
Assessment of Adherence to the Healthy Food Pyramid in Pregnant and Lactating Women

 , , ,
, , ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
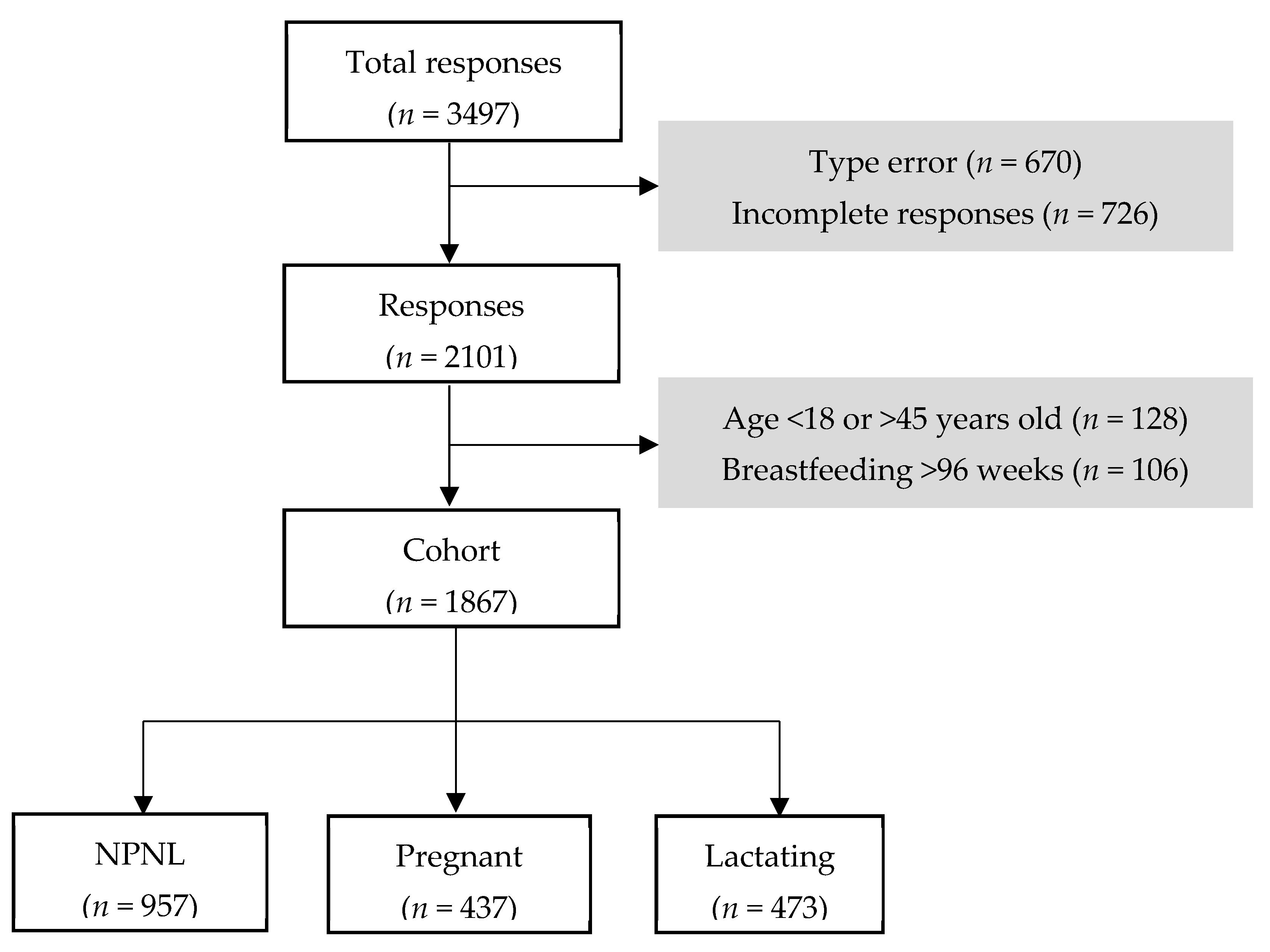
2.1. Study Design and Participants Recruitment
2.2. Measurement of Women Dietary Patterns and Lifestyle
2.3. Statistical Analysis
3. Results
3.1. Population Characteristics
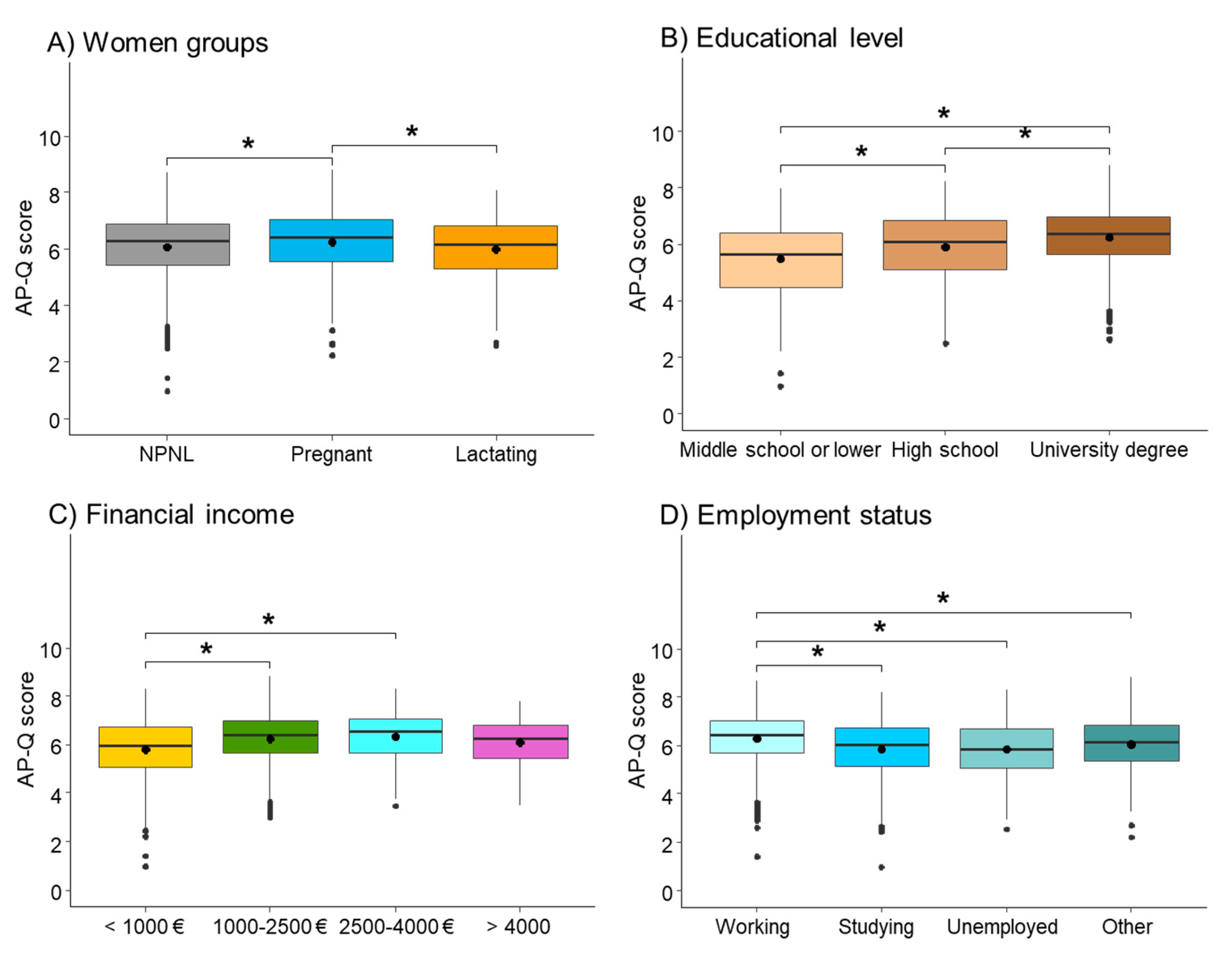
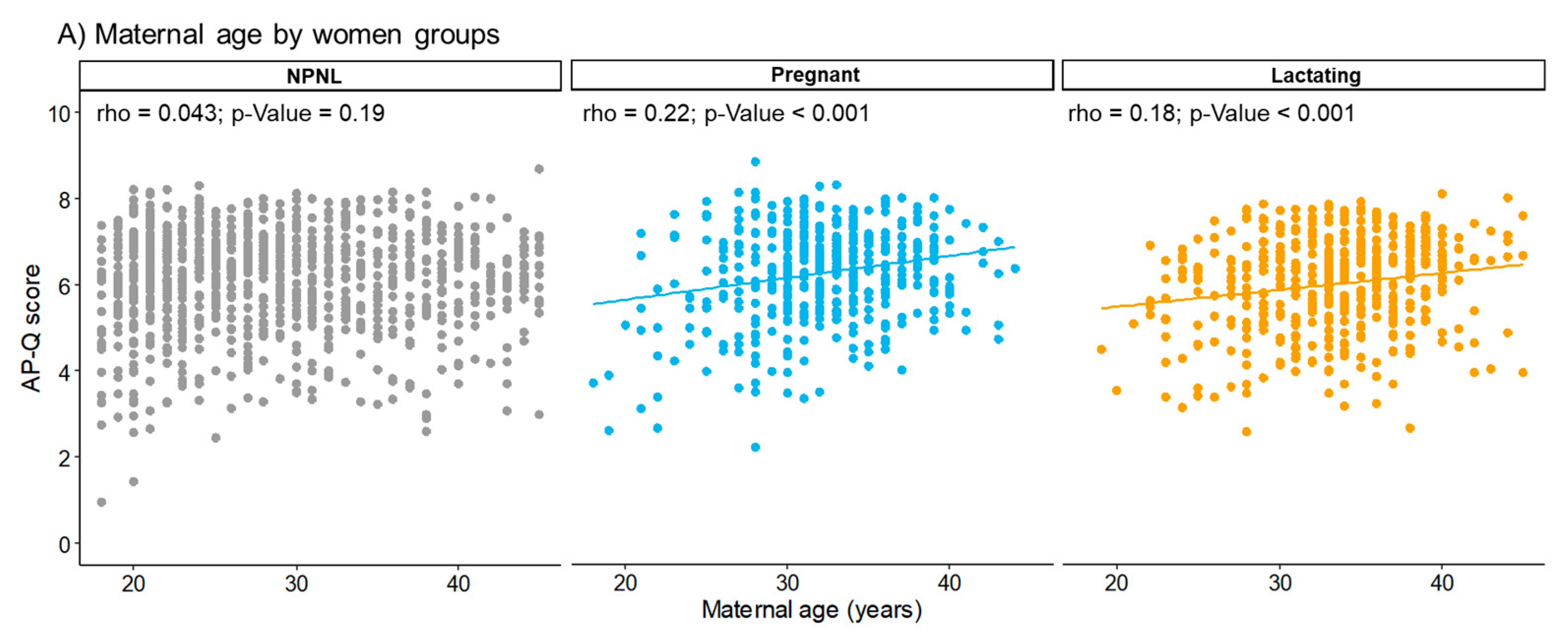
3.2. AP-Q Score and Association between Women
3.3. AP-Q Categories
4. Discussion
5. Conclusions
- Women in our cohort had a moderate adherence to the HFP, with younger women having less healthy lifestyles.
- Educational level, employment status, and high monthly income have a positive influence on adherence to the HFP.
- Breastfeeding women had the lowest adherence to nutritional, lifestyle, and healthy habits, suggesting the need for specific counseling.
- Dairy product consumption was low in the population, and deserves close attention, particularly in pregnant and breastfeeding women.
- Adherence to the recommendations on fruit, vegetable, and olive oil intake was adequate.
- It would be desirable to create guidelines of nutritional and lifestyle recommendations for breastfeeding women. Furthermore, follow-up by a nutritionist could improve women’s health during the puerperium.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bruins, M.J.; Van Dael, P.; Eggersdorfer, M. The Role of Nutrients in Reducing the Risk for Noncommunicable Diseases during Aging. Nutrients 2019, 11, 85. [Google Scholar] [CrossRef] [PubMed]
- Yajnik, C.S.; Deshmukh, U.S. Maternal nutrition, intrauterine programming and consequential risks in the offspring. Rev. Endocr. Metab. Disord. 2008, 9, 203–211. [Google Scholar] [CrossRef]
- Sanidad, M.D. Guía de Práctica Clínica de Atención en el Embarazo y Puerperio. Available online: https://portal.guiasalud.es/wp-content/uploads/2018/12/GPC_533_Embarazo_AETSA_compl.pdf (accessed on 25 June 2021).
- Sanidad, M.D. Guía de Práctica Clínica Sobre Lactancia Materna. Available online: https://www.aeped.es/sites/default/files/guia_de_lactancia_materna.pdf (accessed on 25 June 2021).
- Eleftheriou, D.; Benetou, V.; Trichopoulou, A.; La Vecchia, C.; Bamia, C. Mediterranean diet and its components in relation to all-cause mortality: Meta-analysis. Br. J. Nutr. 2018, 120, 1081–1097. [Google Scholar] [CrossRef]
- Martinez-González, M.A.; Salas-Salvadó, J.; Estruch, R.; Corella, D.; Fitó, M.; Ros, E.; Predimed, I. Benefits of the Mediterranean Diet: Insights From the PREDIMED Study. Prog. Cardiovasc. Dis. 2015, 58, 50–60. [Google Scholar] [CrossRef] [Green Version]
- SENC. Nuevas Guías Alimentarias para la Población Española. Available online: https://www.nutricioncomunitaria.org/es/noticia/piramide-de-la-alimentacion-saludable-senc-2015 (accessed on 25 June 2021).
- Diolintzi, A.; Panagiotakos, D.B.; Sidossis, L.S. From Mediterranean diet to Mediterranean lifestyle: A narrative review. Public Health Nutr. 2019, 22, 2703–2713. [Google Scholar] [CrossRef]
- Bouzas, C.; Bibiloni, M.D.M.; Julibert, A.; Ruiz-Canela, M.; Salas-Salvadó, J.; Corella, D.; Zomeño, M.D.; Romaguera, D.; Vioque, J.; Alonso-Gómez, Á.M.; et al. Adherence to the Mediterranean Lifestyle and Desired Body Weight Loss in a Mediterranean Adult Population with Overweight: A PREDIMED-Plus Study. Nutrients 2020, 12, 2114. [Google Scholar] [CrossRef]
- Melero, V.; García de la Torre, N.; Assaf-Balut, C.; Jiménez, I.; Del Valle, L.; Durán, A.; Bordiú, E.; Valerio, J.J.; Herraiz, M.A.; Izquierdo, N.; et al. Effect of a Mediterranean Diet-Based Nutritional Intervention on the Risk of Developing Gestational Diabetes Mellitus and Other Maternal-Fetal Adverse Events in Hispanic Women Residents in Spain. Nutrients 2020, 12, 3505. [Google Scholar] [CrossRef] [PubMed]
- Parlapani, E.; Agakidis, C.; Karagiozoglou-Lampoudi, T.; Sarafidis, K.; Agakidou, E.; Athanasiadis, A.; Diamanti, E. The Mediterranean diet adherence by pregnant women delivering prematurely: Association with size at birth and complications of prematurity. J. Matern-Fetal Neonatal Med. 2019, 32, 1084–1091. [Google Scholar] [CrossRef] [PubMed]
- Krešić, G.; Dujmović, M.; Mandić, M.L.; Delaš, I. Relationship between Mediterranean diet and breast milk fatty acid profile: A study in breastfeeding women in Croatia. Dairy Sci. Technol. 2013, 93, 287–301. [Google Scholar] [CrossRef] [Green Version]
- Shim, J.S.; Oh, K.; Kim, H.C. Dietary assessment methods in epidemiologic studies. Epidemiol. Health 2014, 36, e2014009. [Google Scholar] [CrossRef] [PubMed]
- Burke, B.S. The dietary history as a tool in research. Journal of the American Dietetic Association. J. Am. Diet. Assoc. 1947, 23, 1041–1046. [Google Scholar]
- Trichopoulou, A.; Costacou, T.; Bamia, C.; Trichopoulos, D. Adherence to a Mediterranean diet and survival in a Greek population. N. Engl. J. Med. 2003, 348, 2599–2608. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kepler, S. Adherence to the Mediterranean diet and quality of life in the SUN Project. Eur. J. Clin. Nutr. 2012, 66, 975. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galilea-Zabalza, I.; Buil-Cosiales, P.; Salas-Salvadó, J.; Toledo, E.; Ortega-Azorín, C.; Díez-Espino, J.; Vázquez-Ruiz, Z.; Zomeño, M.D.; Vioque, J.; Martínez, J.A.; et al. Mediterranean diet and quality of life: Baseline cross-sectional analysis of the PREDIMED-PLUS trial. PLoS ONE 2018, 13, e0198974. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kleiman, S.C. Measuring adherence to the Mediterranean diet. Eur. J. Clin. Nutr. 2012, 66, 973. [Google Scholar] [CrossRef] [Green Version]
- Serra-Majem, L.; Ribas, L.; Ngo, J.; Ortega, R.M.; García, A.; Pérez-Rodrigo, C.; Aranceta, J. Food, youth and the Mediterranean diet in Spain. Development of KIDMED, Mediterranean Diet Quality Index in children and adolescents. Public Health Nutr. 2004, 7, 931–935. [Google Scholar] [CrossRef] [PubMed]
- Zurita-Ortega, F.; Román-Mata, S.; Chacón-Cuberos, R.; Castro-Sánchez, M.; Muros, J.J. Adherence to the Mediterranean Diet Is Associated with Physical Activity, Self-Concept and Sociodemographic Factors in University Student. Nutrients 2018, 10, 966. [Google Scholar] [CrossRef] [Green Version]
- Yannakoulia, M.; Lykou, A.; Kastorini, C.M.; Papasaranti, E.S.; Petralias, A.; Veloudaki, A.; Linos, A.; DIATROFI Program Research Team. Socio-economic and lifestyle parameters associated with diet quality of children and adolescents using classification and regression tree analysis: The DIATROFI study. Public Health Nutr. 2016, 19, 339–347. [Google Scholar] [CrossRef] [Green Version]
- Gila-Díaz, A.; Arribas, S.M.; López de Pablo, Á.L.; López-Giménez, M.R.; Phuthong, S.; Ramiro-Cortijo, D. Development and Validation of a Questionnaire to Assess Adherence to the Healthy Food Pyramid in Spanish Adults. Nutrients 2020, 12, 1656. [Google Scholar] [CrossRef]
- Gila-Díaz, A.; Diaz-Rullo Alcántara, N.; Herranz Carrillo, G.; Singh, P.; Arribas, S.M.; Ramiro-Cortijo, D. Multidimensional Approach to Assess Nutrition and Lifestyle in Breastfeeding Women during the First Month of Lactation. Nutrients 2021, 13, 1766. [Google Scholar] [CrossRef]
- WHO. Breastfeeding. Available online: https://apps.who.int/nutrition/topics/exclusive_breastfeeding/en/index.html (accessed on 25 June 2021).
- Bach-Faig, A.; Berry, E.M.; Lairon, D.; Reguant, J.; Trichopoulou, A.; Dernini, S.; Medina, F.X.; Battino, M.; Belahsen, R.; Miranda, G.; et al. Mediterranean diet pyramid today. Science and cultural updates. Public Health Nutr. 2011, 14, 2274–2284. [Google Scholar] [CrossRef] [Green Version]
- Sotos-Prieto, M.; Moreno-Franco, B.; Ordovás, J.M.; León, M.; Casasnovas, J.A.; Peñalvo, J.L. Design and development of an instrument to measure overall lifestyle habits for epidemiological research: The Mediterranean Lifestyle (MEDLIFE) index. Public Health Nutr. 2015, 18, 959–967. [Google Scholar] [CrossRef]
- EUROSTAT. Women in the EU are Having Their First Child Later. Available online: https://ec.europa.eu/eurostat/web/products-eurostat-news/-/DDN-20210224-1 (accessed on 25 June 2021).
- Fernández, M.Á.L.; Cavanillas, A.B.; Dramaix-Wilmet, M.; Soria, F.S.; Campos, J.D.M.D.; Guibert, D.H. Increase in maternal mortality associated with change in the reproductive pattern in Spain: 1996–2005. J. Epidemiol. Community Health 2009, 63, 433–438. [Google Scholar] [CrossRef] [PubMed]
- Pittman, T. Socioeconomic Factors Play Significant Role in Health Outcomes. Available online: https://physicians.dukehealth.org/articles/socioeconomic-factors-play-significant-role-health-outcomes (accessed on 25 June 2021).
- INE. Renta por Persona y Unidad De Consumo por Nivel de Formacion Alcanzado (Personas de 16 y más años). Available online: https://ine.es/jaxiT3/Datos.htm?t=9943 (accessed on 25 June 2021).
- Predieri, S.; Sinesio, F.; Monteleone, E.; Spinelli, S.; Cianciabella, M.; Daniele, G.M.; Dinnella, C.; Gasperi, F.; Endrizzi, I.; Torri, L.; et al. Gender, Age, Geographical Area, Food Neophobia and Their Relationships with the Adherence to the Mediterranean Diet: New Insights from a Large Population Cross-Sectional Study. Nutrients 2020, 12, 1778. [Google Scholar] [CrossRef]
- Havaš Auguštin, D.; Šarac, J.; Lovrić, M.; Živković, J.; Malev, O.; Fuchs, N.; Novokmet, N.; Turkalj, M.; Missoni, S. Adherence to Mediterranean Diet and Maternal Lifestyle during Pregnancy: Island-Mainland Differentiation in the CRIBS Birth Cohort. Nutrients 2020, 12, 2179. [Google Scholar] [CrossRef] [PubMed]
- Cuervo, M.; Sayon-Orea, C.; Santiago, S.; Martínez, J.A. Dietary and health profiles of Spanish women in preconception, pregnancy and lactation. Nutrients 2014, 6, 4434–4451. [Google Scholar] [CrossRef] [Green Version]
- Spanish-Government. Real Decreto-ley 6/2019, de 1 de Marzo, de Medidas Urgentes para Garantía de la Igualdad de trato y de Oportunidades Entre Mujeres y Hombres en el Empleo y la Ocupación; Jefatura-del-Estado, Ed.; BOE: Madrid, Spain, 2019; Volume 57, pp. 21692–21717. [Google Scholar]
- Blum, J.W.; Beaudoin, C.M.; Caton-Lemos, L. Physical activity patterns and maternal well-being in postpartum women. Matern. Child Health J. 2004, 8, 163–169. [Google Scholar] [CrossRef] [PubMed]
- Døheim, S.K.; Bondevik, G.T.; Eberhard-Gran, M.; Bjorvatn, B. Sleep and depression in postpartum women: A population-based study. Sleep 2009, 32, 847–855. [Google Scholar] [CrossRef] [Green Version]
- Stuebe, A.M.; Meltzer-Brody, S.; Propper, C.; Pearson, B.; Beiler, P.; Elam, M.; Walker, C.; Mills-Koonce, R.; Grewen, K. The Mood, Mother, and Infant Study: Associations between Maternal Mood in Pregnancy and Breastfeeding Outcome. Breastfeed. Med. 2019, 14, 551–559. [Google Scholar] [CrossRef]
- Dusdieker, L.B.; Booth, B.M.; Stumbo, P.J.; Eichenberger, J.M. Effect of supplemental fluids on human milk production. J. Pediatr. 1985, 106, 207–211. [Google Scholar] [CrossRef]
- Zhou, Y.; Zhu, X.; Qin, Y.; Li, Y.; Zhang, M.; Liu, W.; Huang, H.; Xu, Y. Association between total water intake and dietary intake of pregnant and breastfeeding women in China: A cross-sectional survey. BMC Pregnancy Childbirth 2019, 19, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Ndikom, C.M.; Fawole, B.; Ilesanmi, R.E. Extra fluids for breastfeeding mothers for increasing milk production. Cochrane Database Syst. Rev. 2014, 6. [Google Scholar] [CrossRef] [PubMed]
- Mazzocchi, A.; Leone, L.; Agostoni, C.; Pali-Schöll, I. The Secrets of the Mediterranean Diet. Does [Only] Olive Oil Matter? Nutrients 2019, 11, 2941. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clemente, A. Legumbres Españolas para Consumo Humano: ¿qué Estrategias Seguir? Available online: https://www.mapa.gob.es/es/agricultura/temas/producciones-agricolas/ael-alfonsoclementemapa2019_tcm30-508189.pdf (accessed on 25 June 2021).
- Martin-Peláez, S.; Covas, M.I.; Fitó, M.; Kušar, A.; Pravst, I. Health effects of olive oil polyphenols: Recent advances and possibilities for the use of health claims. Mol. Nutr. Food Res. 2013, 57, 760–771. [Google Scholar] [CrossRef]
- Nutrition-and-you. Olive Oil Nutrition Facts. Available online: https://www.nutrition-and-you.com/olive-oil.html (accessed on 25 June 2021).
- Wagner, C.L.; Taylor, S.N.; Johnson, D.D.; Hollis, B.W. The role of vitamin D in pregnancy and lactation: Emerging concepts. Women’s Health 2012, 8, 323–340. [Google Scholar] [CrossRef] [Green Version]
- Gellert, S.; Strohle, A.; Hahn, A. Breastfeeding woman are at higher risk of vitamin D deficiency than non-breastfeeding women-insights from the German VitaMinFemin study. Int. Breastfeed. J. 2016, 12, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Sosa Henriquez, M.; Gómez de Tejada Romero, M.J. Cholecalciferol or Calcifediol in the Management of Vitamin D Deficiency. Nutrients 2020, 12, 1617. [Google Scholar] [CrossRef]
- Pludowski, P.; Karczmarewicz, E.; Bayer, M.; Carter, G.; Chlebna-Sokół, D.; Czech-Kowalska, J.; Dębski, R.; Decsi, T.; Dobrzańska, A.; Franek, E.; et al. Practical guidelines for the supplementation of vitamin D and the treatment of deficits in Central Europe—recommended vitamin D intakes in the general population and groups at risk of vitamin D deficiency. Endokrynol. Pol. 2013, 64, 319–327. [Google Scholar] [CrossRef]
- Reichelt, A.C.; Rank, M.M. The impact of junk foods on the adolescent brain. Birth Defects Res. 2017, 109, 1649–1658. [Google Scholar] [CrossRef]
- Zahedi, H.; Kelishadi, R.; Heshmat, R.; Motlagh, M.E.; Ranjbar, S.H.; Ardalan, G.; Payab, M.; Chinian, M.; Asayesh, H.; Larijani, B.; et al. Association between junk food consumption and mental health in a national sample of Iranian children and adolescents: The CASPIAN-IV study. Nutrition 2014, 30, 1391–1397. [Google Scholar] [CrossRef]
- Chapman, D.J.; Nommsen-Rivers, L. Impact of maternal nutritional status on human milk quality and infant outcomes: An update on key nutrients. Adv. Nutr. 2012, 3, 351–352. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bravi, F.; Wiens, F.; Decarli, A.; Dal Pont, A.; Agostoni, C.; Ferraroni, M. Impact of maternal nutrition on breast-milk composition: A systematic review. Am. J. Clin. Nutr. 2016, 104, 646–662. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jeurink, P.V.; Knipping, K.; Wiens, F.; Barańska, K.; Stahl, B.; Garssen, J.; Krolak-Olejnik, B. Importance of maternal diet in the training of the infant’s immune system during gestation and lactation. Crit. Rev. Food Sci. Nutr. 2019, 59, 1311–1319. [Google Scholar] [CrossRef] [PubMed]
- Rasmussen, K.M. At long last: New information on the association between maternal dietary intake, the composition of human milk, and its nutrient adequacy for infants. Am. J. Clin. Nutr. 2019, 110, 269–270. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| NPNL (n = 957) | Pregnant (n = 437) | Lactating (n = 473) | p-Value | |
|---|---|---|---|---|
| Maternal age (years) | 27.0 [22.0; 34.0] a | 32.0 [29.0; 35.0] b | 34.0 [30.0; 37.0] c | <0.001 |
| Origin | ||||
| Spanish | 91.8% (879) | 89.0% (389) | 85.6% (405) | 0.001 |
| No Spanish | 8.2% (78) | 11.0% (48) | 14.4% (68) | |
| Educational level | ||||
| Middle school or lower | 5.8% (55) | 7.8% (74) | 11.6% (55) | <0.001 |
| High school | 32.8% (314) | 16.9% (74) | 18.4% (87) | |
| University degree | 61.4% (588) | 75.3% (329) | 70.0% (331) | |
| Financial income | ||||
| ≤1000€ | 47.9% (458) | 24.9% (109) | 29.2% (138) | <0.001 |
| 1001–2500€ | 46.5% (445) | 64.5% (278) | 58.6% (277) | |
| 2501–4000€ | 4.8% (46) | 9.2% (40) | 11.0% (52) | |
| ≥4001€ | 0.8% (8) | 1.4% (6) | 1.3% (6) | |
| Employment status | ||||
| Working | 55.0% (526) | 38.7% (169) | 40.0% (189) | <0.001 |
| Studying | 32.4% (310) | 4.4% (19) | 2.8% (13) | |
| Unemployed | 7.7% (74) | 11.7% (51) | 17.1% (81) | |
| Other situations | 4.9% (47) | 45.3% (198) | 40.2% (190) | |
| Comorbidities | 23.5% (225) a | 19.2% (84) b | 17.8% (84) b | 0.024 |
| NPNL (n = 957) | Pregnant (n = 437) | Lactating (n = 473) | p-Value | |
|---|---|---|---|---|
| Physical activity | 0.58 [0.31; 0.87] a | 0.48 [0.24; 0.76] b | 0.40 [0.19; 0.67] c | <0.001 |
| Healthy habits | 0.64 [0.49;0.75] a | 0.68 [0.54;0.76] b | 0.61 [0.48;0.70] c | <0.001 |
| Lifestyle | 0.80 [0.00; 1.00] a | 1.00 [0.60; 1.00] b | 1.00 [0.60; 1.00] b | <0.001 |
| Emotional balance | 0.67 [0.50; 0.80] a | 0.73 [0.60; 0.83] b | 0.70 [0.50; 0.83] b | <0.001 |
| Sleep hygiene | 0.69 [0.46; 0.77] a | 0.54 [0.38; 0.69] b | 0.38 [0.23; 0.54] c | <0.001 |
| Culinary techniques | 0.64 [0.50; 0.79] a | 0.71 [0.50; 0.86] b | 0.64 [0.50; 0.79] a | 0.021 |
| Hydration | 0.73 [0.56; 0.91] a | 0.80 [0.66; 0.96] b | 0.76 [0.64; 0.96] b | <0.001 |
| Water intake | 1.00 [0.80; 1.00] | 1.00 [0.80; 1.00] | 1.00 [0.80; 1.00] | 0.28 |
| Soft drinks | −0.11 [−0.78; −0.11] | −0.11 [−0.62; −0.11] | −0.11 [−0.82; −0.11] | 0.30 |
| Wine & beers | 0.0 [0.0; 0.0] | 0.0 [0.0; 0.0] | 0.0 [0.0; 0.0] | 0.07 |
| Distilled beverages | −0.17 [−0.17; 0.0] a | 0.0 [0.0; 0.0] b | 0.0 [0.0; 0.0] b | <0.001 |
| NPNL (n = 957) | Pregnant (n = 437) | Lactating (n = 473) | p-Value | |
|---|---|---|---|---|
| Grains, seed, and legumes | 0.58 [0.36; 0.78] | 0.60 [0.36; 0.79] | 0.59 [0.35; 0.79] | 0.62 |
| Fruits | 0.80 [0.40; 1.00] a | 1.00 [0.80; 1.00] b | 0.80 [0.40; 1.00] a | <0.001 |
| Vegetables | 0.56 [0.47; 0.64] a | 0.56 [0.47; 0.64] a | 0.58 [0.50; 0.64] b | 0.018 |
| Oil type | 0.92 [0.67; 1.00] | 1.00 [0.67; 1.00] | 0.83 [0.58; 1.00] | 0.20 |
| Dairy products | 0.37 [0.33; 0.43] a | 0.39 [0.33; 0.43] b | 0.37 [0.33; 0.41] a | 0.005 |
| Animal proteins | 0.54 [0.42; 0.62] | 0.54 [0.46; 0.62] | 0.54 [0.42; 0.62] | 0.06 |
| Snacks | 0.72 [0.62; 0.80] a | 0.67 [0.62; 0.77] b | 0.70 [0.62; 0.77] b | 0.002 |
| Pregnant Women | Lactating Women | |||
|---|---|---|---|---|
| β ± SE | p-Value | β ± SE | p-Value | |
| AP-Q score | 0.26 ± 0.07 | 0.001 | −0.02 ± 0.06 | 0.80 |
| Physical activity | −0.03 ± 0.02 | 0.13 | −0.11 ± 0.02 | <0.001 |
| Healthy habits | 0.07 ± 0.01 | <0.001 | 0.0 ± 0.0 | 0.85 |
| Hydration | 0.07 ± 0.02 | <0.001 | 0.04 ± 0.01 | 0.005 |
| Fruits | 0.11 ± 0.02 | <0.001 | 0.04 ± 0.02 | 0.027 |
| Vegetables | 0.0 ± 0.01 | 0.89 | 0.02 ± 0.01 | 0.015 |
| Dairy products | 0.0 ± 0.0 | 0.18 | 0.0 ± 0.0 | 0.19 |
| Snacks | −0.02 ± 0.01 | 0.028 | −0.01 ± 0.01 | 0.027 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gila-Díaz, A.; Witte Castro, A.; Herranz Carrillo, G.; Singh, P.; Yakah, W.; Arribas, S.M.; Ramiro-Cortijo, D. Assessment of Adherence to the Healthy Food Pyramid in Pregnant and Lactating Women. Nutrients 2021, 13, 2372. https://doi.org/10.3390/nu13072372
Gila-Díaz A, Witte Castro A, Herranz Carrillo G, Singh P, Yakah W, Arribas SM, Ramiro-Cortijo D. Assessment of Adherence to the Healthy Food Pyramid in Pregnant and Lactating Women. Nutrients. 2021; 13(7):2372. https://doi.org/10.3390/nu13072372
Chicago/Turabian StyleGila-Díaz, Andrea, Ariadna Witte Castro, Gloria Herranz Carrillo, Pratibha Singh, William Yakah, Silvia M. Arribas, and David Ramiro-Cortijo. 2021. "Assessment of Adherence to the Healthy Food Pyramid in Pregnant and Lactating Women" Nutrients 13, no. 7: 2372. https://doi.org/10.3390/nu13072372