
Vitamin D Status in Pediatric and Young Adult Cystic Fibrosis Patients. Are the New Recommendations Effective?

 , , , , , ,
, , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
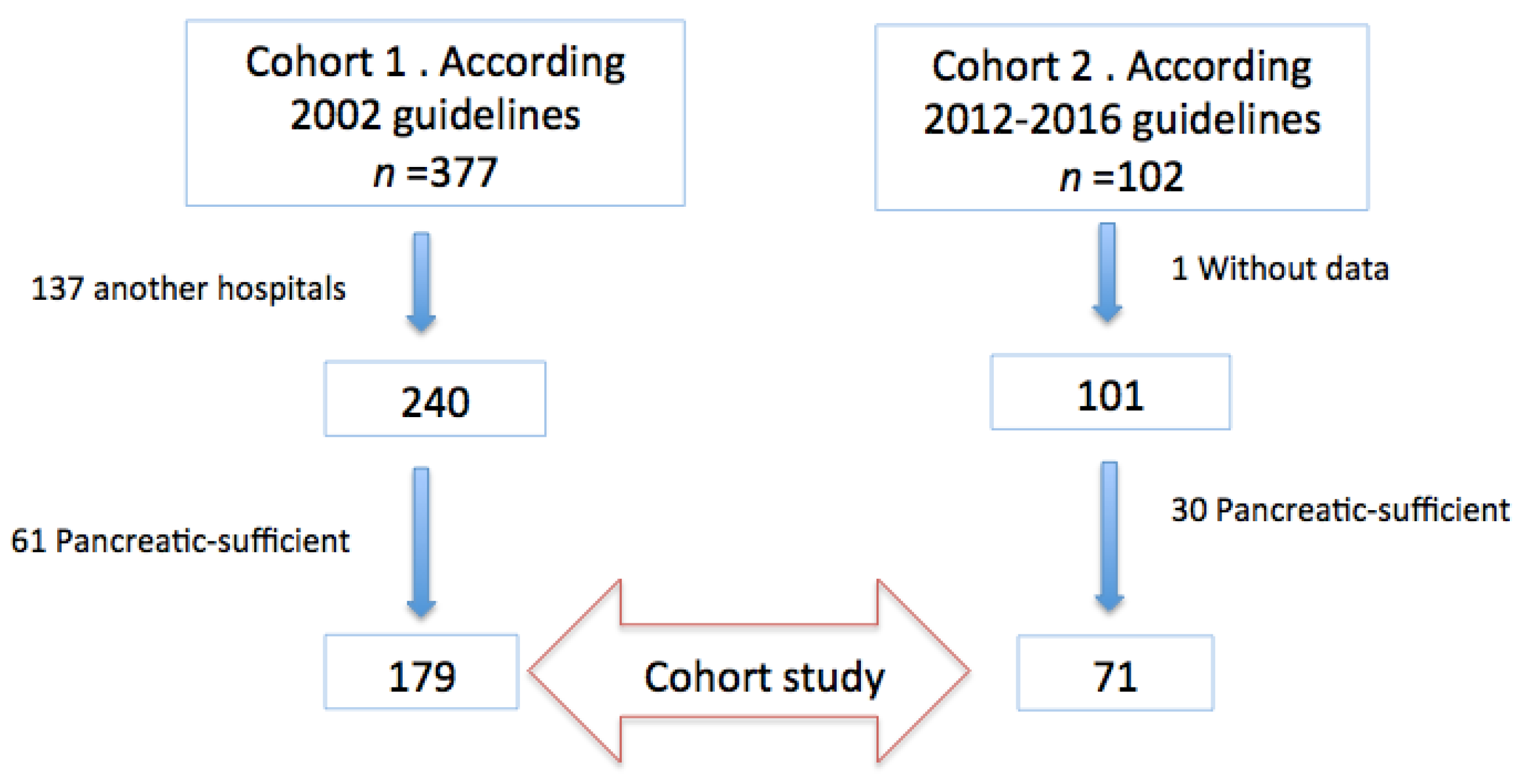
2.1. Study Design
2.2. Patients
2.2.1. Inclusion Criteria
- -
- Patients with a definite CF diagnosis (chloride in sweat >60 mEq/L or positive genetic study) until 40 years old.
- -
- Clinical stability defined by clinical criteria: absence of cough, fever, sputum or hemoptysis in the 2 weeks prior to inclusion in the study.
- -
- Exocrine pancreatic insufficiency: fecal elastase levels <200 mcg/g.
2.2.2. Exclusion Criteria
- -
- Thrombopenia: platelet count <50,000/mm3
- -
- Liver dysfunction: elevated liver enzymes >3-fold the upper limit of normality–ULN-; conjugated bilirubin levels >1 mg/dL or liver failure (prothrombin activity <50% or International Normalized Ratio –INR->1.5).
- -
- Renal failure (glomerular filtration rate <60 mL/min/1.73 m2 or <1 SD of glomerular filtration for age).
- -
- Hospital admission or administration of oral or intravenous antibiotics 2 weeks prior to the beginning of the study.
- -
- Threatening episode of hemoptysis (any volume of expectorated blood capable of endangering the patients’ life) 4 weeks before the beginning of the study.
2.3. Variables
2.4. Data Analysis:
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Rovner, A.J.; Stallings, V.A.; Schall, J.I.; Leonard, M.B.; Zemel, B.S. Vitamin D insufficiency in children, adolescents, and young adults with cystic fibrosis despite routine oral supplementation. Am. J. Clin. Nutr. 2007, 86, 1694–1699. [Google Scholar] [CrossRef]
- Feranchak, A.P.; Sontag, M.K.; Wagener, J.S.; Hammond, K.B.; Accurso, F.J.; Sokol, R.J. Prospective, long-term study of fat-soluble vitamin status in children with cystic fibrosis identified by newborn screen. J. Pediatrics 1999, 135, 10. [Google Scholar] [CrossRef]
- Tangpricha, V.; Kelly, A.; Stephenson, A.; Maguiness, K.; Enders, J.; Robinson, K.A.; Marshall, B.C.; Borowitz, D.; Cystic Fibrosis Foundation Vitamin D Evidence-Based Review Committee. An Update on the Screening, Diagnosis, Management, and Treatment of Vitamin D Deficiency in Individuals with Cystic Fibrosis: Evidence-Based Recommendations from the Cystic Fibrosis Foundation. J. Clin. Endocrinol. Metab. 2012, 97, 1082–1093. [Google Scholar] [CrossRef] [PubMed]
- Turck, D.; Braegger, C.P.; Colombo, C.; Declercq, D.; Morton, A.; Pancheva, R.; Robberecht, E.; Stern, M.; Strandvik, B.; Wolfe, S.; et al. ESPEN-ESPGHAN-ECFS guidelines on nutrition care for infants, children, and adults with cystic fibrosis. Clin. Nutr. 2016, 35, 557–577. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- González Jiménez, D.; Muñoz Codoceo, R.; Garriga García, M.; Molina Arias, M.; Álvarez Beltrán, M.; García Romero, R.; Martínez Costa, C.; Meavilla Olivas, S.M.; Peña Quintana, L.; Gallego Gutiérrez, S.; et al. Vitamin D and chronic lung colonization in pediatric and young adults cystic fibrosis patients. Nutr. Hosp. 2015, 32, 1629–1635. [Google Scholar] [PubMed]
- WHO Child Growth Standards. France: World Health Organization. 2006. Available online: https://www.who.int/childgrowth/standards/en/ (accessed on 2 December 2021).
- Borowitz, D.; Baker, R.D.; Stallings, V. Consensus Report on Nutrition for Pediatric Patients with Cystic Fibrosis. J. Pediatric Gastroenterol. Nutr. 2002, 35, 246–259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sinaasappel, M.; Stern, M.; Littlewood, J.; Wolfe, S.; Steinkamp, G.; Heijerman, H.G.M.; Robberecht, E.; Döring, G. Nutrition in patients with cystic fibrosis: A European Consensus. J. Cyst. Fibros. 2002, 1, 51–75. [Google Scholar] [CrossRef] [Green Version]
- National Center for Environmental Health. Second National Report on Biochemical Indicators of Diet and Nutrition in the U.S. Population. 2012. Available online: https://www.cdc.gov/nutritionreport/pdf/nutrition_book_complete508_final.pdf (accessed on 14 October 2021).
- James, D.R.; Alfaham, M.; Goodchild, M.C. Increased susceptibility to peroxide-induced haemolysis with normal vitamin E concentrations in cystic fibrosis. Clin. Chim. Acta 1991, 204, 279–290. [Google Scholar] [CrossRef]
- Grey, V.; Lands, L.; Pall, H.; Drury, D. Monitoring of 25-OH vitamin D levels in children with cystic fibrosis. J. Pediatr. Gastroenterol. Nutr. 2000, 30, 314–319. [Google Scholar] [CrossRef]
- Aitken, M.L.; Fiel, S.B.; Stern, R.C. Cystic fibrosis: Respiratory manifestations. In Pediatric Respiratory Medicine; Taussig, L.M., Landau, L.I., Eds.; CV Mosby: St Louis, MO, USA, 1999; pp. 1–47. [Google Scholar]
- Stephenson, A.; Brotherwood, M.; Robert, R.; Atenafu, E.; Corey, M.; Tullis, E. Cholecalciferol significantly increases 25-hydroxyvitamin D concentrations in adults with cystic fibrosis. Am. J. Clin. Nutr. 2007, 85, 1307–1311. [Google Scholar] [CrossRef] [Green Version]
- Timmers, N.K.L.M.; Stellato, R.K.; van der Ent, C.K.; Houwen, R.H.J.; Woestenenk, J.W. Vitamin D intake, serum 25-hydroxy vitamin D and pulmonary function in paediatric patients with cystic fibrosis: A longitudinal approach. Br. J. Nutr. 2019, 121, 195–201. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brodlie, M.; Orchard, W.A.; Reeks, G.A.; Pattman, S.; McCabe, H.; O’Brien, C.J.; Thomas, M.F.; Spencer, D.A. Vitamin D in children with cystic fibrosis. Arch. Dis. Child. 2012, 97, 982–984. [Google Scholar] [CrossRef] [PubMed]
- Abu-Fraiha, Y.; Elyashar-Earon, H.; Shoseyov, D.; Cohen-Cymberknoh, M.; Armoni, S.; Kerem, E.; Wilschanski, M. Increasing Vitamin D Serum Levels Is Associated with Reduced Pulmonary Exacerbations in Patients with Cystic Fibrosis. J. Pediatric Gastroenterol. Nutr. 2019, 68, 110–115. [Google Scholar] [CrossRef] [PubMed]
- Lark, R.K.; Lester, G.E.; Ontjes, D.A.; Blackwood, A.D.; Hollis, B.W.; Hensler, M.M.; Aris, R.M. Diminished and erratic absorption of ergocalciferol in adult cystic fibrosis patients. Am. J. Clin. Nutr. 2001, 73, 602–606. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cooke, N.E.; Haddad, J.G. Vitamin D Binding Protein (Gc-Globulin). Endocr. Rev. 1989, 10, 294–307. [Google Scholar] [CrossRef]
- Ginde, A.A.; Mansbach, J.M.; Camargo, C.A. Association Between Serum 25-Hydroxyvitamin D Level and Upper Respiratory Tract Infection in the Third National Health and Nutrition Examination Survey. Arch. Intern. Med. 2009, 169, 384–390. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martínez, I.; García, R.; Calmarza, P.; de Arriba, A.; Martínez-Redondo, D.; Sanz, A. Vitamin D insufficiency in a healthy pediatric population. The importance of early prophylaxis. Nutr. Hosp. 2021, 38, 1155–1161. [Google Scholar] [CrossRef]
- Juhász, M.F.; Varannai, O.; Németh, D.; Szakács, Z.; Kiss, S.; Izsák, V.D.; Martonosi, Á.R.; Hegyi, P.; Párniczky, A. Vitamin D supplementation in patients with cystic fibrosis: A systematic review and meta-analysis. J. Cyst. Fibros. 2020, 16, 36. [Google Scholar] [CrossRef]
- Garavaglia, L.; Duncan, C.; Toucheque, M.; Farley, A.; Moffett, K.S. A quality improvement initiative to improve patient adherence to vitamin supplementation in cystic fibrosis. J. Pediatric Gastroenterol. Nutr. 2017, 64, 292–295. [Google Scholar] [CrossRef] [PubMed]
- Armas, L.A.G.; Hollis, B.W.; Heaney, R.P. Vitamin D2 Is Much Less Effective than Vitamin D3 in Humans. J. Clin. Endocrinol. Metab. 2004, 89, 5387–5391. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holick, M.F. Vitamin D Deficiency. N. Engl. J. Med. 2007, 357, 266–281. [Google Scholar] [CrossRef] [PubMed]
- Galior, K.; Grebe, S.; Singh, R. Development of Vitamin D Toxicity from Overcorrection of Vitamin D Deficiency: A Review of Case Reports. Nutrients 2018, 10, 953. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Planté-Bordeneuve, T.; Berardis, S.; Bastin, P.; Gruson, D.; Henri, L.; Gohy, S. Vitamin D intoxication in patients with cystic fibrosis: Report of a single-center cohort. Sci. Rep. 2021, 11, 7719. [Google Scholar] [CrossRef] [PubMed]
- Liu, P.T. Toll-Like Receptor Triggering of a Vitamin D-Mediated Human Antimicrobial Response. Science 2006, 311, 1770–1773. [Google Scholar] [CrossRef] [PubMed]
- Belderbos, M.E.; Houben, M.L.; Wilbrink, B.; Lentjes, E.; Bloemen, E.M.; Kimpen, J.L.; Rovers, M.; Bont, L. Cord blood vitamin D deficiency is associated with respiratory syncytial virus bronchiolitis. Pediatrics 2011, 127, 1513–1520. [Google Scholar] [CrossRef]
- González Jiménez, D. Vitamina D y colonizaciones pulmonares crónicas en pacientes pediátricos y adultos jóvenes en fibrosis quística. Nutr. Hosp. 2015, 32, 1629–1635. [Google Scholar] [PubMed]
- Simoneau, T.; Bazzaz, O.; Sawicki, G.S.; Gordon, C. Vitamin D Status in Children with Cystic Fibrosis. Associations with Inflammation and Bacterial Colonization. Ann. ATS 2014, 11, 205–210. [Google Scholar] [CrossRef]
- Khazai, N.B.; Judd, S.E.; Jeng, L.; Wolfenden, L.L.; Stecenko, A.; Ziegler, T.R.; Tangpricha, V. Treatment and Prevention of Vitamin D Insufficiency in Cystic Fibrosis Patients: Comparative Efficacy of Ergocalciferol, Cholecalciferol, and UV Light. J. Clin. Endocrinol. Metab. 2009, 94, 2037–2043. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McCauley, L.A.; Thomas, W.; Laguna, T.A.; Regelmann, W.E.; Moran, A.; Polgreen, L.E. Vitamin D Deficiency Is Associated with Pulmonary Exacerbations in Children with Cystic Fibrosis. Ann. ATS 2014, 11, 198–204. [Google Scholar] [CrossRef] [Green Version]
- Thursfield, R.M.; Naderi, K.; Leaver, N.; Rosenthal, M.; Alton, E.W.F.W.; Bush, A.; Davies, J.C. Children with cystic fibrosis demonstrate no respiratory immunological, infective or physiological, consequences of vitamin D deficiency. J. Cyst. Fibros. 2018, 17, 657–665. [Google Scholar] [CrossRef] [PubMed]
- Lehoux Dubois, C.; Labrèche, E.; Boudreau, V.; Colomba, J.; Mailhot, M.; Lavoie, A.; Rabasa-Lhoret, R.; Coriati, A. Extra-skeletal impact of vitamin D supplementation protocol in an adult population with cystic fibrosis. Clin. Nutr. 2019, 38, 1666–1671. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Age | CFF * and ECFS ** Guidelines 2002 (UI/Day) | CFF * Guidelines 2012 (UI/Day) | ECFS ** Guidelines 2016 (UI/Day) |
|---|---|---|---|
| 0–12 months | 400 | 400–500 | 400 |
| 1–10 years | 400–800 | 800–1000 | 800 |
| >10 years | 400–800 | 800–2000 | 800 |
| Variable | Cohort 1 (n = 179) | Cohort 2 (n = 71) | p |
|---|---|---|---|
| Age (year) Mean ± SD (range) | 8.6 ± 5.1 (0.1–17.9) | 8.3 ± 7.0 (0.1–39.3) | 0.703 |
| Age group: % <2 years % 2–10 years % >10 years | 14.0 44.7 41.3 | 19.7 47.9 32.4 | 0.326 |
| Sex (% female) | 45.3 | 36.6 | 0.214 |
| Genetic % Homozygous DF508 * % heterozygous DF508 * % Other | 38.6 44.7 16.8 | 43.7 40.9 15.5 | 0.758 |
| % Neonatal Screening | 27.4 | 54.4 | <0.001 |
| Season % Winter % Autumn % Spring % Summer | 50.3 14.5 35.2 0 | 55.0 16.9 26.8 1.4 | 0.259 |
| Pseudomonas aeruginosa airway colonization (%) | 15.6 | 24.2 | 0.120 |
| FEV **(%) Mean ± SD (range) | 90.1 ± 20.7 (35.6–142.0) | 85.9 ± 20.9 (41.0–139.0) | 0.244 |
| FEV < 80% (%) | 29.7 | 41.9 | 0.141 |
| Variable | Cohort 1 (n = 179) | Cohort 2 (n = 71) | p |
|---|---|---|---|
| Weight (kg) Mean ± SD (range) | 29.25 ± 15.56 (3.1–75) | 26.97±16.81 (3.2–74) | 0.309 |
| Height (cm) Mean ± SD (range) | 125.72 ± 29.5 (50–179.5) | 119.094 ± 31.14 (50–177.7) | 0.116 |
| BMI (z-score) Mean ± SD (range) | −0.29 ± 0.82 (−2.38–2.58) | 0.1 ± 1.02 (−1.9–3.3) | 0.004 |
| Cholesterol (mg/dL) Mean ± SD (range) | 126 ± 27 (50–230) | 125 ± 28 (60–192) | 0.781 |
| % Malnourished % Nutritional risk % Normally nourished % Overweight/obese | 3.3 70.2 22.1 3.9 | 4.3 55.3 31.9 8.5 | 0.741 0.048 0.169 0.203 |
| Variable | Or | 95% CI | p |
|---|---|---|---|
| Cohort 1 | 2.23 | 1.09–4.57 | 0.028 |
| Age (Years) | 0.97 | 0.91–1.03 | 0.330 |
| Neonatal screening | 1.45 | 0.73–2.87 | 0.288 |
| Body mass index (Z-score) | 0.94 | 0.68–1.30 | 0.712 |
| Pseudomonas aeruginosa airway colonization | 1.13 | 0.52–2.44 | 0.757 |
| Season: winter | 0.84 | 0.48–1.47 | 0.539 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mangas-Sánchez, C.; Garriga-García, M.; Serrano-Nieto, M.J.; García-Romero, R.; Álvarez-Beltrán, M.; Crehuá-Gaudiza, E.; Muñoz-Codoceo, R.; Suárez-Cortina, L.; Vicente-Santamaría, S.; Martínez-Costa, C.; et al. Vitamin D Status in Pediatric and Young Adult Cystic Fibrosis Patients. Are the New Recommendations Effective? Nutrients 2021, 13, 4413. https://doi.org/10.3390/nu13124413
Mangas-Sánchez C, Garriga-García M, Serrano-Nieto MJ, García-Romero R, Álvarez-Beltrán M, Crehuá-Gaudiza E, Muñoz-Codoceo R, Suárez-Cortina L, Vicente-Santamaría S, Martínez-Costa C, et al. Vitamin D Status in Pediatric and Young Adult Cystic Fibrosis Patients. Are the New Recommendations Effective? Nutrients. 2021; 13(12):4413. https://doi.org/10.3390/nu13124413
Chicago/Turabian StyleMangas-Sánchez, Carmen, María Garriga-García, María Juliana Serrano-Nieto, Ruth García-Romero, Marina Álvarez-Beltrán, Elena Crehuá-Gaudiza, Rosana Muñoz-Codoceo, Lucrecia Suárez-Cortina, Saioa Vicente-Santamaría, Cecilia Martínez-Costa, and et al. 2021. "Vitamin D Status in Pediatric and Young Adult Cystic Fibrosis Patients. Are the New Recommendations Effective?" Nutrients 13, no. 12: 4413. https://doi.org/10.3390/nu13124413