubMed]
- Bano, G.; Trevisan, C.; Carraro, S.; Solmi, M.; Luchini, C.; Stubbs, B.; Manzato, E.; Sergi, G.; Veronese, N. Inflammation and sarcopenia: A systematic review and meta-analysis. Maturitas 2017, 96, 10–15. [Google Scholar] [CrossRef]
- Lustgarten, M.S.; Price, L.L.; Chale, A.; Phillips, E.M.; Fielding, R.A. Branched chain amino acids are associated with muscle mass in functionally limited older adults. J. Gerontol. A Biol. Sci. Med. Sci. 2014, 69, 717–724. [Google Scholar] [CrossRef] [Green Version]
- Caldo-Silva, A.; Furtado, G.E.; Chupel, M.U.; Bachi, A.L.L.; de Barros, M.P.; Neves, R.; Marzetti, E.; Massart, A.; Teixeira, A.M. Effect of Training-Detraining Phases of Multicomponent Exercises and BCAA Supplementation on Inflammatory Markers and Albumin Levels in Frail Older Persons. Nutrients 2021, 13, 1106. [Google Scholar] [CrossRef]
- Li, Y.C.; Li, Y.Z.; Li, R.; Lan, L.; Li, C.L.; Huang, M.; Shi, D.; Feng, R.N.; Sun, C.H. Dietary Sulfur-Containing Amino Acids Are Associated with Higher Prevalence of Overweight/Obesity in Northern Chinese Adults, an Internet-Based Cross-Sectional Study. Ann. Nutr. Metab. 2018, 73, 44–53. [Google Scholar] [CrossRef]
- Shivappa, N.; Steck, S.E.; Hurley, T.G.; Hussey, J.R.; Hebert, J.R. Designing and developing a literature-derived, population-based dietary inflammatory index. Public Health Nutr. 2014, 17, 1689–1696. [Google Scholar] [CrossRef] [Green Version]
- Custodero, C.; Mankowski, R.T.; Lee, S.A.; Chen, Z.; Wu, S.; Manini, T.M.; Hincapie Echeverri, J.; Sabba, C.; Beavers, D.P.; Cauley, J.A.; et al. Evidence-based nutritional and pharmacological interventions targeting chronic low-grade inflammation in middle-age and older adults: A systematic review and meta-analysis. Ageing Res. Rev. 2018, 46, 42–59. [Google Scholar] [CrossRef]
- Andrich, D.E.; Melbouci, L.; Ou, Y.; Auclair, N.; Mercier, J.; Grenier, J.C.; Lira, F.S.; Barreiro, L.B.; Danialou, G.; Comtois, A.S.; et al. A Short-Term High-Fat Diet Alters Glutathione Levels and IL-6 Gene Expression in Oxidative Skeletal Muscles of Young Rats. Front. Physiol. 2019, 10, 372. [Google Scholar] [CrossRef] [Green Version]
- Su, Y.; Yeung, S.; Chen, Y.M.; Leung, J.; Kwok, T. The associations of dietary inflammatory potential with musculoskeletal health in Chinese community-dwelling older people: The Mr/Ms. OS (Hong Kong) cohort study. JBMR 2022, 37, 1179–1187. [Google Scholar] [CrossRef] [PubMed]
- Kwok, A.W.; Gong, J.S.; Wang, Y.X.; Leung, J.C.; Kwok, T.; Griffith, J.F.; Leung, P.C. Prevalence and risk factors of radiographic vertebral fractures in elderly Chinese men and women: Results of Mr. OS (Hong Kong) and Ms. OS (Hong Kong) studies. Osteoporos. Int. 2013, 24, 877–885. [Google Scholar] [CrossRef] [PubMed]
- Washburn, R.A.; Smith, K.W.; Jette, A.M.; Janney, C.A. The Physical Activity Scale for the Elderly (PASE): Development and evaluation. J. Clin. Epidemiol. 1993, 46, 153–162. [Google Scholar] [CrossRef]
- Liu, B.; Woo, J.; Tang, N.; Ng, K.; Ip, R.; Yu, A. Assessment of total energy expenditure in a Chinese population by a physical activity questionnaire: Examination of validity. Int. J. Food Sci. Nutr. 2001, 52, 269–282. [Google Scholar] [CrossRef]
- Woo, J.; Leung, S.S.F.; Ho, S.C.; Lam, T.H.; Janus, E.D. A food frequency questionnaire for use in the Chinese population in Hong Kong: Description and examination of validity. Nutr. Res. 1997, 17, 1633–1641. [Google Scholar] [CrossRef]
- Doria, E.; Buonocore, D.; Focarelli, A.; Marzatico, F. Relationship between human aging muscle and oxidative system pathway. Oxid. Med. Cell. Longev. 2012, 2012, 830257. [Google Scholar] [CrossRef] [Green Version]
- Cervenka, I.; Agudelo, L.Z.; Ruas, J.L. Kynurenines: Tryptophan’s metabolites in exercise, inflammation, and mental health. Science 2017, 357, eaaf9794. [Google Scholar] [CrossRef] [Green Version]
- Antoniades, C.; Shirodaria, C.; Leeson, P.; Baarholm, O.A.; Van-Assche, T.; Cunnington, C.; Pillai, R.; Ratnatunga, C.; Tousoulis, D.; Stefanadis, C.; et al. MTHFR 677 C>T Polymorphism reveals functional importance for 5-methyltetrahydrofolate, not homocysteine, in regulation of vascular redox state and endothelial function in human atherosclerosis. Circulation 2009, 119, 2507–2515. [Google Scholar] [CrossRef] [Green Version]
- Su, Y.; Elshorbagy, A.; Turner, C.; Refsum, H.; Chan, R.; Kwok, T. Circulating amino acids are associated with bone mineral density decline and ten-year major osteoporotic fracture risk in older community-dwelling adults. Bone 2019, 129, 115082. [Google Scholar] [CrossRef]
- Stevens, L.A.; Coresh, J.; Greene, T.; Levey, A.S. Assessing kidney function--measured and estimated glomerular filtration rate. N. Engl. J. Med. 2006, 354, 2473–2483. [Google Scholar] [CrossRef] [Green Version]
- Orwoll, E.S.; Lapidus, J.; Wang, P.Y.; Vandenput, L.; Hoffman, A.; Fink, H.A.; Laughlin, G.A.; Nethander, M.; Ljunggren, O.; Kindmark, A.; et al. The Limited Clinical Utility of Testosterone, Estradiol, and Sex Hormone Binding Globulin Measurements in the Prediction of Fracture Risk and Bone Loss in Older Men. J. Bone Miner. Res. 2017, 32, 633–640. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heymsfield, S.B.; Smith, R.; Aulet, M.; Bensen, B.; Lichtman, S.; Wang, J.; Pierson, R.N., Jr. Appendicular skeletal muscle mass: Measurement by dual-photon absorptiometry. Am. J. Clin. Nutr. 1990, 52, 214–218. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.K.; Woo, J.; Assantachai, P.; Auyeung, T.W.; Chou, M.Y.; Iijima, K.; Jang, H.C.; Kang, L.; Kim, M.; Kim, S.; et al. Asian Working Group for Sarcopenia: 2019 Consensus Update on Sarcopenia Diagnosis and Treatment. J. Am. Med. Dir. Assoc. 2020, 21, 300–307.e2. [Google Scholar] [CrossRef] [PubMed]
- Morris, C.; O’Grada, C.; Ryan, M.; Roche, H.M.; Gibney, M.J.; Gibney, E.R.; Brennan, L. The relationship between BMI and metabolomic profiles: A focus on amino acids. Proc. Nutr. Soc. 2012, 71, 634–638. [Google Scholar] [CrossRef] [Green Version]
- Elshorbagy, A.K.; Valdivia-Garcia, M.; Graham, I.M.; Palma Reis, R.; Sales Luis, A.; Smith, A.D.; Refsum, H. The association of fasting plasma sulfur-containing compounds with BMI, serum lipids and apolipoproteins. Nutr. Metab. Cardiovasc. Dis. 2012, 22, 1031–1038. [Google Scholar] [CrossRef]
- Yu, R.; Wong, M.; Leung, J.; Lee, J.; Auyeung, T.W.; Woo, J. Incidence, reversibility, risk factors and the protective effect of high body mass index against sarcopenia in community-dwelling older Chinese adults. Geriatr. Gerontol. Int. 2014, 14 (Suppl. S1), 15–28. [Google Scholar] [CrossRef]
- Baron, R.M.; Kenny, D.A. The moderator-mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. J. Pers. Soc. Psychol. 1986, 51, 1173–1182. [Google Scholar] [CrossRef]
- Yamada, M.; Kimura, Y.; Ishiyama, D.; Nishio, N.; Tanaka, T.; Ohji, S.; Otobe, Y.; Koyama, S.; Sato, A.; Suzuki, M.; et al. Plasma Amino Acid Concentrations Are Associated with Muscle Function in Older Japanese Women. J. Nutr. Health Aging 2018, 22, 819–823. [Google Scholar] [CrossRef]
- Katsanos, C.S.; Kobayashi, H.; Sheffield-Moore, M.; Aarsland, A.; Wolfe, R.R. A high proportion of leucine is required for optimal stimulation of the rate of muscle protein synthesis by essential amino acids in the elderly. Am. J. Physiol. Endocrinol. Metab. 2006, 291, E381–E387. [Google Scholar] [CrossRef] [Green Version]
- Dreyer, H.C.; Drummond, M.J.; Pennings, B.; Fujita, S.; Glynn, E.L.; Chinkes, D.L.; Dhanani, S.; Volpi, E.; Rasmussen, B.B. Leucine-enriched essential amino acid and carbohydrate ingestion following resistance exercise enhances mTOR signaling and protein synthesis in human muscle. Am. J. Physiol. Endocrinol. Metab. 2008, 294, E392–E400. [Google Scholar] [CrossRef] [Green Version]
- Khemtong, C.; Kuo, C.H.; Chen, C.Y.; Jaime, S.J.; Condello, G. Does Branched-Chain Amino Acids (BCAAs) Supplementation Attenuate Muscle Damage Markers and Soreness after Resistance Exercise in Trained Males? A Meta-Analysis of Randomized Controlled Trials. Nutrients 2021, 13, 1880. [Google Scholar] [CrossRef] [PubMed]
- Elshorbagy, A.K.; Turner, C.; Bastani, N.; Refsum, H.; Kwok, T. The association of serum sulfur amino acids and related metabolites with incident diabetes: A prospective cohort study. Eur. J. Nutr. 2022. [Google Scholar] [CrossRef] [PubMed]
- Dhar, I.; Svingen, G.F.T.; Ueland, P.M.; Lysne, V.; Svenningsson, M.M.; Tell, G.S.; Nygard, O.K. Plasma Cystathionine and Risk of Incident Stroke in Patients with Suspected Stable Angina Pectoris. J. Am. Heart Assoc. 2018, 7, e008824. [Google Scholar] [CrossRef] [PubMed]
- Dhar, I.; Lysne, V.; Svingen, G.F.T.; Ueland, P.M.; Gregory, J.F.; Bonaa, K.H.; Nygard, O.K. Elevated plasma cystathionine is associated with increased risk of mortality among patients with suspected or established coronary heart disease. Am. J. Clin. Nutr. 2019, 109, 1546–1554. [Google Scholar] [CrossRef]
- DeRatt, B.N.; Ralat, M.A.; Lysne, V.; Tayyari, F.; Dhar, I.; Edison, A.S.; Garrett, T.J.; Midttun, O.; Ueland, P.M.; Nygard, O.K.; et al. Metabolomic Evaluation of the Consequences of Plasma Cystathionine Elevation in Adults with Stable Angina Pectoris. J. Nutr. 2017, 147, 1658–1668. [Google Scholar] [CrossRef] [Green Version]
- Dhar, I.; Svingen, G.F.T.; Pedersen, E.R.; DeRatt, B.; Ulvik, A.; Strand, E.; Ueland, P.M.; Bonaa, K.H.; Gregory, J.F.; Nygard, O.K. Plasma cystathionine and risk of acute myocardial infarction among patients with coronary heart disease: Results from two independent cohorts. Int. J. Cardiol. 2018, 266, 24–30. [Google Scholar] [CrossRef] [Green Version]
- Ishii, I.; Akahoshi, N.; Yamada, H.; Nakano, S.; Izumi, T.; Suematsu, M. Cystathionine gamma-Lyase-deficient mice require dietary cysteine to protect against acute lethal myopathy and oxidative injury. J. Biol. Chem. 2010, 285, 26358–26368. [Google Scholar] [CrossRef] [Green Version]
- Cervo, M.M.; Shivappa, N.; Hebert, J.R.; Oddy, W.H.; Winzenberg, T.; Balogun, S.; Wu, F.; Ebeling, P.; Aitken, D.; Jones, G.; et al. Longitudinal associations between dietary inflammatory index and musculoskeletal health in community-dwelling older adults. Clin. Nutr. 2020, 39, 516–523. [Google Scholar] [CrossRef]
- Jacobsen, D.W. Hyperhomocysteinemia and oxidative stress: Time for a reality check? Arterioscler. Thromb. Vasc. Biol. 2000, 20, 1182–1184. [Google Scholar] [CrossRef] [Green Version]
- De Giuseppe, R.; Tomasinelli, C.E.; Vincenti, A.; Di Napoli, I.; Negro, M.; Cena, H. Sarcopenia and homocysteine: Is there a possible association in the elderly? A narrative review. Nutr. Res. Rev. 2022, 25, 98–111. [Google Scholar] [CrossRef]
- Vidoni, M.L.; Pettee Gabriel, K.; Luo, S.T.; Simonsick, E.M.; Day, R.S. Relationship between Homocysteine and Muscle Strength Decline: The Baltimore Longitudinal Study of Aging. J. Gerontol. A Biol. Sci. Med. Sci. 2018, 73, 546–551. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Veeranki, S.; Tyagi, S.C. Defective homocysteine metabolism: Potential implications for skeletal muscle malfunction. Int. J. Mol. Sci. 2013, 14, 15074–15091. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moaddel, R.; Fabbri, E.; Khadeer, M.A.; Carlson, O.D.; Gonzalez-Freire, M.; Zhang, P.; Semba, R.D.; Ferrucci, L. Plasma Biomarkers of Poor Muscle Quality in Older Men and Women from the Baltimore Longitudinal Study of Aging. J. Gerontol. A Biol. Sci. Med. Sci. 2016, 71, 1266–1272. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ottestad, I.; Ulven, S.M.; Oyri, L.K.L.; Sandvei, K.S.; Gjevestad, G.O.; Bye, A.; Sheikh, N.A.; Biong, A.S.; Andersen, L.F.; Holven, K.B. Reduced plasma concentration of branched-chain amino acids in sarcopenic older subjects: A cross-sectional study. Br. J. Nutr. 2018, 120, 445–453. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Men, Mean (SD) | Women, Mean (SD) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Variables | DII | p-Value a | p-Value b | DII | p-Value a | p-Value b | ||||
| T1, n = 498 | T2, n = 475 | T3, n = 451 | T1, n = 552 | T2, n = 522 | T3, n = 496 | |||||
| Age (year) | 71.6 (4.8) | 71.5 (4.5) | 72.1 (4.8) | 0.115 | - | 71.5 (4.9) | 72.2 (5) | 72.5 (5.3) | 0.001 | - |
| BMI (kg/m2) | 23.6 (3.1) | 23.6 (3) | 23.3 (3.2) | 0.116 | 0.154 | 24.0 (3.5) | 24.1 (3.3) | 23.8 (3.3) | 0.474 | 0.636 |
| Appendicular muscle mass (kg/m2) | 7.3 (0.8) | 7.3 (0.8) | 7.2 (0.8) | 0.015 | 0.029 | 6.1 (0.8) | 6.1 (0.7) | 6.1 (0.7) | 0.105 | 0.173 |
| Grip strength (kg) | 35.2 (6.7) | 34.8 (6.3) | 33.8 (6.5) | 0.001 | 0.003 | 23.0 (4.5) | 22.4 (4.3) | 22.2 (4.3) | 0.003 | 0.029 |
| Gait speed (m/s) | 1.1 (0.2) | 1.1 (0.2) | 1.0 (0.2) | <0.001 | <0.001 | 1.0 (0.2) | 1.0 (0.2) | 0.9 (0.2) | <0.001 | 0.001 |
| 5-time chair stand (s) | 12.2 (3.6) | 12.3 (3.4) | 12.8 (3.8) | 0.006 | 0.010 | 12.6 (4.5) | 13.2 (4.7) | 13.8 (5.4) | <0.001 | 0.001 |
| Sarcopenia (yes, %) | 111 (22.3%) | 101 (21.3%) | 145 (32.2%) | 0.001 | 0.001 | 56 (10.1%) | 63 (12.1%) | 57 (11.5%) | 0.476 | 0.653 |
| Branched chain amino acids | ||||||||||
| Valine (uM) | 301.6 (45.6) | 307.6 (45.1) | 306.1 (44.4) | 0.116 | 0.076 | 279 (44.4) | 279.2 (42.7) | 279.7 (45.9) | 0.780 | 0.644 |
| Leucine (uM) | 155.8 (23.9) | 158.6 (24.5) | 158.1 (25.1) | 0.137 | 0.089 | 140.8 (23) | 140.5 (20.9) | 140.3 (23.1) | 0.699 | 0.953 |
| Isoleucine (uM) | 83.9 (14.8) | 85.3 (15.4) | 85.7 (14.7) | 0.067 | 0.044 | 75.4 (13.7) | 76.1 (13.8) | 76 (14) | 0.474 | 0.380 |
| Aromatic amino acids | ||||||||||
| Phenylalanine (uM) | 97.7 (12.9) | 98.3 (13.5) | 98.8 (13.3) | 0.180 | 0.188 | 96.7 (14.6) | 96.7 (13.7) | 96 (14.2) | 0.471 | 0.405 |
| Tryptophan (uM) | 61.6 (10.5) | 61.1 (10.7) | 61.1 (11.9) | 0.487 | 0.620 | 56.7 (10.1) | 56 (9.7) | 57 (11.6) | 0.679 | 0.489 |
| Tyrosine (uM) | 85.1 (14.6) | 84.5 (14.7) | 83.6 (14.4) | 0.108 | 0.122 | 82.6 (14.2) | 82.9 (15) | 81.8 (14.3) | 0.420 | 0.380 |
| Sulfur amino acids | ||||||||||
| Methionine (uM) | 31.2 (4.9) | 31 (4.6) | 30.9 (4.7) | 0.314 | 0.389 | 23.9 (4.2) | 24.1 (4.7) | 23.7 (4.3) | 0.525 | 0.571 |
| tHcy (uM) c | 14.9 (4.2) | 15.5 (4.8) | 16.2 (6.6) | 0.001 | 0.001 | 13 (4.5) | 13.1 (4.3) | 13.2 (3.9) | 0.278 c | 0.853 c |
| Cystathionine (nM) c | 278.3 (178.2) | 280.6 (204.7) | 303.8 (191.2) | 0.003 | 0.0038 | 235.5 (262.5) | 240.5 (150.4) | 233.2 (140.4) | 0.378 c | 0.745 c |
| tCys (uM) | 359.1 (44.6) | 361.4 (40.6) | 362.4 (49.3) | 0.257 | 0.461 | 352.1 (46.6) | 350.2 (42.4) | 354.6 (43.4) | 0.384 | 0.928 |
| Taurine (uM) | 170.0 (31.2) | 172.3 (34.8) | 172.8 (31.7) | 0.158 c | 0.107 c | 171.7 (30.9) | 170.7 (36) | 169.5 (31) | 0.235 c | 0.308 c |
| tGSH (uM) | 4.2 (1.4) | 4.2 (1.4) | 4.0 (1.2) | 0.065 | 0.079 | 4.3 (1.4) | 4.2 (1.3) | 4.2 (1.3) | 0.152 | 0.171 |
| Amino Acids | Grip Strength (kg) | Gait Speed (m/s) | Chair Stand Test (s) | Appendicular Muscle Mass (kg/m2) |
|---|---|---|---|---|
| Men | ||||
| β Estimate (SE) a | β Estimate (SE) a | β Estimate (SE) a | β Estimate (SE) a | |
| DII (per one tertile) | −0.557 (0.199) b | −0.034 (0.007) b,c | 0.281 (0.117) b | −0.024 (0.015) |
| Branched chain amino acids | ||||
| Valine (per one tertile) | 0.674 (0.213) b,c | 0.015 (0.007) b | −0.021 (0.126) | −0.025 (0.016) |
| Leucine (per one tertile) | 1.099 (0.214) b,c | 0.010 (0.007) | −0.061 (0.127) | −0.011 (0.016) |
| Isoleucine (per one tertile) | 0.612 (0.214) b | 0.009 (0.007) | −0.041 (0.126) | −0.043 (0.016) b |
| Aromatic amino acids | ||||
| Phenylalanine (per one tertile) | 0.069 (0.212) | 0.011 (0.007) | −0.18 (0.124) | −0.023 (0.016) |
| Tryptophan (per one tertile) | 0.547 (0.202) b | 0.007 (0.007) | −0.104 (0.119) | 0.028 (0.015) |
| Tyrosine (per one tertile) | −0.391 (0.206) | 0.019 (0.007) b | −0.068 (0.121) | 0 (0.016) |
| Sulfur amino acids | ||||
| Methionine (per one tertile) | 0.541 (0.201) b | 0.025 (0.007) b,c | −0.213 (0.118) | 0.043 (0.015) b |
| tHcy (per one tertile) | −0.873 (0.226) b,c | −0.019 (0.008) b | 0.476 (0.133) b,c | −0.073 (0.017) b,c |
| Cystathionine (per one tertile) | −0.341 (0.212) | 0.006 (0.007) | 0.143 (0.125) | −0.039 (0.016) b |
| tCys (per one tertile) | −0.636 (0.22) b,c | −0.008 (0.008) | 0.198 (0.129) | −0.06 (0.017) b,c |
| Taurine (per one tertile) | −0.082 (0.205) | 0.004 (0.007) | −0.188 (0.121) | −0.032 (0.015) b |
| tGSH (per one tertile) | 0.328 (0.203) | −0.009 (0.007) | 0.226 (0.119) | 0.031 (0.015) b |
| Women | ||||
| β Estimate (SE) a | β Estimate (SE) a | β Estimate (SE) a | β Estimate (SE) a | |
| DII (per one tertile) | −0.219 (0.129) | −0.015 (0.006) b | 0.442 (0.150) b,c | −0.017 (0.014) |
| Branched chain amino acids | ||||
| Valine (per one tertile) | 0.278 (0.137) b | 0.001 (0.006) | −0.054 (0.16) | −0.014 (0.015) |
| Leucine (per one tertile) | 0.266 (0.138) | −0.002 (0.006) | −0.041 (0.161) | −0.014 (0.015) |
| Isoleucine (per one tertile) | 0.321 (0.138) | 0.004 (0.006) | −0.173 (0.161) | −0.011 (0.015) |
| Aromatic amino acids | ||||
| Phenylalanine (per one tertile) | −0.008 (0.134) | −0.005 (0.006) | 0.098 (0.155) | −0.064 (0.015) b,c |
| Tryptophan (per one tertile) | 0.575 (0.129) b,c | 0.001 (0.006) | 0.003 (0.15) | 0.025 (0.014) |
| Tyrosine (per one tertile) | 0.314 (0.132) b | 0.002 (0.006) | 0.057 (0.154) | −0.019 (0.015) |
| Sulfur amino acids | ||||
| Methionine (per one tertile) | 0.108 (0.13) | 0.010 (0.006) | 0.025 (0.151) | 0.003 (0.015) |
| tHcy (per one tertile) | −0.343 (0.151) b | −0.011 (0.007) | 0.007 (0.176) | −0.054 (0.017) b,c |
| Cystathionine (per one tertile) | −0.420 (0.141) b,c | −0.022 (0.007) b,c | 0.227 (0.165) | −0.003 (0.016) |
| tCys (per one tertile) | 0.020 (0.145) | −0.008 (0.007) | −0.162 (0.169) | −0.057 (0.016) b,c |
| Taurine (per one tertile) | −0.129 (0.13) | −0.002 (0.006) | −0.059 (0.152) | −0.074 (0.014) b,c |
| tGSH (per one tertile) | 0.033 (0.131) | −0.012 (0.006) b | 0.106 (0.152) | 0.010 (0.015) |
| AAs | Grip Strength (kg) | Gait Speed (m/s) | Chair Stand Test (s) | Appendicular Muscle Mass (kg/m2) | Sarcopenia d (yes) | Sarcopenia d (yes) |
|---|---|---|---|---|---|---|
| Men | ||||||
| β Estimate (SE) a | β Estimate (SE) a | β Estimate (SE) a | β Estimate (SE) a | OR (95%CI) a | OR (95%CI) e | |
| DII (per one tertile) | −0.321 (0.143) b | −0.014 (0.006) b | 0.076 (0.104) | 0.009 (0.01) | 1.09 (0.86, 1.40) | 1.12 (0.89, 1.41) |
| Branched chain amino acids | ||||||
| Valine (per one tertile) | −0.073 (0.154) | 0 (0.007) | −0.014 (0.111) | −0.016 (0.011) | 1.10 (0.84, 1.43) | 0.79 (0.62, 1.00) |
| Leucine (per one tertile) | −0.046 (0.156) | 0.004 (0.007) | −0.178 (0.112) | 0.001 (0.011) | 0.94 (0.72, 1.22) | 0.70 (0.55, 0.90) b |
| Isoleucine (per one tertile) | 0.077 (0.154) | 0.001 (0.007) | −0.131 (0.112) | −0.006 (0.011) | 0.96 (0.74, 1.24) | 0.74 (0.58, 0.95) b |
| Aromatic amino acids | ||||||
| Phenylalanine (per one tertile) | −0.045 (0.151) | 0.001 (0.006) | −0.146 (0.11) | 0.001 (0.011) | 1.01 (0.78, 1.31) | 0.82 (0.65, 1.04) |
| Tryptophan (per one tertile) | 0.168 (0.145) | 0.012 (0.006) | 0.042 (0.105) | 0.013 (0.01) | 1.09 (0.85, 1.39) | 0.99 (0.79, 1.25) |
| Tyrosine (per one tertile) | 0.317 (0.148) b | 0 (0.006) | −0.074 (0.108) | 0.003 (0.011) | 0.97 (0.75, 1.24) | 0.75 (0.60, 0.95) b |
| Sulfur amino acids | ||||||
| Methionine (per one tertile) | 0.203 (0.144) | 0.001 (0.006) | −0.195 (0.105) | −0.004 (0.01) | 0.88 (0.69, 1.13) | 0.88 (0.69, 1.10) |
| tHcy (per one tertile) | −0.016 (0.163) | 0.002 (0.007) | 0.199 (0.118) | −0.012 (0.012) | 0.97 (0.73, 1.27) | 0.84 (0.65, 1.09) |
| Cystathionine (per one tertile) | −0.310 (0.152) b | 0.002 (0.006) | −0.158 (0.11) | −0.016 (0.011) | 1.10 (0.84, 1.44) | 0.98 (0.76, 1.25) |
| tCys (per one tertile) | −0.265 (0.158) | 0.004 (0.007) | 0.266 (0.114) b | −0.008 (0.011) | 1.42 (1.08, 1.88) b | 1.26 (0.98, 1.63) |
| Taurine (per one tertile) | −0.007 (0.147) | 0.010 (0.006) | −0.198 (0.106) | −0.013 (0.011) | 1.01 (0.79, 1.30) | 1.07 (0.85, 1.36) |
| tGSH (per one tertile) | 0.483 (0.145) b,c | 0.014 (0.006) b | −0.260 (0.105) b | 0.006 (0.010) | 0.88 (0.68, 1.13) | 1.00 (0.79, 1.27) |
| Women | ||||||
| β estimate (SE) a | β estimate (SE) a | β estimate (SE) a | β estimate (SE) a | OR (95%CI) a | OR (95%CI) e | |
| DII (per one tertile) | 0.070 (0.099) | −0.004 (0.005) | 0.182 (0.173) | −0.007 (0.009) | 0.82 (0.63, 1.06) | 0.80 (0.63, 1.02) |
| Branched chain amino acids | ||||||
| Valine (per one tertile) | 0.02 (0.106) | 0.006 (0.006) | −0.228 (0.184) | −0.019 (0.01) | 1.27 (0.96, 1.67) | 0.78 (0.61, 1.01) |
| Leucine (per one tertile) | 0.069 (0.107) | 0.003 (0.006) | −0.235 (0.186) | −0.009 (0.01) | 1.39 (1.05, 1.84) b | 0.88 (0.68, 1.13) |
| Isoleucine (per one tertile) | −0.045 (0.107) | −0.001 (0.006) | 0.1 (0.185) | −0.017 (0.01) | 1.30 (0.99, 1.71) | 0.83 (0.65, 1.07) |
| Aromatic amino acids | ||||||
| Phenylalanine (per one tertile) | 0.135 (0.103) | 0.009 (0.006) | −0.156 (0.178) | 0.006 (0.01) | 1.22 (0.93, 1.60) | 0.85 (0.66, 1.09) |
| Tryptophan (per one tertile) | −0.022 (0.100) | 0.006 (0.005) | −0.361 (0.173) b | −0.023 (0.009) b | 1.22 (0.94, 1.58) | 1.00 (0.78, 1.27) |
| Tyrosine (per one tertile) | 0.052 (0.102) | 0.002 (0.005) | −0.271 (0.177) | −0.011 (0.01) | 1.35 (1.03, 1.77) b | 0.94 (0.74, 1.20) |
| Sulfur amino acids | ||||||
| Methionine (per one tertile) | 0.16 (0.100) | −0.007 (0.005) | −0.007 (0.174) | −0.007 (0.009) | 1.44 (1.10, 1.89) b | 1.10 (0.86, 1.41) |
| tHcy (per one tertile) | −0.107 (0.117) | −0.003 (0.006) | −0.062 (0.203) | 0.005 (0.011) | 1.02 (0.75, 1.37) | 0.79 (0.59, 1.04) |
| Cystathionine (per one tertile) | −0.129 (0.109) | −0.002 (0.006) | −0.022 (0.189) | −0.006 (0.010) | 0.96 (0.72, 1.28) | 0.78 (0.60, 1.02) |
| tCys (per one tertile) | −0.279 (0.111) b | 0.005 (0.006) | −0.097 (0.195) | 0.007 (0.010) | 1.22 (0.91, 1.64) | 0.85 (0.65, 1.10) |
| Taurine (per one tertile) | −0.066 (0.100) | −0.008 (0.005) | −0.011 (0.174) | −0.009 (0.009) | 1.41 (1.08, 1.84) b | 1.11 (0.87, 1.42) |
| tGSH (per one tertile) | 0 (0.101) | −0.008 (0.005) | 0.122 (0.176) | 0.028 (0.009) b,c | 0.92 (0.71, 1.19) | 1.02 (0.80, 1.30) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Su, Y.; Elshorbagy, A.; Turner, C.; Refsum, H.; Kwok, T. The Association of Circulating Amino Acids and Dietary Inflammatory Potential with Muscle Health in Chinese Community-Dwelling Older People. Nutrients 2022, 14, 2471. https://doi.org/10.3390/nu14122471
Su Y, Elshorbagy A, Turner C, Refsum H, Kwok T. The Association of Circulating Amino Acids and Dietary Inflammatory Potential with Muscle Health in Chinese Community-Dwelling Older People. Nutrients. 2022; 14(12):2471. https://doi.org/10.3390/nu14122471
Chicago/Turabian StyleSu, Yi, Amany Elshorbagy, Cheryl Turner, Helga Refsum, and Timothy Kwok. 2022. "The Association of Circulating Amino Acids and Dietary Inflammatory Potential with Muscle Health in Chinese Community-Dwelling Older People" Nutrients 14, no. 12: 2471. https://doi.org/10.3390/nu14122471