
Dietary Intake, Eating Behavior, Physical Activity, and Quality of Life in Infertile Women with PCOS and Obesity Compared with Non-PCOS Obese Controls

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
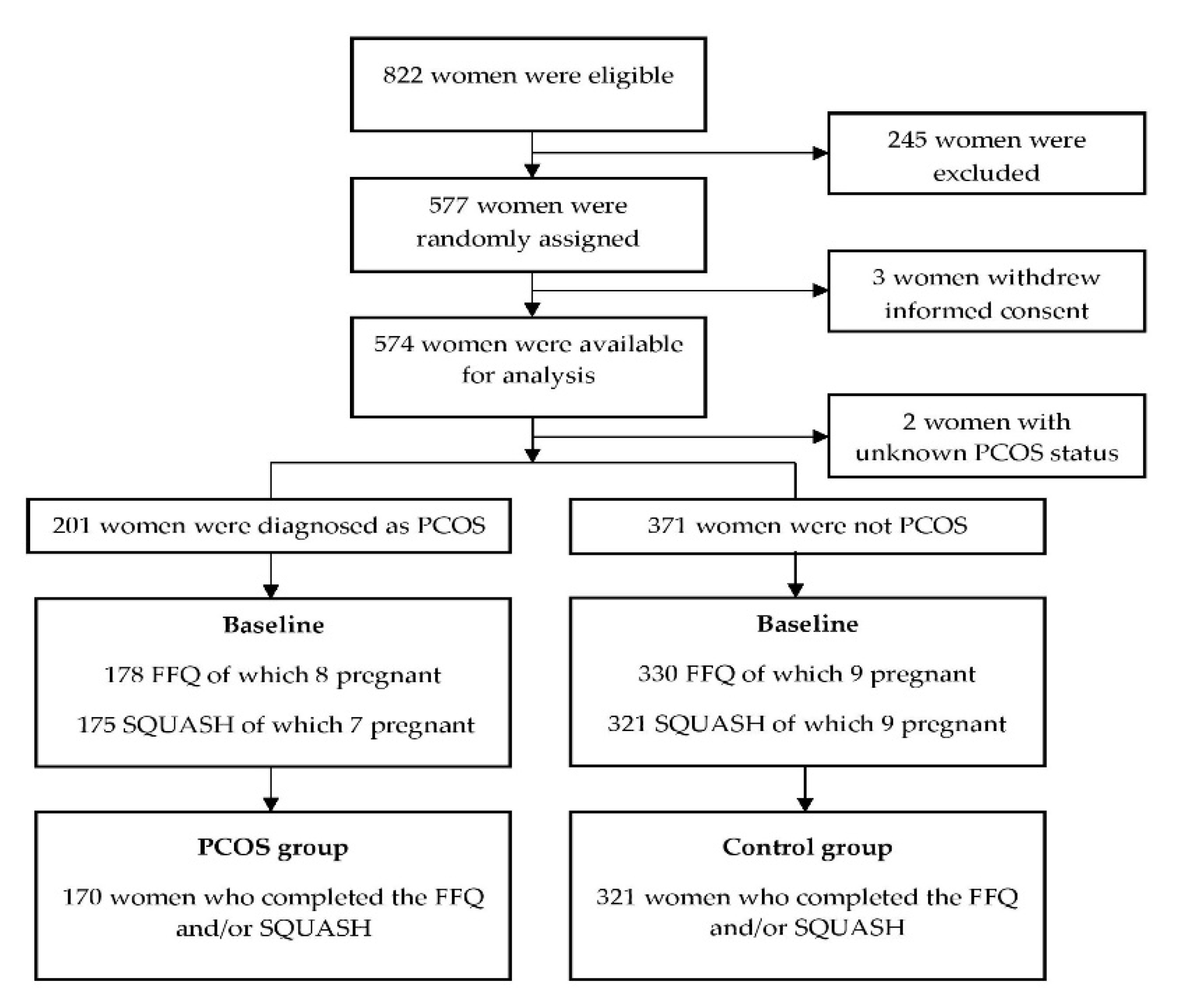
2.1. Study Population
2.2. Clinical and Laboratory Measurements
2.3. Diet, Eating Behavior, Physical Activity, and QoL
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Azziz, R.; Carmina, E.; Chen, Z.; Dunaif, A.; Laven, J.S.; Legro, R.S.; Lizneva, D.; Natterson-Horowtiz, B.; Teede, H.J.; Yildiz, B.O. Polycystic ovary syndrome. Nat. Rev. Dis. Primers 2016, 2, 16057. [Google Scholar] [CrossRef] [PubMed]
- Lim, S.S.; Davies, M.J.; Norman, R.J.; Moran, L.J. Overweight, obesity and central obesity in women with polycystic ovary syndrome: A systematic review and meta-analysis. Hum. Reprod. Update 2012, 18, 618–637. [Google Scholar] [CrossRef] [PubMed]
- Hoeger, K.M.; Oberfield, S.E. Do women with PCOS have a unique predisposition to obesity? Fertil. Steril. 2012, 97, 13–17. [Google Scholar] [CrossRef] [PubMed]
- Robinson, S.; Chan, S.P.; Spacey, S.; Anyaoku, V.; Johnston, D.G.; Franks, S. Postprandial thermogenesis is reduced in polycystic ovary syndrome and is associated with increased insulin resistance. Clin. Endocrinol. 1992, 36, 537–543. [Google Scholar] [CrossRef] [PubMed]
- Hirschberg, A.L.; Naessén, S.; Stridsberg, M.; Byström, B.; Holtet, J. Impaired cholecystokinin secretion and disturbed appetite regulation in women with polycystic ovary syndrome. Gynecol. Endocrinol. Off. J. Int. Soc. Gynecol. Endocrinol. 2004, 19, 79–87. [Google Scholar] [CrossRef]
- Teede, H.J.; Joham, A.E.; Paul, E.; Moran, L.J.; Loxton, D.; Jolley, D.; Lombard, C. Longitudinal weight gain in women identified with polycystic ovary syndrome: Results of an observational study in young women. Obesity 2013, 21, 1526–1532. [Google Scholar] [CrossRef]
- Delitala, A.P.; Capobianco, G.; Delitala, G.; Cherchi, P.L.; Dessole, S. Polycystic ovary syndrome, adipose tissue and metabolic syndrome. Arch. Gynecol. Obstet. 2017, 296, 405–419. [Google Scholar] [CrossRef]
- Dunaif, A. Insulin resistance and the polycystic ovary syndrome: Mechanism and implications for pathogenesis. Endocr. Rev. 1997, 18, 774–800. [Google Scholar] [CrossRef] [Green Version]
- Faghfoori, Z.; Fazelian, S.; Shadnoush, M.; Goodarzi, R. Nutritional management in women with polycystic ovary syndrome: A review study. Diabetes Metab. Syndr. 2017, 11 Suppl 1, S429–S432. [Google Scholar] [CrossRef]
- Douglas, C.C.; Norris, L.E.; Oster, R.A.; Darnell, B.E.; Azziz, R.; Gower, B.A. Difference in dietary intake between women with polycystic ovary syndrome and healthy controls. Fertil. Steril. 2006, 86, 411–417. [Google Scholar] [CrossRef]
- Altieri, P.; Cavazza, C.; Pasqui, F.; Morselli, A.M.; Gambineri, A.; Pasquali, R. Dietary habits and their relationship with hormones and metabolism in overweight and obese women with polycystic ovary syndrome. Clin. Endocrinol. 2013, 78, 52–59. [Google Scholar] [CrossRef]
- Toscani, M.K.; Mario, F.M.; Radavelli-Bagatini, S.; Spritzer, P.M. Insulin resistance is not strictly associated with energy intake or dietary macronutrient composition in women with polycystic ovary syndrome. Nutr. Res. 2011, 31, 97–103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, A.W.; Kazemi, M.; Jarrett, B.Y.; Vanden Brink, H.; Hoeger, K.M.; Spandorfer, S.D.; Lujan, M.E. Dietary and Physical Activity Behaviors in Women with Polycystic Ovary Syndrome per the New International Evidence-Based Guideline. Nutrients 2019, 11, 2711. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moran, L.J.; Ranasinha, S.; Zoungas, S.; McNaughton, S.A.; Brown, W.J.; Teede, H.J. The contribution of diet, physical activity and sedentary behaviour to body mass index in women with and without polycystic ovary syndrome. Hum. Reprod. 2013, 28, 2276–2283. [Google Scholar] [CrossRef] [Green Version]
- van Strien, T. Causes of Emotional Eating and Matched Treatment of Obesity. Curr. Diab. Rep. 2018, 18, 35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burton, P.; Smit, H.J.; Lightowler, H.J. The influence of restrained and external eating patterns on overeating. Appetite 2007, 49, 191–197. [Google Scholar] [CrossRef] [PubMed]
- Teede, H.J.; Misso, M.L.; Costello, M.F.; Dokras, A.; Laven, J.; Moran, L.; Piltonen, T.; Norman, R.J.; International, P.N. Recommendations from the international evidence-based guideline for the assessment and management of polycystic ovary syndrome. Fertil. Steril. 2018, 110, 364–379. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Regidor, P.A.; Schindler, A.E.; Lesoine, B.; Druckman, R. Management of women with PCOS using myo-inositol and folic acid: New clinical data and review of the literature. Horm. Mol. Biol. Clin. Investig. 2018, 34. [Google Scholar] [CrossRef] [PubMed]
- Barrea, L.; Marzullo, P.; Muscogiuri, G.; Di Somma, C.; Scacchi, M.; Orio, F.; Aimaretti, G.; Colao, A.; Savastano, S. Source and amount of carbohydrate in the diet and inflammation in women with polycystic ovary syndrome. Nutr. Res. Rev. 2018, 31, 291–301. [Google Scholar] [CrossRef]
- Gibson-Helm, M.E.; Lucas, I.M.; Boyle, J.A.; Teede, H.J. Women’s experiences of polycystic ovary syndrome diagnosis. Fam. Pract. 2014, 31, 545–549. [Google Scholar] [CrossRef]
- Sharma, A.; Walker, D.M.; Atiomo, W. National survey on management of weight reduction in PCOS women in the United Kingdom. Eur. J. Obstet. Gyn. R. B. 2010, 152, 181–185. [Google Scholar] [CrossRef]
- Mutsaerts, M.A.; van Oers, A.M.; Groen, H.; Burggraaff, J.M.; Kuchenbecker, W.K.; Perquin, D.A.; Koks, C.A.; van Golde, R.; Kaaijk, E.M.; Schierbeek, J.M.; et al. Randomized Trial of a Lifestyle Program in Obese Infertile Women. N. Engl. J. Med. 2016, 374, 1942–1953. [Google Scholar] [CrossRef] [PubMed]
- Mutsaerts, M.A.; Groen, H.; ter Bogt, N.C.; Bolster, J.H.; Land, J.A.; Bemelmans, W.J.; Kuchenbecker, W.K.; Hompes, P.G.; Macklon, N.S.; Stolk, R.P.; et al. The LIFESTYLE study: Costs and effects of a structured lifestyle program in overweight and obese subfertile women to reduce the need for fertility treatment and improve reproductive outcome: A randomised controlled trial. BMC Women’s Health 2010, 10, 22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rotterdam ESHRE/ASRM-Sponsored PCOS Consensus Workshop Group: Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome. Fertil. Steril. 2004, 81, 19–25. [CrossRef] [PubMed]
- van Dammen, L.; Wekker, V.; van Oers, A.M.; Mutsaerts, M.A.Q.; Painter, R.C.; Zwinderman, A.H.; Groen, H.; van de Beek, C.; Muller Kobold, A.C.; Kuchenbecker, W.K.H.; et al. Effect of a lifestyle intervention in obese infertile women on cardiometabolic health and quality of life: A randomized controlled trial. PLoS ONE 2018, 13, e0190662. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van den Brink, C.; Ocké, M.; Houben, A.; van Nierop, P.; Droomers, M. Validation of a Community Health Services Food Consumption Questionnaire in the Netherlands; RIVM National Institute for Public Health and the Environment: Bilthoven, The Netherlands, 2005.
- Wendel-Vos, G.C.; Schuit, A.J.; Saris, W.H.; Kromhout, D. Reproducibility and relative validity of the short questionnaire to assess health-enhancing physical activity. J. Clin. Epidemiol. 2003, 56, 1163–1169. [Google Scholar] [CrossRef] [Green Version]
- van Strien, T.; Frijters, J.E.R.; Bergers, G.P.A.; Defares, P.B. The Dutch Eating Behavior Questionnaire (DEBQ) for assessment of restrained, emotional, and external eating behavior. Int. J. Eat. Disord. 1986, 5, 295–315. [Google Scholar] [CrossRef]
- Aaronson, N.K.; Muller, M.; Cohen, P.D.; Essink-Bot, M.L.; Fekkes, M.; Sanderman, R.; Sprangers, M.A.; te Velde, A.; Verrips, E. Translation, validation, and norming of the Dutch language version of the SF-36 Health Survey in community and chronic disease populations. J. Clin. Epidemiol. 1998, 51, 1055–1068. [Google Scholar] [CrossRef]
- Van Elten, T.M.; Van Poppel, M.N.M.; Gemke, R.; Groen, H.; Hoek, A.; Mol, B.W.; Roseboom, T.J. Cardiometabolic Health in Relation to Lifestyle and Body Weight Changes 3(-)8 Years Earlier. Nutrients 2018, 10, 1953. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Elten, T.M.; Karsten, M.D.A.; Geelen, A.; van Oers, A.M.; van Poppel, M.N.M.; Groen, H.; Gemke, R.; Mol, B.W.; Mutsaerts, M.A.Q.; Roseboom, T.J.; et al. Effects of a preconception lifestyle intervention in obese infertile women on diet and physical activity; A secondary analysis of a randomized controlled trial. PLoS ONE 2018, 13, e0206888. [Google Scholar] [CrossRef] [Green Version]
- Larsson, I.; Hulthen, L.; Landen, M.; Palsson, E.; Janson, P.; Stener-Victorin, E. Dietary intake, resting energy expenditure, and eating behavior in women with and without polycystic ovary syndrome. Clin. Nutr. 2016, 35, 213–218. [Google Scholar] [CrossRef] [PubMed]
- Barnard, L.; Ferriday, D.; Guenther, N.; Strauss, B.; Balen, A.H.; Dye, L. Quality of life and psychological well being in polycystic ovary syndrome. Hum. Reprod. 2007, 22, 2279–2286. [Google Scholar] [CrossRef] [PubMed]
- Elsenbruch, S.; Hahn, S.; Kowalsky, D.; Offner, A.H.; Schedlowski, M.; Mann, K.; Janssen, O.E. Quality of life, psychosocial well-being, and sexual satisfaction in women with polycystic ovary syndrome. J. Clin. Endocrinol. Metab. 2003, 88, 5801–5807. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahnis, A.; Riedl, A.; Figura, A.; Steinhagen-Thiessen, E.; Liebl, M.E.; Klapp, B.F. Psychological and sociodemographic predictors of premature discontinuation of a 1-year multimodal outpatient weight-reduction program: An attrition analysis. Patient Prefer. Adherence 2012, 6, 165–177. [Google Scholar] [CrossRef] [Green Version]
- Teixeira, P.J.; Going, S.B.; Houtkooper, L.B.; Cussler, E.C.; Metcalfe, L.L.; Blew, R.M.; Sardinha, L.B.; Lohman, T.G. Pretreatment predictors of attrition and successful weight management in women. Int. J. Obes. Relat. Metab Disord. 2004, 28, 1124–1133. [Google Scholar] [CrossRef] [Green Version]
- Behboodi Moghadam, Z.; Fereidooni, B.; Saffari, M.; Montazeri, A. Measures of health-related quality of life in PCOS women: A systematic review. Int. J. Women’s Health 2018, 10, 397–408. [Google Scholar] [CrossRef] [Green Version]
- Ching, H.L.; Burke, V.; Stuckey, B.G. Quality of life and psychological morbidity in women with polycystic ovary syndrome: Body mass index, age and the provision of patient information are significant modifiers. Clin. Endocrinol. 2007, 66, 373–379. [Google Scholar] [CrossRef]
- Hebert, J.R.; Clemow, L.; Pbert, L.; Ockene, I.S.; Ockene, J.K. Social desirability bias in dietary self-report may compromise the validity of dietary intake measures. Int. J. Epidemiol. 1995, 24, 389–398. [Google Scholar] [CrossRef]
- Adams, S.A.; Matthews, C.E.; Ebbeling, C.B.; Moore, C.G.; Cunningham, J.E.; Fulton, J.; Hebert, J.R. The effect of social desirability and social approval on self-reports of physical activity. Am. J. Epidemiol. 2005, 161, 389–398. [Google Scholar] [CrossRef]


{kind=link}
| PCOS (n = 170) | non-PCOS (n = 321) | p-Value | |
|---|---|---|---|
| Age (y) | 28.0 ± 4.2 | 30.8 ± 4.4 | <0.001 |
| Western European Ethnicity | 153 (90%) | 287 (89.4%) | 0.84 |
| Education | 0.79 | ||
| Primary school | 6 (3.8%) | 12 (3.9%) | |
| Secondary education | 41 (25.6%) | 71 (26.8%) | |
| Intermediate Vocational Education | 79 (49.4%) | 149 974.8%) | |
| Higher Vocational Education and University | 34 (21.3%) | 78 (25.2%) | |
| Current smoker | 43 (25.6%) | 73 (23.0%) | 0.52 |
| Anthropometrics | |||
| Weight (kg) | 104.0 ± 12.7 | 103.2 ± 13.0 | 0.54 |
| BMI | 36.0 ± 3.5 | 36.0 ± 3.3 | 0.93 |
| Waist circumference (cm) | 108.7 ± 9.1 | 107.6 ± 9.3 | 0.21 |
| Hip circumference (cm) | 124.6 ± 9.0 | 125.4 ± 8.7 | 0.33 |
| Waist-hip circumference ratio | 0.87 ± 0.07 | 0.86 ± 0.06 | 0.02 |
| Blood pressure | |||
| Systolic blood pressure (mmHg) | 126.2 ± 13.6 | 127.7 ± 14.1 | 0.28 |
| Diastolic blood pressure (mmHg) | 80.0 ± 8.9 | 80.2 ± 9.4 | 0.74 |
| Biochemical measures | |||
| hs-CRP (mg/L) | 4.6 (2.2; 8.7) | 4.0 (1.9; 7.0) | 0.06 |
| Triglycerides (mmoL/L) | 1.1 (0.8; 1.6) | 1.1 (0.8; 1.5) | 0.76 |
| Total cholesterol (mmoL/L) | 4.7 ± 0.9 | 4.8 ± 0.9 | 0.62 |
| HDL-C (mmoL/L) | 1.1 ± 0.2 | 1.2 ± 0.3 | 0.30 |
| LDL-C (mmoL/L) | 3.1 ± 0.8 | 3.1 ± 0.9 | 0.81 |
| Fasting glucose (mmoL/L) | 5.4 ± 0.9 | 5.4 ± 0.6 | 0.47 |
| Fasting insulin (pmoL/L) | 116.5 ± 60.5 | 92.4 ± 51.1 | <0.001 |
| HOMA-IR | 4.1 ± 2.7 | 3.2 ± 1.9 | <0.001 |
| Metabolic syndrome | 80 (59.3%) | 148 (54.0%) | 0.32 |
| PCOS (n = 170) | Non-PCOS (n = 321) | Crude B or OR (95% CI) | p-Value | Adjusted * B or OR (95% CI) | Adjusted * p-Value | |
|---|---|---|---|---|---|---|
| Diet | ||||||
| Vegetable intake (g/day) | 107 (78.6; 157) | 129 (85.7; 179) | −17.4 (−31.7 to −3.19) | 0.02 | −8.31 (−25.0 to 8.36) | 0.33 |
| Fruit intake (g/day) | 100 (57.1; 143) | 85.7 (42.9; 142.9) | 8.61 (−6.19 to 23.4) | 0.25 | 15.4 (−1.63 to 32.4) | 0.08 |
| Sugary drinks (glasses/day) | ||||||
| <0.5 | 49 (32.2%) | 114 (40.4%) | ref | ref | ref | Ref |
| 0.5–1 | 25 (16.4%) | 51 (18.1%) | 1.14 (0.64 to 2.05) | 0.66 | 0.95 (0.49 to 1.86) | 0.88 |
| >1 | 78 (51.3%) | 117 (41.5%) | 1.55 (1.00 to 2.41) | 0.05 | 0.72 (0.42 to 1.23) | 0.23 |
| Alcoholic beverages | ||||||
| No | 110 (68.3%) | 182 (61.3%) | ref | ref | ref | ref |
| Yes | 51 (31.7%) | 115 (38.7%) | 0.73 (0.49 to 1.10) | 0.14 | 0.70 (0.43 to 1.13) | 0.15 |
| Savory snacks (handful/week) | ||||||
| <2 | 67 (41.6%) | 121 (40.5%) | ref | ref | ref | ref |
| 2–10 | 53 (32.9%) | 104 (34.8%) | 0.92 (0.59 to 1.44) | 0.72 | 0.91 (0.54 to 1.54) | 0.72 |
| >10 | 41 (25.5%) | 74 (24.7%) | 1.00 (0.62 to 1.62) | 1.00 | 0.88 (0.49 to 1.57) | 0.67 |
| Sweet snacks (portion/week) | ||||||
| <2 | 56 (35.2%) | 103 (34.3%) | ref | ref | ref | ref |
| 2–10 | 77 (48.4%) | 153 (51.0%) | 0.93 (0.61 to 1.42) | 0.72 | 0.94 (0.57 to 1.55) | 0.80 |
| >10 | 26 (16.4%) | 44 (14.7%) | 1.09 (0.61 to 1.95) | 0.78 | 0.95 (0.47 to 1.93) | 0.89 |
| Eating behavior | ||||||
| Emotional eating overall sore | 34.6 ± 11.2 | 34.1 ± 11.3 | 0.49 (−1.64 to 2.61) | 0.65 | 2.03 (−0.45 to 4.51) | 0.11 |
| External eating overall score | 27.7 ± 6.3 | 27.5 ± 5.8 | 0.23 (−0.90 to 1.35) | 0.69 | 0.26 (−1.05 to 1.57) | 0.70 |
| Restricted eating overall score | 32.3 ± 5.9 | 31.7 ± 6.1 | 0.61 (−0.53 to 1.75) | 0.30 | 0.81 (−0.51 to 2.13) | 0.23 |
| Physical activity | ||||||
| Total moderate-to-vigorous physical activity (minute/week) | ||||||
| <200 | 54 (32.1%) | 108 (34.6%) | ref | ref | ref | ref |
| 200–700 | 59 (34.1%) | 98 (31.4%) | 1.20 (0.76 to 1.91) | 0.43 | 1.44 (0.84 to 2.49) | 0.19 |
| >700 | 55 (32.7%) | 106 (34.0%) | 1.04 (0.65 to 1.65) | 0.88 | 0.92 (0.53 to 1.58) | 0.75 |
| Leisure time moderate-to-vigorous physical activity | ||||||
| No | 40 (23.8%) | 61 (19.6%) | ref | ref | ref | ref |
| Yes | 128 (76.2%) | 251 (80.4%) | 0.78 (0.50 to 1.22) | 0.28 | 0.92 (0.53 to 1.60) | 0.77 |
| Commuting moderate-to-vigorous physical activity | ||||||
| No | 105 (62.5%) | 218 (69.9%) | ref | ref | ref | ref |
| Yes | 63 (37.5%) | 94 (30.1%) | 1.39 (0.94 to 2.07) | 0.10 | 1.29 (0.81 to 2.06) | 0.28 |
| Quality of life | ||||||
| Physical Component Score | 49.1 ± 9.5 | 50.2 ± 9.1 | −1.04 (−2.85 to 0.77) | 0.26 | −1.26 (−3.29 to 0.76) | 0.22 |
| Mental Component Score | 50.2 ± 8.5 | 49.4 ± 10.4 | 0.80 (−1.12 to 2.71) | 0.41 | 0.45 (−1.72 to 2.62) | 0.69 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, Z.; Groen, H.; Cantineau, A.E.P.; van Elten, T.M.; Karsten, M.D.A.; van Oers, A.M.; Mol, B.W.J.; Roseboom, T.J.; Hoek, A. Dietary Intake, Eating Behavior, Physical Activity, and Quality of Life in Infertile Women with PCOS and Obesity Compared with Non-PCOS Obese Controls. Nutrients 2021, 13, 3526. https://doi.org/10.3390/nu13103526
Wang Z, Groen H, Cantineau AEP, van Elten TM, Karsten MDA, van Oers AM, Mol BWJ, Roseboom TJ, Hoek A. Dietary Intake, Eating Behavior, Physical Activity, and Quality of Life in Infertile Women with PCOS and Obesity Compared with Non-PCOS Obese Controls. Nutrients. 2021; 13(10):3526. https://doi.org/10.3390/nu13103526
Chicago/Turabian StyleWang, Zheng, Henk Groen, Astrid E. P. Cantineau, Tessa M. van Elten, Matty D. A. Karsten, Anne M. van Oers, Ben W. J. Mol, Tessa J. Roseboom, and Annemieke Hoek. 2021. "Dietary Intake, Eating Behavior, Physical Activity, and Quality of Life in Infertile Women with PCOS and Obesity Compared with Non-PCOS Obese Controls" Nutrients 13, no. 10: 3526. https://doi.org/10.3390/nu13103526