
Tapioca Resistant Maltodextrin as a Carbohydrate Source of Oral Nutrition Supplement (ONS) on Metabolic Indicators: A Clinical Trial


Abstract
:1. Introduction
2. Materials and Methods
2.1. Oral Nutritional Supplements Composition
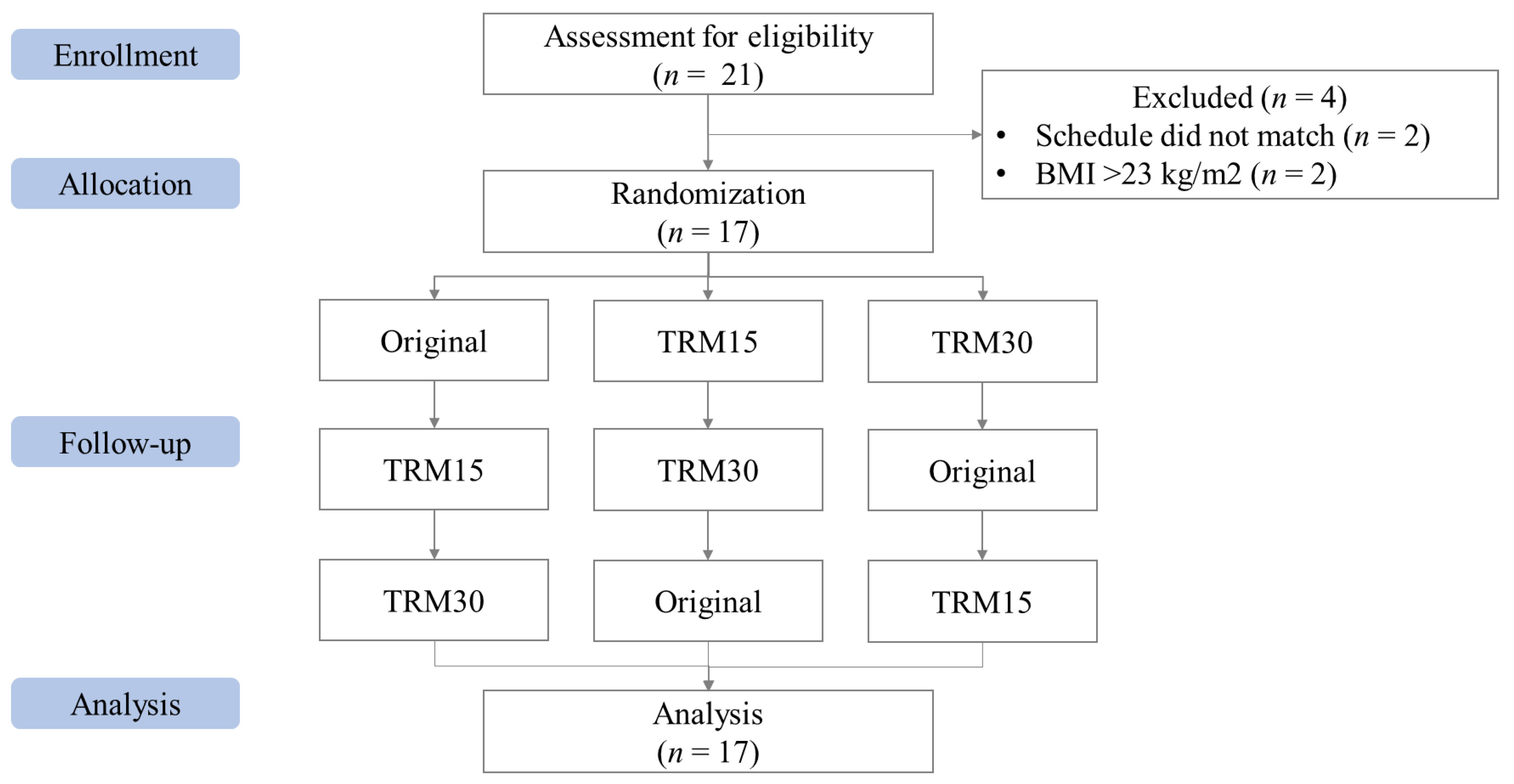
2.2. Study Design
2.2.1. Phase I: Acute Effect of Three Developed ONS on Blood Glucose, Insulin Responses, Subjective Appetite, Sensory Acceptability, and Gastrointestinal (GI) Tolerability
Study Protocol
Blood Sample Analysis
Subjective Appetite Measurement
Sensory Acceptability
Gastrointestinal (GI) Tolerability
Statistical Analysis
2.2.2. Phase II: Long-Term (12 Weeks) Effect of Selected ONS on Blood Lipid Profile, Gastrointestinal (GI) Tolerability, and Dietary Intake
Study Protocol
Blood Sample Analysis
Gastrointestinal (GI) Tolerability
Dietary Intake
Physical Activity
Statistical Analysis
2.3. Ethics
3. Results
3.1. Phase I: Acute Effects of Three Developed ONS on Blood Glucose, Insulin Responses, Subjective Appetite, Sensory Acceptability, and Gastrointestinal (GI) Tolerability
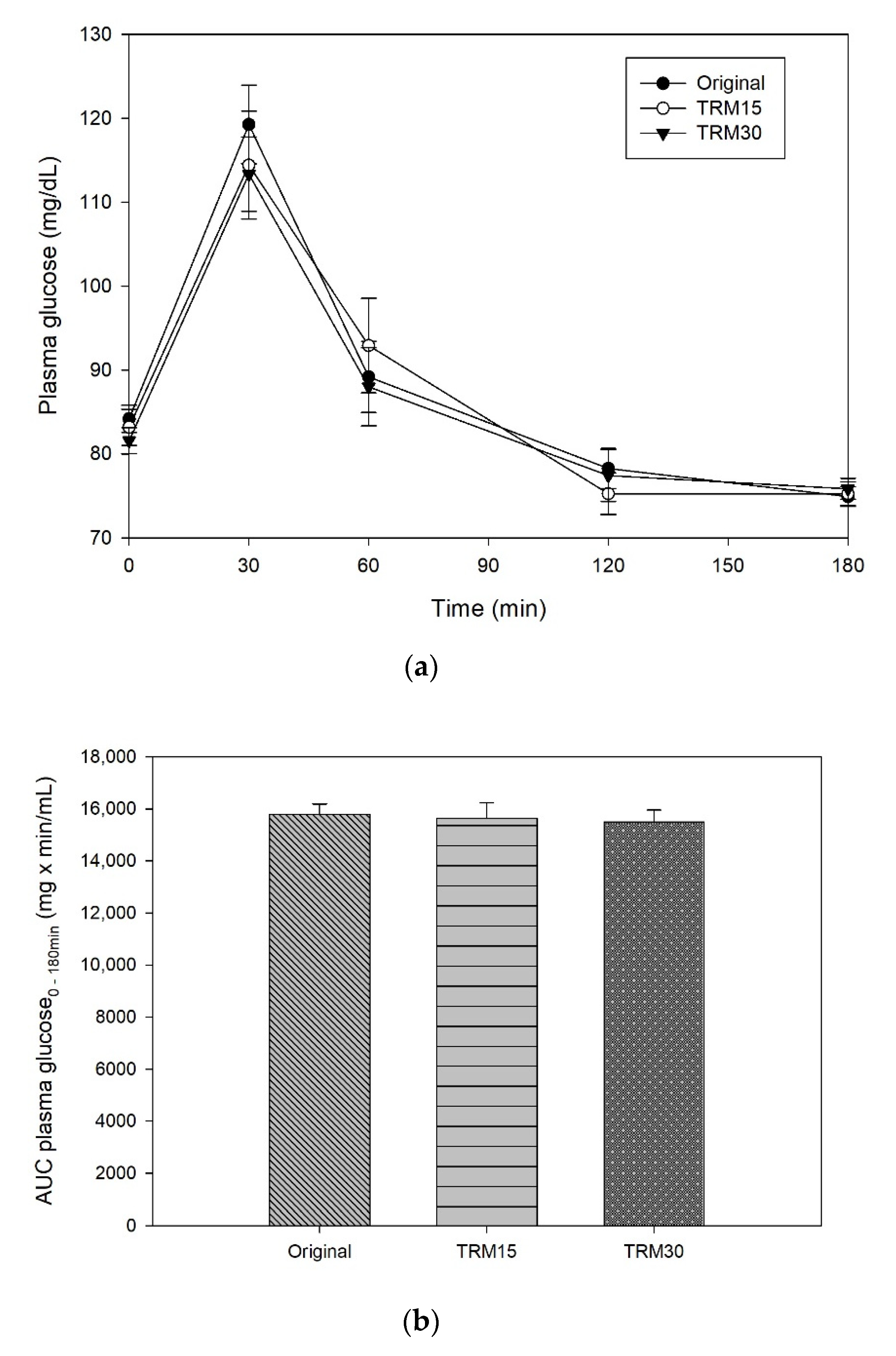
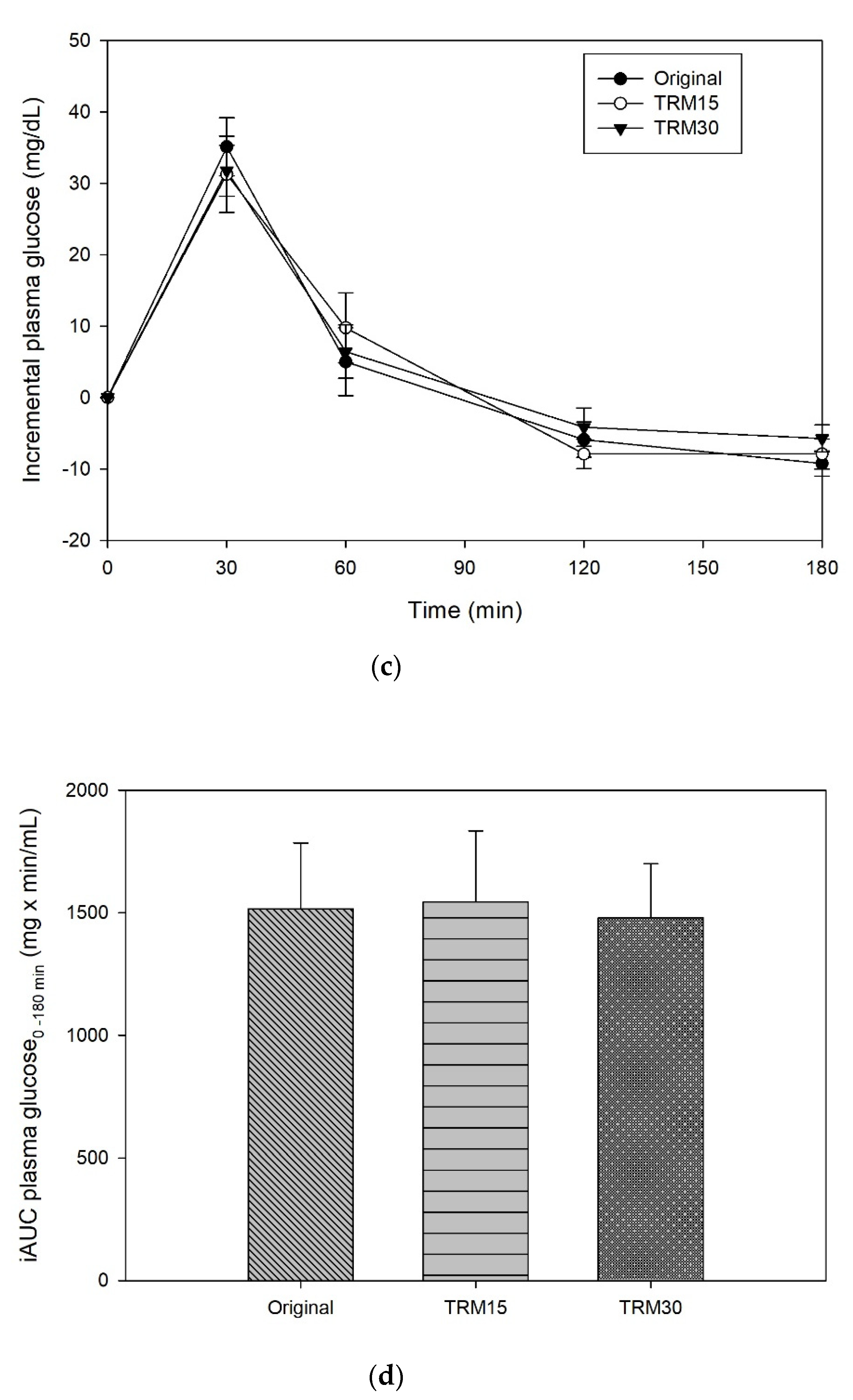
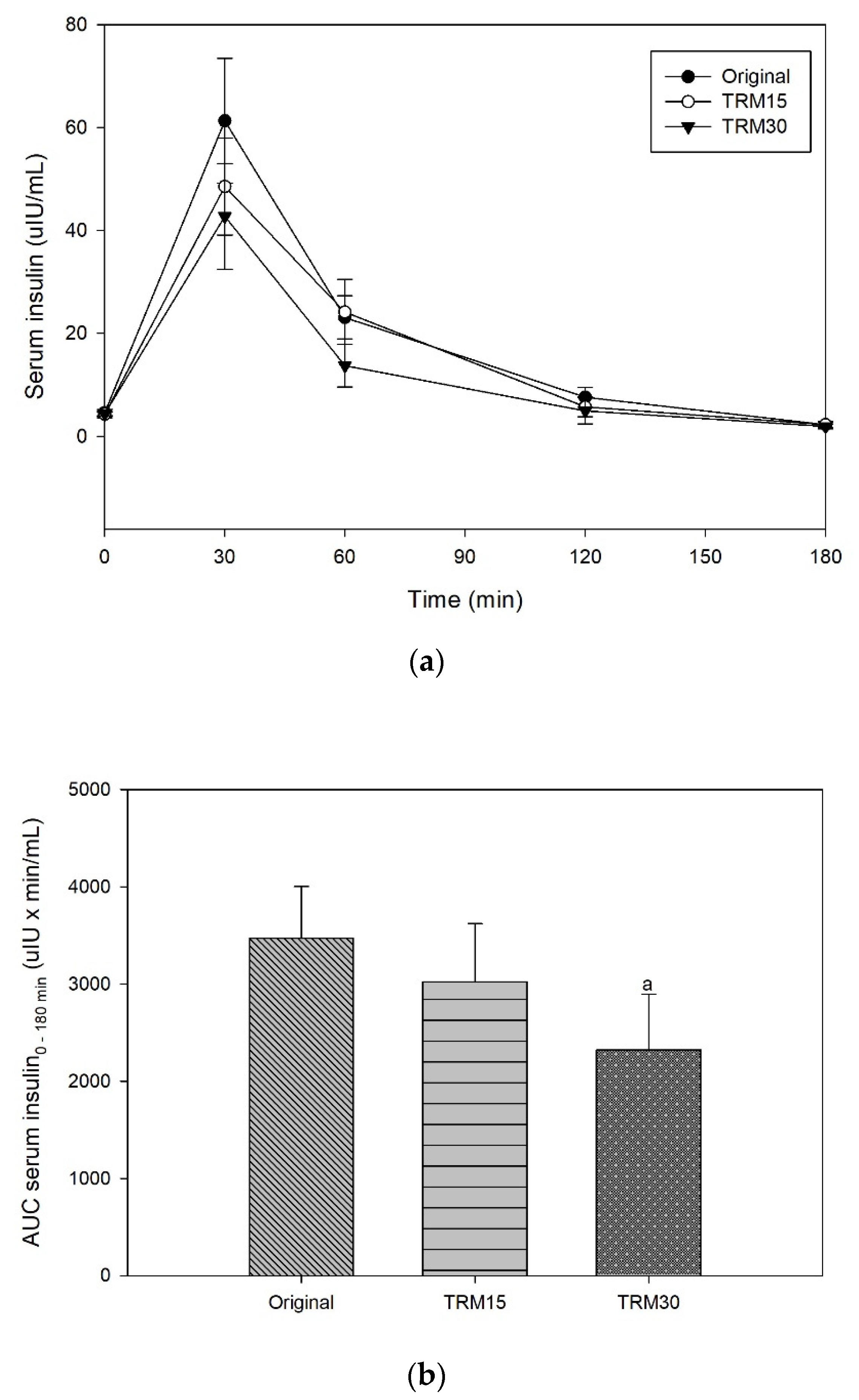
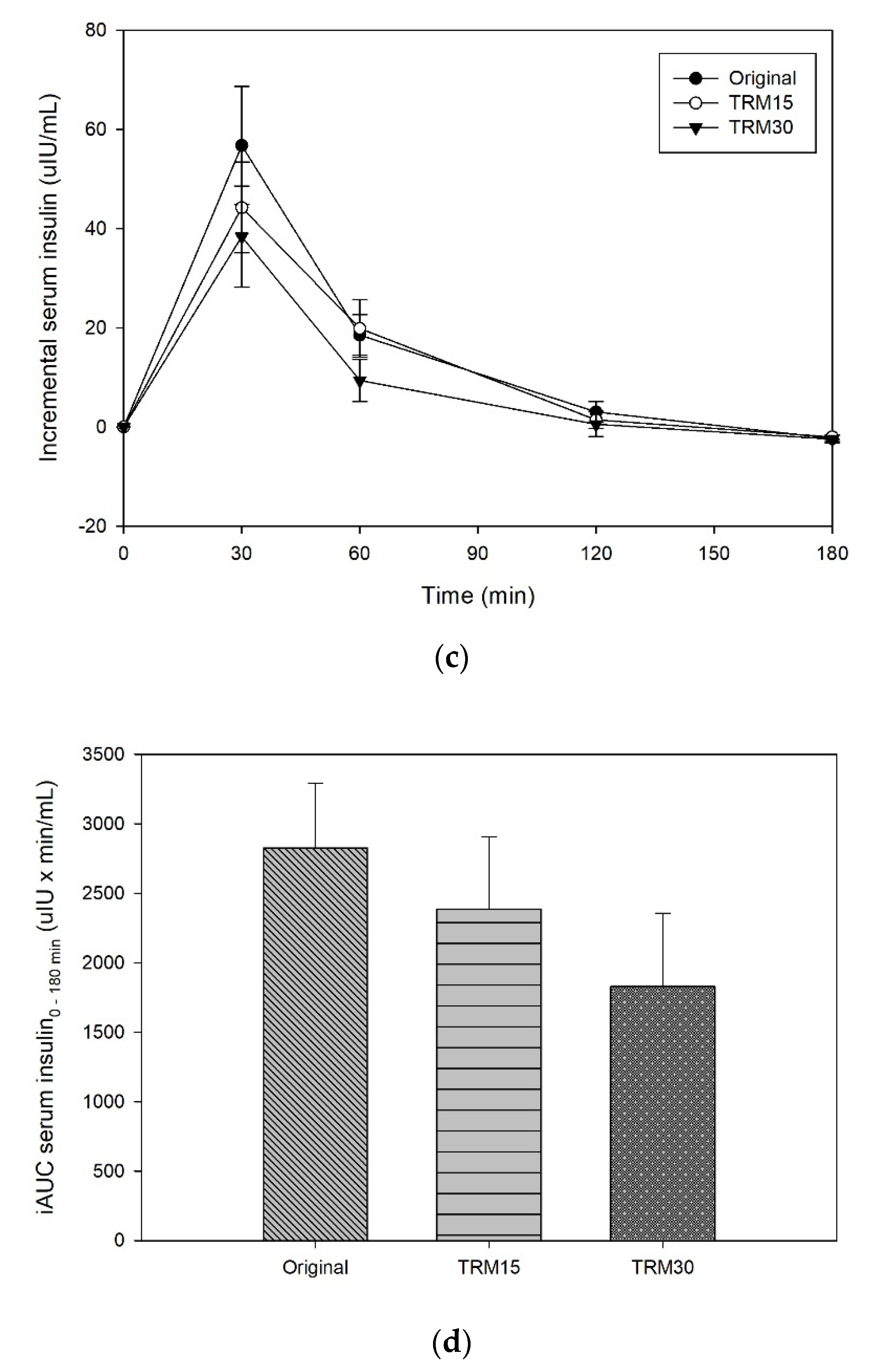
3.1.1. Postprandial Plasma Glucose and Insulin Response
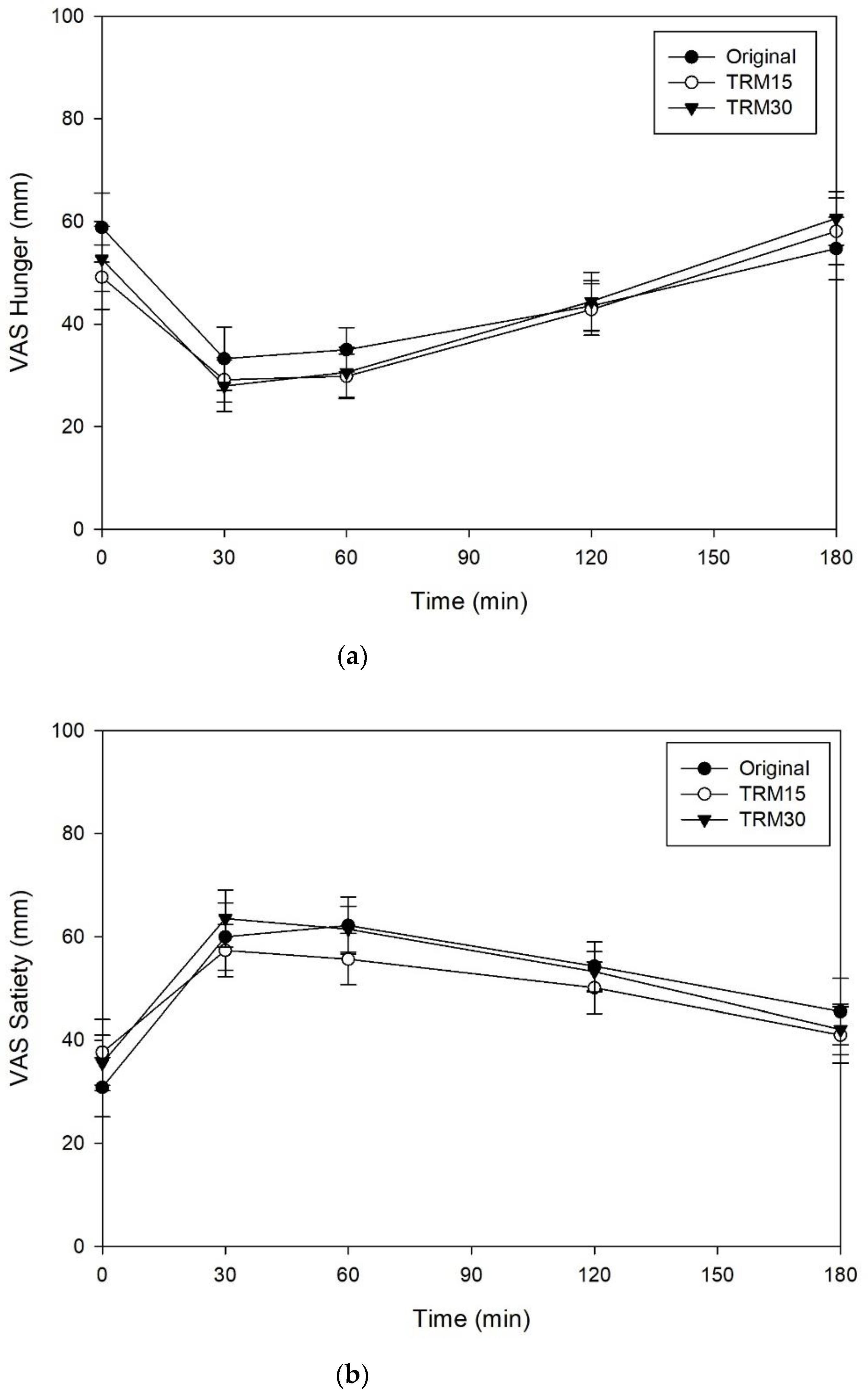
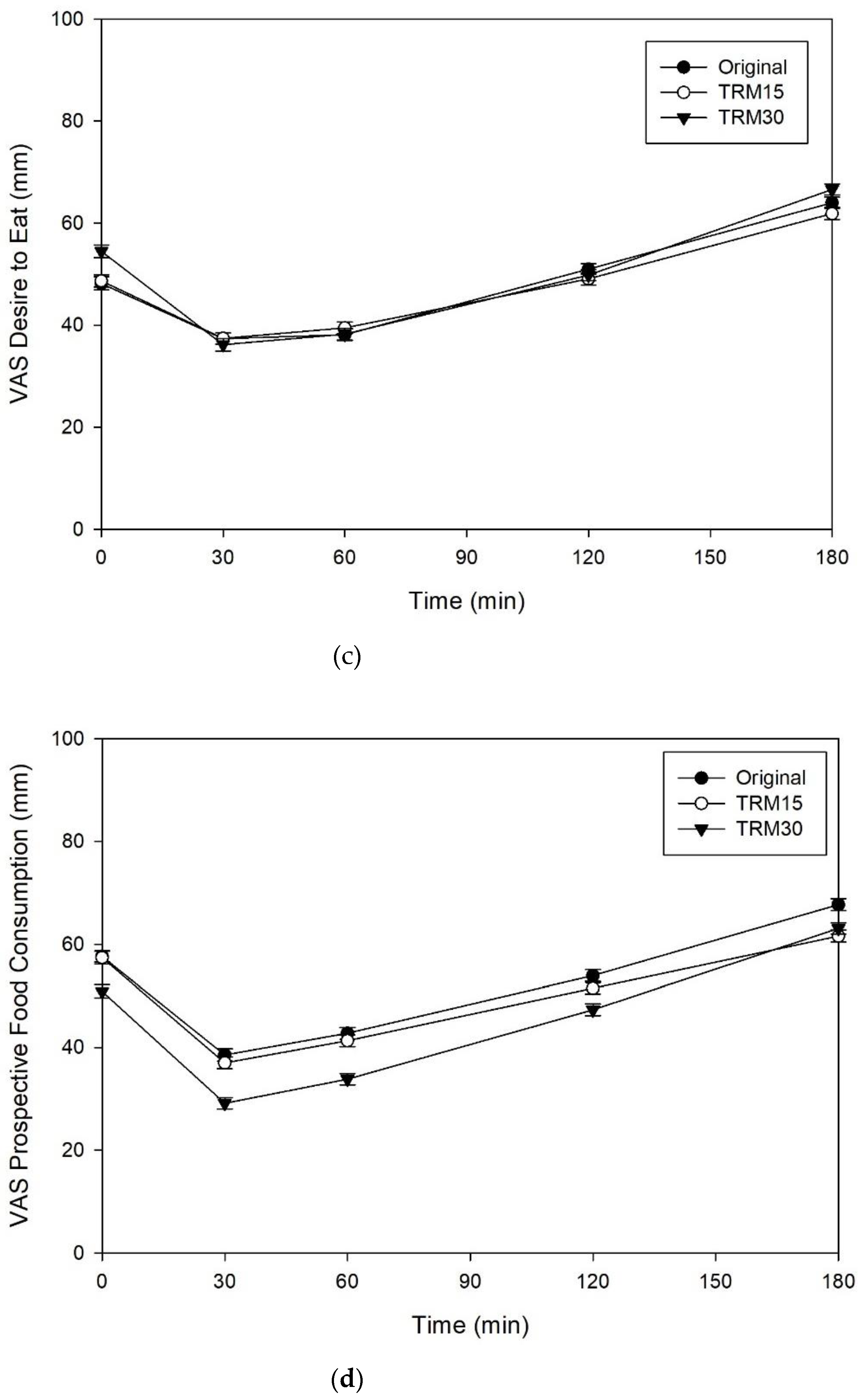
3.1.2. Subjective Appetite
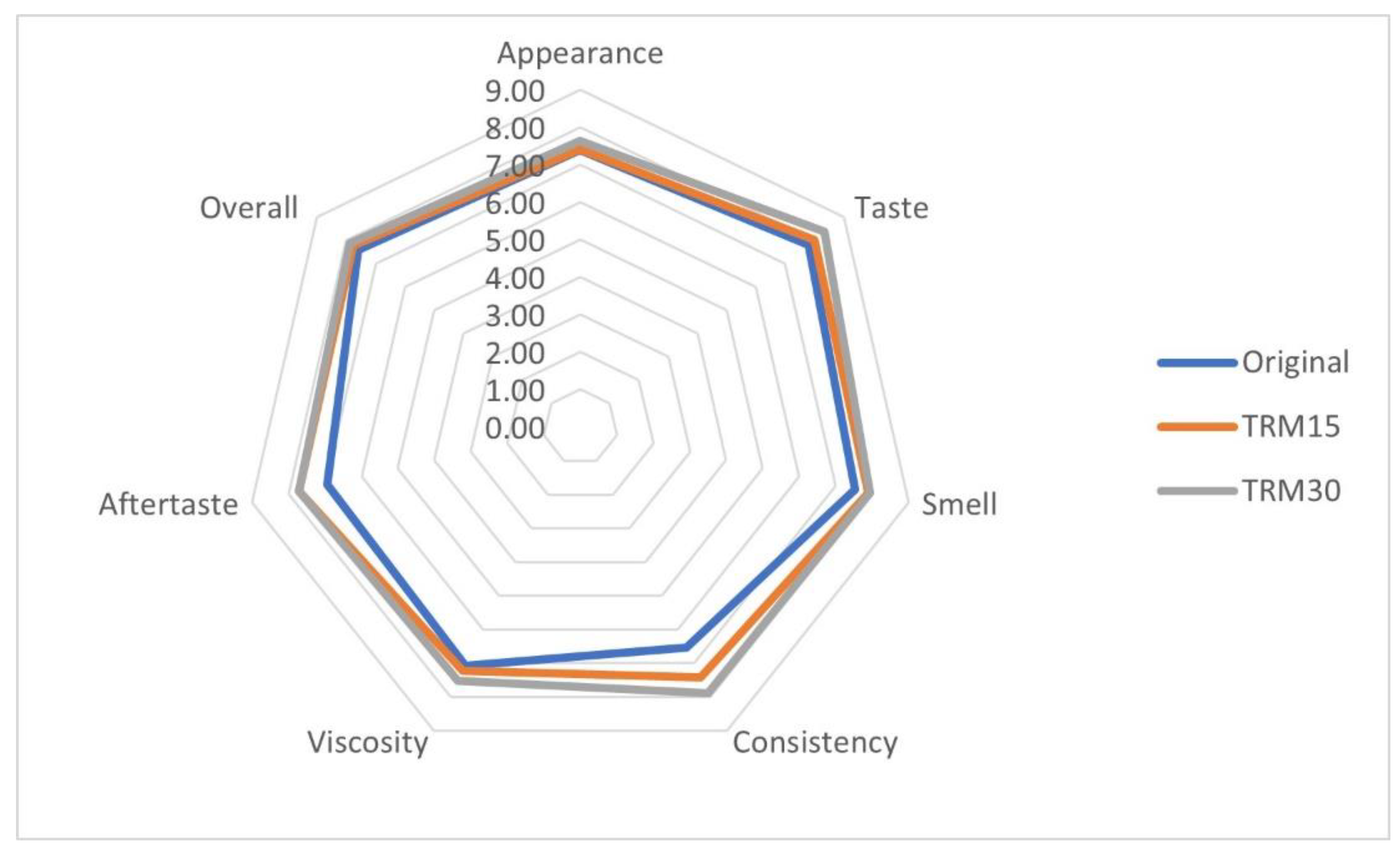
3.1.3. Sensory Acceptability
3.1.4. Gastrointestinal Tolerability
3.2. Phase 2: Long-Term (12 Weeks) Effect of TM30 on Blood Lipid Profile, Gastrointestinal (GI) Tolerability, and Dietary Intake
3.2.1. Baseline Characteristics
3.2.2. Effect of ONS Supplementation on Metabolic Markers
3.2.3. Effect of ONS Supplementation on Body Composition and Food Intake
3.2.4. Effect of ONS Supplementation on GI Tolerability
4. Discussion
Strengths and Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Toraya-Avilés, R.; Segura-Campos, M.; Chel-Guerrero, L.; Betancur-Ancona, D. Some Nutritional Characteristics of Enzymatically Resistant Maltodextrin from Cassava (Manihot esculenta Crantz) Starch. Plant Foods Hum. Nutr. 2017, 72, 149–155. [Google Scholar] [CrossRef] [PubMed]
- Banpong Novitat, C.L. Role of Cal-DM: Glucose Polymer for Health. 2019. Available online: https://www.bpnovitat.com/blank-2 (accessed on 24 April 2021).
- Ohkuma, K.; Wakabayashi, S. Fibersol-2: A Soluble, Non-Digestible, Starch-Derived Dietary Fibre. In Advanced Dietary Fibre Technology; McCleary, B.V., Prosky, L., Eds.; Blackwell Science Ltd.: Oxford, UK, 2001; pp. 509–523. [Google Scholar]
- Livesey, G.; Tagami, H. Interventions to lower the glycemic response to carbohydrate foods with a low-viscosity fiber (resistant maltodextrin): Meta-analysis of randomized controlled trials. Am. J. Clin. Nutr. 2008, 89, 114–125. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, S.; Guerin-Deremaux, L.; Pochat, M.; Wils, D.; Reifer, C.; Miller, L.E. NUTRIOSE dietary fiber supplementation improves insulin resistance and determinants of metabolic syndrome in overweight men: A double-blind, randomized, placebo-controlled study. Appl. Physiol. Nutr. Metab. 2010, 35, 773–782. [Google Scholar] [CrossRef] [PubMed]
- Kishimoto, Y.; Oga, H.; Tagami, H.; Okuma, K.; Gordon, D.T. Suppressive effect of resistant maltodextrin on postprandial blood triacylglycerol elevation. Eur. J. Nutr. 2007, 46, 133–138. [Google Scholar] [CrossRef] [PubMed]
- Guérin-Deremaux, L.; Li, S.; Pochat, M.; Wils, D.; Mubasher, M.; Reifer, C.; Miller, L.E. Effects of NUTRIOSE® dietary fiber supplementation on body weight, body composition, energy intake, and hunger in overweight men. Int. J. Food Sci. Nutr. 2011, 62, 628–635. [Google Scholar] [CrossRef] [PubMed]
- Ye, Z.; Arumugam, V.; Haugabrooks, E.; Williamson, P.; Hendrich, S. Soluble dietary fiber (Fibersol-2) decreased hunger and increased satiety hormones in humans when ingested with a meal. Nutr. Res. 2015, 35, 393–400. [Google Scholar] [CrossRef] [PubMed]
- Astina, J.; Sapwarobol, S. Attenuation of glycaemic and insulin responses following tapioca resistant maltodextrin consumption in healthy subjects: A randomised cross-over controlled trial. J. Nutr. Sci. 2020, 9, e29. [Google Scholar] [CrossRef] [PubMed]
- Wakabayashi, S.; Kishimoto, Y.; Nanbu, S.; Matsuoka, A. Effects of Indigestible Dextrin on Postprandial Rise in Blood Glucose Levels in Man. J. Jpn. Assoc. Diet. Fiber Res. 1999, 3, 13–19. [Google Scholar]
- Wolf, B.W.; Wolever, T.M.; Bolognesi, C.; Zinker, B.A.; Garleb, K.A. Glycemic response to a rapidly digested starch is not affected by the addition of an indigestible dextrin in humans. Nutr. Res. 2001, 21, 1099–1106. [Google Scholar] [CrossRef]
- Lochs, H.; Allison, S.P.; Meier, R.; Pirlich, M.; Kondrup, J.; Schneider, S.; van den Berghe, G.; Pichard, C. Introductory to the ESPEN Guidelines on Enteral Nutrition: Terminology, Definitions and General Topics. Clin. Nutr. 2006, 25, 180–186. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malone, A.M. Enteral formula selection: A review of selected product categories. Pract. Gastroenterol. 2005, 29, 44–74. [Google Scholar]
- Savino, P. Knowledge of constituent ingredients in enteral nutrition formulas can make a difference in patient response to enteral feeding. Nutr. Clin. Pract. 2018, 33, 90–98. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blundell, J.; De Graaf, C.; Hulshof, T.; Jebb, S.; Livingstone, B.; Lluch, A.; Mela, D.; Salah, S.; Schuring, E.; Van Der Knaap, H. Appetite control: Methodological aspects of the evaluation of foods. Obes. Rev. 2010, 11, 251–270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lawless, H.T.; Heymann, H. Sensory Evaluation of Food: Principles and Practices; Springer Science & Business Media: New York, NY, USA, 2013. [Google Scholar]
- Jacqz-Aigrain, E.; Kassai, B.; Cornu, C.; Cazaubiel, J.M.; Housez, B.; Cazaubiel, M.; Prevel, J.M.; Bell, M.; Boileau, A.; de Cock, P. Gastrointestinal tolerance of erythritol-containing beverage in young children: A double-blind, randomised controlled trial. Eur. J. Clin. Nutr. 2015, 69, 746–751. [Google Scholar] [CrossRef]
- Lewis, S.J.; Heaton, K.W. Stool form scale as a useful guide to intestinal transit time. Scand. J. Gastroenterol. 1997, 32, 920–924. [Google Scholar] [CrossRef] [PubMed]
- Tan, W.S.; Chia, P.F.; Ponnalagu, S.; Karnik, K.; Henry, C.J. The Role of Soluble Corn Fiber on Glycemic and Insulin Response. Nutrients 2020, 12, 961. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brouns, F.; Bjorck, I.; Frayn, K.; Gibbs, A.; Lang, V.; Slama, G.; Wolever, T. Glycaemic index methodology. Nutr. Res. Rev. 2005, 18, 145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Devitt, A.A.; Williams, J.A.; Choe, Y.S.; Hustead, D.S.; Mustad, V.A. Glycemic responses to glycemia-targeted specialized-nutrition beverages with varying carbohydrates compared to a standard nutritional beverage in adults with type 2 diabetes. Adv. Biosci. Biotechnol. 2013, 4, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Friedewald, W.T.; Levy, R.I.; Fredrickson, D.S. Estimation of the Concentration of Low-Density Lipoprotein Cholesterol in Plasma, Without Use of the Preparative Ultracentrifuge. Clin. Chem. 1972, 18, 499–502. [Google Scholar] [CrossRef] [PubMed]
- National Institute of Health CKD-EPI Adults (Conventional Units). Available online: https://www.niddk.nih.gov/health-information/professionals/clinical-tools-patient-management/kidney-disease/laboratory-evaluation/glomerular-filtration-rate-calculators/ckd-epi-adults-conventional-units (accessed on 22 November 2021).
- Institute of Nutrition, M.U. Food Composition Database for INMUCAL Program; Institute of Nutrition, Mahidol University Bangkok: Bangkok, Thailand, 2005. [Google Scholar]
- Armstrong, T.; Bull, F. Development of the World Health Organization Global Physical Activity Questionnaire (GPAQ). J. Public Health 2006, 14, 66–70. [Google Scholar] [CrossRef]
- Pohl, M.; Mayr, P.; Mertl-Roetzer, M.; Lauster, F.; Lerch, M.; Eriksen, J.; Haslbeck, M.; Rahlfs, V.W. Glycaemic control in type II diabetic tube-fed patients with a new enteral formula low in carbohydrates and high in monounsaturated fatty acids: A randomised controlled trial. Eur. J. Clin. Nutr. 2005, 59, 1221–1232. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Faul, F.; Erdfelder, E.; Lang, A.-G.; Buchner, A. G* Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Anjom-Shoae, J.; Keshteli, A.H.; Sadeghi, O.; Pouraram, H.; Afshar, H.; Esmaillzadeh, A.; Adibi, P. Association between dietary insulin index and load with obesity in adults. Eur. J. Nutr. 2020, 59, 1563–1575. [Google Scholar] [CrossRef]
- American Diabetes, A. 2. Classification and diagnosis of diabetes: Standards of Medical Care in Diabetes—2021. Diabetes Care 2021, 44 (Suppl. S1), S15–S33. [Google Scholar] [CrossRef] [PubMed]
- Juntunen, K.S.; Laaksonen, D.E.; Autio, K.; Niskanen, L.K.; Holst, J.J.; Savolainen, K.E.; Liukkonen, K.-H.; Poutanen, K.S.; Mykkänen, H.M. Structural differences between rye and wheat breads but not total fiber content may explain the lower postprandial insulin response to rye bread. Am. J. Clin. Nutr. 2003, 78, 957–964. [Google Scholar] [CrossRef] [PubMed]
- Eelderink, C.; Schepers, M.; Preston, T.; Vonk, R.J.; Oudhuis, L.; Priebe, M.G. Slowly and rapidly digestible starchy foods can elicit a similar glycemic response because of differential tissue glucose uptake in healthy men. Am. J. Clin. Nutr. 2012, 96, 1017–1024. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Canfora, E.E.; Jocken, J.W.; Blaak, E.E. Short-chain fatty acids in control of body weight and insulin sensitivity. Nat. Rev. Endocrinol. 2015, 11, 5Ora77-91. [Google Scholar] [CrossRef]
- Kishimoto, Y.; Yoshikawa, Y.; Miyazato, S.; Oga, H.; Yamada, T.; Tagami, H.; Hashizume, C.; Yamamoto, K. Effect of resistant maltodextrin on digestion and absorption of lipids. J. Health Sci. 2009, 55, 838–844. [Google Scholar] [CrossRef] [Green Version]
- Bhoite, R.; Chandrasekaran, A.; Pratti, V.L.; Satyavrat, V.; Aacharya, S.; Mane, A.; Mehta, S.; Kale, R.M.; Nagamuthu, G.; Selvaraj, S. Effect of a High-Protein High-Fibre Nutritional Supplement on Lipid Profile in Overweight/Obese Adults with Type 2 Diabetes Mellitus: A 24-Week Randomized Controlled Trial. J. Nutr. Metab. 2021, 2021, 6634225. [Google Scholar] [CrossRef]
- Silverman, M.G.; Ference, B.A.; Im, K.; Wiviott, S.D.; Giugliano, R.P.; Grundy, S.M.; Braunwald, E.; Sabatine, M.S. Association between lowering LDL-C and cardiovascular risk reduction among different therapeutic interventions: A systematic review and meta-analysis. JAMA 2016, 316, 1289–1297. [Google Scholar] [CrossRef] [Green Version]
- Packard, C.; Chapman, M.J.; Sibartie, M.; Laufs, U.; Masana, L. Intensive low-density lipoprotein cholesterol lowering in cardiovascular disease prevention: Opportunities and challenges. Heart 2021, 107, 1369–1375. [Google Scholar] [CrossRef] [PubMed]
- Guérin-Deremaux, L.; Pochat, M.; Reifer, C.; Wils, D.; Cho, S.; Miller, L.E. The soluble fiber NUTRIOSE induces a dose-dependent beneficial impact on satiety over time in humans. Nutr. Res. 2011, 31, 665–672. [Google Scholar] [CrossRef] [PubMed]
- Guérin-Deremaux, L.; Pochat, M.; Reifer, C.; Wils, D.; Cho, S.; Miller, L.E. Dose-response impact of a soluble fiber, NUTRIOSE®, on energy intake, body weight and body fat in humans. Glob. Epidemic Obes. 2013, 1, 2. [Google Scholar] [CrossRef] [Green Version]
- Goda, T.; Kajiya, Y.; Suruga, K.; Tagami, H.; Livesey, G. Availability, fermentability, and energy value of resistant maltodextrin: Modeling of short-term indirect calorimetric measurements in healthy adults. Am. J. Clin. Nutr. 2006, 83, 1321–1330. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Emilien, C.H.; Zhu, Y.; Hsu, W.H.; Williamson, P.; Hollis, J.H. The effect of soluble fiber dextrin on postprandial appetite and subsequent food intake in healthy adults. Nutrition 2018, 47, 6–12. [Google Scholar] [CrossRef]
- Whelan, K.; Efthymiou, L.; Judd, P.A.; Preedy, V.R.; Taylor, M.A. Appetite during consumption of enteral formula as a sole source of nutrition: The effect of supplementing pea-fibre and fructo-oligosaccharides. Br. J. Nutr. 2006, 96, 350–356. [Google Scholar] [CrossRef]
- Templeman, N.M.; Skovsø, S.; Page, M.M.; Lim, G.E.; Johnson, J.D. A causal role for hyperinsulinemia in obesity. J. Endocrinol. 2017, 232, R173–R183. [Google Scholar] [CrossRef] [Green Version]
- Al Hommos, N.A.; Ebenibo, S.; Edeoga, C.; Dagogo-Jack, S. Trajectories of Body Weight and Fat Mass in Relation to Incident Prediabetes in a Biracial Cohort of Free-Living Adults. J. Endocr. Soc. 2021, 5, bvaa164. [Google Scholar] [CrossRef]
- den Boer, A.; Boesveldt, S.; Lawlor, J.B. How sweetness intensity and thickness of an oral nutritional supplement affects intake and satiety. Food Qual. Prefer. 2019, 71, 406–414. [Google Scholar] [CrossRef]
- Eswaran, S.; Muir, J.; Chey, W.D. Fiber and functional gastrointestinal disorders. Am. J. Gastroenterol. 2013, 108, 718–727. [Google Scholar] [CrossRef]
- Continence Foundation of Australia Bristol Stool Chart. Available online: https://www.continence.org.au/bristol-stool-chart (accessed on 24 April 2021).









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Ingredients | Original | TRM15 | TRM30 |
|---|---|---|---|
| Carbohydrate (g) | 32.73 | 32.67 | 32.63 |
| TRM (% of carbohydrate) | 0.00 | 11.74 | 23.48 |
| TM (% of carbohydrate) | 78.26 | 66.52 | 54.78 |
| Sucrose (% of carbohydrate) | 21.74 | 21.74 | 21.74 |
| Protein (g) | 9.85 | 9.85 | 9.85 |
| Whey protein isolate (% of protein) | 49.11 | 49.11 | 49.11 |
| Soy protein isolate (% of protein) | 50.89 | 50.89 | 50.89 |
| Fat (g) | 9.05 | 9.05 | 9.05 |
| Blended omega-3 oil powder (% of fat) | 49.78 | 49.78 | 49.78 |
| Rice bran creamer (% of fat) | 49.78 | 49.78 | 49.78 |
| Soy lecithin (% of fat) | 0.45 | 0.45 | 0.45 |
| Baseline Characteristics | All Subjects (n = 17) |
|---|---|
| Gender (male/female) | 7/10 |
| Age (year) | 26.24 ± 0.62 |
| Body weight (kg) | 56.05 ± 2.02 |
| BMI (kg/m2) | 21.29 ± 0.50 |
| Fasting plasma glucose (mg/dL) Fasting insulin (µIU/mL) | 91.62 ± 1.46 4.87 ± 0.68 |
| Parameters | Pre-DM (n = 9) | Normal (n = 13) | All (n = 22) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Week 0 | Week 12 | p-Value | Week 0 | Week 12 | p-Value | Week 0 | Week 12 | p-Value | |
| FBG (mg/dL) | 100.22 ± 2.44 | 95.78 ± 4.02 | 0.216 | 86.31 ± 1.71 | 89.08 ± 1.76 | 0.175 | 92 ± 2.04 | 91.82 ± 2.02 | 0.924 |
| HbA1C (%) | 5.79 ± 0.06 | 5.5 ± 0.09 | 0.006 * | 5.31 ± 0.05 | 5.00 ± 0.06 | <0.001 * | 5.5 ± 0.07 | 5.2 ± 0.07 | <0.001 * |
| Insulin (µIU/mL) | 12.61 ± 2.8 | 12.77 ± 2.47 | 0.917 | 7.28 ± 0.99 | 7.39 ± 1.09 | 0.942 | 9.46 ± 1.37 | 9.59 ± 1.3 | 0.931 |
| Total cholesterol (mg/dL) | 198.33 ± 7.62 | 193.67 ± 10.46 | 0.508 | 193.31 ± 9.03 | 190.85 ± 5.87 | 0.753 | 195.36 ± 6.07 | 192 ± 5.37 | 0.543 |
| HDL | 45.22 ± 3.51 | 46.67 ± 2.74 | 0.466 | 52.85 ± 4 | 54.85 ± 3.62 | 0.242 | 49.73 ± 2.83 | 51.5 ± 2.52 | 0.156 |
| LDL | 132.33 ± 6.82 | 125.33 ± 8.51 | 0.252 | 121.46 ± 7.91 | 115.46 ± 5.32 | 1.000 | 125.91 ± 5.45 | 119.5 ± 4.69 | 0.247 |
| Triglyceride | 104.11 ± 15.35 | 107 ± 18.81 | 0.857 | 94.46 ± 15.38 | 102.15 ± 12.22 | 0.196 | 98.41 ± 10.85 | 104.14 ± 10.28 | 0.385 |
| AST | 21 ± 2.39 | 22.22 ± 2.38 | 0.522 | 18.23 ± 1.6 | 21.46 ± 3.09 | 0.141 | 19.36 ± 1.36 | 21.77 ± 2.03 | 0.139 |
| ALT | 29.22 ± 5.01 | 35.11 ± 8.01 | 0.319 | 19.08 ± 2.98 | 18.69 ± 3.36 | 0.783 | 23.23 ± 2.84 | 25.41 ± 4.11 | 0.723 |
| BUN | 10.67 ± 0.5 | 10.78 ± 0.88 | 0.834 | 11.23 ± 1.2 | 10.04 ± 0.75 | 0.321 | 11 ± 0.73 | 10.34 ± 0.56 | 0.674 |
| Creatinine | 0.8 ± 0.05 | 0.79 ± 0.04 | 0.434 | 0.78 ± 0.05 | 0.79 ± 0.04 | 0.655 | 0.79 ± 0.03 | 0.79 ± 0.03 | 0.971 |
| eGFR | 110.78 ± 4.8 | 111.11 ± 3.92 | 0.831 | 111.15 ± 3.61 | 111.85 ± 3 | 0.827 | 111 ± 2.83 | 111.55 ± 2.33 | 0.776 |
| Parameter | Pre-DM (n = 9) | Normal (n = 13) | All (n = 22) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Week 0 | Week 12 | p-Value | Week 0 | Week 12 | p-Value | Week 0 | Week 12 | p-Value | |
| Body weight (kg) | 69.84 ± 4.7 | 71.16 ± 4.65 | 0.128 | 62.26 ± 4.12 | 62.21 ± 3.96 | 0.907 | 65.36 ± 3.13 | 65.87 ± 3.1 | 0.252 |
| BMI (kg/m2) | 25.59 ± 1.1 | 26.1 ± 1.06 | 0.140 | 23.5 ± 1.15 | 23.52 ± 1.12 | 0.959 | 24.35 ± 0.83 | 24.58 ± 0.82 | 0.193 |
| Fat (%) | 28.51 ± 2.64 | 29.19 ± 2.55 | 0.381 | 27.17 ± 2.87 | 27.05 ± 2.65 | 0.869 | 27.72 ± 1.97 | 27.92 ± 1.86 | 0.699 |
| Fat mass (kg) | 20.11 ± 2.31 | 20.88 ± 2.2 | 0.303 | 17.26 ± 2.67 | 17.01 ± 2.44 | 0.944 | 18.43 ± 1.82 | 18.59 ± 1.72 | 0.417 |
| FFM (kg) | 49.73 ± 3.59 | 50.27 ± 3.59 | 0.201 | 45 ± 3.29 | 45.21 ± 3.27 | 0.593 | 46.94 ± 2.43 | 47.28 ± 2.43 | 0.211 |
| Muscle mass (kg) | 47.01 ± 3.44 | 47.54 ± 3.45 | 0.201 | 42.53 ± 3.13 | 42.74 ± 3.12 | 0.593 | 44.36 ± 2.32 | 44.7 ± 2.32 | 0.211 |
| BMR (kcal) | 1457 ± 95.24 | 1472 ± 94.81 | 0.184 | 1341.92 ± 86.48 | 1348.69 ± 86.49 | 0.463 | 1389 ± 63.96 | 1399.14 ± 64.04 | 0.139 |
| Visceral fat rating | 8.22 ± 1.3 | 9 ± 1.27 | 0.023 * | 5.31 ± 1.02 | 5.15 ± 0.9 | 0.584 | 6.5 ± 0.84 | 6.73 ± 0.83 | 0.308 |
| Participants | Nutrient | Week 0 | Week 3 | Week 6 | Week 9 | Week 12 | p-Value |
|---|---|---|---|---|---|---|---|
| All participants | Energy (kcal) | 1103.99 ± 75.6 | 1086.98 ± 61.51 | 1164.97 ± 92.03 | 1189.08 ± 74.22 | 1182.67 ± 84.83 | 0.416 |
| (n = 22) | Carbohydrate (g) | 141.77 ± 9.28 | 134.54 ± 9.06 | 145.41 ± 11.74 | 149.76 ± 11.42 | 148.71 ± 11.41 | 0.539 |
| Fat (g) | 39.28 ± 3.77 | 40.41 ± 3.26 | 43.05 ± 4.46 | 42.91 ± 3.05 | 42.75 ± 3.49 | 0.650 | |
| Protein (g) | 45.77 ± 3.77 | 48.3 ± 4.49 | 49.54 ± 4.13 | 50.91 ± 3.78 | 51.31 ± 4.28 | 0.502 | |
| Normal | Energy (kcal) | 1075.93 ± 71.22 | 1050.54 ± 59.84 | 1109.91 ± 81.71 | 1158.42 ± 98.95 | 1173.24 ± 117.7 | 0.593 |
| (n = 13) | Carbohydrate (g) | 141.65 ± 11.87 | 130.82 ± 10.91 | 142.22 ± 10.91 | 145.26 ± 17.18 | 146.78 ± 15.59 | 0.629 |
| Fat (g) | 36.73 ± 3.03 | 38.83 ± 4.33 | 38.95 ± 4.53 | 42.38 ± 3.07 | 41.91 ± 4.87 | 0.190 | |
| Protein (g) | 44.64 ± 4.09 | 45.12 ± 5.43 | 47.62 ± 3.98 | 48.99 ± 4.34 | 52.22 ± 6.46 | 0.247 | |
| Pre-DM | Energy (kcal) | 1144.51 ± 159.17 | 1139.61 ± 126.22 | 1244.5 ± 196.31 | 1233.35 ± 117.12 | 1196.29 ± 126.96 | 0.728 |
| (n = 9) | Carbohydrate (g) | 141.94 ± 15.72 | 139.91 ± 16.2 | 150 ± 24.96 | 156.26 ± 13.74 | 151.51 ± 17.52 | 0.863 |
| Fat (g) | 42.95 ± 8.28 | 42.69 ± 5.15 | 48.97 ± 8.71 | 43.67 ± 6.25 | 43.96 ± 5.15 | 0.525 | |
| Protein (g) | 47.41 ± 7.39 | 52.9 ± 7.79 | 52.3 ± 8.57 | 53.68 ± 7.01 | 50 ± 5.19 | 0.979 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Astina, J.; Saphyakhajorn, W.; Borompichaichartkul, C.; Sapwarobol, S. Tapioca Resistant Maltodextrin as a Carbohydrate Source of Oral Nutrition Supplement (ONS) on Metabolic Indicators: A Clinical Trial. Nutrients 2022, 14, 916. https://doi.org/10.3390/nu14050916
Astina J, Saphyakhajorn W, Borompichaichartkul C, Sapwarobol S. Tapioca Resistant Maltodextrin as a Carbohydrate Source of Oral Nutrition Supplement (ONS) on Metabolic Indicators: A Clinical Trial. Nutrients. 2022; 14(5):916. https://doi.org/10.3390/nu14050916
Chicago/Turabian StyleAstina, Junaida, Weeraya Saphyakhajorn, Chaleeda Borompichaichartkul, and Suwimol Sapwarobol. 2022. "Tapioca Resistant Maltodextrin as a Carbohydrate Source of Oral Nutrition Supplement (ONS) on Metabolic Indicators: A Clinical Trial" Nutrients 14, no. 5: 916. https://doi.org/10.3390/nu14050916