
Are We Sentenced to Pharmacotherapy? Promising Role of Lycopene and Vitamin A in Benign Urologic Conditions

Abstract
:1. Introduction
2. Benign Prostatic Hyperplasia
2.1. BPH Epidemiological Studies
2.2. BPH Experimental Studies
2.3. BPH Clinical Studies
3. Prostatitis
3.1. Prostatitis Experimental Studies
3.2. Prostatitis Clinical Studies
4. UTI
4.1. UTI Experimental Studies
4.2. UTI Clinical Studies
5. Urolithiasis
Urolithiasis Experimental Studies
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Borel, P.; Moussa, M.; Reboul, E.; Lyan, B.; Defoort, C.; Vincent-Baudry, S.; Maillot, M.; Gastaldi, M.; Darmon, M.; Portugal, H.; et al. Human Plasma Levels of Vitamin E and Carotenoids Are Associated with Genetic Polymorphisms in Genes Involved in Lipid Metabolism. J. Nutr. 2007, 137, 2653–2659. [Google Scholar] [CrossRef] [Green Version]
- Widjaja-Adhi, M.A.K.; Golczak, M. The Molecular Aspects of Absorption and Metabolism of Carotenoids and Retinoids in Vertebrates. Biochim. Biophys. Acta (BBA) Mol. Cell Biol. Lipids 2020, 1865, 158571. [Google Scholar] [CrossRef]
- Widjaja-Adhi, M.A.K.; Lobo, G.P.; Golczak, M.; von Lintig, J. A Genetic Dissection of Intestinal Fat-Soluble Vitamin and Carotenoid Absorption. Hum. Mol. Genet. 2015, 24, 3206–3219. [Google Scholar] [CrossRef] [Green Version]
- Moran, N.E.; Erdman, J.W.; Clinton, S.K. Complex Interactions between Dietary and Genetic Factors Impact Lycopene Metabolism and Distribution. Arch. Biochem. Biophys. 2013, 539, 171–180. [Google Scholar] [CrossRef] [Green Version]
- Dao, D.Q.; Ngo, T.C.; Thong, N.M.; Nam, P.C. Is Vitamin A an Antioxidant or a Pro-Oxidant? J. Phys. Chem. B 2017, 121, 9348–9357. [Google Scholar] [CrossRef]
- Huang, Z.; Liu, Y.; Qi, G.; Brand, D.; Zheng, S. Role of Vitamin A in the Immune System. J. Clin. Med. 2018, 7, 258. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dulińska-Litewka, J.; Sharoni, Y.; Hałubiec, P.; Łazarczyk, A.; Szafrański, O.; McCubrey, J.A.; Gąsiorkiewicz, B.; Laidler, P.; Bohn, T. Recent Progress in Discovering the Role of Carotenoids and Their Metabolites in Prostatic Physiology and Pathology with a Focus on Prostate Cancer—A Review—Part I: Molecular Mechanisms of Carotenoid Action. Antioxidants 2021, 10, 585. [Google Scholar] [CrossRef] [PubMed]
- Smith, J.W.; Ford, N.A.; Thomas-Ahner, J.M.; Moran, N.E.; Bolton, E.C.; Wallig, M.A.; Clinton, S.K.; Erdman, J.W. Mice Lacking β-Carotene-15,15’-Dioxygenase Exhibit Reduced Serum Testosterone, Prostatic Androgen Receptor Signaling, and Prostatic Cellular Proliferation. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2016, 311, R1135–R1148. [Google Scholar] [CrossRef]
- Agarwal, D.; Are, R. Review Synthèse. Volume 19, 2000. Available online: http://www.chm.bris.ac.uk/org/aggarwal/publications.php(accessed on 6 February 2022).
- Palozza, P.; Catalano, A.; Simone, R.; Cittadini, A. Lycopene as a Guardian of Redox Signalling. Acta Biochim. Pol. 2012, 59, 21–25. [Google Scholar]
- Mustra Rakic, J.; Liu, C.; Veeramachaneni, S.; Wu, D.; Paul, L.; Ausman, L.M.; Wang, X.-D. Dietary Lycopene Attenuates Cigarette Smoke-Promoted Nonalcoholic Steatohepatitis by Preventing Suppression of Antioxidant Enzymes in Ferrets. J. Nutr. Biochem. 2021, 91, 108596. [Google Scholar] [CrossRef] [PubMed]
- Rao, A.V.; Ray, M.R.; Rao, L.G. Lycopene. In Advances in Food and Nutrition Research; Elservier: Amsterdam, The Netherlands, 2006; pp. 99–164. [Google Scholar]
- Veeramachaneni, S.; Ausman, L.M.; Choi, S.W.; Russell, R.M.; Wang, X.-D. High Dose Lycopene Supplementation Increases Hepatic Cytochrome P4502E1 Protein and Inflammation in Alcohol-Fed Rats. J. Nutr. 2008, 138, 1329–1335. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nahum, A.; Zeller, L.; Danilenko, M.; Prall, O.W.J.; Watts, C.K.W.; Sutherland, R.L.; Levy, J.; Sharoni, Y. Lycopene Inhibition of IGF-Induced Cancer Cell Growth Depends on the Level of Cyclin D1. Eur. J. Nutr. 2006, 45, 275–282. [Google Scholar] [CrossRef] [PubMed]
- Wood, S.M.; Beckham, C.; Yosioka, A.; Darban, H.; Watson, R.R. β-Carotene and Selenium Supplementation Enhances Immune Response in Aged Humans. Integr. Med. 2000, 2, 85–92. [Google Scholar] [CrossRef]
- Choi, S.; Kim, H. The Remedial Potential of Lycopene in Pancreatitis through Regulation of Autophagy. Int. J. Mol. Sci. 2020, 21, 5775. [Google Scholar] [CrossRef]
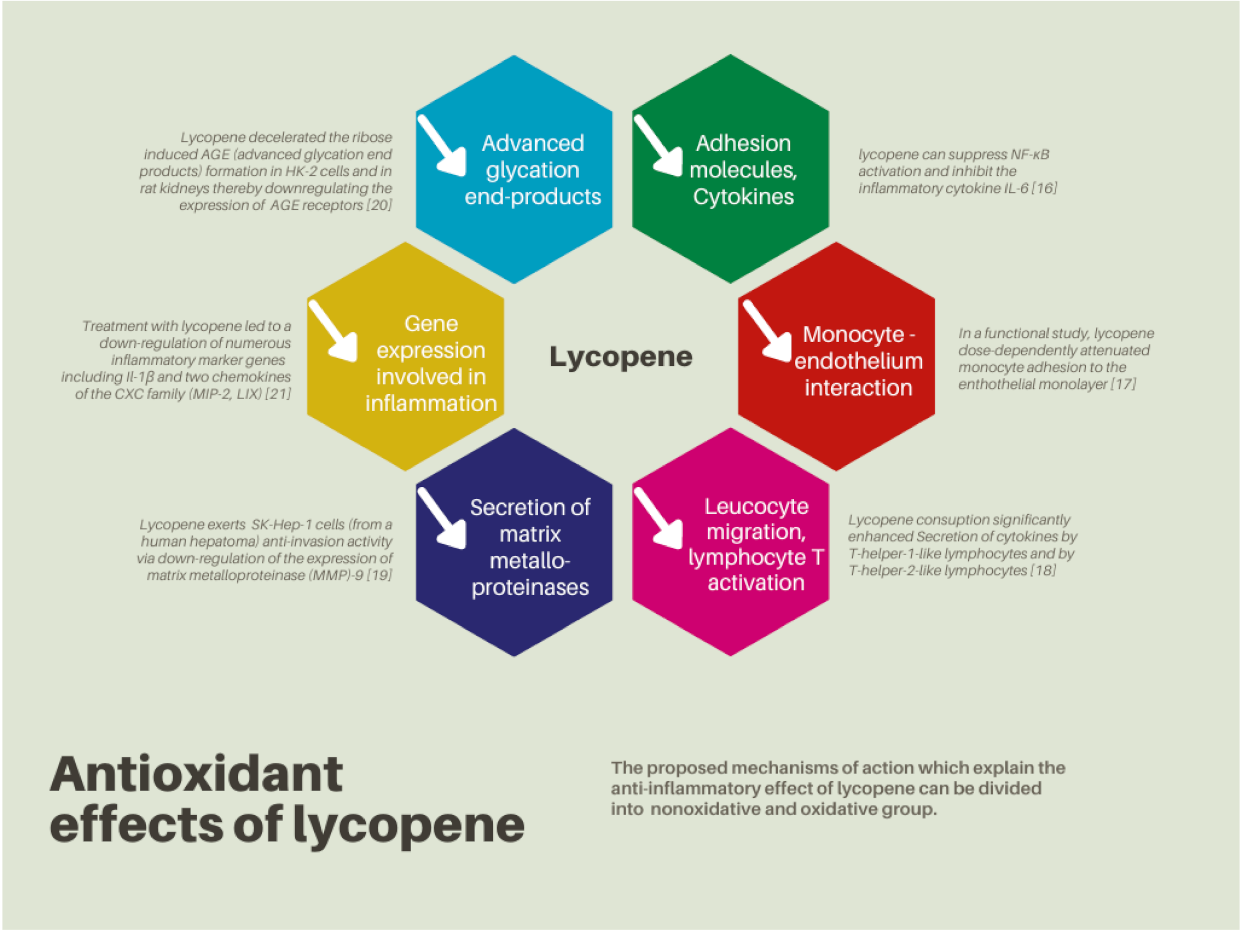
- Hung, C.-F.; Huang, T.-F.; Chen, B.-H.; Shieh, J.-M.; Wu, P.-H.; Wu, W.-B. Lycopene Inhibits TNF-α-Induced Endothelial ICAM-1 Expression and Monocyte-Endothelial Adhesion. Eur. J. Pharmacol. 2008, 586, 275–282. [Google Scholar] [CrossRef]
- Watzl, B.; Bub, A.; Brandstetter, B.R.; Rechkemmer, G. Modulation of Human T-Lymphocyte Functions by the Consumption of Carotenoid-Rich Vegetables. Br. J. Nutr. 1999, 82, 383–389. [Google Scholar] [CrossRef] [Green Version]
- Huang, C.-S.; Fan, Y.-E.; Lin, C.-Y.; Hu, M.-L. Lycopene Inhibits Matrix Metalloproteinase-9 Expression and down-Regulates the Binding Activity of Nuclear Factor-Kappa B and Stimulatory Protein-1. J. Nutr. Biochem. 2007, 18, 449–456. [Google Scholar] [CrossRef]
- Tabrez, S.; Al-Shali, K.Z.; Ahmad, S. Lycopene Powers the Inhibition of Glycation-Induced Diabetic Nephropathy: A Novel Approach to Halt the AGE-RAGE Axis Menace. BioFactors 2015, 41, 372–381. [Google Scholar] [CrossRef]
- Herzog, A.; Siler, U.; Spitzer, V.; Seifert, N.; Denelavas, A.; Hunziker, P.B.; Hunziker, W.; Goralczyk, R.; Wertz, K. Lycopene Reduced Gene Expression of Steroid Targets and Inflammatory Markers in Normal Rat Prostate. FASEB J. 2005, 19, 1–24. [Google Scholar] [CrossRef]
- Mozos, I.; Stoian, D.; Caraba, A.; Malainer, C.; Horbańczuk, J.O.; Atanasov, A.G. Lycopene and Vascular Health. Front. Pharmacol. 2018, 9. [Google Scholar] [CrossRef]
- di Mascio, P.; Kaiser, S.; Sies, H. Lycopene as the Most Efficient Biological Carotenoid Singlet Oxygen Quencher. Arch. Biochem. Biophys. 1989, 274, 532–538. [Google Scholar] [CrossRef]
- Kong, K.-W.; Khoo, H.-E.; Prasad, K.N.; Ismail, A.; Tan, C.-P.; Rajab, N.F. Revealing the Power of the Natural Red Pigment Lycopene. Molecules 2010, 15, 959–987. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boon, C.S.; Xu, Z.; Yue, X.; Julian, D.; Weiss, J.; Decker, E.A. Factors Affecting Lycopene Oxidation in Oil-in-Water Emulsions. J. Agric. Food Chem. 2008, 56, 1408–1414. [Google Scholar] [CrossRef]
- Chen, Y.; Xiao, W.; Wang, Y.; Liu, H.; Li, X.; Yuan, Y. Lycopene Overproduction in Saccharomyces Cerevisiae through Combining Pathway Engineering with Host Engineering. Microb. Cell Factories 2016, 15, 113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, J.; Xu, X.; Xu, Q.; Zhang, Z.; Jiang, L.; Huang, H. Efficient Production of Lycopene by Engineered E. Coli Strains Harboring Different Types of Plasmids. Bioprocess Biosyst. Eng. 2018, 41, 489–499. [Google Scholar] [CrossRef]
- Sies, H.; Jones, D. Oxidative Stress 3. In Encyclopedia of Stress; Elsevier/Academic Press: London, UK, 2007; pp. 45–48. [Google Scholar]
- Roleira, F.M.F.; Tavares-da-Silva, E.J.; Varela, C.L.; Costa, S.C.; Silva, T.; Garrido, J.; Borges, F. Plant Derived and Dietary Phenolic Antioxidants: Anticancer Properties. Food Chem. 2015, 183, 235–258. [Google Scholar] [CrossRef]
- Petyaev, I.M. Lycopene Deficiency in Ageing and Cardiovascular Disease. Oxidative Med. Cell. Longev. 2016, 2016, 3218605. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heber, D.; Lu, Q.-Y. Overview of Mechanisms of Action of Lycopene. Exp. Biol. Med. 2002, 227, 920–923. [Google Scholar] [CrossRef]
- Bramley, P.M. Is Lycopene Beneficial to Human Health? Phytochemistry 2000, 54, 233–236. [Google Scholar] [CrossRef]
- Shi, J. Lycopene in Tomatoes: Chemical and Physical Properties Affected by Food Processing. Crit. Rev. Biotechnol. 2000, 20, 293–334. [Google Scholar] [CrossRef]
- Porrini, M.; Riso, P. Promises and Perils of Lycopene/Tomato Supplementation and Cancer Prevention What Are Typical Lycopene Intakes? J. Nutr. 2005, 135, 2074S. [Google Scholar] [CrossRef] [Green Version]
- Stahl, W.; Sies, H. Uptake of Lycopene and Its Geometrical Isomers Is Greater from Heat-Processed than from Unprocessed Tomato Juice in Humans. J. Nutr. 1992, 122, 2161–2166. [Google Scholar] [CrossRef]
- Egan, K.B. The Epidemiology of Benign Prostatic Hyperplasia Associated with Lower Urinary Tract Symptoms. Urol. Clin. N. Am. 2016, 43, 289–297. [Google Scholar] [CrossRef] [PubMed]
- Parsons, J.K.; Patel, N. Epidemiology and Etiology of Benign Prostatic Hyperplasia and Bladder Outlet Obstruction. Indian J. Urol. 2014, 30, 170. [Google Scholar] [CrossRef] [PubMed]
- Ramello, A.; Vitale, C.; Marangella, M. Epidemiology of Nephrolithiasis. J. Nephrol. 2000, 13, S45–S50. [Google Scholar]
- Gushchin, B.; Me, F. Epidemiological Data on the Prevalent Diagnostic and Treatment Procedures for Chronic Prostatitis in the Ambulatory Care Setting. In Presented at the National Institutes of Health, International Prostatitis Collaborative Network. In Proceedings of the 3rd Annual Meeting, Arlington, VA, USA, 23 October 2000. [Google Scholar]
- Schappert, S.M.; Rechtsteiner, E.A. Ambulatory Medical Care Utilization Estimates for 2006; National Health Statistics Report; no 8; US Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Health Statistics: Hyattsville, MD, USA, 2008; pp. 1–29. [Google Scholar]
- Beebe-Dimmer, J.L.; Wood, D.P.; Gruber, S.B.; Douglas, J.A.; Bonner, J.D.; Mohai, C.; Zuhlke, K.A.; Shepherd, C.; Cooney, K.A. Use of Complementary and Alternative Medicine in Men with Family History of Prostate Cancer: A Pilot Study. Urology 2004, 63, 282–287. [Google Scholar] [CrossRef] [PubMed]
- Auffenberg, G.B.; Helfand, B.T.; McVary, K.T. Established Medical Therapy for Benign Prostatic Hyperplasia. Urol. Clin. N. Am. 2009, 36, 443–459. [Google Scholar] [CrossRef] [PubMed]
- Mcnicholas, T.; Kirby, R. Benign Prostatic Hyperplasia and Male Lower Urinary Tract Symptoms (LUTS). BMJ Clin. Evid. 2011, 2011, 1801. [Google Scholar]
- Steers, W.D. 5α-Reductase Activity in the Prostate. Urology 2001, 58, 17–24. [Google Scholar] [CrossRef]
- Lepor, H. Medical Treatment of Benign Prostatic Hyperplasia. Rev. Urol. Dis. State Rev. 2011, 13, 20–33. [Google Scholar] [CrossRef]
- Hirshburg, J.M.; Kelsey, P.A.; Therrien, C.A.; Gavino, A.C.; Reichenberg, J.S. Adverse Effects and Safety of 5-Alpha Reductase Inhibitors (Finasteride, Dutasteride): A Systematic Review. J. Clin. Aesthetic Dermatol. 2016, 9, 56. [Google Scholar]
- Dunn, C.J.; Matheson, A.; Faulds, D.M. Tamsulosin. Drugs Aging 2002, 19, 135–161. [Google Scholar] [CrossRef] [PubMed]
- Clinton, S.K.; Emenhiser, C.; Schwartz, S.J.; Bostwick, D.G.; Williams, A.W.; Moore, B.J.; Erdman, J.W.; El, J.W. Cis-Trans Lycopene Isomers, Carotenoids, and Retinol in the Human Prostate. Cancer Epidemiol. Biomark. Prev. 1996, 5, 823. [Google Scholar]
- Palan, P.; Naz, R. Changes in Various Antioxidant Levels in Human Seminal Plasma Related to Immunoinfertility. Arch. Androl. 1996, 36, 139–143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siler, U.; Barella, L.; Spitzer, V.; Schnorr, J.; Lein, M.; Goralczyk, R.; Wertz, K. Lycopene and Vitamin E Interfere with Autocrine/Paracrine Loops in the Dunning Prostate Cancer Model. FASEB J. 2004, 18, 1019–1021. [Google Scholar] [CrossRef]
- Tavani, A.; Longoni, E.; Bosetti, C.; Maso, L.D.; Polesel, J.; Montella, M.; Ramazzotti, V.; Negri, E.; Franceschi, S.; Vecchia, C. la Intake of Selected Micronutrients and the Risk of Surgically Treated Benign Prostatic Hyperplasia: A Case-Control Study from Italy. Eur. Urol. 2006, 50, 549–554. [Google Scholar] [CrossRef]
- Kristal, A.R.; Arnold, K.B.; Schenk, J.M.; Neuhouser, M.L.; Goodman, P.; Penson, D.F.; Thompson, I.M. Dietary Patterns, Supplement Use, and the Risk of Symptomatic Benign Prostatic Hyperplasia: Results from the Prostate Cancer Prevention Trial. Am. J. Epidemiol. 2008, 167, 925–934. [Google Scholar] [CrossRef]
- Obermüller-Jevic, U.C.; Olano-Martin, E.; Corbacho, A.M.; Eiserich, J.P.; van der Vliet, A.; Valacchi, G.; Cross, C.E.; Packer, L. Lycopene Inhibits the Growth of Normal Human Prostate Epithelial Cells In Vitro. J. Nutr. 2003, 133, 3356–3360. [Google Scholar] [CrossRef] [Green Version]
- Bonvissuto, G.; Minutoli, L.; Morgia, G.; Bitto, A.; Polito, F.; Irrera, N.; Marini, H.; Squadrito, F.; Altavilla, D. Effect of Serenoa Repens, Lycopene, and Selenium on Proinflammatory Phenotype Activation: An In Vitro And In Vivo Comparison Study. Urology 2011, 77, 248.e9–248.e16. [Google Scholar] [CrossRef]
- Minutoli, L.; Altavilla, D.; Marini, H.; Rinaldi, M.; Irrera, N.; Pizzino, G.; Bitto, A.; Arena, S.; Cimino, S.; Squadrito, F.; et al. Inhibitors of Apoptosis Proteins in Experimental Benign Prostatic Hyperplasia: Effects of Serenoa Repens, Selenium and Lycopene. J. Biomed. Sci. 2014, 21, 19. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.-S.; Bowen, P.; Chen, L.; Duncan, C.; Ghosh, L.; Sharifi, R.; Christov, K. Effects of Tomato Sauce Consumption on Apoptotic Cell Death in Prostate Benign Hyperplasia and Carcinoma. Nutr. Cancer 2003, 47, 40–47. [Google Scholar] [CrossRef]
- Wang, L.; Hou, Y.; Wang, R.; Pan, Q.; Li, D.; Yan, H.; Sun, Z. Inhibitory Effect of Astaxanthin on Testosterone-Induced Benign Prostatic Hyperplasia in Rats. Mar. Drugs 2021, 19, 652. [Google Scholar] [CrossRef]
- Coulson, S.; Rao, A.; Beck, S.L.; Steels, E.; Gramotnev, H.; Vitetta, L. A Phase II Randomised Double-Blind Placebo-Controlled Clinical Trial Investigating the Efficacy and Safety of ProstateEZE Max: A Herbal Medicine Preparation for the Management of Symptoms of Benign Prostatic Hypertrophy. Complementary Ther. Med. 2013, 21, 172–179. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Liang, W.; Zhang, G. Efficacy and Safety of Lycopene in the Treatment of Benign Prostatic Hyperplasia with Lower Urinary Tract Symptoms. Zhonghua Nan Ke Xue 2019, 25, 1001–1004. [Google Scholar] [PubMed]
- Schwarz, S.; Obermüller-Jevic, U.C.; Hellmis, E.; Koch, W.; Jacobi, G.; Biesalski, H.-K. Lycopene Inhibits Disease Progression in Patients with Benign Prostate Hyperplasia. J. Nutr. 2008, 138, 49–53. [Google Scholar] [CrossRef]
- Carrasco, C.; Blanco, L.; Abengozar, Á. Effects of Lycopene-Enriched, Organic, Extra Virgin Olive Oil on Benign Prostatic Hyperplasia: A Pilot Study. Altern. Health Med. 2021, AT6322, online ahead of print. [Google Scholar]
- Morgia, G.; Russo, G.I.; Voce, S.; Palmieri, F.; Gentile, M.; Giannantoni, A.; Blefari, F.; Carini, M.; Minervini, A.; Ginepri, A.; et al. Serenoa Repens, Lycopene and Selenium versus Tamsulosin for the Treatment of LUTS/BPH. An Italian Multicenter Double-Blinded Randomized Study between Single or Combination Therapy (PROCOMB Trial). Prostate 2014, 74, 1471–1480. [Google Scholar] [CrossRef]
- Krieger, J.N. NIH Consensus Definition and Classification of Prostatitis. JAMA 1999, 282, 236–237. [Google Scholar] [CrossRef]
- Habermacher, G.M.; Chason, J.T.; Schaeffer, A.J. Prostatitis/Chronic Pelvic Pain Syndrome. Annu. Rev. Med. 2006, 57, 195–206. [Google Scholar] [CrossRef]
- Pontari, M.A.; Ruggieri, M.R. Mechanisms in prostatitis/chronic pelvic pain syndrome. J. Urol. 2004, 172, 839–845. [Google Scholar] [CrossRef] [Green Version]
- Zou, Y.; Sun, Q.; Li, J.; Yang, C.; Yang, J.; Zhang, L. Effects of E/Z Isomers of Lycopene on Experimental Prostatic Hyperplasia in Mice. Fitoterapia 2014, 99, 211–217. [Google Scholar] [CrossRef] [PubMed]
- Shahed, A.R.; Shoskes, D.A. Oxidative Stress in Prostatic Fluid of Patients With Chronic Pelvic Pain Syndrome: Correlation With Gram Positive Bacterial Growth and Treatment Response. J. Androl. 2000, 21, 669–675. [Google Scholar] [PubMed]
- de Stefano, D.; Maiuri, M.C.; Simeon, V.; Grassia, G.; Soscia, A.; Cinelli, M.P.; Carnuccio, R. Lycopene, Quercetin and Tyrosol Prevent Macrophage Activation Induced by Gliadin and IFN-γ. Eur. J. Pharmacol. 2007, 566, 192–199. [Google Scholar] [CrossRef]
- Han, C.H.; Yang, C.H.; Sohn, D.W.; Kim, S.W.; Kang, S.H.; Cho, Y.-H. Synergistic Effect between Lycopene and Ciprofloxacin on a Chronic Bacterial Prostatitis Rat Model. Int. J. Antimicrob. Agents 2008, 31, 102–107. [Google Scholar] [CrossRef]
- Morgia, G.; Cimino, S.; Favilla, V.; Russo, G.I.; Squadrito, F.; Mucciardi, G.; Masieri, L.; Minutoli, L.; Grosso, G.; Castelli, T. Effects of Serenoa Repens, Selenium and Lycopene (Profluss®) on Chronic Inflammation Associated with Benign Prostatic Hyperplasia: Results of “FLOG” (Flogosis and Profluss in Prostatic and Genital Disease), a Multicentre Italian Study. Int. Braz. J. Urol. 2013, 39, 214–221. [Google Scholar] [CrossRef]
- Morgia, G.; Mucciardi, G.; Galì, A.; Madonia, M.; Marchese, F.; di Benedetto, A.; Romano, G.; Bonvissuto, G.; Castelli, T.; Macchione, L.; et al. Treatment of chronic prostatitis/chronic pelvic pain syndrome category IIIA with Serenoa repens plus selenium and lycopene (profluss®) versus S. repens alone: An Italian randomized multicenter-controlled study. Urol. Int. 2010, 84, 400–406. [Google Scholar] [CrossRef]
- Cai, T.; Tiscione, D.; Gallelli, L.; Verze, P.; Palmieri, A.; Mirone, V.; Bartoletti, R.; Malossini, G. Serenoa Repens Associated with Selenium and Lycopene Extract and Bromelain and Methylsulfonylmethane Extract Are Able to Improve the Efficacy of Levofloxacin in Chronic Bacterial Prostatitis Patients. Arch. Ital. Urol. E Androl. 2016, 88, 177. [Google Scholar] [CrossRef] [Green Version]
- Laupland, K.B.; Ross, T.; Pitout, J.D.D.; Church, D.L.; Gregson, D.B. Community-Onset Urinary Tract Infections: A Population-Based Assessment. Infection 2007, 35, 150–153. [Google Scholar] [CrossRef] [PubMed]
- Epp, A.; Larochelle, A. Recurrent Urinary Tract Infection. J. Obstet. Gynaecol. Can. 2017, 39, e422–e431. [Google Scholar] [CrossRef]
- GRIEBLING, T.L. Urologic diseases in america project: Trends in resource use for urinary tract infections in women. J. Urol. 2005, 173, 1281–1287. [Google Scholar] [CrossRef]
- Scholes, D.; Hooton, T.M.; Roberts, P.L.; Stapleton, A.E.; Gupta, K.; Stamm, W.E. Risk Factors for Recurrent Urinary Tract Infection in Young Women. J. Infect. Dis. 2000, 182, 1177–1182. [Google Scholar] [CrossRef] [Green Version]
- Kurutas, E.B.; Ciragil, P.; Gul, M.; Kilinc, M. The Effects of Oxidative Stress in Urinary Tract Infection. Mediat. Inflamm. 2005, 2005, 242–244. [Google Scholar] [CrossRef] [PubMed]
- Gul, M.; Kurutas, E.; Ciragil, P.; Cetinkaya, A.; Kilinc, M.; Aral, M.; Buyukbese, M.A. Urinary Tract Infection Aggravates Oxidative Stress in Diabetic Patients. Tohoku J. Exp. Med. 2005, 206, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jung, C.; Brubaker, L. The Etiology and Management of Recurrent Urinary Tract Infections in Postmenopausal Women. Climacteric 2019, 22, 242–249. [Google Scholar] [CrossRef] [PubMed]
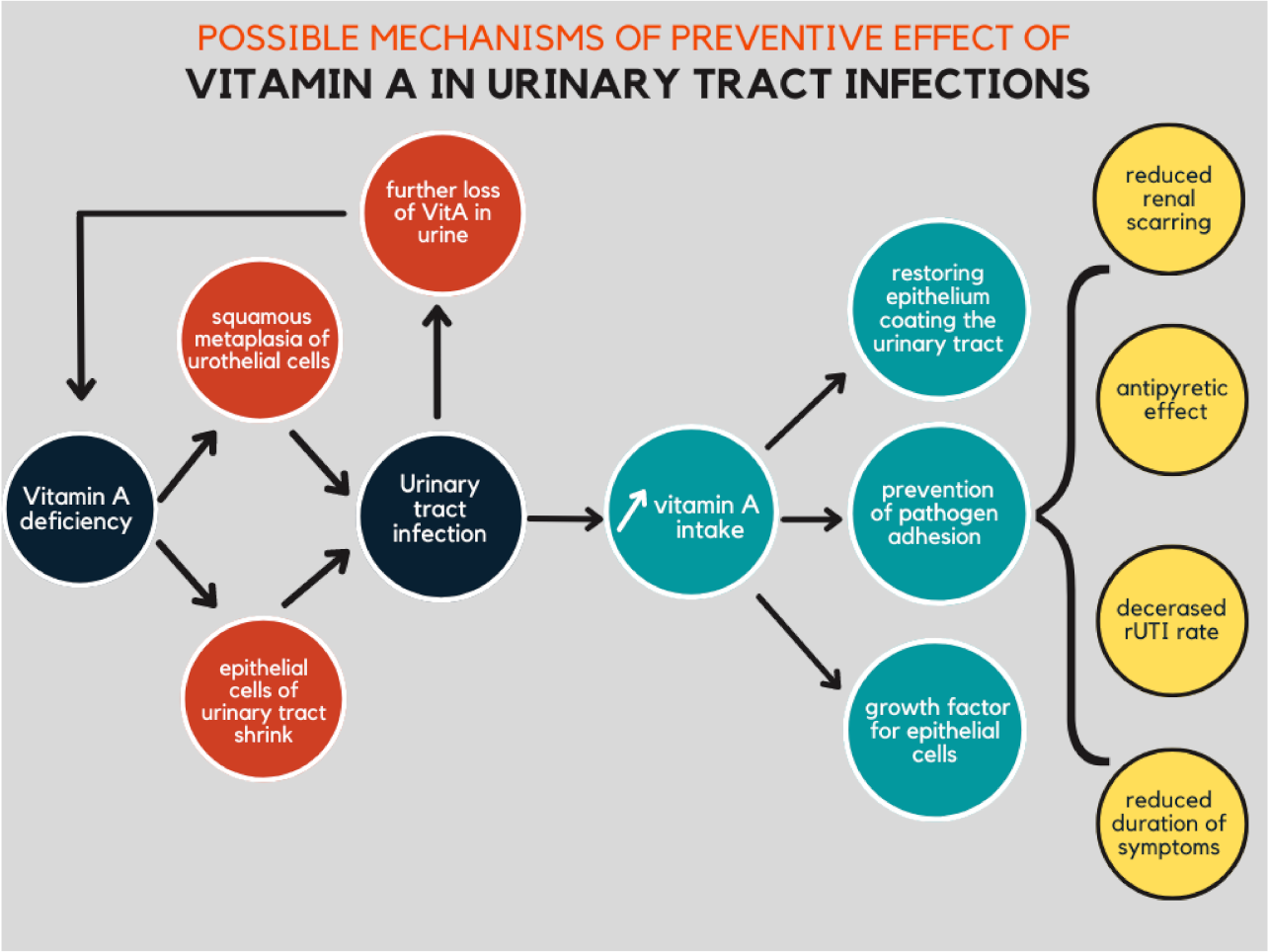
- Friedman, A.; Sklan, D. Antigen-Specific Immune Response Impairment in the Chick as Influenced by Dietary Vitamin A. J. Nutr. 1989, 119, 790–795. [Google Scholar] [CrossRef]
- Chandra, R.K. Increased Bacterial Binding to Respiratory Epithelial Cells in Vitamin A Deficiency. BMJ 1988, 297, 834–835. [Google Scholar] [CrossRef] [Green Version]
- McDowell, E.M.; DeSanti, A.M.; Newkirk, C.; Strum, J.M. Effects of Vitamin A-Deficiency and Inflammation on the Conducting Airway Epithelium of Syrian Golden Hamsters. Virchows Arch. B Cell Pathol. Incl. Mol. Pathol. 1990, 59, 231–242. [Google Scholar] [CrossRef]
- Munday, J.; McKinnon, H.; Aberdein, D. Cystitis, Pyelonephritis, and Urolithiasis in Rats Accidentally Fed a Diet Deficient in Vitamin A. J. Am. Assoc. Lab. Anim. Sci. 2009, 48, 790–794. [Google Scholar]
- Kahbazi, M.; Sharafkhah, M.; Yousefichaijan, P.; Taherahmadi, H.; Rafiei, M.; Kaviani, P.; Abaszadeh, S.; Massoudifar, A.; Mohammadbeigi, A. Vitamin A Supplementation Is Effective for Improving the Clinical Symptoms of Urinary Tract Infections and Reducing Renal Scarring in Girls with Acute Pyelonephritis: A Randomized, Double-Blind Placebo-Controlled, Clinical Trial Study. Complementary Ther. Med. 2019, 42, 429–437. [Google Scholar] [CrossRef]
- Dalirani, R.; Zoshk, Y.; Sharifian, M.; Mohkam, M.; Karimi, A.; Fahimzad, A.; Varzandefar, M. Kidney Diseases Role of Vitamin A in Preventing Renal Scarring After Acute Pyelonephritis. Iran J. Kidney Dis. 2011, 5, 320–323. [Google Scholar]
- Yilmaz, A.; Bahat, E.; Yilmaz, G.G.; Hasanoglu, A.; Akman, S.; Guven, A.G. Adjuvant Effect of Vitamin A on Recurrent Lower Urinary Tract Infections. Pediatrics Int. 2007, 49, 310–313. [Google Scholar] [CrossRef] [PubMed]
- Sakhaee, K. Recent Advances in the Pathophysiology of Nephrolithiasis. Kidney Int. 2009, 75, 585–595. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yasui, T.; Okada, A.; Hamamoto, S.; Ando, R.; Taguchi, K.; Tozawa, K.; Kohri, K. Pathophysiology-Based Treatment of Urolithiasis. Int. J. Urol. 2017, 24, 32–38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Naghii, M.; Jafari, M.; Mofid, M.; Eskandari, E.; Hedayati, M.; Khalagie, K. The Efficacy of Antioxidant Therapy against Oxidative Stress and Androgen Rise in Ethylene Glycol Induced Nephrolithiasis in Wistar Rats. Hum. Exp. Toxicol. 2015, 34, 744–754. [Google Scholar] [CrossRef]
- Grases, F.; Garcia-Gonzalez, R.; Genestar, C.; Torres, J.J.; March, J.G. Vitamin A and Urolithiasis. Clin. Chim. Acta 1998, 269, 147–157. [Google Scholar] [CrossRef]
- Bardaoui, M.; Sakly, R.; Neffati, F.; Najjar, M.F.; el Hani, A. Effect of Vitamin A Supplemented Diet on Calcium Oxalate Renal Stone Formation in Rats. Exp. Toxicol. Pathol. 2010, 62, 573–576. [Google Scholar] [CrossRef]
- Kankesan, J.; Vanama, R.; Renlund, R. Source of a Micro-Nutrient in a Semi-Synthetic Basal Diet as a Causative Factor in Inducing Urinary Calculi in Rats and Its Inhibition by PSC 833, a Potent Inhibitor of P-Glycoprotein. Comp. Med. 2003, 53, 444–447. [Google Scholar]
- Sakly, R.; Fekih, M.; ben Amor, A.; Najjar, M.F.; Mbazaa, M. Rôle Possible de La Carence En Vitamines A et E Dans Les Lithiases Idiopathiques Chez l’homme. Ann. Urol. 2003, 37, 217–219. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Year | Studied Population | Intervention | Results | Ref. |
|---|---|---|---|---|---|
| Carrasco et al. | 2021 | 20 men aged > 50 allocated into one of two groups: healthy-men (n = 10) and BPH (n = 10) | For a period of 30 days, both groups ingested 20 mL of lycopene daily | PSA levels and reported symptoms improved in the BPH group; however, the difference was not statistically significant. The overall antioxidant status was significantly increased in the healthy-men group (p < 0.05) | [61] |
| Coulson et al. | 2012 | 57 men aged 40–80 years with BPH, randomized into intervention and placebo groups | For three months, the patients in the intervention group received one capsule per day of herbal preparation (n = 32). The patients in the second group were given a placebo (n = 25) | The IPSS score in the intervention group decreased by 36%, while in the placebo group, the reduction of symptoms reached 8% (p < 0.05) | [58] |
| Li et al. | 2019 | 120 patients diagnosed with BPH | All the participants consumed lycopene tablets 500 mg twice a day for 1 year | After two and four months of treatment, there was a significant improvement in the IPSS, QoL score, and Qmax compared with the baseline. The prostate volume did not change before and after medication intake | [59] |
| Morgia et al. | 2014 | 225 patients aged 55–80 years | Participants were assigned to group A, consuming SeR–Se–Ly, group B, taking tamsulosin, or group C, receiving both products | The decrease in IPSS score was significantly more noticeable in Group C than group A (p < 0.05) and group B (p < 0.01). The changes in IPSS score and Qmax levels were more pronounced for combination therapy versus monotherapies (<0.05). | [62] |
| Schwarz et al. | 2008 | 40 patients with histologically proven BPH without coexisting prostate cancer | Patients were assigned to lycopene receiving group at a dose of 15 mg/d for six months, or a placebo group | After six months of lycopene intake, PSA levels significantly decreased (p < 0.05). Meanwhile, there was no change in the placebo group. The levels of lycopene assessed in plasma increased after lycopene intervention (p < 0.0001), whereas the concentration of other carotenoids did not change. | [60] |
| Study | Year | Studied Population | Intervention | Results | Ref. |
|---|---|---|---|---|---|
| Cai et al. | 2016 | 79 patients suffering from CBP | The participants were assigned to one of two groups: Group A taking levofloxacin 500 mg once daily for two weeks with lycopene and methylsulfonylmethane addition; Group B receiving only the antibiotic | In group A there was a significant improvement in NIH-CPSI (−17.6 ± 2.65) and IPSS (−12.2 ± 2.33) scores versus Group B (mean difference: −9 ± 1.82; −8.33 ± 1.71, respectively) | [72] |
| Morgia et al. | 2010 | 102 patients suffering from IIIa CP/CPPS, aged 23–49 years | Patients were randomly assigned into two groups: group A receiving Profluss (S. repens, selenium, and lycopene) or group B taking S. repens alone for two months | The NIH-CPSI score significantly improved (p < 0.001) in both groups; the decrease in IPSS score and improvement in the maximum peak flow rate was seen in both arms, but was more pronounced in group A. The decrease of PSA and WBC count (p < 0.007) was only reported in group A | [71] |
| Morgia et al. | 2013 | 168 patients suffering from BPH submitted to prostate biopsy for PCa suspicion. Two additional cores were taken for PCI evaluation | The first group consisted of 108 participants with histological diagnosis of PCI randomized to Profluss group (I) or to control group (Ic). The second group consisted of 60 participants with histological diagnosis of BPH, randomized to Profluss + α-blocker treatment group (II) or to the control group (IIc) | Alleviation of inflammatory state, decrease in mean values of interleukins (CD20, CD3, CD68), and mean PSA levels in group I compared to group Ic. The extension and grading of inflammatory state in group II were also decreased compared to IIc, but not statistically significantly. A statistically significant difference in interleukin levels (CD20, CD3, CD68, CD8) was reported in group II compared to IIc | [70] |
| Study | Year | Material | Intervention | Results | Ref. |
|---|---|---|---|---|---|
| Kahbazi et al. | 2017 | 90 females aged 2–12 years diagnosed with UTIs and the first episode of APN | Participants were randomized into two groups: in addition to antibiotics the intervention group was given 10 days of oral vitamin A while the control group received 10 days of placebo | Duration of symptoms (fever, urinary frequency, and poor feeding) was significantly reduced in the intervention group. The second 99mTc-DMSA scan revealed worsening of patients’ kidney status in 22.2% of participants in the vitamin A group and 44.7% of patients in the placebo group (p = 0.003) | [84] |
| Yilmaz et al. | 2007 | 24 patients with uncomplicated rUTI were included | Patients were randomized into two groups: the first receiving a single dose of 200,000 IU vitamin A in addition to antibiotic treatment and the second being a control group | In the six months after treatment, the chance of suffering rUTI reduced from 3.58 to 0.75 in the intervention group. UTIs were statistically less frequent during the six months follow-up after vitamin A supplementation compared to the control group | [86] |
| Study | Year | Material | Intervention | Results | Ref. |
|---|---|---|---|---|---|
| Bardaoui et al. | 2009 | 24 male Wistar rats were randomized into three groups | Group A was fed a normal diet. Group B was given a lithogenic diet. Group C received a lithogenic diet for three weeks then a vitamin A supplemented diet for the three last weeks. | The glomerular filtration rate and the urinary excretion of citric acid—which fell in group B—were restored in group C. | [91] |
| Munday et al. | 2009 | 100 female Sprague–Dawley rats | Rats were randomized to a group fed with diets that included a vitamin premix or a group fed with albumin or milk powder | Examination of the 44 rats fed the albumin diet (vitamin A deficient diet) that completed the 34-wk experiment revealed urolithiasis in 27%, and nephrolithiasis in 5% | [83] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kutwin, P.; Falkowski, P.; Łowicki, R.; Borowiecka-Kutwin, M.; Konecki, T. Are We Sentenced to Pharmacotherapy? Promising Role of Lycopene and Vitamin A in Benign Urologic Conditions. Nutrients 2022, 14, 859. https://doi.org/10.3390/nu14040859
Kutwin P, Falkowski P, Łowicki R, Borowiecka-Kutwin M, Konecki T. Are We Sentenced to Pharmacotherapy? Promising Role of Lycopene and Vitamin A in Benign Urologic Conditions. Nutrients. 2022; 14(4):859. https://doi.org/10.3390/nu14040859
Chicago/Turabian StyleKutwin, Piotr, Piotr Falkowski, Roman Łowicki, Magdalena Borowiecka-Kutwin, and Tomasz Konecki. 2022. "Are We Sentenced to Pharmacotherapy? Promising Role of Lycopene and Vitamin A in Benign Urologic Conditions" Nutrients 14, no. 4: 859. https://doi.org/10.3390/nu14040859