
Anthropometrics, Dietary Intake and Body Composition in Urea Cycle Disorders and Branched Chain Organic Acidemias: A Case Study of 18 Adults on Low-Protein Diets

 , ,
, ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. General Characteristics, Dietray Intake, Biochemical Parameters and Body Composition
3.1.1. Subject Characteristics
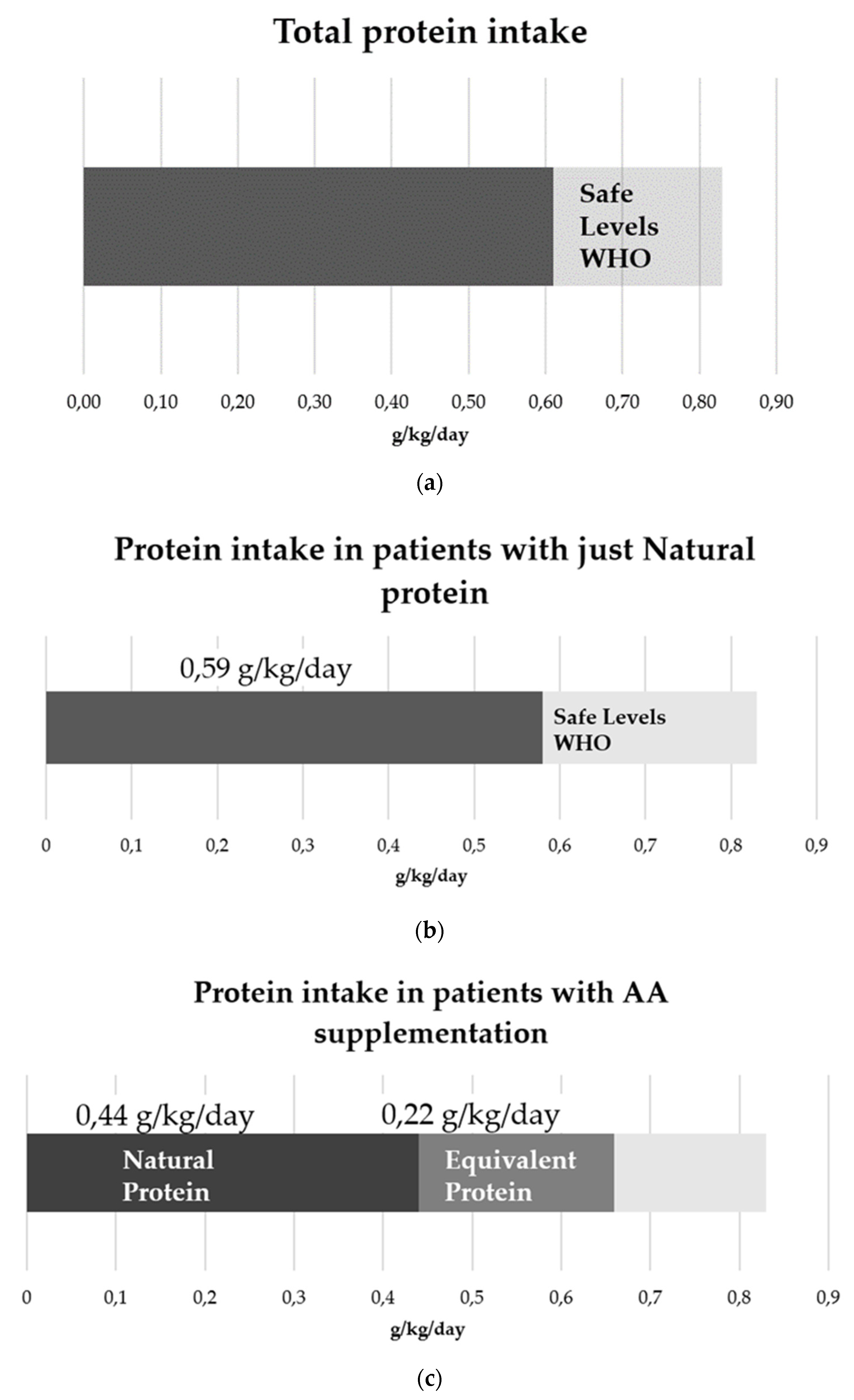
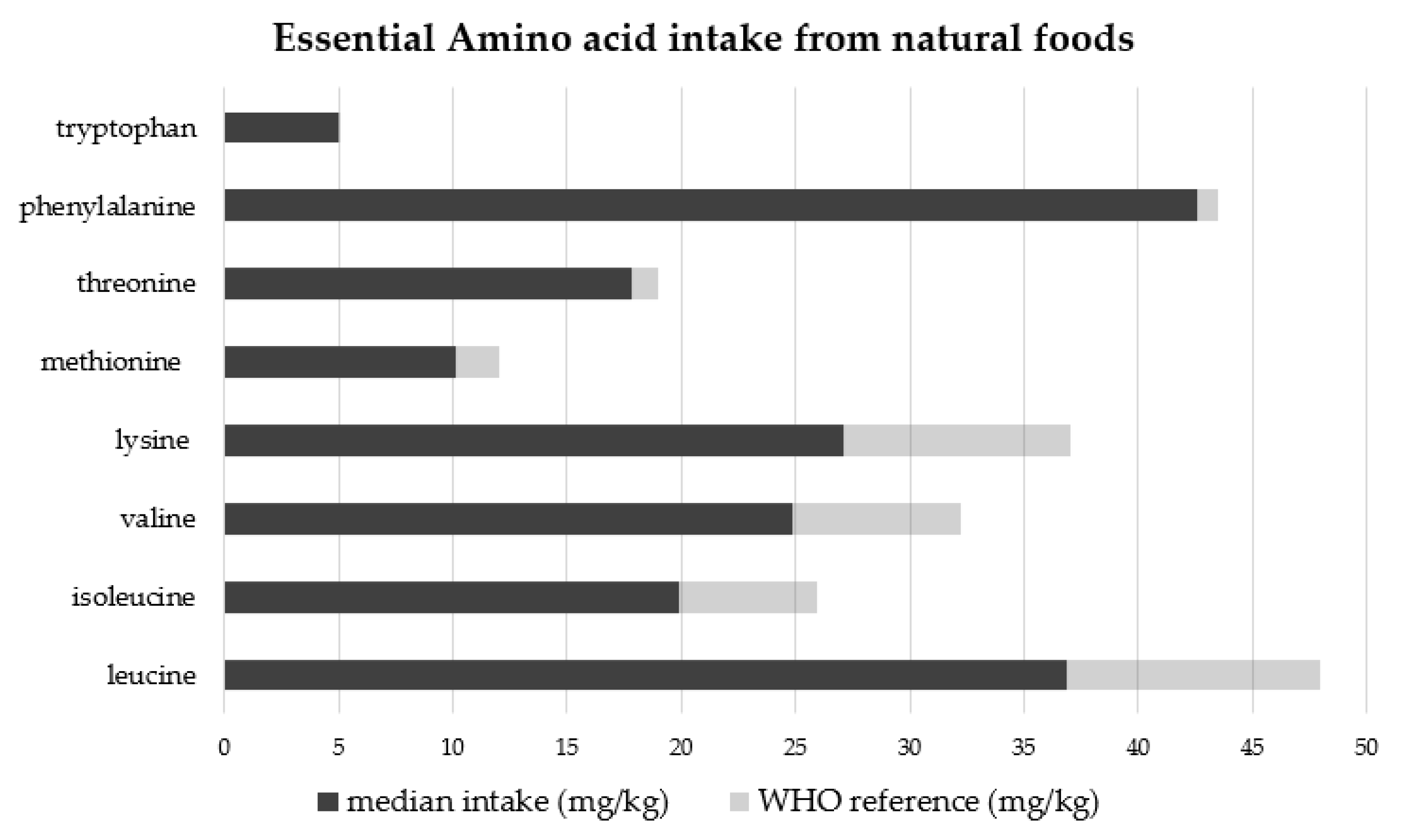
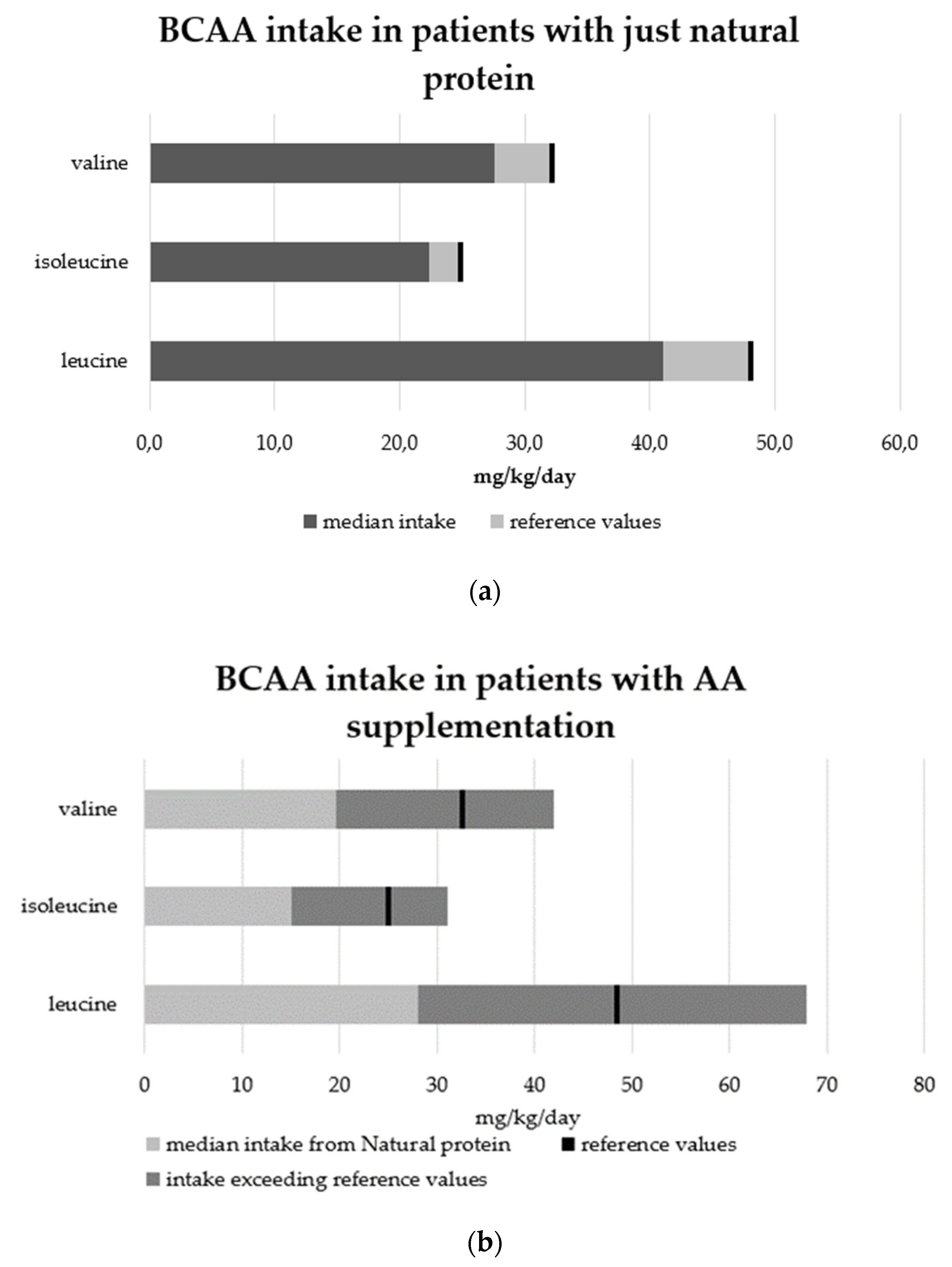
3.1.2. Dietary Intake
3.1.3. Biochemical Parameters
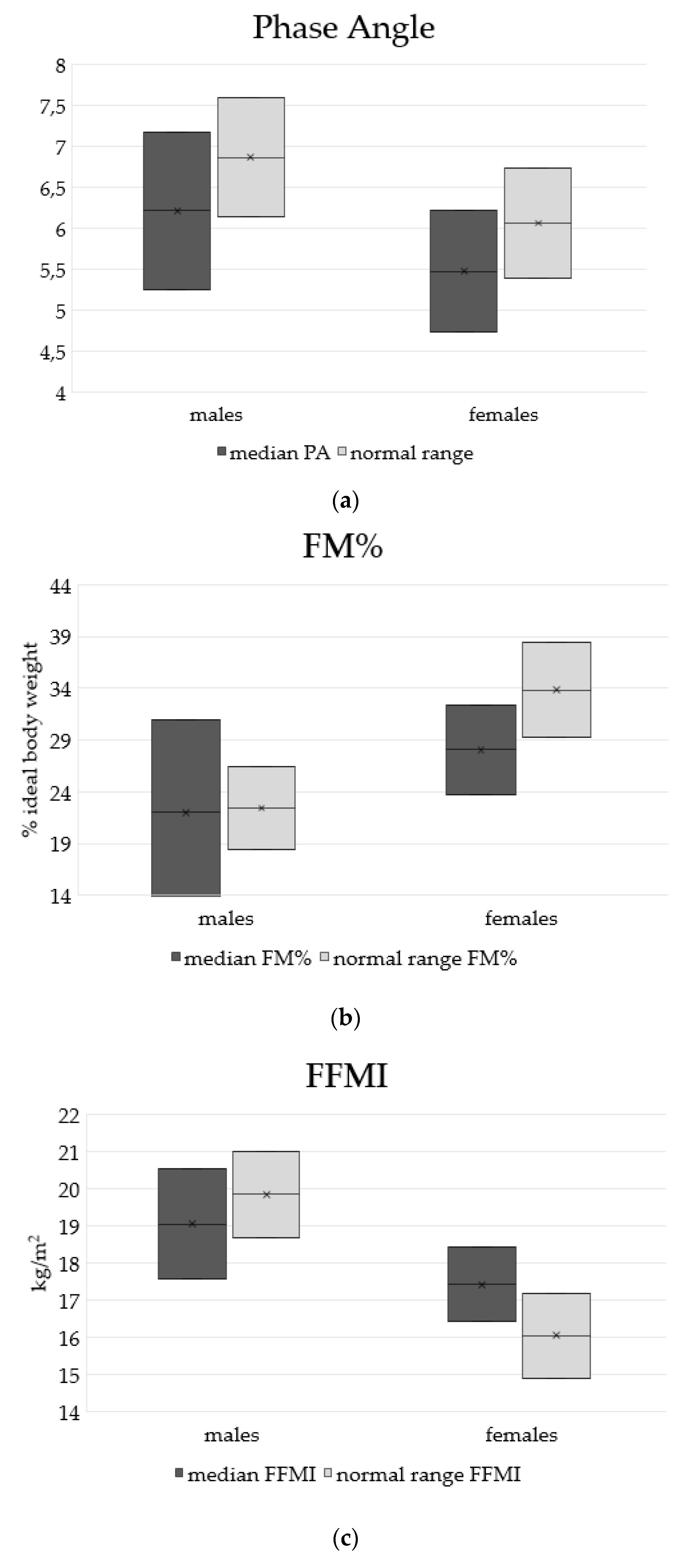
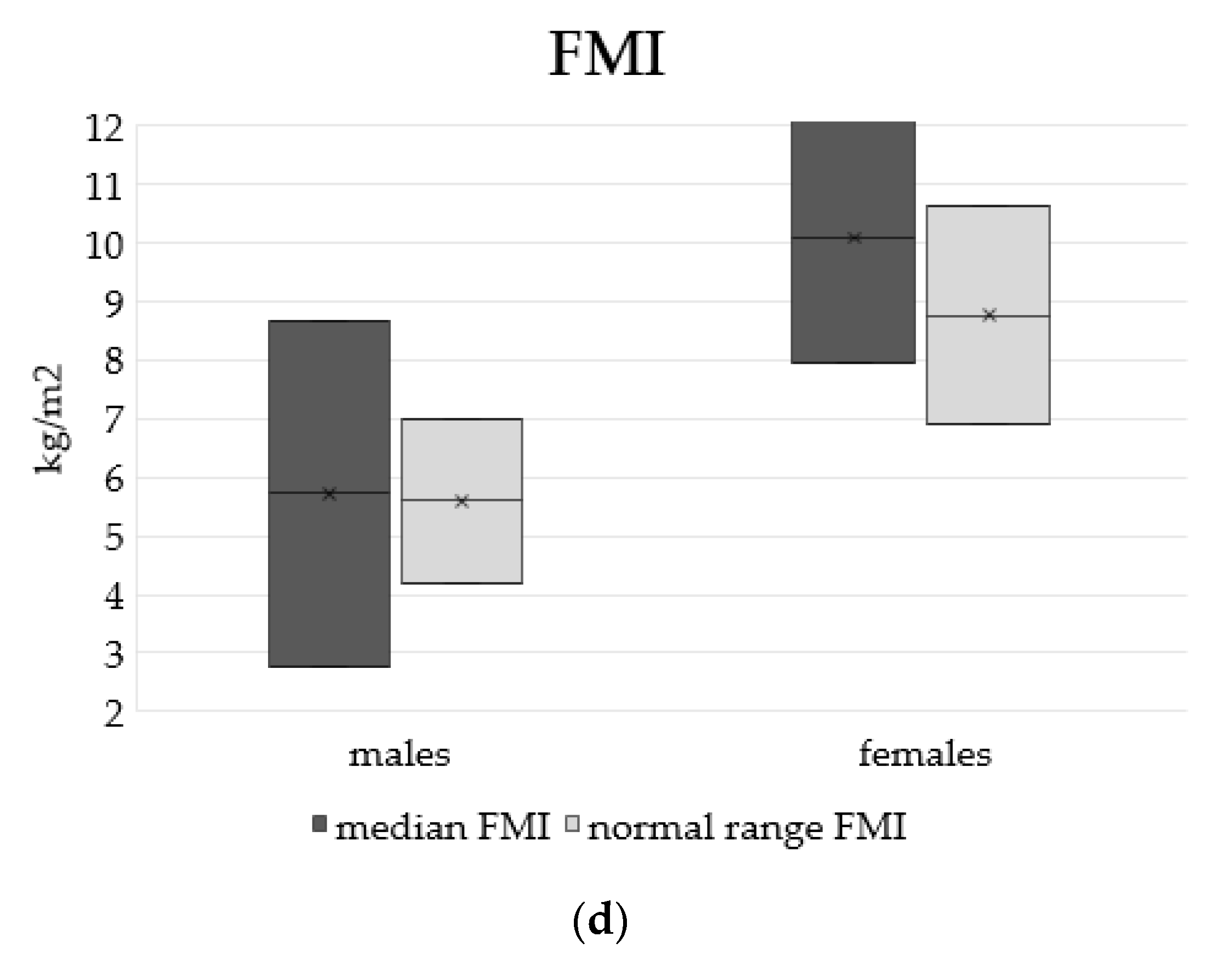
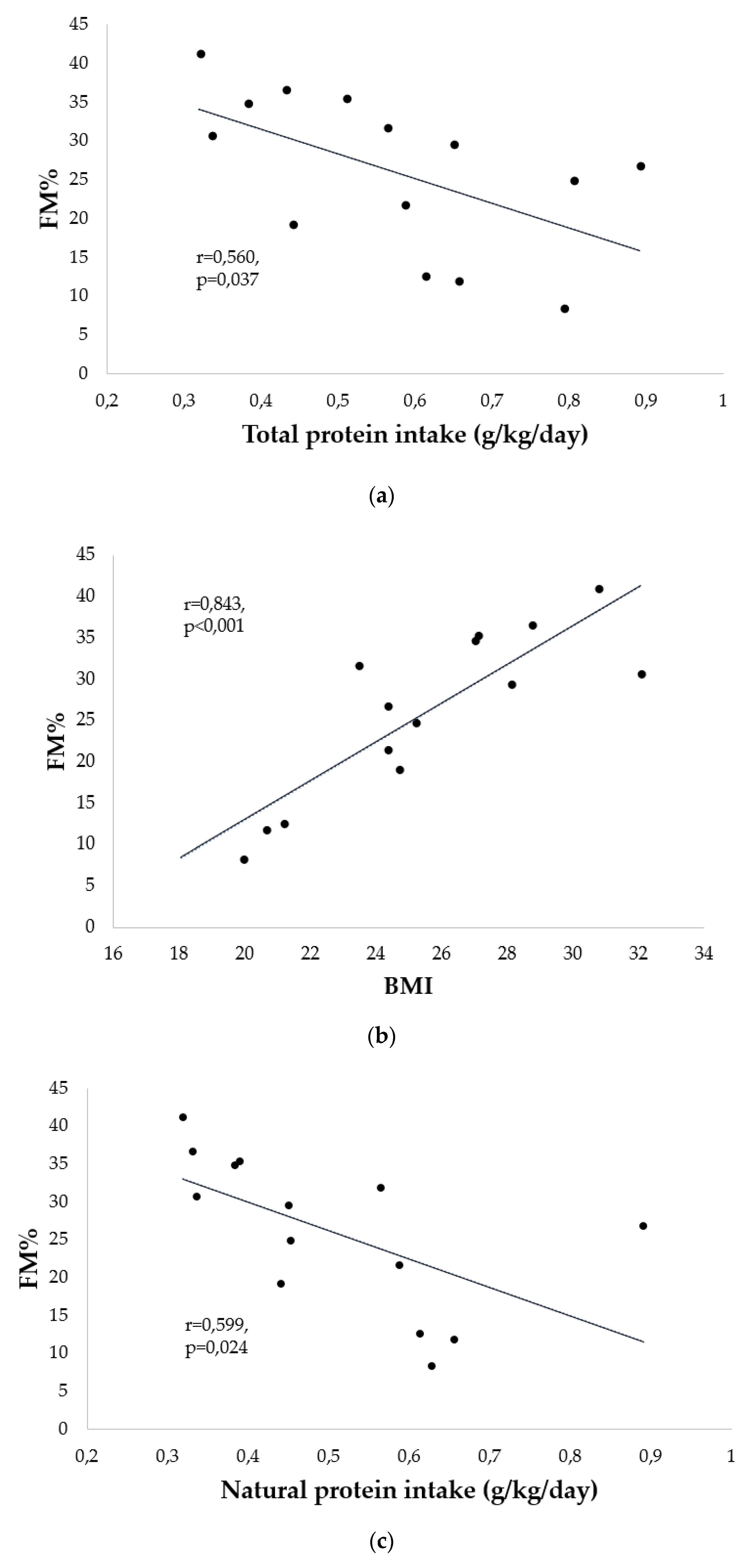
3.1.4. Body Composition
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Boyer, S.W.; Barclay, L.J.; Burrage, L.C. Inherited Metabolic Disorders: Aspects of Chronic Nutrition Management. Nutr. Clin. Pract. 2015, 30, 502–510. [Google Scholar] [CrossRef] [Green Version]
- Häberle, J.; Burlina, A.; Chakrapani, A.; Dixon, M.; Karall, D.; Lindner, M.; Mandel, H.; Martinelli, D.; Pintos-Morell, G.; Santer, R.; et al. Suggested guidelines for the diagnosis and management of urea cycle disorders: First revision. J. Inherit. Metab. Dis. 2019, 42, 1192–1230. [Google Scholar] [CrossRef] [PubMed]
- Forny, P.; Hörster, F.; Ballhausen, D.; Chakrapani, A.; Chapman, K.A.; Dionisi-Vici, C.; Dixon, M.; Grünert, S.C.; Grunewald, S.; Haliloglu, G.; et al. Guidelines for the diagnosis and management of methylmalonic acidaemia and propionic acidaemia: First revision. J. Inherit. Metab. Dis. 2021, 44, 566–592. [Google Scholar] [CrossRef]
- Joint WHO/FAO/UNU Expert Consultation. Protein and amino acid requirements in human nutrition. World Health Organ. Tech. Rep. Ser. 2007, 935, 1–265. [Google Scholar]
- Molema, F.; Gleich, F.; Burgard, P.; van der Ploeg, A.T.; Summar, M.L.; Chapman, K.A.; Barić, I.; Lund, A.M.; Kölker, S.; Williams, M.; et al. Evaluation of dietary treatment and amino acid supplementation in organic acidurias and urea-cycle disorders: On the basis of information from a European multicenter registry. J. Inherit. Metab. Dis. 2019, 42, 1162–1175. [Google Scholar] [CrossRef] [Green Version]
- Van Wegberg, A.M.J.; MacDonald, A.; Ahring, K.; Bélanger-Quintana, A.; Blau, N.; Bosch, A.M.; Burlina, A.; Campistol, J.; Feillet, F.; Giżewska, M.; et al. The complete European guidelines on phenylketonuria: Diagnosis and treatment. Orphanet J. Rare Dis. 2017, 12, 162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Laet, C.; Dionisi-Vici, C.; Leonard, J.V.; McKiernan, P.; Mitchell, G.; Monti, L.; de Baulny, H.O.; Pintos-Morell, G.; Spiekerkötter, U. Recommendations for the management of tyrosinaemia type 1. Orphanet J. Rare Dis. 2013, 8, 8. [Google Scholar] [CrossRef] [Green Version]
- Frazier, D.M.; Allgeier, C.; Homer, C.; Marriage, B.J.; Ogata, B.; Rohr, F.; Splett, P.L.; Stembridge, A.; Singh, R.H. Nutrition management guideline for maple syrup urine disease: An evidence- and consensus-based approach. Mol. Genet. Metab. 2014, 112, 210–217. [Google Scholar] [CrossRef] [PubMed]
- Morris, A.A.M.; Kožich, V.; Santra, S.; Andria, G.; Ben-Omran, T.I.M.; Chakrapani, A.B.; Crushell, E.; Henderson, M.J.; Hochuli, M.; Huemer, M.; et al. Guidelines for the diagnosis and management of cystathionine beta-synthase deficiency. J. Inherit. Metab. Dis. 2017, 40, 49–74. [Google Scholar] [CrossRef] [Green Version]
- Evans, M.; Truby, H.; Boneh, A. The Relationship between Dietary Intake, Growth, and Body Composition in Inborn Errors of Intermediary Protein Metabolism. J. Pediatr. 2017, 188, 163–172. [Google Scholar] [CrossRef]
- de Castro, M.J.; Sánchez-Pintos, P.; Abdelaziz-Salem, N.; Leis, R.; Couce, M.L. Evaluation of body composition, physical activity, and food intake in patients with inborn errors of intermediary metabolism. Nutrients 2021, 13, 2111. [Google Scholar] [CrossRef]
- Molema, F.; Haijes, H.; Janssen, M.; Bosch, A.; van Spronsen, F.; Mulder, M.; Verhoeven-Duif, N.; Jans, J.; van der Ploeg, A.; Wagenmakers, M.; et al. High protein prescription in methylmalonic and propionic acidemia patients and its negative association with long-term outcome. Clin. Nutr. 2021, 40, 3622–3630. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, C.; Pinto, A.; Faria, A.; Teixeira, D.; van Wegberg, A.M.J.; Ahring, K.; Feillet, F.; Calhau, C.; MacDonald, A.; Moreira-Rosário, A.; et al. Is the Phenylalanine-Restricted Diet a Risk Factor for Overweight or Obesity in Patients with Phenylketonuria (PKU)? A Systematic Review and Meta-Analysis. Nutrients 2021, 13, 3443. [Google Scholar] [CrossRef]
- Loeber, J.G.; Platis, D.; Zetterström, R.H.; Almashanu, S.; Boemer, F.; Bonham, J.R.; Borde, P.; Brincat, I.; Cheillan, D.; Dekkers, E.; et al. Neonatal screening in europe revisited: An ISNS perspective on the current state and developments since 2010. Int. J. Neonatal Screen. 2021, 7, 15. [Google Scholar] [CrossRef] [PubMed]
- Burrage, L.C.; McConnell, J.; Haesler, R.; O’Riordan, M.A.; Sutton, V.R.; Kerr, D.S.; McCandless, S.E. High prevalence of overweight and obesity in females with phenylketonuria. Mol. Genet. Metab. 2012, 107, 43–48. [Google Scholar] [CrossRef]
- Aldámiz-Echevarría, L.; Bueno, M.A.; Couce, M.L.; Lage, S.; Dalmau, J.; Vitoria, I.; Andrade, F.; Blasco, J.; Alcalde, C.; Gil, D.; et al. Anthropometric characteristics and nutrition in a cohort of PAH-deficient patients. Clin. Nutr. 2014, 33, 702–717. [Google Scholar] [CrossRef]
- Rocha, J.C.; MacDonald, A.; Trefz, F. Is overweight an issue in phenylketonuria? Mol. Genet. Metab. 2013, 110, S18–S24. [Google Scholar] [CrossRef]
- Dietary Reference Values for nutrients Summary report. EFSA Supporting Publ. 2017, 14, e15121. [CrossRef] [Green Version]
- Coin, A.; Sergi, G.; Minicuci, N.; Giannini, S.; Barbiero, E.; Manzato, E.; Pedrazzoni, M.; Minisola, S.; Rossini, M.; Del Puente, A.; et al. Fat-free mass and fat mass reference values by dual-energy X-ray absorptiometry (DEXA) in a 20–80 year-old Italian population. Clin. Nutr. 2008, 27, 87–94. [Google Scholar] [CrossRef]
- Anja, B.W.; Danielzik, S.; Dörhöfer, R.P.; Later, W.; Wiese, S.; Müller, M.J. Phase angle from bioelectrical impedance analysis: Population reference values by age, sex, and body mass index. J. Parenter. Enter. Nutr. 2006, 30, 309–316. [Google Scholar] [CrossRef]
- Francini-Pesenti, F.; Gugelmo, G.; Lenzini, L.; Vitturi, N. Nutrient intake and nutritional status in adult patients with inherited metabolic diseases treated with low-protein diets: A review on urea cycle disorders and branched chain organic acidemias. Nutrients 2020, 12, 3331. [Google Scholar] [CrossRef] [PubMed]
- Halton, T.L.; Hu, F.B. The effects of high protein diets on thermogenesis, satiety and weight loss: A critical review. J. Am. Coll. Nutr. 2004, 23, 373–385. [Google Scholar] [CrossRef]
- Jahan Mihan, A. The Role of Source of Protein in Regulation of Food Intake, Satiety, Body Weight and Body Composition. J. Nutr. Heal. Food Eng. 2017, 6, 186–193. [Google Scholar] [CrossRef] [Green Version]
- Myles, J.G.; Manoli, I.; Venditti, C.P. Effects of medical food leucine content in the management of methylmalonic and propionic acidemias. Curr. Opin. Clin. Nutr. Metab. Care 2018, 21, 42–48. [Google Scholar] [CrossRef] [PubMed]
- Duan, Y.; Li, F.; Li, Y.; Tang, Y.; Kong, X.; Feng, Z.; Anthony, T.; Watford, M.; Hou, Y.; Wu, G.; et al. The role of leucine and its metabolites in protein and energy metabolism. Amino Acids 2016, 48, 41–51. [Google Scholar] [CrossRef]
- Humphrey, M.; Truby, H.; Boneh, A. New ways of defining protein and energy relationships in inborn errors of metabolism. Mol. Genet. Metab. 2014, 112, 247–258. [Google Scholar] [CrossRef] [PubMed]
- César Rocha, J.; Van Rijn, M.; Van Dam, E.; Ahring, K.; Bélanger-Quintana, A.; Dokoupil, K.; Gokmen Ozel, H.; Lammardo, A.M.; Robert, M.; Heidenborg, C.; et al. Weight Management in Phenylketonuria: What Should Be Monitored? Ann. Nutr. Metab. 2016, 68, 60–65. [Google Scholar] [CrossRef] [Green Version]
- Elagizi, A.; Kachur, S.; Lavie, C.J.; Carbone, S.; Pandey, A.; Ortega, F.B.; Milani, R.V. An Overview and Update on Obesity and the Obesity Paradox in Cardiovascular Diseases. Prog. Cardiovasc. Dis. 2018, 61, 142–150. [Google Scholar] [CrossRef] [Green Version]
- Pes, G.M.; Licheri, G.; Soro, S.; Longo, N.P.; Salis, R.; Tomassini, G.; Niolu, C.; Errigo, A.; Dore, M.P. Overweight: A protective factor against comorbidity in the elderly. Int. J. Environ. Res. Public Health 2019, 16, 3656. [Google Scholar] [CrossRef] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient | Sex | Age | Disease | Body Mass Index | Energy Intake (kcal/kg/day) | Natural Protein Intake (g/kg/day) | Protein Equivalent Intake (g/kg/day) | Total Protein Intake (g/kg/day) | Physical Activity Level | Type of Feeding |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | M | 19 | Methylmalonic acidemia—Cobalamin C type OMIM 277400 | 24.4 | 27.3 | 0.89 | -- | 0.89 | Sedentary | Orally |
| 2 | F | 21 | Glutaric aciduria type 1 OMIM 231670 | 23.5 | 15.5 | 0.56 | -- | 0.56 | Sedentary | Orally |
| 3 | M | 39 | Ornithine transcarbamylase OMIM 300461 | 27.0 | 18.7 | 0.38 | -- | 0.38 | Sedentary | Orally |
| 4 | F | 21 | Citrullinemia OMIM 215700 | 28.8 | 18.6 | 0.33 | 0.10 | 0.43 | Sedentary | Orally |
| 5 | M | 28 | Propionic acidemia OMIM 606054 | 25.2 | 28 | 0.45 | 0.35 | 0.80 | Sedentary | Orally |
| 6 | M | 34 | Argininosuccinic aciduria OMIM 207900 | 24.4 | 22.6 | 0.59 | -- | 0.59 | Sedentary | Orally |
| 7 | F | 38 | Argininosuccinic aciduria OMIM 207900 | 30.8 | 16.2 | 0.32 | -- | 0.32 | Sedentary | Orally |
| 8 | M | 36 | Methylmalonic acidemia—Cobalamin B type OMIM 607568 | 28.1 | 20.9 | 0.45 | 0.20 | 0.65 | Sedentary | Orally |
| 9 | F | 26 | Argininosuccinic aciduria OMIM 207900 | 27.1 | 27.9 | 0.39 | 0.12 | 0.51 | Sedentary | Orally |
| 10 | F | 26 | Methylmalonic acidemia—Cobalamin B type OMIM 607568 | 23.9 | 27.4 | 0.74 | -- | 0.74 | Sedentary—mobilization on wheelchair | Orally |
| 11 | M | 19 | Argininosuccinic aciduria OMIM 207900 | 20.7 | 31.2 | 0.66 | -- | 0.66 | Sedentary | Orally |
| 12 | M | 17 | Argininosuccinic aciduria OMIM 207900 | 21.2 | 26 | 0.61 | -- | 0.61 | Sedentary | Orally |
| 13 | F | 34 | Argininosuccinic aciduria OMIM 207900 | 18.1 | 34.2 | 0.64 | -- | 0.64 | Sedentary | Orally |
| 14 | F | 35 | Arginase deficiency OMIM 207800 | 27.4 | 21.3 | 0.43 | 0.36 | 0.79 | Sedentary | Orally |
| 15 | M | 18 | Argininosuccinic aciduria OMIM 207900 | 24.5 | 22.7 | 0.44 | -- | 0.44 | Sedentary | Orally |
| 16 | M | 28 | Citrullinemia OMIM 215700 | 32.1 | 21.8 | 0.34 | -- | 0.34 | Sedentary | Orally |
| 17 | F | 39 | Isovaleric acidemia OMIM 243500 | 21.4 | 21 | 0.81 | -- | 0.81 | Sedentary | Orally |
| 18 | M | 32 | Ornithine transcarbamylase OMIM 300461 | 20 | 33.7 | 0.62 | 0.16 | 0.79 | Sedentary | Orally |
| Medium values | 28.6 | 24.9 | 23.7 | 0.54 | 0.22 referred to subjects on AA supplementation (33.3%) | 0.61 |
| Parameter | Sample Median Value ± SD | Reference Values |
|---|---|---|
| Albumin | 41.8 ± 3.5 g/L | 35–52 g/L |
| Total protein | 72.7 ± 4.5 g/L | 64–83 g/L |
| Transthyretin | 278 ± 70.2 mg/L | 200–400 mg/L |
| Total cholesterol | 4.5 ± 1.7 mmol/L | 2.00–6.19 mmol/L |
| HDL cholesterol | 1.1 ± 0.3 mmol/L | 0.3–0.8 mmol/L |
| Triglycerides | 1.2 ± 0.6 mmol/L | <1.69 mmol/L |
| Glucose | 4.8 ± 0.6 mmol/L | 3.7–5.6 mmol/L |
| Sample Median Value ± Standard Deviation | Patients on AA Supplementation (39%) | Patients without AA Supplementation (61%) | Reference Values | |
|---|---|---|---|---|
| Leucine | 80.8 ± 33.1 | 76 ± 36.5 | 83.2 ± 36.5 | 78–160 |
| Isoleucine | 66 ± 73.9 | 35.3 ± 15 | 81.3 ± 15 | 34–84 |
| Valine | 145.6 ± 62.8 | 136.8 ± 69.2 | 150 ± 69.2 | 143–352 |
| Lysine | 132.7 ± 68.6 | 156.2 ± 69.1 | 121 ± 69.1 | 111–248 |
| Methionine | 41.7 ±52.2 | 22,7 ± 6,7 | 51.2 ± 6.7 | 14–49 |
| Threonine | 108.6 ± 35.8 | 110.8 ± 32.7 | 107.4 ± 32.7 | 72–168 |
| Phenylalanine | 45.6 ± 9.9 | 41 ± 12.3 | 47.9 ± 12.3 | 39–74 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gugelmo, G.; Lenzini, L.; Francini-Pesenti, F.; Fasan, I.; Spinella, P.; Valentini, R.; Miraval, A.; Avogaro, A.; Vitturi, N. Anthropometrics, Dietary Intake and Body Composition in Urea Cycle Disorders and Branched Chain Organic Acidemias: A Case Study of 18 Adults on Low-Protein Diets. Nutrients 2022, 14, 467. https://doi.org/10.3390/nu14030467
Gugelmo G, Lenzini L, Francini-Pesenti F, Fasan I, Spinella P, Valentini R, Miraval A, Avogaro A, Vitturi N. Anthropometrics, Dietary Intake and Body Composition in Urea Cycle Disorders and Branched Chain Organic Acidemias: A Case Study of 18 Adults on Low-Protein Diets. Nutrients. 2022; 14(3):467. https://doi.org/10.3390/nu14030467
Chicago/Turabian StyleGugelmo, Giorgia, Livia Lenzini, Francesco Francini-Pesenti, Ilaria Fasan, Paolo Spinella, Romina Valentini, Angela Miraval, Angelo Avogaro, and Nicola Vitturi. 2022. "Anthropometrics, Dietary Intake and Body Composition in Urea Cycle Disorders and Branched Chain Organic Acidemias: A Case Study of 18 Adults on Low-Protein Diets" Nutrients 14, no. 3: 467. https://doi.org/10.3390/nu14030467