
Adherence to Dietary Recommendations after One Year of Intervention in Breast Cancer Women: The DIANA-5 Trial

 , , , ,
, , , ,  add
Show full author list
add
Show full author list
Abstract
:1. Introduction
2. Materials and Methods
- To provide copy of the clinical and pathological notes concerning their BC;
- To complete a questionnaire on their medical history and major cancer risk factors, such as menstrual history and reproductive and behavioral factors (e.g., oral contraceptive use, smoking habits);
- To fill in 24 h food frequency diary about the previous day’s food intake;
- To attend a visit for anthropometric and body composition measurements;
- To provide a 20 mL blood sample for metabolic/hormonal assays (plasma glucose, triglycerides, total, LDL and HDL cholesterol, serum insulin, and serum testosterone);
- To agree to participate in the dietary intervention in case of randomization to the IG.
2.1. Dietary Intervention
- Reducing caloric intake through the preferred consumption of highly satiating foods (whole grain cereals, legumes, and vegetables);
- Reducing high glycemic index food (refined flours, potatoes, white rice, corn flakes) and high insulinemic foods (sugar and milk). Nuts and legume flours were proposed in sweet and savory cookery recipes. Desserts were prepared without adding sugars, but using instead nuts, fresh fruit, dates, and small amounts of dates, raisins, and dried apricots;
- Reducing sources of saturated fats (red and processed meat, milk, and dairy products) and avoiding trans fatty acids (margarines and industrial snacks and pastries). Cold-pressed extra-virgin olive oil was the main source of fat. The consumption of nuts and seeds was encouraged;
- Reducing protein intake, mainly animal proteins. Among animal food, fish, especially cold-water fish (e.g., salmon and mackerel), rich in omega-3 polyunsaturated fatty acids, was privileged.
2.2. Dietary Data Collection
2.3. Statistical Analysis
- Whole-grain products (whole bread, whole rice, other whole grain cereals, unsweetened muesli, oat flakes);
- Unsweetened beverages (vegetable milk, tea, barley coffee);
- Vegetables (all vegetables except potatoes);
- Fruit (all kinds of fruit);
- Legumes and soy products (legumes, tofu/tempeh);
- Recommended animal protein products (fish, mollusks, and crustaceans);
- Dried fruit (apricots, raisins, plums);
- Nuts and seeds (hazelnuts, almonds, walnuts, nut creams, and oilseeds);
- Vegetable oils (extra virgin olive oil, seeds oil);
- Spices and seasonings (miso, tamari, spices);
- Sugary beverages (sugary beverages, animal milk);
- Alcoholic drinks (wine, beer, spirits);
- Sweets and cakes (white sugar, artificial sweeteners, chocolate, candies, biscuits, ice creams, brioches);
- Refined cereals (white bread, white rice, egg noodles, corn flakes, sweetened muesli);
- Discouraged animal protein products (red meat, processed meat);
- Discouraged vegetable protein products (seitan);
- Dairy products (all kinds of fresh or seasoned cheese, including pizza or pasta);
- Starchy vegetables (potatoes, mashed potatoes, French fries);
- Butter and other discouraged seasonings (butter, lard cream, margarine, ready sauces, mayonnaise, ketchup).
- White meat, eggs, coffee, unsweetened citrus juices, and unsweetened fruit juices were considered neutral food (not recommended but not discouraged).
3. Results
3.1. Baseline Metabolic and Anthropometric Characteristics of the Study Population by Randomization Group
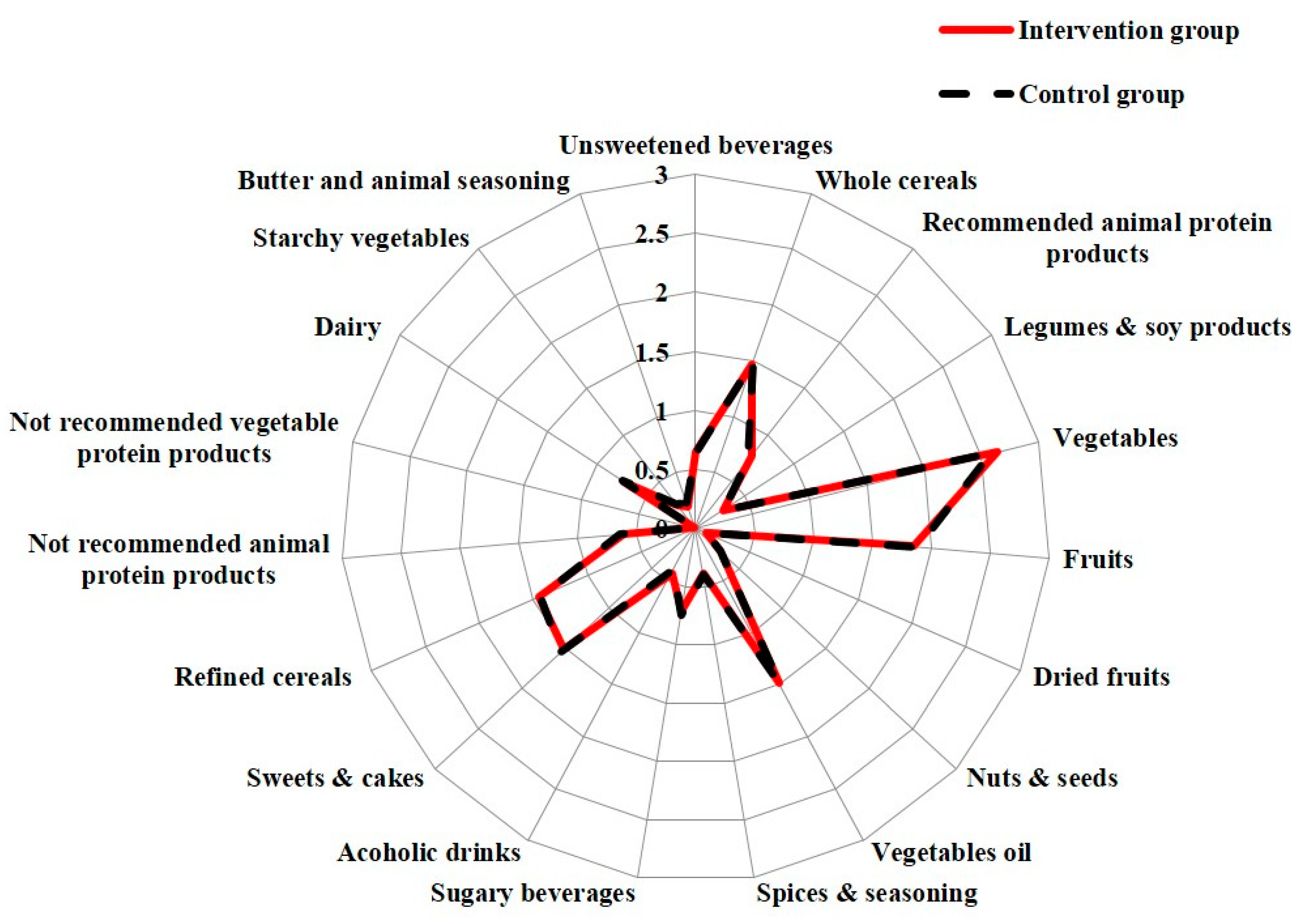
3.2. Baseline Dietary Daily Frequency of Consumption of Recommended and Discouraged Food by Randomization Group
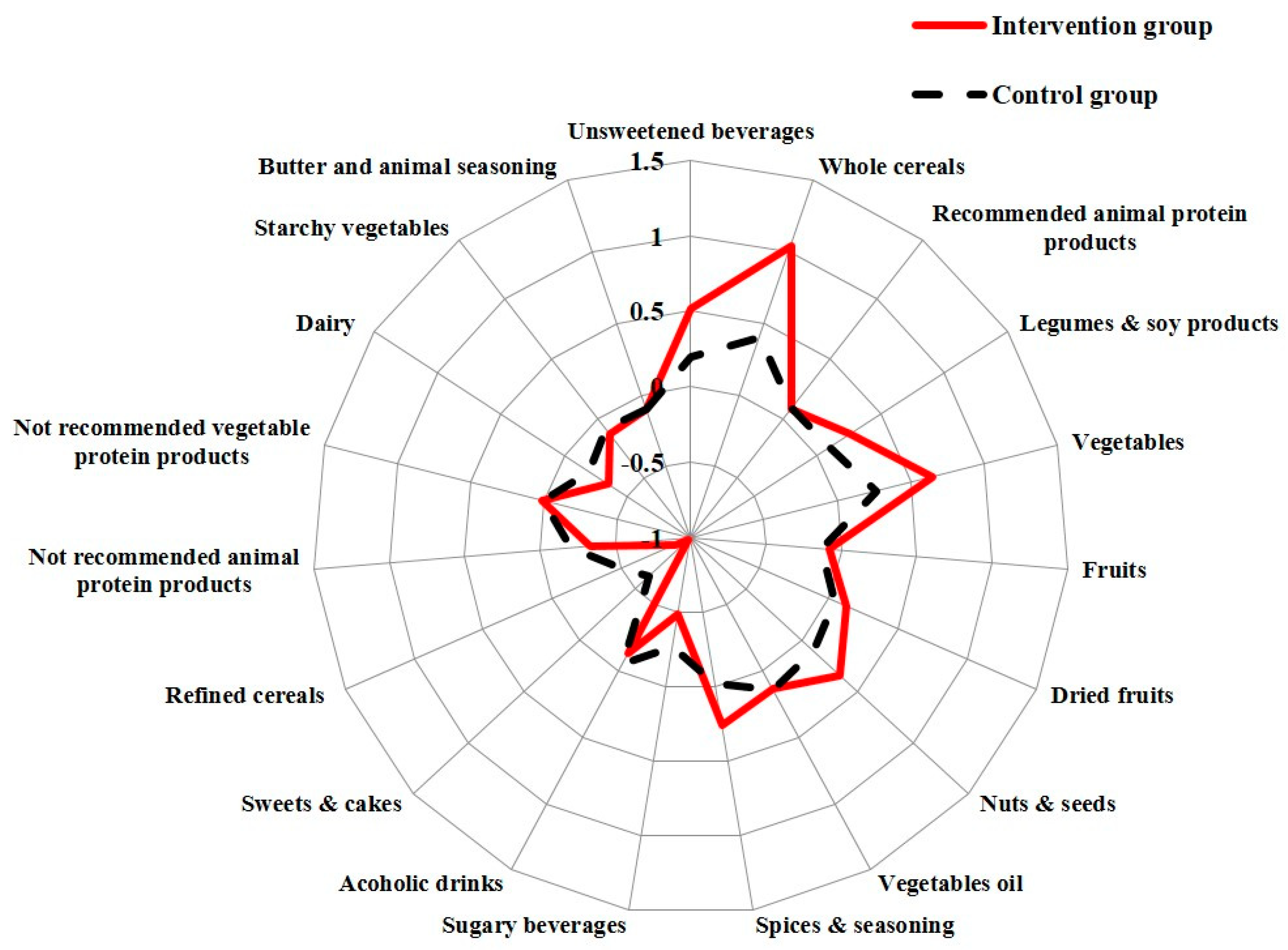
3.3. Changes of Food Frequencies Consumption by Randomization Group
3.4. Changes of Anthropometric and Metabolic Parameters by Randomization Group
3.5. Changes in ΔMS Parameters According to the Δ of Recommended Food Consumption and Discouraged Food Consumption after One Year of Dietary Intervention
3.6. Association between the Adherence to DIANA-5 Dietary Recommendations and Δbody Weight
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Cancer Research Fund, American Institute for Cancer Research. Food, Nutrition, Physical Activity and the Prevention of Cancer: A Global Perspective; AICR: Washington, DC, USA, 2007. [Google Scholar]
- Berrino, F.; Bellati, C.; Secreto, G.; Camerini, E.; Pala, V.; Panico, S.; Allegro, G.; Kaaks, R. Reducing bioavailable sex hormones through a comprehensive change in diet: The diet and androgens (DIANA) randomized trial. Cancer Epidemiol. Biomark. Prev. 2001, 10, 25–33. [Google Scholar]
- Kaaks, R.; Bellati, C.; Venturelli, E.; Rinaldi, S.; Secreto, G.; Biessy, C.; Pala, V.; Sieri, S.; Berrino, F. Effects of dietary intervention on IGF-I and IGF-binding proteins, and related alterations in sex steroid metabolism: The Diet and Androgens (DIANA) Randomised Trial. Eur. J. Clin. Nutr. 2003, 57, 1079–1088. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agnoli, C.; Berrino, F.; Abagnato, C.A.; Muti, P.; Panico, S.; Crosignani, P.; Krogh, V. Metabolic syndrome and postmenopausal breast cancer in the ORDET cohort: A nested case-control study. Nutr. Metab. Cardiovasc. Dis. 2010, 20, 41–48. [Google Scholar] [CrossRef] [Green Version]
- Berrino, F.; Pasanisi, P.; Bellati, C.; Venturelli, E.; Krogh, V.; Mastroianni, A.; Berselli, E.; Muti, P.; Secreto, G. Serum testosterone levels and breast cancer recurrence. Int. J. Cancer 2005, 113, 499–502. [Google Scholar] [CrossRef]
- Villarini, A.; Pasanisi, P.; Traina, A.; Mano, M.P.; Bonanni, B.; Panico, S.; Scipioni, C.; Galasso, R.; Paduos, A.; Simeoni, M.; et al. Lifestyle and breast cancer recurrences: The DIANA-5 trial. Tumori J. 2012, 98, 1–18. [Google Scholar] [CrossRef]
- Berrino, F.; Villarini, A.; Traina, A.; Bonanni, B.; Panico, S.; Mano, M.P.; Mercandino, A.; Galasso, R.; Barbero, M.; Simeoni, M.; et al. Metabolic syndrome and breast cancer prognosis. Breast Cancer Res. Treat. 2014, 147, 159–165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bruno, E.; Gargano, G.; Villarini, A.; Traina, A.; Johansson, H.; Mano, M.P.; Santucci De, M.M.; Simeoni, M.; Consolaro, E.; Mercandino, A.; et al. Adherence to WCRF/AICR cancer prevention recommendations and metabolic syndrome in breast cancer patients. Int. J. Cancer 2016, 138, 237–244. [Google Scholar] [CrossRef] [Green Version]
- Rezac, S.; Kok, C.R.; Heermann, M.; Hutkins, R. Fermented Foods as a Dietary Source of Live Organisms. Front. Microbiol. 2018, 9, 1785. [Google Scholar] [CrossRef]
- Alberti, K.G.; Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z.; Cleeman, J.I.; Donato, K.A.; Fruchart, J.C.; James, W.P.; Loria, C.M.; Smith, S.C., Jr. Harmonizing the metabolic syndrome: A joint interim statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation 2009, 120, 1640–1645. [Google Scholar]
- Chlebowski, R.T.; Blackburn, G.L.; Thomson, C.A.; Nixon, D.W.; Shapiro, A.; Hoy, M.K.; Goodman, M.T.; Giuliano, A.E.; Karanja, N.; McAndrew, P.; et al. Dietary fat reduction and breast cancer outcome: Interim efficacy results from the Women’s Intervention Nutrition Study. J. Natl. Cancer Inst. 2006, 98, 1767–1776. [Google Scholar] [CrossRef] [Green Version]
- Pierce, J.P.; Natarajan, L.; Caan, B.J.; Parker, B.A.; Greenberg, E.R.; Flatt, S.W.; Rock, C.L.; Kealey, S.; Al-Delaimy, W.K.; Bardwell, W.A.; et al. Influence of a diet very high in vegetables, fruit, and fiber and low in fat on prognosis following treatment for breast cancer: The Women’s Healthy Eating and Living (WHEL) randomized trial. JAMA 2007, 298, 289–298. [Google Scholar] [CrossRef]
- Allin, K.H.; Nordestgaard, B.G.; Flyger, H.; Bojesen, S.E. Elevated pre-treatment levels of plasma C-reactive protein are associated with poor prognosis after breast cancer: A cohort study. Breast Cancer Res. 2011, 13, R55. [Google Scholar] [CrossRef] [Green Version]
- Duggan, C.; Irwin, M.L.; Xiao, L.; Henderson, K.D.; Smith, A.W.; Baumgartner, R.N.; Baumgartner, K.B.; Bernstein, L.; Ballard-Barbash, R.; McTiernan, A. Associations of insulin resistance and adiponectin with mortality in women with breast cancer. J. Clin. Oncol. 2011, 29, 32–39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goodwin, P.J.; Ennis, M.; Pritchard, K.I.; Trudeau, M.E.; Koo, J.; Madarnas, Y.; Hartwick, W.; Hoffman, B.; Hood, N. Fasting insulin and outcome in early-stage breast cancer: Results of a prospective cohort study. J. Clin. Oncol. 2002, 20, 42–51. [Google Scholar] [CrossRef]
- Micheli, A.; Meneghini, E.; Secreto, G.; Berrino, F.; Venturelli, E.; Cavalleri, A.; Camerini, T.; Di Mauro, M.G.; Cavadini, E.; De Palo, G.; et al. Plasma testosterone and prognosis of postmenopausal breast cancer patients. J. Clin. Oncol. 2007, 25, 2685–2690. [Google Scholar] [CrossRef] [PubMed]
- Esposito, K.; Marfella, R.; Ciotola, M.; Di Palo, C.; Giugliano, F.; Giugliano, G.; D’Armiento, M.; D’Andrea, F.; Giugliano, D. Effect of a mediterranean-style diet on endothelial dysfunction and markers of vascular inflammation in the metabolic syndrome: A randomized trial. JAMA 2004, 292, 1440–1446. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Babio, N.; Toledo, E.; Estruch, R.; Ros, E.; MartÃnez-González, M.A.; Castañer, O.; Bulló, M.; Corella, D.; Arós, F.; Gómez-Gracia, E.; et al. Mediterranean diets and metabolic syndrome status in the PREDIMED randomized trial. CMAJ 2014, 186, E649–E657. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fappa, E.; Yannakoulia, M.; Ioannidou, M.; Skoumas, Y.; Pitsavos, C.; Stefanadis, C. Telephone counseling intervention improves dietary habits and metabolic parameters of patients with the metabolic syndrome: A randomized controlled trial. Rev. Diabet Stud. 2012, 9, 36–45. [Google Scholar] [CrossRef] [Green Version]
- Salas-Salvado, J.; Fernandez-Ballart, J.; Ros, E.; Martinez-Gonzalez, M.A.; Fito, M.; Estruch, R.; Corella, D.; Fiol, M.; Gomez-Gracia, E.; Aros, F.; et al. Effect of a Mediterranean diet supplemented with nuts on metabolic syndrome status: One-year results of the PREDIMED randomized trial. Arch. Intern. Med. 2008, 168, 2449–2458. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Howard-Anderson, J.; Ganz, P.A.; Bower, J.E.; Stanton, A.L. Quality of life, fertility concerns, and behavioral health outcomes in younger breast cancer survivors: A systematic review. J. Natl. Cancer Inst. 2012, 104, 386–405. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thomson, C.A.; Giuliano, A.; Rock, C.L.; Ritenbaugh, C.K.; Flatt, S.W.; Faerber, S.; Newman, V.; Caan, B.; Graver, E.; Hartz, V.; et al. Measuring dietary change in a diet intervention trial: Comparing food frequency questionnaire and dietary recalls. Am. J. Epidemiol. 2003, 157, 754–762. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| IG | CG | p * | |
|---|---|---|---|
| (N = 769) | (N = 773) | ||
| Age at recruitment (years) | 52.0 ± 8.5 | 51.7 ± 8.3 | 0.37 |
| Education (%) | |||
| First level | 24.7 | 25.4 | |
| Second level | 46 | 47.8 | 0.34 |
| Third level | 29.3 | 26.8 | |
| ER-negative (%) | 21.3 | 20.6 | 0.62 |
| Menopause (%) | 40.9 | 39.4 | 0.61 |
| Natural menopause (%) | 80.2 | 80.2 | 0.98 |
| Tumor stage (%) | |||
| IA | 43.1 | 41.8 | |
| IB | 17.6 | 17.2 | |
| IIA | 13.6 | 14.2 | |
| IIB | 9.7 | 11.5 | |
| IIIA | 9 | 9.5 | |
| IIIB | 0.6 | 1.1 | |
| IIIC | 6.4 | 4.7 | 0.46 |
| Height (cm) | 160.8 ± 6.3 | 160.6 ± 6.3 | 0.52 |
| Weight (kg) | 68.9 ± 13.0 | 68.3 ± 12.8 | 0.28 |
| BMI (kg/m2) | 26.7 ± 5.0 | 26.5 ± 5.1 | 0.5 |
| Waist circumference (cm) | 87.5 ± 12.4 | 86.8 ± 12.3 | 0.29 |
| Systolic blood pressure (mm/Hg) | 127.5 ± 18.5 | 126.4 ± 18.6 | 0.26 |
| Diastolic blood pressure (mm/Hg) | 82.4 ± 11.4 | 81.6 ± 11.9 | 0.18 |
| Fasting glucose (mg/dL) | 94.3 ± 18.1 | 94.0 ± 16.1 | 0.67 |
| HDL (mg/dL) | 60.3 ± 15.6 | 61.5 ± 15.5 | 0.13 |
| Triglycerides (mg/dL) | 113.8 ± 68.0 | 109.4 ± 61.3 | 0.18 |
| Number of MS parameters | |||
| 0 | 12.4 | 16.2 | |
| 1 | 23 | 22 | |
| 2 | 24.6 | 26.7 | |
| 3 | 23 | 21.4 | |
| 4 | 12.3 | 10.8 | |
| 5 | 4.7 | 2.9 | 0.1 |
| IG | CG | IG | CG | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Baseline Mean ± SD | 1 Year Mean ± SD | p * | Baseline Mean ± SD | 1 Year Mean ± SD | p * | Δ | Δ | p ** | |
| (N = 689) | (N = 689) | (N = 655) | (N = 655) | ||||||
| Weight (kg) | 68.9 ± 12.9 | 66.5 ± 13.1 | <0.001 | 67.7 ± 12.4 | 66.8 ± 12.5 | <0.001 | −2.4 | −0.9 | <0.001 |
| BMI (kg/m2) | 26.6 ± 5.0 | 25.7 ± 5.0 | <0.001 | 26.2 ± 4.9 | 25.8 ± 4.9 | <0.001 | −1.0 | −0.4 | <0.001 |
| Waist circ. (cm) | 87.3 ± 12.3 | 84.7 ± 12.3 | <0.001 | 86.2 ± 12.1 | 85.2 ± 11.8 | <0.001 | −2.6 | −1.0 | <0.001 |
| Diastolic pressure (mm/Hg) | 82.4 ± 11.4 | 80.8 ± 11.7 | <0.001 | 81.2 ± 11.9 | 80.4 ± 10.4 | 0.02 | −1.6 | −0.8 | 0.16 |
| Systolic pressure (mm/Hg) | 127.7 ± 18.2 | 125.5 ± 19.1 | <0.001 | 126.0 ± 18.2 | 125.2 ± 17.8 | 0.24 | −2.2 | −0.8 | 0.1 |
| Fasting glucose (mg/dL) | 94.2 ± 17.2 | 92.5 ± 16.3 | <0.001 | 93.7 ± 14.0 | 93.1 ± 13.7 | 0.21 | −1.7 | −0.5 | 0.04 |
| HDL (mg/dL) | 60.8 ± 15.7 | 61.2 ± 16.1 | 0.28 | 62.3 ± 15.5 | 62.7 ± 16.0 | 0.34 | 0.4 | 0.4 | 0.95 |
| Triglycerides (mg/dL) | 114.3 ± 70.8 | 100.3 ± 61.6 | <0.001 | 107.4 ± 59.6 | 99.2 ± 51.6 | <0.001 | −14.0 | −8.2 | 0.03 |
| Number of MS parameters | |||||||||
| 0 | 12.3 | 18 | 16.2 | 18.9 | 5.7 | 2.7 | |||
| 1 | 23 | 22 | 22 | 23.5 | −1.0 | 1.5 | |||
| 2 | 24.7 | 29.2 | 26.7 | 28 | 4.5 | 1.3 | |||
| 3 | 23 | 18.6 | 21.4 | 16.8 | −4.4 | −4.6 | |||
| 4 | 12.3 | 10 | 10.8 | 9.7 | −2.3 | −1.1 | |||
| 5 | 4.7 | 2.2 | <0.001 | 2.9 | 3.1 | <0.001 | −2.5 | 0.2 | 0.01 |
| RFC/day § | 10.1 ± 5.4 | 13.9 ± 5.9 | <0.001 | 10.1 ± 5.3 | 11.4 ± 5.4 | <0.001 | 1.8 | 1.3 | <0.001 |
| DFC/day § | 5.6 ± 3.1 | 2.6 ± 2.8 | <0.001 | 5.6 ± 3.9 | 3.9 ± 2.9 | <0.001 | −3.0 | −1.8 | <0.001 |
| DCI § | 2.6 ± 2.7 | 6.9 ± 6.0 | <0.001 | 2.6 ± 2.2 | 4.3 ± 4.5 | <0.001 | 4.5 | 1.9 | <0.001 |
| ΔMS Parameters (a) | ||||
|---|---|---|---|---|
| ΔRFC/Day § | Worsening | No Change | Low Improvement | High Improvement |
| 1st Tertile (<+1) (n = 435) | 1 | 1 | 1 | 1 |
| 2nd Tertile (1 to 5) (n = 494) | 0.84 (0.46–1.54) | 1 | 0.94 (0.51–1.74) | 1.26 (0.67–2.38) |
| 3rd Tertile (>5) (n = 369) | 0.75 (0.39–1.43) | 1 | 0.96 (0.50–1.84) | 1.37 (0.70–2.67) |
| ΔMS Parameters (b) | ||||
| ΔDFC/Day § | Worsening | No Change | Low Improvement | High Improvement |
| 1st Tertile (<−1) (n = 356) | 1 | 1 | 1 | 1 |
| 2nd Tertile (−3 to –1) (n = 478) | 1.02 (0.55–1.88) | 1 | 1.07 (0.58–2.02) | 1.26 (0.66–2.40) |
| 3rd Tertile(>−4) (n = 464) | 1.18 (0.61–2.27) | 1 | 1.53 (0.79–2.96) | 2.02 (1.03–3.98) |
| 1st Tertile ΔRFC (<+1) (n = 435) | 2nd Tertile ΔRFC (+1 to +5) (n = 494) | 3rd Tertile ΔRFC (>+5) (n = 369) | |
|---|---|---|---|
| 1st TertileΔDFC (<−1) (n = 356) | 1 | 0.67 (0.39–1.13) | 0.74 (0.39–1.40) |
| 2nd TertileΔDFC (−3 to −1) (n = 478) | 1.08 (0.66–1.77) | 1.51 (0.94–2.40) | 1.64 (0.98–2.72) |
| 3rd TertileΔDFC (>−4) (n = 464) | 1.18 (0.70–1.97) | 2.10 (1.29–3.40) | 4.14 (2.51–6.28) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bruno, E.; Krogh, V.; Gargano, G.; Grioni, S.; Bellegotti, M.; Venturelli, E.; Panico, S.; Santucci de Magistris, M.; Bonanni, B.; Zagallo, E.; et al. Adherence to Dietary Recommendations after One Year of Intervention in Breast Cancer Women: The DIANA-5 Trial. Nutrients 2021, 13, 2990. https://doi.org/10.3390/nu13092990
Bruno E, Krogh V, Gargano G, Grioni S, Bellegotti M, Venturelli E, Panico S, Santucci de Magistris M, Bonanni B, Zagallo E, et al. Adherence to Dietary Recommendations after One Year of Intervention in Breast Cancer Women: The DIANA-5 Trial. Nutrients. 2021; 13(9):2990. https://doi.org/10.3390/nu13092990
Chicago/Turabian StyleBruno, Eleonora, Vittorio Krogh, Giuliana Gargano, Sara Grioni, Manuela Bellegotti, Elisabetta Venturelli, Salvatore Panico, Maria Santucci de Magistris, Bernardo Bonanni, Emanuela Zagallo, and et al. 2021. "Adherence to Dietary Recommendations after One Year of Intervention in Breast Cancer Women: The DIANA-5 Trial" Nutrients 13, no. 9: 2990. https://doi.org/10.3390/nu13092990