
From Mum to Bum: An Observational Study Protocol to Follow Digestion of Human Milk Oligosaccharides and Glycoproteins from Mother to Preterm Infant

 , , and
, , and
Abstract
:1. Introduction
1.1. The ‘From Mum to Bum’ Study
1.2. Aim and Hypothesis
2. Materials and Methods
2.1. Study Design and Setting
2.2. Sample Size Calculation
2.3. Recruitment Criteria
2.3.1. Inclusion Criteria for Preterm Mother–Infant Pairs
2.3.2. Inclusion Criteria for Full-Term Mother–Infant Pairs
2.3.3. Exclusion Criteria for (Pre)term Mother–Infant Pairs
2.4. Sampling Procedures
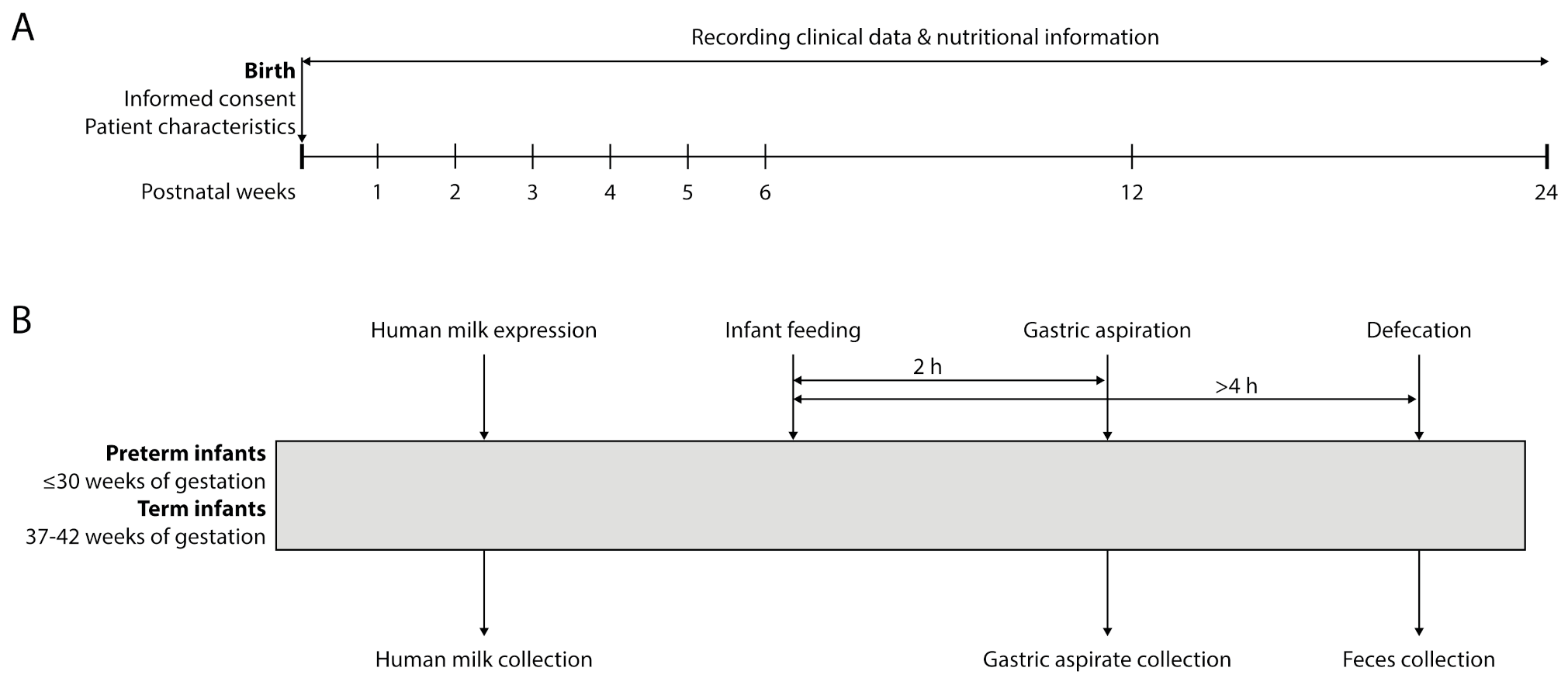
2.4.1. Data Collection Timeline
2.4.2. Human Milk
2.4.3. Gastric Aspirate
2.4.4. Feces
2.4.5. Clinical Data Collection
2.5. Primary Outcome
2.6. Secondary Outcomes
- Microbiota composition in early life and its development over time, assessed using 16S rRNA gene amplicon sequencing and quantitative PCR (qPCR).
- The effect of (corrected) human milk intake on the relative abundance of Bifidobacterium spp.
- The relationship between preterm microbiota composition and weight gain in early life assessed by means of anthropometrics (weight, length and head circumference) and 16S rRNA gene amplicon sequencing.
- The relationship between preterm microbiota composition and registered clinical variables.
2.7. Sample and Data Processing
2.7.1. Total Carbohydrates and Human Milk Oligosaccharides
2.7.2. Metaproteomic and Peptidomic Analysis
2.7.3. Microbiota Analysis
2.7.4. Calorimetry
2.8. Data Availability
2.9. Ethics Approval and Consent to Participate
2.10. Data Management
3. Results
3.1. Data Analysis and Assessments
3.1.1. Carbohydrates and Oligosaccharides
3.1.2. Microbiota Data
3.1.3. Metaproteomics and Peptidomics
3.1.4. Calorimetry
3.1.5. Relationships between Data
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Agostoni, C.; Braegger, C.; Decsi, T.; Kolacek, S.; Koletzko, B.; Michaelsen, K.F.; Mihatsch, W.; Moreno, L.A.; Puntis, J.; Shamir, R.; et al. Breast-feeding: A commentary by the ESPGHAN Committee on Nutrition. J. Pediatr. Gastroenterol. Nutr. 2009, 49, 112–125. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gartner, L.M.; Morton, J.; Lawrence, R.A.; Naylor, A.J.; O’Hare, D.; Schanler, R.J.; Eidelman, A.I. Breastfeeding and the use of human milk. Pediatrics 2005, 115, 496–506. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nanda, R.; Das, P.; Tripathy, P.K. Breast milk: Immunosurveillance in infancy. Asian Pac. J. Trop. Dis. 2014, 4, S505–S512. [Google Scholar] [CrossRef]
- Rodríguez, J.M.; Murphy, K.; Stanton, C.; Ross, R.P.; Kober, O.I.; Juge, N.; Avershina, E.; Rudi, K.; Narbad, A.; Jenmalm, M.C.; et al. The composition of the gut microbiota throughout life, with an emphasis on early life. Microb. Ecol. Health Dis. 2015, 26, 26050. [Google Scholar] [CrossRef]
- Gregory, K.E.; Samuel, B.S.; Houghteling, P.; Shan, G.; Ausubel, F.M.; Sadreyev, R.I.; Walker, W.A. Influence of maternal breast milk ingestion on acquisition of the intestinal microbiome in preterm infants. Microbiome 2016, 4, 68. [Google Scholar] [CrossRef] [Green Version]
- Pacheco, A.R.; Barile, D.; Underwood, M.A.; Mills, D.A. The Impact of the Milk Glycobiome on the Neonate Gut Microbiota. Annu. Rev. Anim. Biosci. 2015, 3, 419–445. [Google Scholar] [CrossRef] [Green Version]
- Holton, T.A.; Vijayakumar, V.; Dallas, D.C.; Guerrero, A.; Borghese, R.A.; Lebrilla, C.B.; German, J.B.; Barile, D.; Underwood, M.A.; Shields, D.C. Following the digestion of milk proteins from mother to baby. J. Proteome Res. 2014, 13, 5777–5783. [Google Scholar] [CrossRef] [Green Version]
- Neu, J. Gastrointestinal maturation and implications for infant feeding. Early Hum. Dev. 2007, 83, 767–775. [Google Scholar] [CrossRef]
- Dallas, D.C.; Sela, D.; Underwood, M.A.; German, J.B.; Lebrilla, C. Protein-Linked Glycan Degradation in Infants Fed Human Milk. Glycobiology [Special Issue]. J. Glycom. Lipidom. 2012, 2. [Google Scholar] [CrossRef] [Green Version]
- Krajmalnik-Brown, R.; Ilhan, Z.-E.; Kang, D.-W.; DiBaise, J.K. Effects of Gut Microbes on Nutrient Absorption and Energy Regulation. Nutr. Clin. Pract. 2012, 27, 201–214. [Google Scholar] [CrossRef] [Green Version]
- Commare, C.E.; Tappenden, K.A. Development of the Infant Intestine: Implications for Nutrition Support. Nutr. Clin. Pract. 2007, 22, 159–173. [Google Scholar] [CrossRef]
- Bode, L. Human milk oligosaccharides: Every baby needs a sugar mama. Glycobiology 2012, 22, 1147–1162. [Google Scholar] [CrossRef] [Green Version]
- Henderickx, J.G.E.; Zwittink, R.D.; van Lingen, R.A.; Knol, J.; Belzer, C. The Preterm Gut Microbiota: An Inconspicuous Challenge in Nutritional Neonatal Care. Front. Cell. Infect. Microbiol. 2019, 9, 85. [Google Scholar] [CrossRef]
- Henderickx, J.G.; Zwittink, R.D.; Renes, I.B.; van Lingen, R.A.; van Zoeren-Grobben, D.; Jebbink, L.J.G.; Boeren, S.; van Elburg, R.M.; Knol, J.; Belzer, C. Maturation of the preterm gastrointestinal tract can be defined by host and microbial markers for digestion and barrier defense. Sci. Rep. 2021, 11, 1–12. [Google Scholar] [CrossRef]
- Jacquot, A.; Neveu, D.; Aujoulat, F.; Mercier, G.; Marchandin, H.; Jumas-Bilak, E.; Picaud, J.C. Dynamics and clinical evolution of bacterial gut microflora in extremely premature patients. J. Pediatr. 2011, 158, 390–396. [Google Scholar] [CrossRef]
- Rougé, C.; Goldenberg, O.; Ferraris, L.; Berger, B.; Rochat, F.; Legrand, A.; Göbel, U.B.; Vodovar, M.; Voyer, M.; Rozé, J.-C.; et al. Investigation of the intestinal microbiota in preterm infants using different methods. Anaerobe 2010, 16, 362–370. [Google Scholar] [CrossRef]
- Costello, E.K.; Carlisle, E.M.; Bik, E.M.; Morowitz, M.J.; Relman, D.A. Microbiome assembly across multiple body sites in low-birthweight infants. MBio 2013, 4, e00782-13. [Google Scholar] [CrossRef]
- Turnbaugh, P.J.; Ley, R.E.; Mahowald, M.A.; Magrini, V.; Mardis, E.R.; Gordon, J.I. An obesity-associated gut microbiome with increased capacity for energy harvest. Nature 2006, 444, 1027–1031. [Google Scholar] [CrossRef]
- Jumpertz, R.; Le, D.S.; Turnbaugh, P.J.; Trinidad, C.; Bogardus, C.; Gordon, J.I.; Krakoff, J. Energy-balance studies reveal associations between gut microbes, caloric load, and nutrient absorption in humans. Am. J. Clin. Nutr. 2011, 94, 58–65. [Google Scholar] [CrossRef] [Green Version]
- Grier, A.; Qiu, X.; Bandyopadhyay, S.; Holden-Wiltse, J.; Kessler, H.A.; Gill, A.L.; Hamilton, B.; Huyck, H.; Misra, S.; Mariani, T.J.; et al. Impact of prematurity and nutrition on the developing gut microbiome and preterm infant growth. Microbiome 2017, 5, 158. [Google Scholar] [CrossRef]
- Zwittink, R.D.; van Zoeren-Grobben, D.; Martin, R.; van Lingen, R.A.; Groot Jebbink, L.J.; Boeren, S.; Renes, I.B.; van Elburg, R.M.; Belzer, C.; Knol, J. Metaproteomics reveals functional differences in intestinal microbiota development of preterm infants. Mol. Cell. Proteom. 2017, 16, 1610–1620. [Google Scholar] [CrossRef] [Green Version]
- Young, J.C.; Pan, C.; Adams, R.M.; Brooks, B.; Banfield, J.F.; Morowitz, M.J.; Hettich, R.L. Metaproteomics reveals functional shifts in microbial and human proteins during a preterm infant gut colonization case. Proteomics 2015, 15, 3463–3473. [Google Scholar] [CrossRef] [Green Version]
- Arboleya, S.; Martinez-Camblor, P.; Solís, G.; Suárez, M.; Fernández, N.; de Los Reyes-Gavilán, C.G.; Gueimonde, M. Intestinal Microbiota and Weight-Gain in Preterm Neonates. Front. Microbiol. 2017, 8, 183. [Google Scholar] [CrossRef]
- Hug, L.; Alexander, M.; You, D.; Alkema, L.; UN Inter-Agency Group for Child Mortality Estimation. National, regional, and global levels and trends in neonatal mortality between 1990 and 2017, with scenario-based projections to 2030: A systematic analysis. Lancet Glob. Health. 2019, 7, e710–e720. [Google Scholar] [CrossRef] [Green Version]
- Örs, R. The practical aspects of enteral nutrition in preterm infants. J. Pediatr. Neonatal Individ. Med. 2013, 2, 35–40. [Google Scholar] [CrossRef]
- Brennan, A.-M.; Murphy, B.P.; Kiely, M.E. Optimising preterm nutrition: Present and future. Proc. Nutr. Soc. 2016, 75, 154–161. [Google Scholar] [CrossRef] [Green Version]
- Stoll, B.J.; Hansen, N.I.; Adams-Chapman, I.; Fanaroff, A.A.; Hintz, S.R.; Vohr, B.; Higgins, R.D.; National Institute of Child Health and Human Development Neonatal Research Network. Neurodevelopmental and growth impairment among extremely low-birth-weight infants with neonatal infection. JAMA 2004, 292, 2357. [Google Scholar] [CrossRef] [Green Version]
- Sammallahti, S.; Kajantie, E.; Matinolli, H.-M.; Pyhälä, R.; Lahti, J.; Heinonen, K.; Lahti, M.; Pesonen, A.-K.; Eriksson, J.G.; Hovi, P.; et al. Nutrition after preterm birth and adult neurocognitive outcomes. PLoS ONE 2017, 12, e0185632. [Google Scholar] [CrossRef] [Green Version]
- Zwittink, R.D.; Van Zoeren-Grobben, D.; Renes, I.B.; Van Lingen, R.A.; Norbruis, O.F.; Martin, R.; Groot Jebbink, L.J.; Knol, J.; Belzer, C. Dynamics of the bacterial gut microbiota in preterm and term infants after intravenous amoxicillin/ceftazidime treatment. BMC Pediatr. 2020, 20, 195. [Google Scholar] [CrossRef]
- Zwittink, R.D.; Renes, I.B.; van Lingen, R.A.; van Zoeren-Grobben, D.; Konstanti, P.; Norbruis, O.F.; Martin, R.; Jebbink, L.J.G.; Knol, J.; Belzer, C. Association between duration of intravenous antibiotic administration and early-life microbiota development in late-preterm infants. Eur. J. Clin. Microbiol. Infect. Dis. 2018, 37, 475–483. [Google Scholar] [CrossRef] [Green Version]
- Borewicz, K.; Gu, F.; Saccenti, E.; Arts, I.C.W.; Penders, J.; Thijs, C.; van Leeuwen, S.S.; Lindner, C.; Nauta, A.; van Leusen, E.; et al. Correlating Infant Fecal Microbiota Composition and Human Milk Oligosaccharide Consumption by Microbiota of 1-Month-Old Breastfed Infants. Mol. Nutr. Food Res. 2019, 63, 1801214. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.; Li, M.; Wu, S.; Lebrilla, C.B.; Chapkin, R.S.; Ivanov, I.; Donovan, S.M. Fecal Microbiota Composition of Breast-fed Infants is Correlated with Human Milk Oligosaccharides Consumed. J. Pediatr. Gastroenterol. Nutr. 2015, 60, 825. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Z.; Neupane, A.; Vo, R.; White, J.; Wang, X.; Marzano, S.-Y.L. Comparing Gut Microbiome in Mothers’ Own Breast Milk- and Formula-Fed Moderate-Late Preterm Infants. Front. Microbiol. 2020, 11, 891. [Google Scholar] [CrossRef] [PubMed]
- Garrido, D.; Dallas, D.C.; Mills, D.A. Consumption of human milk glycoconjugates by infant-associated bifidobacteria: Mechanisms and implications. Microbiology 2013, 159, 649–664. [Google Scholar] [CrossRef]
- Chia, L.W.; Mank, M.; Blijenberg, B.; Bongers, R.S.; van Limpt, K.; Wopereis, H.; Tims, S.; Stahl, B.; Belzer, C.; Knol, J. Cross-feeding between Bifidobacterium infantis and Anaerostipes caccae on lactose and human milk oligosaccharides. Benef. Microbes 2020, 12, 69–83. [Google Scholar] [CrossRef]
- Mank, M.; Hauner, H.; Heck, A.J.R.; Stahl, B. Targeted LC-ESI-MS2 characterization of human milk oligosaccharide diversity at 6 to 16 weeks post-partum reveals clear staging effects and distinctive milk groups. Anal. Bioanal. Chem. 2020, 412, 6887–6907. [Google Scholar] [CrossRef]
- Dallas, D.C.; Guerrero, A.; Khaldi, N.; Borghese, R.; Bhandari, A.; Underwood, M.A.; Lebrilla, C.B.; German, J.B.; Barile, D. A peptidomic analysis of human milk digestion in the infant stomach reveals protein-specific degradation patterns. J. Nutr. 2014, 144, 815–820. [Google Scholar] [CrossRef] [Green Version]
- Cox, J.; Mann, M. MaxQuant enables high peptide identification rates, individualized p.p.b.-range mass accuracies and proteome-wide protein quantification. Nat Biotechnol. 2008, 26, 1367–1372. [Google Scholar] [CrossRef]
- Parada, A.E.; Needham, D.M.; Fuhrman, J.A. Every base matters: Assessing small subunit rRNA primers for marine microbiomes with mock communities, time series and global field samples. Environ. Microbiol. 2016, 18, 1403–1414. [Google Scholar] [CrossRef]
- Apprill, A.; McNally, S.; Parsons, R.; Weber, L. Minor revision to V4 region SSU rRNA 806R gene primer greatly increases detection of SAR11 bacterioplankton. Aquat. Microb. Ecol. 2015, 75, 129–137. [Google Scholar] [CrossRef] [Green Version]
- Thompson-Chagoyán, O.C.; Maldonado, J.; Gil, A. Colonization and Impact of Disease and Other Factors on Intestinal Microbiota. Dig. Dis. Sci. 2007, 52, 2069–2077. [Google Scholar] [CrossRef]
- Song, Y.; Liu, C.; Finegold, S.M. Real-time PCR quantitation of clostridia in feces of autistic children. Appl. Environ. Microbiol. 2004, 70, 6459–6465. [Google Scholar] [CrossRef] [Green Version]
- Guo, P.; Zhang, K.; Ma, X.; He, P. Clostridium species as probiotics: Potentials and challenges. J. Anim. Sci. Biotechnol. 2020, 11, 24. [Google Scholar] [CrossRef]
- Suzuki, M.T.; Taylor, L.T.; DeLong, E.F. Quantitative analysis of small-subunit rRNA genes in mixed microbial populations via 5′-nuclease assays. Appl. Environ. Microbiol. 2000, 66, 4605–4614. [Google Scholar] [CrossRef] [Green Version]
- Jian, C.; Luukkonen, P.; Yki-Järvinen, H.; Salonen, A.; Korpela, K. Quantitative PCR provides a simple and accessible method for quantitative microbiota profiling. PLoS ONE 2020, 15, e0227285. [Google Scholar] [CrossRef] [Green Version]
- Matsuda, K.; Tsuji, H.; Asahara, T.; Kado, Y.; Nomoto, K. Sensitive quantitative detection of commensal bacteria by rRNA-targeted reverse transcription-PCR. Appl. Environ. Microbiol. 2007, 73, 32–39. [Google Scholar] [CrossRef] [Green Version]
- Matsuda, K.; Tsuji, H.; Asahara, T.; Matsumoto, K.; Takada, T.; Nomoto, K. Establishment of an Analytical System for the Human Fecal Microbiota, Based on Reverse Transcription-Quantitative PCR Targeting of Multicopy rRNA Molecules. Appl. Environ. Microbiol. 2009, 75, 1961–1969. [Google Scholar] [CrossRef] [Green Version]
- Haarman, M.; Knol, J. Quantitative real-time PCR analysis of fecal Lactobacillus species in infants receiving a prebiotic infant formula. Appl. Environ. Microbiol. 2006, 72, 2359–2365. [Google Scholar] [CrossRef] [Green Version]
- Wierdsma, N.J.; Peters, J.H.C.; van Bokhorst-de van der Schueren, M.A.E.; Mulder, C.J.J.; Metgod, I.; van Bodegraven, A.A. Bomb calorimetry, the gold standard for assessment of intestinal absorption capacity: Normative values in healthy ambulant adults. J. Hum. Nutr. Diet. 2014, 27, 57–64. [Google Scholar] [CrossRef]
- Lubetzky, R.; Vaisman, N.; Mimouni, F.B.; Dollberg, S. Energy expenditure in human milk- versus formula-fed preterm infants. J. Pediatr. 2003, 143, 750–753. [Google Scholar] [CrossRef]
- Hosoi, S.; Honma, K.; Daimatsu, T.; Kiyokawa, M.; Aikawa, T.; Watanabe, S. Lower energy content of human milk than calculated using conversion factors. Pediatr. Int. 2005, 47, 7–9. [Google Scholar] [CrossRef]
- De Curtis, M.; Senterre, J.; Rigo, J. Estimated and measured energy content of infant formulas. J. Pediatr. Gastroenterol. Nutr. 1986, 5, 746–749. [Google Scholar] [CrossRef]
- Lemons, J.A.; Moorehead, H.; Jansen, R.D.; Schreiner, R.L. The energy content of infant formulas. Early Hum. Dev. 1982, 6, 305–308. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2019. [Google Scholar]
- Tyanova, S.; Temu, T.; Sinitcyn, P.; Carlson, A.; Hein, M.Y.; Geiger, T.; Mann, M.; Cox, J. The Perseus computational platform for comprehensive analysis of (prote)omics data. Nat. Methods. 2016, 13, 731–740. [Google Scholar] [CrossRef]
- Davis, J.C.C.; Totten, S.M.; Huang, J.O.; Nagshbandi, S.; Kirmiz, N.; Garrido, D.A.; Lewis, Z.T.; Wu, L.D.; Smilowitz, J.T.; German, J.B.; et al. Identification of Oligosaccharides in Feces of Breast-fed Infants and Their Correlation with the Gut Microbial Community. Mol. Cell. Proteom. 2016, 15, 2987–3002. [Google Scholar] [CrossRef] [Green Version]
- Coppa, G.V.; Pierani, P.; Zampini, L.; Bruni, S.; Carloni, I.; Gabrielli, O. Characterization of oligosaccharides in milk and feces of breast-fed infants by high-performance anion-exchange chromatography. In Bioactive Components of Human Milk. Advances in Experimental Medicine and Biology; Newburg, D.S., Ed.; Springer: Boston, MA, USA, 2001; Volume 501, pp. 307–314. ISBN 978-1-4615-1371-1. [Google Scholar]
- Chaturvedi, P.; Warren, C.D.; Buescher, C.R.; Pickering, L.K.; Newburg, D.S. Survival of human milk oligosaccharides in the intestine of infants. Adv. Exp. Med. Biol. 2001, 501, 315–323. [Google Scholar] [CrossRef]
- Albrecht, S.; Schols, H.A.; Van Den Heuvel, E.G.H.M.; Voragen, A.G.J.; Gruppen, H. Occurrence of oligosaccharides in feces of breast-fed babies in their first six months of life and the corresponding breast milk. Carbohydr. Res. 2011, 346, 2540–2550. [Google Scholar] [CrossRef]
- De Leoz, M.L.A.; Wu, S.; Strum, J.S.; Niñonuevo, M.R.; Gaerlan, S.C.; Mirmiran, M.; German, J.B.; Mills, D.A.; Lebrilla, C.B.; Underwood, M.A. A quantitative and comprehensive method to analyze human milk oligosaccharide structures in the urine and feces of infants. Anal. Bioanal. Chem. 2013, 405, 4089–4105. [Google Scholar] [CrossRef] [Green Version]
- De Leoz, M.L.A.; Kalanetra, K.M.; Bokulich, N.A.; Strum, J.S.; Underwood, M.A.; German, J.B.; Mills, D.A.; Lebrilla, C.B. Human milk glycomics and gut microbial genomics in infant feces show a correlation between human milk oligosaccharides and gut microbiota: A proof-of-concept study. J. Proteome Res. 2015, 14, 491–502. [Google Scholar] [CrossRef] [Green Version]
- Underwood, M.A.; Gaerlan, S.; De Leoz, M.L.A.; Dimapasoc, L.; Kalanetra, K.M.; Lemay, D.G.; German, J.B.; Mills, D.A.; Lebrilla, C.B. Human Milk Oligosaccharides in Premature Infants: Absorption, Excretion and Influence on the Intestinal Microbiota. Pediatr. Res. 2015, 78, 670. [Google Scholar] [CrossRef] [Green Version]
- Dominguez-Bello, M.G.; Costello, E.K.; Contreras, M.; Magris, M.; Hidalgo, G.; Fierer, N.; Knight, R. Delivery mode shapes the acquisition and structure of the initial microbiota across multiple body habitats in newborns. Proc. Natl. Acad. Sci. USA 2010, 107, 11971–11975. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Collado, M.C.; Cernada, M.; Neu, J.; Pérez-Martínez, G.; Gormaz, M.; Vento, M. Factors influencing gastrointestinal tract and microbiota immune interaction in preterm infants. Pediatr. Res. 2015, 77, 726–731. [Google Scholar] [CrossRef] [PubMed]
- Howland, V.; Klaedtke, M.; Ruhnau, J.; Dhople, V.M.; Grabe, H.J.; Völker, U.; Heckmann, M.; Hammer, E. Impact of Storage Conditions on the Breast Milk Peptidome. Nutrients 2020, 12, 2733. [Google Scholar] [CrossRef] [PubMed]
- Shaw, A.G.; Sim, K.; Powell, E.; Cornwell, E.; Cramer, T.; McClure, Z.E.; Li, M.S.; Kroll, J.S. Latitude in sample handling and storage for infant faecal microbiota studies: The elephant in the room? Microbiome 2016, 4, 40. [Google Scholar] [CrossRef] [Green Version]
- Gorzelak, M.A.; Gill, S.K.; Tasnim, N.; Ahmadi-Vand, Z.; Jay, M.; Gibson, D.L. Methods for Improving Human Gut Microbiome Data by Reducing Variability through Sample Processing and Storage of Stool. PLoS ONE 2015, 10, e0134802. [Google Scholar] [CrossRef]
- Wu, W.-K.; Chen, C.-C.; Panyod, S.; Chen, R.-A.; Wu, M.-S.; Sheen, L.-Y.; Chang, S.-C. Optimization of fecal sample processing for microbiome study—The journey from bathroom to bench. J. Formos. Med. Assoc. 2019, 118, 545–555. [Google Scholar] [CrossRef]


{kind=link}
| Target | Name | Sequence (5′–3′) | Amplicon Length (bp) | Tm | Reference | |
|---|---|---|---|---|---|---|
| 16S | Forward | BACT_1369F | CGG TGA ATA CGT TCY CGG | 142 | 56 | Suzuki et al. [44] |
| Reverse | PROK_1492R | GGW TAC CTT GTT ACG ACT T | ||||
| Bacteroides-Prevotella-Porphyromonas | Forward | - | GGT GTC GGC TTA AGT GC CAT | 140 | 68 | Jian et al. [45] |
| Reverse | - | CGG AYG TAA GGG CCG TGC | ||||
| Bifidobacterium spp. | Forward | - | TCG CGT CYG GTG TGA AAG | 243 | 58 | Jian et al. [45] |
| Reverse | - | CCA CAT CCA GCR TCC AC | ||||
| Clostridium cluster XIVa | Forward | - | CGG TAC CTG ACT AAG AAG C | 429 | 55 | Jian et al. [45] |
| Reverse | - | AGT TTY ATT CTT GCG AAC G | ||||
| Enterobacteriaceae spp. | Forward | En-lsu-3F | TGC CGT AAC TTC GGG AGA AGG CA | 428 | 60 | Matsuda et al. [46] |
| Reverse | En-lsu-3′R | TCA AGG ACC AGT GTT CAG TGT C | ||||
| Enterococcus spp. | Forward | g-Encoc-F | ATC AGA GGG GGA TAA CAC TT | 337 | 55 | Matsuda et al. [47] |
| Reverse | g-Encoc-R | ACT CTC ATC CTT GTT CTT CTC | ||||
| Lactobacillus spp. | Forward | F_alllact_IS | TGG ATG CCT TGG CAC TAG GA | 92 | 58 | Haarman et al. [48] |
| Reverse | R_alllact_IS | AAA TCT CCG GAT CAA AGC TTA CTT AT | ||||
| Probe | P_alllact_IS | TAT TAG TTC CGT CCT TCA TC | 68 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Henderickx, J.G.E.; d’Haens, E.J.; Hemels, M.A.C.; Schoorlemmer, M.E.; Giezen, A.; van Lingen, R.A.; Knol, J.; Belzer, C. From Mum to Bum: An Observational Study Protocol to Follow Digestion of Human Milk Oligosaccharides and Glycoproteins from Mother to Preterm Infant. Nutrients 2021, 13, 3430. https://doi.org/10.3390/nu13103430
Henderickx JGE, d’Haens EJ, Hemels MAC, Schoorlemmer ME, Giezen A, van Lingen RA, Knol J, Belzer C. From Mum to Bum: An Observational Study Protocol to Follow Digestion of Human Milk Oligosaccharides and Glycoproteins from Mother to Preterm Infant. Nutrients. 2021; 13(10):3430. https://doi.org/10.3390/nu13103430
Chicago/Turabian StyleHenderickx, Jannie G. E., Esther J. d’Haens, Marieke A. C. Hemels, Mariëtte E. Schoorlemmer, Astrid Giezen, Richard A. van Lingen, Jan Knol, and Clara Belzer. 2021. "From Mum to Bum: An Observational Study Protocol to Follow Digestion of Human Milk Oligosaccharides and Glycoproteins from Mother to Preterm Infant" Nutrients 13, no. 10: 3430. https://doi.org/10.3390/nu13103430