
Intervention Fidelity Focusing on Interaction between Participants and Facilitators in a Telephone-Delivered Health Coaching Intervention for the Prevention and Management of Type 2 Diabetes

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Intervention
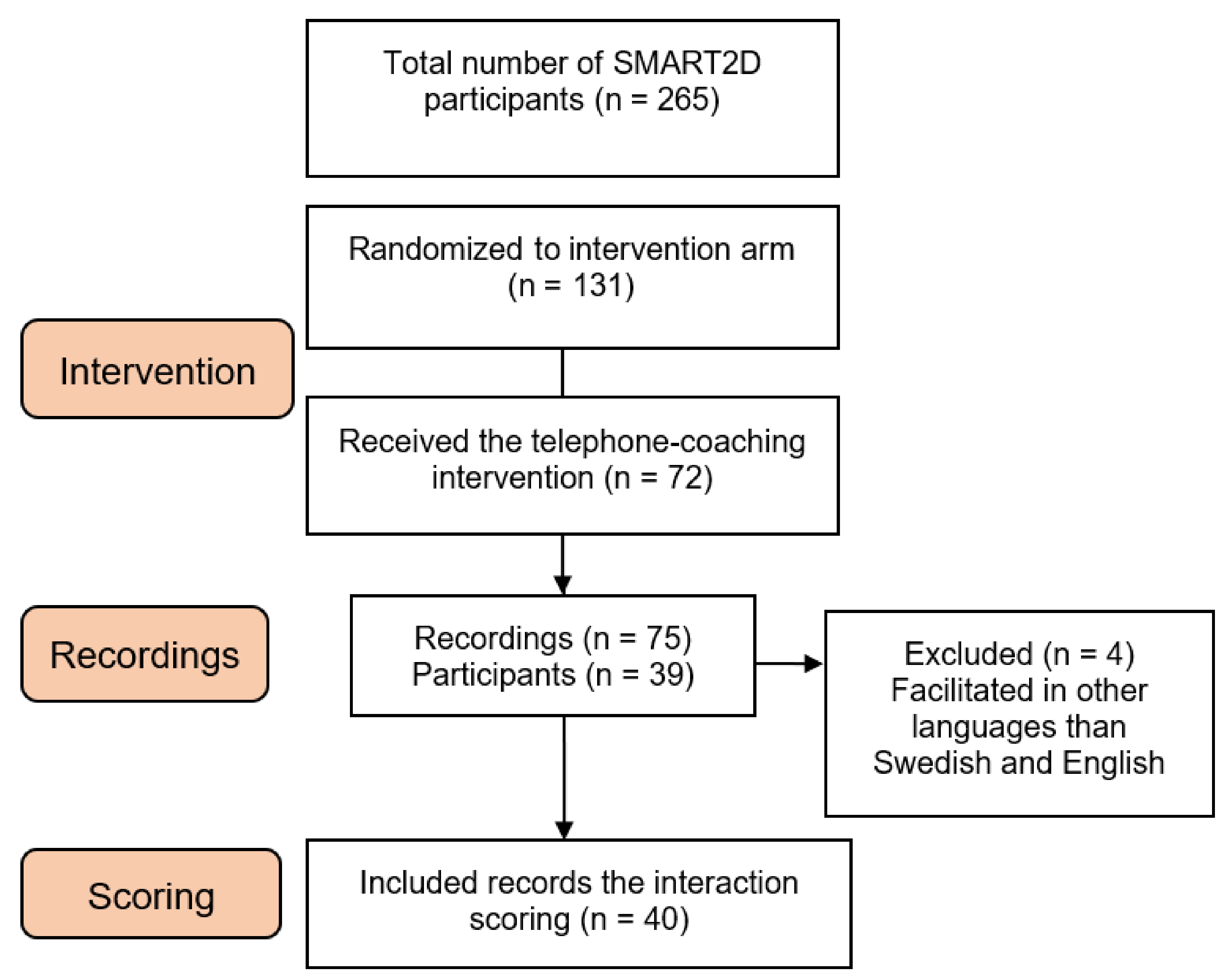
2.2. Study Participants
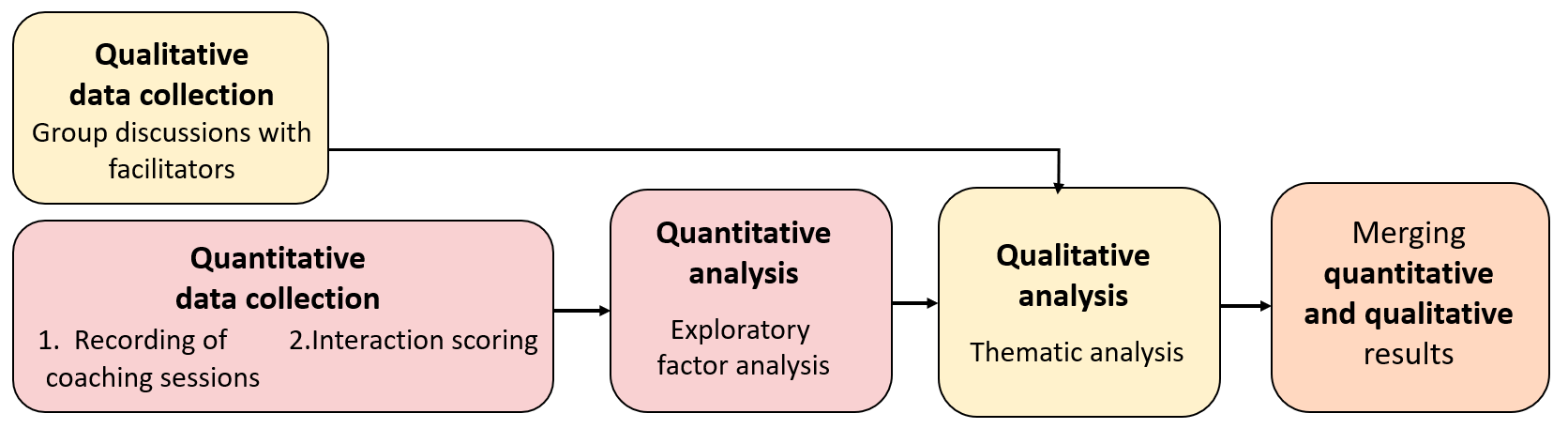
2.3. Study Design
2.3.1. Part 1: Quantitative Data Collection and Analysis
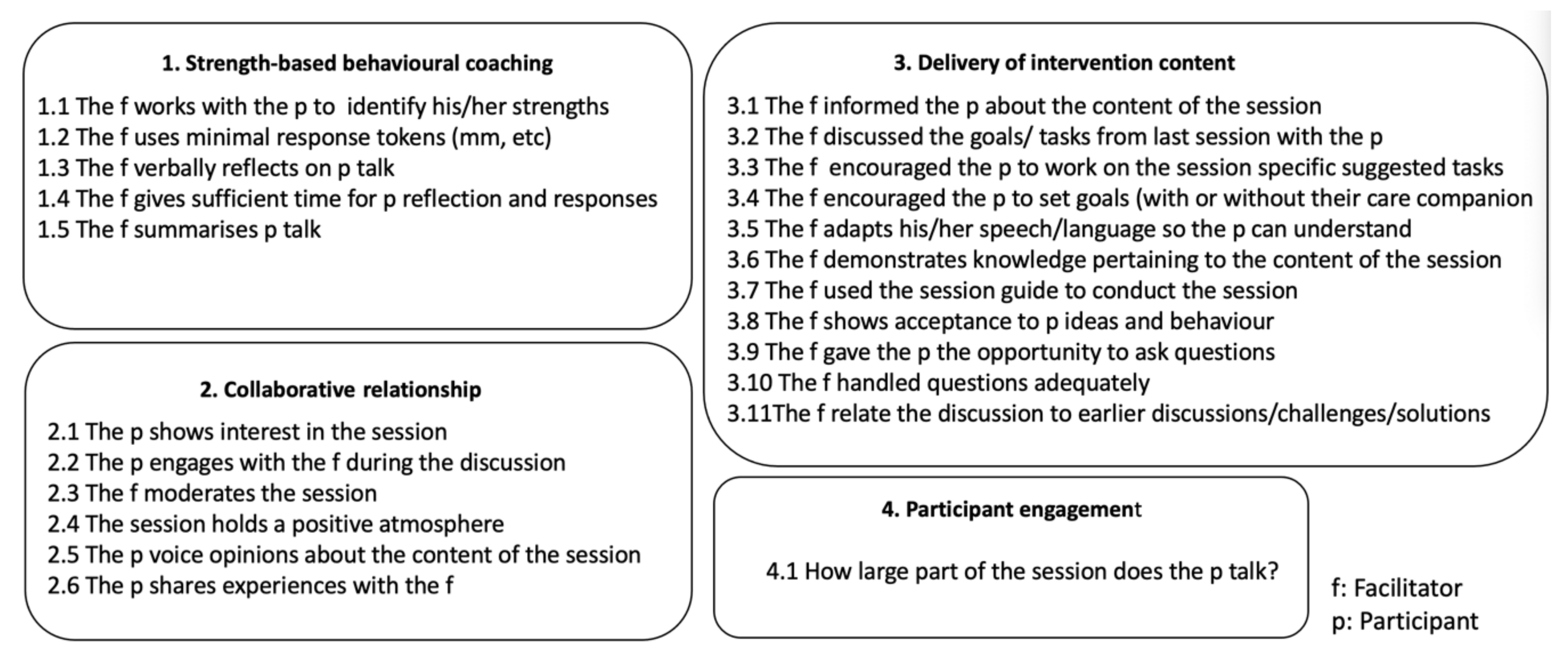
2.3.2. Interaction Scoring Tool
2.3.3. Scoring
2.3.4. Data Analysis
2.3.5. Part 2: Qualitative Data Collection and Analysis
3. Results
3.1. Quantifying the Interaction
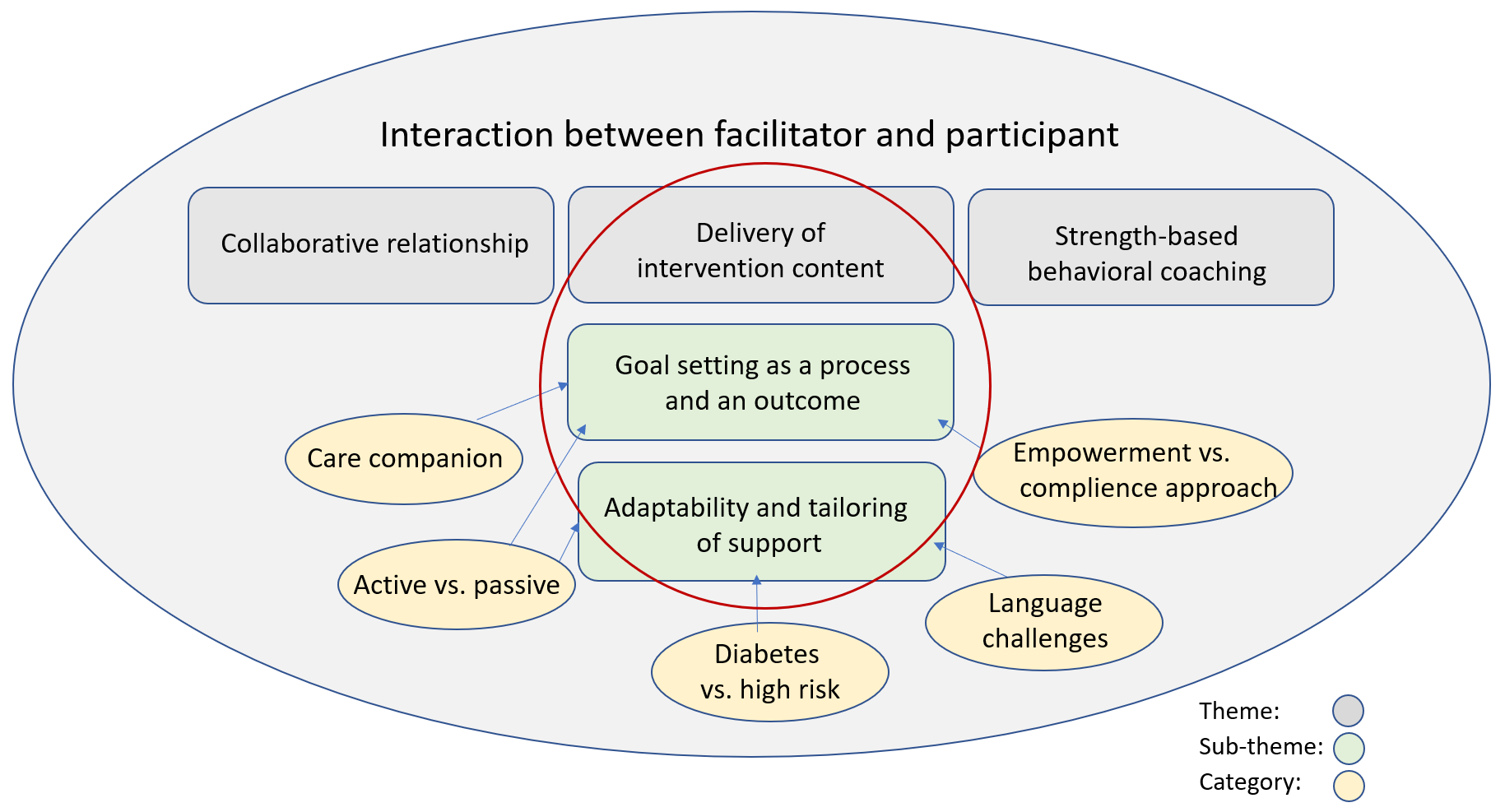
3.2. Qualifying the Interaction
3.2.1. Goal Setting as a Process and an Outcome
F1: No, I think I write down a lot of what they say like: I want to, or I have a problem with this, or I never eat lunch or something. And I put that in and then I can go back and read that. Yes, so in some way they have issues, but it is not goals, really. But yes, I try to go back and discuss what they said to me.
M: So, you don’t mention goals?
F2: I definitely write down the goal, for example this client was walking and I asked: Have you been continuing walking and I mention it every ten days, asking specifically what he is doing.
M: Do you think that is important to be specific?
F4: So, I think it is very good to be specific because they have so many stories as well. At the end of the day, you’ll get a long list, they will have done everything in the manual, but you will not have the specific goals right? So, I think that it is good to put them in, the specific goals.
F2: So, I told them: Hey, so, an example of things that you can do for activities would be that you identify healthy recipes to cook and then he says: “Yes, but my wife is the one who cooks, she is my [participant’s] care companion.” She was there, he talked to her that day. “But yes, that is something we can do, yes, I can see something healthy and then tell her.” It seems like she is around when he is talking to me. And they are very active, so I suggested goals, then he said: “Yes, ok, this is something I can do.” And then I wrote it down as a goal.
F1: Well I have one couple who sit down and go through and are super prepared when I talk to them. But I would say that they are maybe an exception…
F4: Yes, and then there is one who has a friend and a daughter so there are three of them who discuss and do things with them. So, you know these are a few of the success stories that I see. And you can see that …they have specific goals and they decide yes, I will do the steps and I promise, I hope that I can do like five thousand steps every day, that’s my goal, we will see if I can achieve that. So, I’ve seen those.
F3: The best chance of anything happening is that they live together. But it seems much more informal. “Yes, yes we discussed it”, there is no, “we sat down and we talked about our goals”. That just doesn’t happen, even in the ones for me who are working, who are living together.
F4: Like for my participants for example I suggest, so how about, I mean have you thought about doing this, doing that, and they are like yes, I have tried that. One participant said that she has tried standing one leg while brushing her teeth and God, that doesn’t work for her because she doesn’t have balance but she decided to stand while talking on the phone. And then, that is just one aspect on top of the walks that she has decided she is going to make, which is great. So, she decided she could, she tried, yes, she tried. But she decided she will do the standing while talking on the phone and then she will take some walks with her husband every day at least for 30 min, and then she will decide, I mean, they will try to increase the time they do the walking. […] This is the thing when you have a situation for them to reflect and that is the situation I’m talking about. So, when they start reflecting upon it then you know an idea pops up and it becomes a goal.
F3: But I’m thinking in general if we have someone who is already very, very physically active and we pass that message on, but in terms of goals, there is no need for particular goals! If I talk to a person who is walking, I don’t know, 15,000 steps a day and who is very active, and he is playing bandy and he is playing this and he is playing that. I don’t think I need to convince him during that particular session. Then I need to inform him of the content of the session and the message of the session. But to then try to get someone who is already very active to start walking upstairs if he already is… it is not my idea of an achievement.
3.2.2. Adaptability and Tailoring of Support
F1: Yes, and they have a lot of things going on… yesterday I talked to someone about “nyckelhålet” [Swedish healthy food label] and she told me: “Yes, when I got my diagnosis, like when was it was one year ago, I had a dietician talk or help, lecturing me about “nyckelhålet” and stuff like that so I know that already. A lot of my people have this.”
F3: I was concerned that it would not be enough or that it would you know… That was not met. People were very happy, and the conversations can go on for as long as you want. I think that I was not expecting this personal, personal relationship to the development which is also what leads me to think that what are we actually delivering? We are delivering this package, but I think for a lot of people it is more than that. Or even other than that, there is this very strong social support factor that I feel that I’m delivering. Not only for diabetes, but for health. Because one person has called me “her personal health”. And I say: Yes, we are here to facilitate but the main thing is to support you in to working with someone else. But also, the fact that people are very lonely and do have a lot of concerns. This is not just a delivery, this is more.
F2: And obviously the sessions that I do in Spanish feel more comfortable because it feels that it has a better flow. In terms of when they say something for example, sometimes the participants in Swedish just say something and stop and then it’s like they don’t want to continue talking about it, while the participants in Spanish, they just want to go on and on about one specific little thing.
4. Discussion
5. Strengths and Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Puckrein, G.A.; Egan, B.M.; Howard, G. Social and medical determinants of cardiometabolic health: The big picture. Ethn. Dis. 2015, 25, 521. [Google Scholar] [PubMed]
- Osborn, C.Y.; de Groot, M.; Wagner, J.A. Racial and ethnic disparities in diabetes complications in the northeastern United States: The role of socioeconomic status. J. Natl. Med Assoc. 2013, 105, 51–58. [Google Scholar]
- Engelen, L.; Gale, J.; Chau, J.Y.; Hardy, L.L.; Mackey, M.; Johnson, N.; Shirley, D.; Bauman, A. Who is at risk of chronic disease? Associations between risk profiles of physical activity, sitting and cardio-metabolic disease in Australian adults. Aust. N. Z. J. Public Health 2017, 41, 178–183. [Google Scholar] [PubMed]
- Captieux, M.; Pearce, G.; Parke, H.L.; Epiphaniou, E.; Wild, S.; Taylor, S.J.; Pinnock, H. Supported self-management for people with type 2 diabetes: A meta-review of quantitative systematic reviews. Lancet 2017, 390, S32. [Google Scholar]
- World Health Organization. Global Report on Diabetes; World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- Heinrich, E.; Schaper, N.C.; de Vries, N.K. Self-management interventions for type 2 diabetes: A systematic review. Eur. Diabetes Nurs. 2010, 7, 71–76. [Google Scholar]
- Lorig, K.R.; Holman, H.R. Self-management education: History, definition, outcomes, and mechanisms. Ann. Behav. Med. 2003, 26, 1–7. [Google Scholar]
- Alvarsson, M.; Hilding, A.; Östenson, C.G. Factors determining normalization of glucose intolerance in middle-aged Swedish men and women: A 8–10-year follow-up. Diabet. Med. 2009, 26, 345–353. [Google Scholar] [CrossRef]
- Glechner, A.; Keuchel, L.; Affengruber, L.; Titscher, V.; Sommer, I.; Matyas, N.; Wagner, G.; Kien, C.; Klerings, I.; Gartlehner, G. Effects of lifestyle changes on adults with prediabetes: A systematic review and meta-analysis. Prim. Care Diabetes 2018, 12, 393–408. [Google Scholar]
- Gregg, E.W.; Chen, H.; Wagenknecht, L.E.; Clark, J.M.; Delahanty, L.M.; Bantle, J.; Pownall, H.J.; Johnson, K.C.; Safford, M.M.; Kitabchi, A.E.; et al. Association of an intensive lifestyle intervention with remission of type 2 diabetes. JAMA 2012, 308, 2489–2496. [Google Scholar] [CrossRef] [Green Version]
- Mottalib, A.; Sakr, M.; Shehabeldin, M. Diabetes remission after nonsurgical intensive lifestyle intervention in obese patients with type 2 diabetes. J. Diabetes Res. 2015, 2015, 1–4. [Google Scholar]
- Lean, M.E.; Leslie, W.S.; Barnes, A.C.; Brosnahan, N.; Thom, G.; McCombie, L.; Peters, C.; Zhyzhneuskaya, S.; Al-Mrabeh, A.; Hollingsworth, K.G.; et al. Primary care-led weight management for remission of type 2 diabetes (DiRECT): An open-label, cluster-randomised trial. Lancet 2018, 391, 541–551. [Google Scholar] [CrossRef] [Green Version]
- Boelsen-Robinson, T.; Peeters, A.; Beauchamp, A.; Chung, A.; Gearon, E.; Backholer, K. A systematic review of the effectiveness of whole-of-community interventions by socioeconomic position. Obesity Rev. 2015, 16, 806–816. [Google Scholar] [CrossRef] [PubMed]
- Dennis, S.M.; Harris, M.; Lloyd, J.; Davies, G.P.; Faruqi, N.; Zwar, N. Do people with existing chronic conditions benefit from telephone coaching? A rapid review. Aust. Health Rev. 2013, 37, 381–388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lindner, H.; Menzies, D.; Kelly, J.; Taylor, S.; Shearer, M. Coaching for behaviour change in chronic disease: A review of the literature and the implications for coaching as a self-management intervention. Aust. J. Prim. Health 2003, 9, 177–185. [Google Scholar] [CrossRef]
- Rothlind, E.; Fors, U.; Salminen, H.; Wändell, P.; Ekblad, S. Circling the undefined—A grounded theory study of intercultural consultations in Swedish primary care. PLoS ONE 2018, 13, e0203383. [Google Scholar] [CrossRef]
- Kleinman, A. What Really Matters: LIVING a Moral Life Amidst Uncertainty and Danger; Oxford University Press: Oxford, UK, 2007. [Google Scholar]
- Kleinman, A.; Benson, P. Anthropology in the clinic: The problem of cultural competency and how to fix it. PLoS Med. 2006, 3, e294. [Google Scholar] [CrossRef] [Green Version]
- Wong, C.K.; Wong, W.C.; Lam, C.L.; Wan, Y.F.; Wong, W.H.; Chung, K.L.; Dai, D.; Tsui, E.L.; Fong, D.Y. Effects of patient empowerment programme (PEP) on clinical outcomes and health service utilization in type 2 diabetes mellitus in primary care: An observational matched cohort study. PLoS ONE 2014, 9, e95328. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anderson, R.M.; Funnell, M.M. Patient empowerment: Reflections on the challenge of fostering the adoption of a new paradigm. Patient Educ. Couns. 2005, 57, 153–157. [Google Scholar] [CrossRef]
- Anderson, R.M.; Funnell, M.M. Patient empowerment: Myths and misconceptions. Patient Educ. Couns. 2010, 79, 277–282. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Zyl, L.E.; Stander, M.W. A strengths-based approach towards coaching in a multicultural environment. In Interdisciplinary Handbook of the Person-Centered Approach; Springer: Berlin/Heidelberg, Germany, 2013; pp. 245–257. [Google Scholar]
- Rubak, S.; Sandbæk, A.; Lauritzen, T.; Christensen, B. Motivational interviewing: A systematic review and meta-analysis. Br. J. Gen. Pract. 2005, 55, 305–312. [Google Scholar] [PubMed]
- Minary, L.; Alla, F.; Cambon, L.; Kivits, J.; Potvin, L. Addressing complexity in population health intervention research: The context/intervention interface. J. Epidemiol. Community Health 2018, 72, 319–323. [Google Scholar] [CrossRef] [PubMed]
- Bilodeau, A.; Potvin, L. Unpacking complexity in public health interventions with the Actor–Network Theory. Health Promot. Int. 2018, 33, 173–181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farzadnia, S.; Giles, H. Patient-provider interaction: A communication accommodation theory perspective. Int. J. Soc. Cult. Lang. 2015, 3, 17–34. [Google Scholar]
- Barry, E.; Roberts, S.; Oke, J.; Vijayaraghavan, S.; Normansell, R.; Greenhalgh, T. Efficacy and effectiveness of screen and treat policies in prevention of type 2 diabetes: Systematic review and meta-analysis of screening tests and interventions. Br. Med. J. 2017, 356, i6538. [Google Scholar] [CrossRef] [Green Version]
- Bellg, A.J.; Borrelli, B.; Resnick, B.; Hecht, J.; Minicucci, D.S.; Ory, M.; Ogedegbe, G.; Orwig, D.; Ernst, D.; Czajkowski, S. Enhancing treatment fidelity in health behavior change studies: Best practices and recommendations from the NIH Behavior Change Consortium. Health Psychol. 2004, 23, 443. [Google Scholar] [CrossRef] [PubMed]
- Toomey, E.; Hardeman, W.; Hankonen, N.; Byrne, M.; McSharry, J.; Matvienko-Sikar, K.; Lorencatto, F. Focusing on fidelity: Narrative review and recommendations for improving intervention fidelity within trials of health behaviour change interventions. Health Psychol. Behav. Med. 2020, 8, 132–151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miller, W.R.; Rollnick, S. The effectiveness and ineffectiveness of complex behavioral interventions: Impact of treatment fidelity. Contemp. Clin. Trials 2014, 37, 234–241. [Google Scholar] [CrossRef] [PubMed]
- Jelsma, J.G.; Mertens, V.C.; Forsberg, L.; Forsberg, L. How to measure motivational interviewing fidelity in randomized controlled trials: Practical recommendations. Contemp. Clin. Trials 2015, 43, 93–99. [Google Scholar] [CrossRef] [PubMed]
- Karolinska Institutet. SMART2D. 2019. Available online: http://ki.se/en/gph/smart2d (accessed on 15 June 2021).
- Timm, L. Feasibility of Type 2 Diabetes Prevention: Processes for Detection, Self-Management and Support in Socioeconomically Disadvantaged Areas; Karolinska Institutet: Solna, Sweden, 2021. [Google Scholar]
- Timm, L.; Harcke, K.; Karlsson, I.; Sidney Annerstedt, K.; Alvesson, H.M.; Stattin, N.S.; Forsberg, B.C.; Östenson, C.G.; Daivadanam, M. Early detection of type 2 diabetes in socioeconomically disadvantaged areas in Stockholm—Comparing reach of community and facility-based screening. Global Health Action 2020, 13, 1795439. [Google Scholar] [CrossRef]
- Saaristo, T.; Peltonen, M.; Lindström, J.; Saarikoski, L.; Sundvall, J.; Eriksson, J.G.; Tuomilehto, J. Cross-sectional evaluation of the Finnish diabetes risk score: A tool to identify undetected type 2 diabetes, abnormal glucose tolerance and metabolic syndrome. Diabetes Vasc. Dis. Res. 2005, 2, 67–72. [Google Scholar] [CrossRef]
- Guwatudde, D.; Absetz, P.; Delobelle, P.; Östenson, C.G.; Olmen Van, J.; Alvesson, H.M.; Mayega, R.W.; Kiracho, E.E.; Kiguli, J.; Sundberg, C.J.; et al. Study protocol for the SMART2D adaptive implementation trial: A cluster randomised trial comparing facility-only care with integrated facility and community care to improve type 2 diabetes outcomes in Uganda, South Africa and Sweden. BMJ Open 2018, 8, e019981. [Google Scholar] [CrossRef] [PubMed]
- Creswell, J.W.; Klassen, A.C.; Plano Clark, V.L.; Smith, K.C. Best Practices for Mixed Methods Research in the Health Sciences; National Institutes of Health: Bethesda, MD, USA, 2011; Volume 2013, pp. 541–545.
- McHugh, M.L. Interrater reliability: The kappa statistic. Biochem. Med. 2012, 22, 276–282. [Google Scholar] [CrossRef]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hair, J.F.; Black, W.C.; Babin, B.J.; Anderson, R.E.; Tatham, R.L. Multivariate Data Analysis; Pearson Prentice Hall: Hoboken, NJ, USA, 2006. [Google Scholar]
- Fayers, P.M.; Machin, D. Multi-Item Scales, in Quality of Life the Assessment, Analysis and Interpretation of Patient-Reported Outcomes; John Wiley and Sons: Hoboken, NJ, USA, 2007; pp. 123–124. [Google Scholar]
- Fayers, P.M.; Machin, D. Choosing and Scoring Questionnaires, in Quality of Life the Assessment, Analysis and Interpretation of Patient-Reported Outcomes; John Wiley & Sons: Hoboken, NJ, USA, 2007; p. 216. [Google Scholar]
- Green, J.T. Qualitative Methods for Health Research, 3rd ed.; SAGE: London, UK, 2014. [Google Scholar]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Malterud, K.; Siersma, V.D.; Guassora, A.D. Sample size in qualitative interview studies: Guided by information power. Qual. Health Res. 2016, 26, 1753–1760. [Google Scholar] [CrossRef] [PubMed]
- Van Daele, T.; Van Audenhove, C.; Hermans, D.; Van den Bergh, O.; Van den Broucke, S. Empowerment implementation: Enhancing fidelity and adaptation in a psycho-educational intervention. Health Promot. Int. 2014, 29, 212–222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Dam, H.A.; Van Der Horst, F.G.; Knoops, L.; Ryckman, R.M.; Crebolder, H.F.; Van Den Borne, B.H. Social support in diabetes: A systematic review of controlled intervention studies. Patient Educ. Couns. 2005, 59, 1–12. [Google Scholar] [CrossRef]
- Fisher, E.B.; Boothroyd, R.I.; Coufal, M.M.; Baumann, L.C.; Mbanya, J.C.; Rotheram-Borus, M.J.; Sanguanprasit, B.; Tanasugarn, C. Peer support for self-management of diabetes improved outcomes in international settings. Health Aff. 2012, 31, 130–139. [Google Scholar] [CrossRef] [Green Version]
- Dale, J.; Williams, S.; Bowyer, V. What is the effect of peer support on diabetes outcomes in adults? A systematic review. Diabet. Med. 2012, 29, 1361–1377. [Google Scholar] [CrossRef]
- Greenhalgh, T.; Heath, I. Measuring Quality in the Therapeutic Relationship; The Kings Fund: London, UK, 2010. [Google Scholar]
- De Jong Gierveld, J.; Van Tilburg, T.; Dykstra, P. Loneliness and social isolation. In The Cambridge Handbook of Personal Relationships; Vangelisti, A., Perlman, D., Eds.; Cambridge University Press: Cambridge, UK, 2016. [Google Scholar]
- Breitenstein, S.M.; Gross, D.; Garvey, C.A.; Hill, C.; Fogg, L.; Resnick, B. Implementation fidelity in community-based interventions. Res. Nurs. Health 2010, 33, 164–173. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Session | Title | Content |
|---|---|---|
| 1 | Introductory session | Getting to know the program. Why work with a care companion to make lifestyle changes? |
| 2 | Increase physical activity in daily life and reduce sedentary lifestyle | The importance of physical activity and how this can be increased in daily life |
| 3 | Healthy eating: Regular, balanced and healthy | The importance of regular, balanced and healthy meals |
| 4 | Physical activity through the life course | Discussion on how physical activity levels have changed over the years |
| 5 | Fruit and vegetables | The importance of eating fruit and vegetables every day |
| 6 | Increasing your daily physical activity | Discussion on current situation and potential possibilities for improvements |
| 7 | Sugar | How sugar consumption can be decreased in daily life |
| 8 | Finding a physical activity that suits you | Discussion of options/choices to physical activity |
| 9 | Healthy lifestyle—moving forward | How has it been to try to change to a healthier lifestyle and how can this be maintained? |
| Factor 1 | Factor 2 | Factor 3 | ||
|---|---|---|---|---|
| Statement | Collaborative Relationship | Delivery of Intervention Content | Strength-Based Behavioral Coaching | |
| 5.4 | The session holds a positive atmosphere | 0.97 | ||
| 5.2 | The participant engages with the facilitator during the session | 0.89 | ||
| 5.1 | The participant shows interest in the session | 0.83 | ||
| 4.1 | The facilitator works with the participant to identify his/her strengths | 0.58 | ||
| 6.7 | The facilitator used the session guide to conduct the session | 0.83 | ||
| 6.3 | The facilitator encouraged the participant to work on the sessions specific suggested tasks | 0.69 | ||
| 6.4 | The facilitator encouraged the participant to set goals | 0.64 | ||
| 6.1 | The facilitator informed the participant about the content of the session | 0.60 | ||
| 6.6 | The facilitator demonstrated knowledge pertaining to the content of the session | 0.54 | ||
| 6.9 | The facilitator gave the participant the opportunity to ask questions | 0.85 | ||
| 4.4 | The facilitator gave sufficient time for participant reflection and response | 0.74 | ||
| 5.6 | The participant shares experiences with the facilitator | 0.56 | ||
| 4.3 | The facilitator verbally reflects on participant’s talk | 0.49 | ||
| 4.5 | The facilitator summarizes participant’s talk | 0.44 | ||
| Eigenvalue | 5.0 | 1.7 | 1.3 | |
| Variance explained | 57% | 19% | 15% | |
| Cronbach’s alpha | 0.89 | 0.83 | 0.74 |
| Collaborative Relationship | Delivery of Intervention Content | Strength-Based Behavioral Coaching | |
|---|---|---|---|
| Median (IQR) | Median (IQR) | Median (IQR) | |
| Total (n = 40) | 75 (69–81) | 81 (76–94) | 75 (70–78) |
| Comparison between facilitators (F) | 75 (75–81) | 94 (85–100) | 76 (70–80) |
| F1 (n = 10) | |||
| F2 (n = 10) | 75 (59–75) | 75 (73–75) | 70 (65–75) |
| F3 (n = 12) | 78 (72–97) | 81 (79–92) | 75 (71–80) |
| F4 (n= 8) | 78 (70–84) | 81 (78–90) | 73 (70–75) |
| p-value | 0.1465 | 0.0017 * | 0.2079 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Timm, L.; Karlsson, I.; Sidney Annerstedt, K.; Absetz, P.; Forsberg, B.C.; Daivadanam, M.; Mølsted Alvesson, H. Intervention Fidelity Focusing on Interaction between Participants and Facilitators in a Telephone-Delivered Health Coaching Intervention for the Prevention and Management of Type 2 Diabetes. Nutrients 2021, 13, 3862. https://doi.org/10.3390/nu13113862
Timm L, Karlsson I, Sidney Annerstedt K, Absetz P, Forsberg BC, Daivadanam M, Mølsted Alvesson H. Intervention Fidelity Focusing on Interaction between Participants and Facilitators in a Telephone-Delivered Health Coaching Intervention for the Prevention and Management of Type 2 Diabetes. Nutrients. 2021; 13(11):3862. https://doi.org/10.3390/nu13113862
Chicago/Turabian StyleTimm, Linda, Ida Karlsson, Kristi Sidney Annerstedt, Pilvikki Absetz, Birger C. Forsberg, Meena Daivadanam, and Helle Mølsted Alvesson. 2021. "Intervention Fidelity Focusing on Interaction between Participants and Facilitators in a Telephone-Delivered Health Coaching Intervention for the Prevention and Management of Type 2 Diabetes" Nutrients 13, no. 11: 3862. https://doi.org/10.3390/nu13113862