
Effect of Dietary Supplementation with a Natural Extract of Sclerocarya birrea on Glycemic Metabolism in Subjects with Prediabetes: A Randomized Double-Blind Placebo-Controlled Study

 ,
,  ,
,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
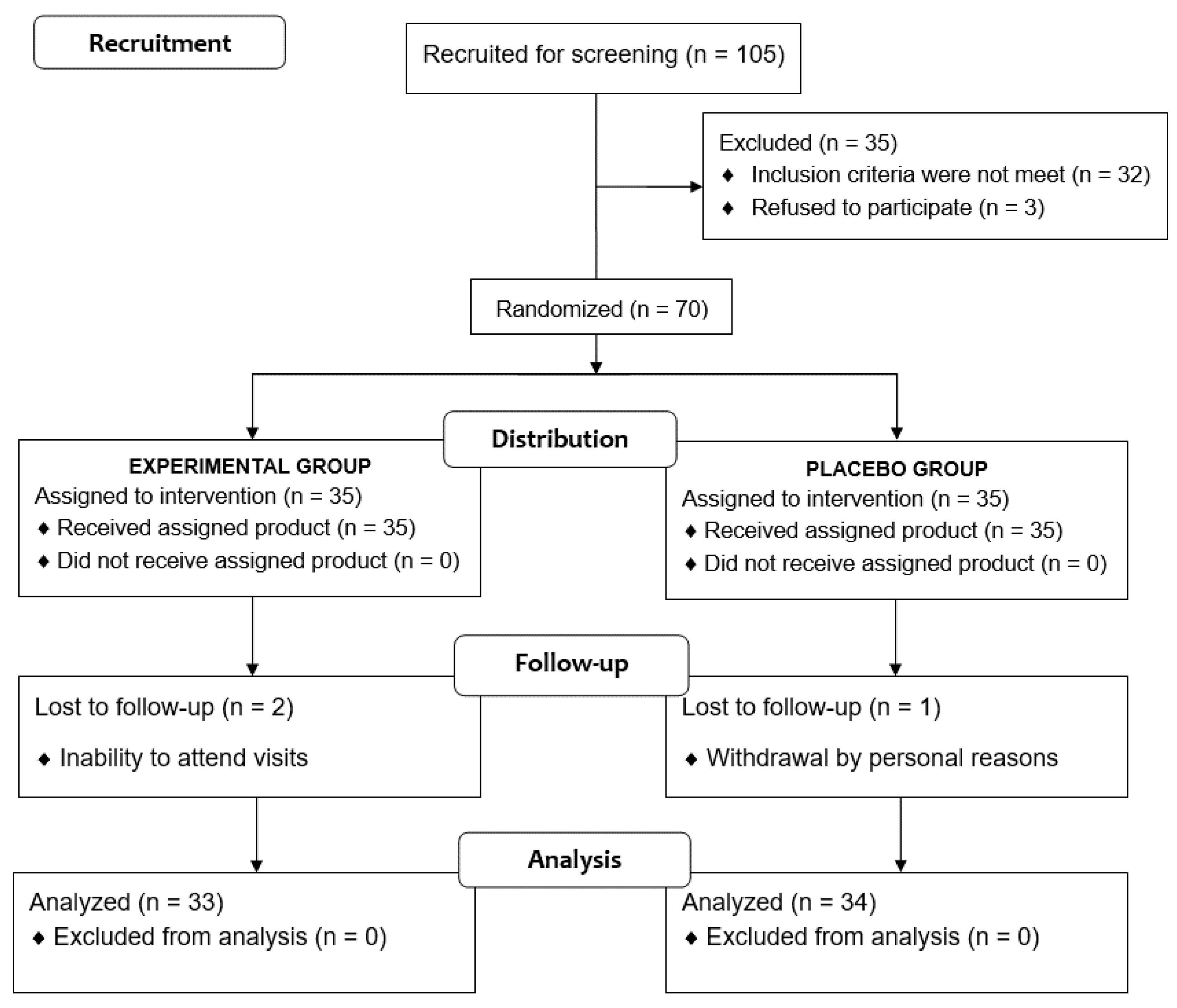
2.1. Study Design and Participants
2.2. Intervention and Study Procedures
2.3. Study Variables
2.4. Statistical Analysis
3. Results
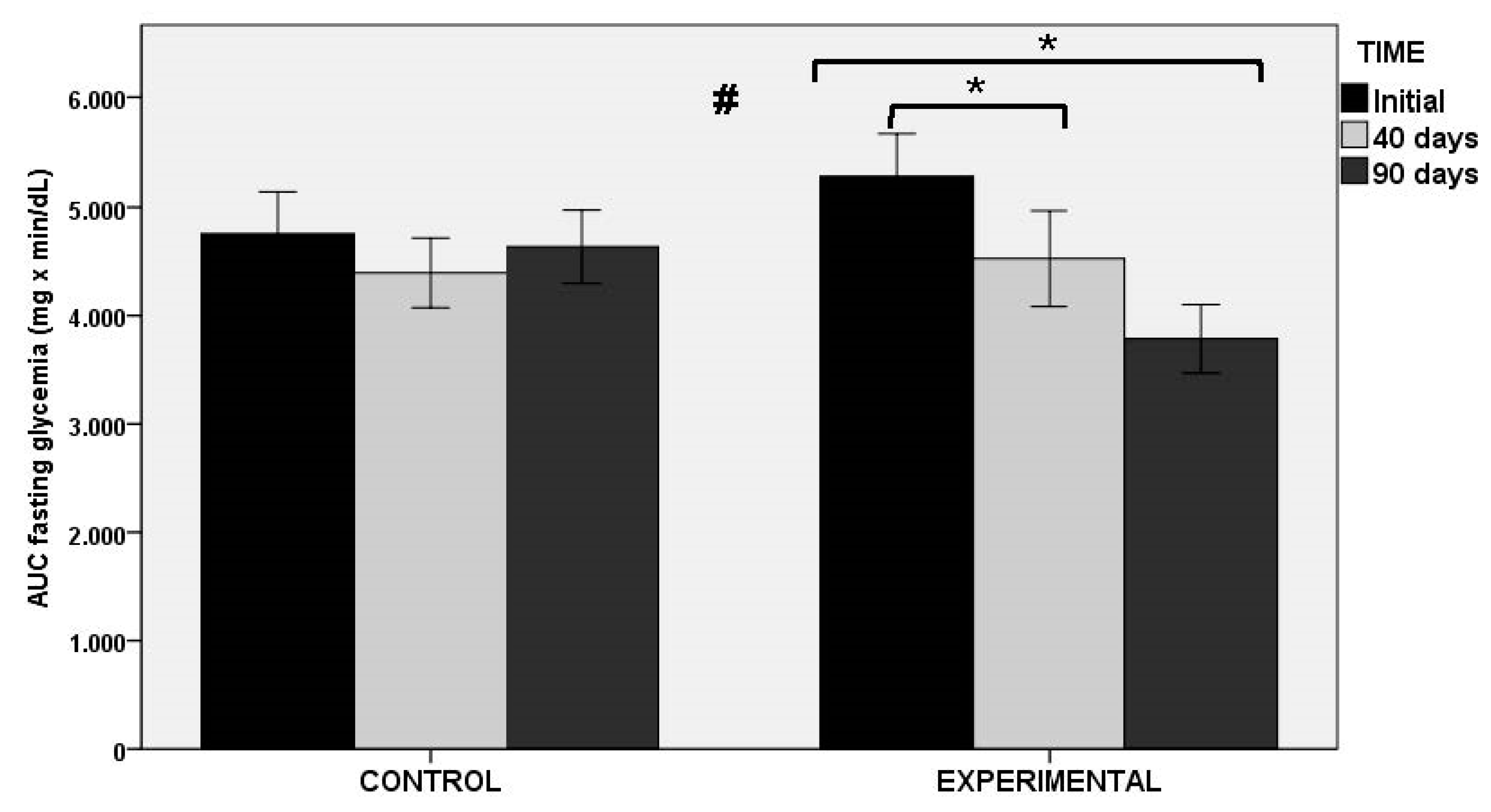
3.1. Glucose Metabolism
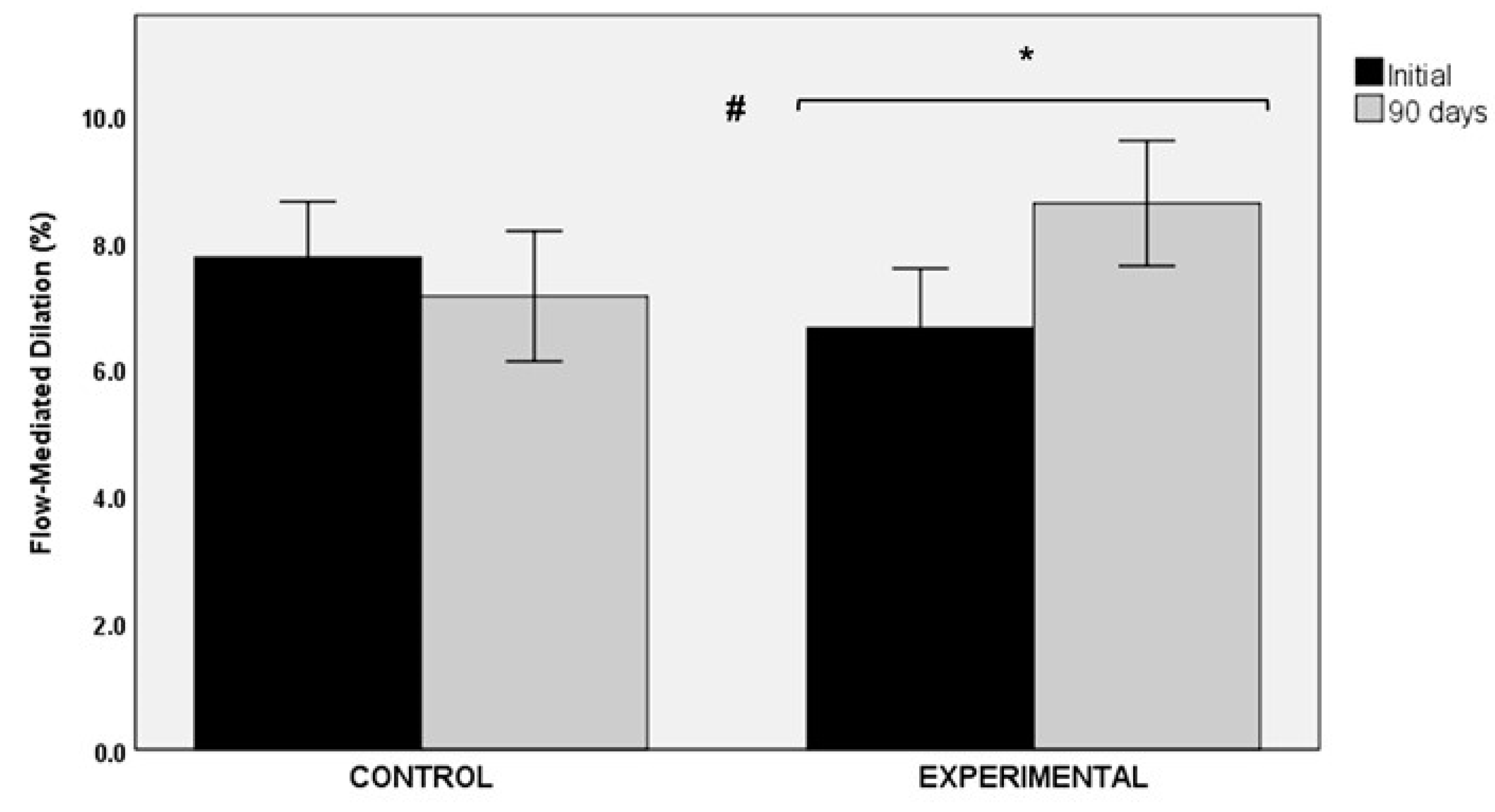
3.2. Flow-Mediated Dilation
3.3. Lipid Profile
3.4. Anthropometric Variables
3.5. Inflammatory Biomarkers
3.6. Blood Pressure
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- American Diabetes Association. Prediabetes. Diagnosis. Available online: https://www.diabetes.org/a1c/diagnosis (accessed on 30 April 2021).
- World Health Organization. Definition and Diagnosis of Diabetes Mellitus and Intermediate Hyperglycemia: Report of a WHO/IDF Consultation; World Health Organization: Geneva, Switzerland, 2006; pp. 1–50. [Google Scholar]
- Tabak, A.G.; Herder, C.; Rathmann, W.; Brunner, E.J.; Kivimaki, M. Prediabetes: A high-risk state for diabetes development. Lancet 2012, 379, 2279–2290. [Google Scholar] [CrossRef] [Green Version]
- Huang, D.; Refaat, M.; Mohammedi, K.; Jayyousi, A.; Al Suwaidi, J.; Abi Khalil, C. Macrovascular complications in patients with diabetes and prediabetes. Biomed Res. Int. 2017, 2017, 7839101. [Google Scholar] [CrossRef]
- Brannick, B.; Wynn, A.; Dagogo-Jack, S. Prediabetes as a toxic environment for the initiation of microvascular and macrovascular complications. Exp. Biol. Med. (Maywood) 2016, 241, 1323–1331. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- International Diabetes Federation. IDF Diabetes Atlas. Ninth Edition. 2019. Available online: www.diabetes.atlas.org (accessed on 30 April 2021).
- Hostalek, U. Global epidemiology of prediabetes—Present and future perspectives. Clin. Diabetes Endocrinol. 2019, 5, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luc, K.; Schramm-Luc, A.; Guzik, T.J.; Mikolajczyk, T.P. Oxidative stress and inflammatory markers in prediabetes and diabetes. J. Physiol. Pharmacol. 2019, 70, 70. [Google Scholar] [CrossRef]
- Alam, F.; Islam, M.A.; Khalil, M.I.; Gan, S.H. Metabolic control of type 2 diabetes by targeting the GLUT4 glucose transporter: Intervention approaches. Curr Pharm Des. 2016, 22, 3034–3049. [Google Scholar] [CrossRef] [PubMed]
- Huang, X.; Liu, G.; Guo, J.; Su, Z. The PI3K/AKT pathway in obesity and type 2 diabetes. Int. J. Biol. Sci. 2018, 14, 1483–1496. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaneto, H.; Nakatani, Y.; Kawamori, D.; Miyatsuka, T.; Matsuoka, T.A.; Matsuhisa, M.; Yamasaki, Y. Role of oxidative stress, endoplasmic reticulum stress, and c-Jun N-terminal kinase in pancreatic beta-cell dysfunction and insulin resistance. Int. J. Biochem. Cell Biol. 2005, 37, 1595–1608. [Google Scholar] [CrossRef] [PubMed]
- Mayans, L. Metabolic syndrome: Insulin resistance and prediabetes. FP Essent. 2015, 435, 11–16. [Google Scholar] [PubMed]
- Tuomilehto, J.; Lindström, J.; Eriksson, J.G.; Valle, T.T.; Hämäläinen, H.; Ilanne-Parikka, P.; Keinänen-Kiukaanniemi, S.; Laakso, M.; Louheranta, A.; Rastas, M.; et al. Finnish Diabetes Prevention Study Group. Prevention of type 2 diabetes mellitus by changes in lifestyle among subjects with impaired glucose tolerance. N. Engl. J. Med. 2001, 344, 1343–1350. [Google Scholar] [CrossRef] [PubMed]
- Hamman, R.F.; Wing, R.R.; Edelstein, S.L.; Lachin, J.M.; Bray, G.A.; Delahanty, L.; Hoskin, M.; Kriska, A.M.; Mayer-Davis, E.J.; Pi-Sunyer, X.; et al. Effect of weight loss with lifestyle intervention on risk of diabetes. Diabetes Care 2006, 29, 2102–2107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Derosa, G.; Limas, C.P.; Macías, P.C.; Estrella, A.; Maffioli, P. Dietary and nutraceutical approach to type 2 diabetes. Arch. Med. Sci. 2014, 10, 336–344. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Onaolapo, A.Y.; Onaolapo, O.J. Nutraceuticals and diet-based phytochemicals in type 2 diabetes mellitus: From whole food to components with defined roles and mechanisms. Curr. Diabetes Rev. 2019, 16, 12–25. [Google Scholar] [CrossRef] [PubMed]
- Mariod, A.A.; Abdelwahab, S.I. Sclerocarya birrea (Marula), an African tree of nutritional and medicinal uses: A review. Food Rev. Int. 2012, 28, 375–388. [Google Scholar] [CrossRef]
- Mousinho, N.M.; van Tonder, J.J.; Steenkamp, V. In vitro anti-diabetic activity of Sclerocarya birrea and Ziziphus mucronata. Nat. Prod. Commun. 2013, 8, 1279–1284. [Google Scholar]
- Ojewole, J.A. Hypoglycemic effect of Sclerocarya birrea [(A. Rich.) Hochst.] [Anacardiaceae] stem-bark aqueous extract in rats. Phytomedicine 2003, 10, 675–681. [Google Scholar] [CrossRef]
- Dimo, T.; Rakotonirina, S.V.; Tan, P.V.; Azay, J.; Dongo, E.; Kamtchouing, P.; Cros, G. Effect of Sclerocarya birrea (Anacardiaceae) stem bark methylene chloride/methanol extract on streptozotocin-diabetic rats. J. Ethnopharmacol. 2007, 110, 434–438. [Google Scholar] [CrossRef]
- Gondwe, M.; Kamadyaapa, D.R.; Tufts, M.; Chuturgoon, A.A.; Musabayane, C.T. Sclerocarya birrea [(A. Rich.) Hochst.] [Anacardiaceae] stem-bark ethanolic extract (SBE) modulates blood glucose, glomerular filtration rate (GFR) and mean arterial blood pressure (MAP) of STZ-induced diabetic rats. Phytomedicine 2008, 15, 699–709. [Google Scholar] [CrossRef] [PubMed]
- Tsabang, N.; Ngah, N.; Estella, F.T.; Agbor, G.A. Herbal Medicine and Treatment of Diabetes in Africa: Case Study in Cameroon. Diabetes Case Reports 2017, 1, 1000112. [Google Scholar] [CrossRef]
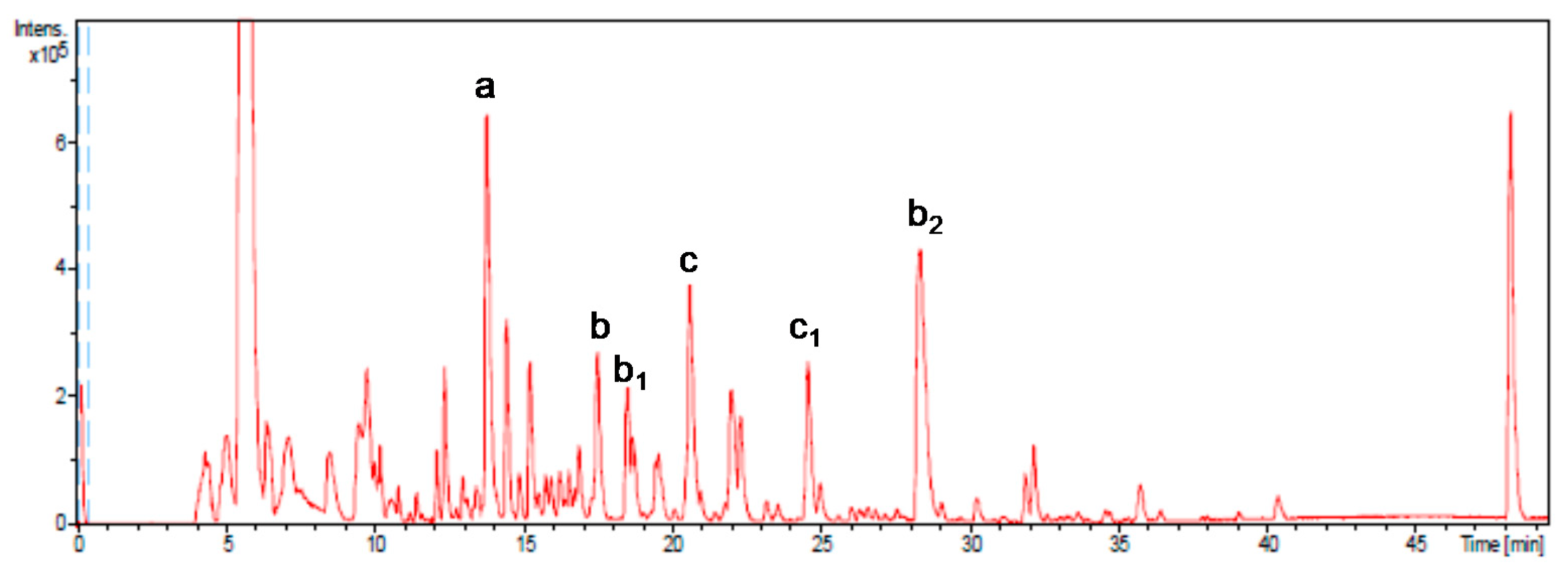
- Jiménez-Sánchez, C.; Lozano-Sánchez, J.; Gabaldón-Hernández, J.A.; Segura-Carretero, A.; Fernández-Gutiérrez, A. RP-HPLC-ESI-QTOF/MS2 based strategy for the comprehensive metabolite profiling of Sclerocarya birrea (marula) bark. Ind. Crops Prod. 2015, 71, 214–234. [Google Scholar] [CrossRef]
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; de Simone, G.; Dominiczak, A.; et al. ESC Scientific Document Group. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur. Heart J. 2018, 39, 3021–3104. [Google Scholar] [CrossRef] [PubMed]
- Corretti, M.C.; Anderson, T.J.; Benjamin, E.J.; Celermajer, D.; Charbonneau, F.; Creager, M.A.; Deanfield, J.; Drexler, H.; Gerhard-Herman, M.; Herrington, D.; et al. International Brachial Artery Reactivity Task Force. Guidelines for the ultrasound assessment of endothelial-dependent flow-mediated vasodilation of the brachial artery: A report of the International Brachial Artery Reactivity Task Force. J. Am. Coll. Cardiol. 2002, 39, 257–265. [Google Scholar] [CrossRef] [Green Version]
- Armstrong, F.; Bull, F. Development of the World Health Organization Global Physical Activity Questionnaire (GPAQ). J. Public Health 2006, 14, 66–70. [Google Scholar] [CrossRef]
- Ahn, H.Y.; Kim, M.; Seo, C.R.; Yoo, H.J.; Lee, S.H.; Lee, J.H. The effects of Jerusalem artichoke and fermented soybean powder mixture supplementation on blood glucose and oxidative stress in subjects with prediabetes or newly diagnosed type 2 diabetes. Nutr. Diabetes 2018, 8, 42. [Google Scholar] [CrossRef] [PubMed]
- Movahed, A.; Raj, P.; Nabipour, I.; Mahmoodi, M.; Ostovar, A.; Kalantarhormozi, M.; Netticadan, T. Efficacy and Safety of Resveratrol in Type 1 Diabetes Patients: A Two-Month Preliminary Exploratory Trial. Nutrients 2020, 12, 161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ngueguim, F.T.; Esse, E.C.; Dzeufiet, P.D.; Gounoue, R.K.; Bilanda, D.C.; Kamtchouing, P.; Dimo, T. Oxidised palm oil and sucrose induced hyperglycemia in normal rats: Effects of Sclerocarya birrea stem barks aqueous extract. BMC Complement. Altern. Med. 2016, 16, 47. [Google Scholar] [CrossRef] [Green Version]
- Makom Ndifossap, I.G.; Frigerio, F.; Casimir, M.; Ngueguim Tsofack, F.; Dongo, E.; Kamtchouing, P.; Dimo, T.; Maechler, P. Sclerocarya birrea (Anacardiaceae) stem-bark extract corrects glycaemia in diabetic rats and acts on beta-cells by enhancing glucose-stimulated insulin secretion. J. Endocrinol. 2010, 205, 79–86. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ojewole, J.A. Vasorelaxant and hypotensive effects of Sclerocarya birrea (A Rich) Hochst (Anacardiaceae) stem bark aqueous extract in rats. Cardiovasc. J. South Afr. 2006, 17, 117–123. [Google Scholar]
- Belemtougri, R.G.; Dzamitika, S.A.; Oudraogo, Y.; Sawadogo, L. Effects of water crude leaf extract of Sclerocarya birrea (A. Rich) Hochts (Anacardiacea) on normotensive rat blood pressure. J. Biol. Sci. 2007, 7, 570–574. [Google Scholar] [CrossRef] [Green Version]
- Ojewole, J.A. Evaluation of the analgesic, anti-inflammatory and anti-diabetic properties of Sclerocarya birrea (A. Rich.) Hochst. stem-bark aqueous extract in mice and rats. Phytother. Res. 2004, 18, 601–608. [Google Scholar] [CrossRef]
- Fotio, A.L.; Dimo, T.; Nguelefack, T.B.; Dzeufiet, P.D.; Ngo Lemba, E.; Temdie, R.J.; Ngueguim, F.; Olleros, M.L.; Vesin, D.; Dongo, E.; et al. Acute and chronic anti-inflammatory properties of the stem bark aqueous and methanol extracts of Sclerocarya birrea (Anacardiaceae). Inflammopharmacology 2009, 17, 229–237. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Control Group (n = 33) | Experimental Group (n = 34) |
|---|---|---|
| Gender | ||
| Men | 17 | 19 |
| Women | 16 | 15 |
| Age, years, mean ± SD | 31.5 ± 15.2 | 33.1 ± 13.2 |
| Physical activity, % | ||
| 1 (inactive) | 29.4 | 33.3 |
| 2 (moderately inactive) | 17.6 | 15.2 |
| 3 (moderately active) | 29.4 | 24.2 |
| 4 (very active) | 23.5 | 27.3 |
| Variables | Pre-Intervention | Intervention Period | Significant Differences | ||
|---|---|---|---|---|---|
| Baseline | 40 Days | 90 Days | Within-Group p Value | Between-Group p Value | |
| AUC of OGTT, mg·min/dL (at fasting serum glucose) | |||||
| Control group (n = 34) | 4755 ± 2265 | 4394 ± 1879 | 4636 ± 1969 | 1.0 | <0.004 |
| Experimental group (n = 33) | 5286 ± 2260 | 4526 ± 2543 | 3786 ± 1817 | <0.001 | |
| AUC of OGTT, mg·min/dL (at 0 mg/dL) | |||||
| Control group (n = 34) | 17,401 ± 2284 | 16,892 ± 1933 | 17,229 ± 2152 | 1.0 | <0.002 |
| Experimental group (n = 33) | 17,809 ± 2534 | 16,908 ± 2825 | 16,219 ± 2176 | <0.001 | |
| Glucose peak at OGTT, mg/dL | |||||
| Control group (n = 34) | 179 ± 29 | 174 ± 25 | 175 ± 22 | 1.0 | <0.011 |
| Experimental group (n = 33) | 181 ± 34 | 170 ± 32 | 161 ± 28 | <0.001 | |
| HbA1c, % | |||||
| Control group (n = 34) | 5.22 ± 0.36 | 5.23 ± 0.40 | 5.22 ± 0.37 | 1.0 | 0.469 |
| Experimental group (n = 33) | 5.33 ± 0.44 | 5.35 ± 0.42 | 5.24 ± 0.43 | 0.543 | |
| Fasting serum glucose, mg/dL | |||||
| Control group (n = 34) | 103.4 ± 3.0 | 102.6 ± 4.9 | 103.6 ± 5.4 | 1.0 | 0.107 |
| Experimental group (n = 33) | 104.2 ± 5.0 | 104.3 ± 5.9 | 102.9 ± 5.3 | 0.329 | |
| Fasting serum insulin, mU/L | |||||
| Control group (n = 34) | 9.36 ± 6.55 | 10.80 ± 8.09 | 10.16 ± 6.18 | 1.0 | <0.027 |
| Experimental group (n = 33) | 9.78 ± 6.82 | 7.70 ± 5.07 | 8.11 ± 4.46 | 0.148 | |
| HOMA-IR | |||||
| Control group (n = 34) | 2.40 ± 1.70 | 2.76 ± 2.13 | 2.61 ± 1.62 | 1.0 | <0.034 |
| Experimental group (n = 33) | 2.54 ± 1.80 | 2.01 ± 1.38 | 2.08 ± 1.20 | 0.313 | |
| QUICKI index | |||||
| Control group (n = 34) | 0.35 ± 0.03 | 0.34 ± 0.03 | 0.34 ± 0.03 | 0.632 | <0.034 |
| Experimental group (n = 33) | 0.35 ± 0.03 | 0.36 ± 0.03 | 0.35 ± 0.03 | 0.07 | |
| HOMA-β1 | |||||
| Control group (n = 34) | 83.29 ± 55.81 | 98.49 ± 73.12 | 89.82 ± 50.68 | 1.0 | <0.027 |
| Experimental group (n = 33) | 89.41 ± 65.51 | 70.94 ± 42.30 | 75.47 ± 39.21 | 0.438 | |
| Insulin/glucose ratio | |||||
| Control group (n = 34) | 0.09 ± 0.06 | 0.10 ± 0.08 | 0.10 ± 0.06 | 1.0 | <0.022 |
| Experimental group (n = 33) | 0.09 ± 0.07 | 0.07 ± 0.05 | 0.08 ± 0.04 | 0.280 | |
| 1 h post-OGTT glucose, mg/dL | |||||
| Control group (n = 34) | 161.09 ± 36.07 | 155.71 ± 27.56 | 155.00 ± 29.50 | 0.798 | 0.081 |
| Experimental group (n = 33) | 168.52 ± 39.10 | 154.03 ± 39.42 | 156.91 ± 31.11 | <0.001 | |
| 2 h post-OGTT glucose, mg/dL | |||||
| Control group (n = 34) | 121.35 ± 23.86 | 119.53 ± 20.90 | 124.00 ± 23.38 | 1.0 | <0.050 |
| Experimental group (n = 33) | 125.79 ± 23.27 | 121.09 ± 22.01 | 117.12 ± 20.55 | <0.028 | |
| Variables | Pre-Intervention | Intervention Period | Significant Differences | ||
|---|---|---|---|---|---|
| Baseline | 40 Days | 90 Days | Within-Group p Value | Between-Group p Value | |
| Serum cholesterol, mg/dL | |||||
| Control group (n = 34) | 194 ± 34 | 192 ± 36 | 198 ± 41 | 1.0 | 0.641 |
| Experimental group (n = 33) | 191 ± 36 | 187 ± 38 | 189 ± 38 | 1.0 | |
| LDL-C, mg/dL | |||||
| Control group (n = 34) | 113.4 ± 25.2 | 114.8 ± 33.7 | 118.1 ± 28.1 | 0.610 | 0.662 |
| Experimental group (n = 33) | 102.8 ± 27.2 | 108.1 ± 30.7 | 111.4 ± 34.6 | 0.851 | |
| HDL-C, mg/dL | |||||
| Control group (n = 34) | 60.1 ± 15.1 | 59.0 ± 15.3 | 58.1 ± 13.2 | 0.252 | 0.639 |
| Experimental group (n = 33) | 59.9 ± 12.1 | 58.3 ± 12.1 | 59.1 ± 10.8 | 1.0 | |
| Serum triglycerides, mg/dL | |||||
| Control group (n = 34) | 94 ± 57 | 99 ± 61 | 99 ± 54 | 1.0 | 0.101 |
| Experimental group (n = 33) | 98 ± 54 | 87 ± 48 | 89 ± 42 | 0.531 | |
| Variables | Pre-Intervention | Intervention Period | Significant Differences | ||
|---|---|---|---|---|---|
| Baseline | 40 Days | 90 Days | Within-Group p Value | Between-Group p Value | |
| Body weight, kg | |||||
| Control group (n = 34) | 75.2 ± 18.2 | 75.2 ± 18.1 | 75.2 ± 17.9 | 1.0 | 0.469 |
| Experimental group (n = 33) | 75.2 ± 18.3 | 74.9 ± 18.3 | 74.7 ± 18.3 | 0.543 | |
| Body mass index (BMI), kg/m2 | |||||
| Control group (n = 34) | 26.1 ± 5.3 | 26.1 ± 5.2 | 26.1 ± 5.2 | 1.0 | 0.261 |
| Experimental group (n = 33) | 25.9 ± 6.9 | 25.9 ± 6.9 | 25.8 ± 7.0 | 0.304 | |
| Fat mass, % | |||||
| Control group (n = 34) | 25.4 ± 9.3 | 25.3 ± 9.3 | 25.4 ± 9.0 | 1.0 | 0.890 |
| Experimental group (n = 33) | 29.1 ± 10.4 | 29.1 ± 10.6 | 29.3 ± 10.4 | 1.0 | |
| Waist-to-hip ratio | |||||
| Control group (n = 34) | 0.79 ± 0.09 | 0.79 ± 0.10 | 0.79 ± 0.10 | 1.0 | 0.928 |
| Experimental group (n = 33) | 0.79 ± 0.10 | 0.78 ± 0.10 | 0.79 ± 0.10 | 1.0 | |
| Variables | Pre-Intervention | Intervention Period | Significant Differences | ||
|---|---|---|---|---|---|
| Baseline | 40 Days | 90 Days | Within-Group p Value | Between-Group p Value | |
| IL-6, pg/mL | |||||
| Control group (n = 34) | 4.37 ± 1.37 | 4.43 ± 1.25 | 4.36 ± 1.41 | 1.0 | 0.284 |
| Experimental group (n = 33) | 4.34 ± 1.79 | 4.17 ± 1.71 | 4.08 ± 1.41 | 0.159 | |
| E-selectin, ng/mL | |||||
| Control group (n = 34) | 16.62 ± 1.53 | 16.59 ± 1.45 | 16.23 ± 0.96 | 0.878 | 0.001 |
| Experimental group (n = 33) | 17.59 ± 1.11 | 16.52 ± 0.99 | 15.70 ± 1.06 | 0.001 | |
| Blood pressure (BP) | |||||
| Systolic BP, mmHg | |||||
| Control group (n = 34) | 120 ± 18 | 119 ± 17 | 120 ± 16 | 1.0 | 0.259 |
| Experimental group (n = 33) | 125 ± 18 | 122 ± 18 | 119 ± 17 | 0.001 | |
| Diastolic BP, mmHg | |||||
| Control group (n = 34) | 76 ± 11 | 78 ± 10 | 76 ± 9 | 1.0 | 0.132 |
| Experimental group (n = 33) | 78 ± 10 | 76 ± 11 | 76 ± 12 | 0.265 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Victoria-Montesinos, D.; Sánchez-Macarro, M.; Gabaldón-Hernández, J.A.; Abellán-Ruiz, M.S.; Querol-Calderón, M.; Luque-Rubia, A.J.; Bernal-Morell, E.; Ávila-Gandía, V.; López-Román, F.J. Effect of Dietary Supplementation with a Natural Extract of Sclerocarya birrea on Glycemic Metabolism in Subjects with Prediabetes: A Randomized Double-Blind Placebo-Controlled Study. Nutrients 2021, 13, 1948. https://doi.org/10.3390/nu13061948
Victoria-Montesinos D, Sánchez-Macarro M, Gabaldón-Hernández JA, Abellán-Ruiz MS, Querol-Calderón M, Luque-Rubia AJ, Bernal-Morell E, Ávila-Gandía V, López-Román FJ. Effect of Dietary Supplementation with a Natural Extract of Sclerocarya birrea on Glycemic Metabolism in Subjects with Prediabetes: A Randomized Double-Blind Placebo-Controlled Study. Nutrients. 2021; 13(6):1948. https://doi.org/10.3390/nu13061948
Chicago/Turabian StyleVictoria-Montesinos, Desirée, Maravillas Sánchez-Macarro, José Antonio Gabaldón-Hernández, María Salud Abellán-Ruiz, María Querol-Calderón, Antonio J. Luque-Rubia, Enrique Bernal-Morell, Vicente Ávila-Gandía, and Francisco Javier López-Román. 2021. "Effect of Dietary Supplementation with a Natural Extract of Sclerocarya birrea on Glycemic Metabolism in Subjects with Prediabetes: A Randomized Double-Blind Placebo-Controlled Study" Nutrients 13, no. 6: 1948. https://doi.org/10.3390/nu13061948