
Association between Mediterranean Dietary Pattern and Breakfast Quality with Physical Fitness in School Children: The HIIT Project

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Measurements
2.2.1. Body Composition
2.2.2. Mediterranean Dietary Pattern
2.2.3. Breakfast Quality
2.2.4. Physical Fitness
2.2.5. Physical Activity
2.3. Statistical Analyses
3. Results
4. Discussion
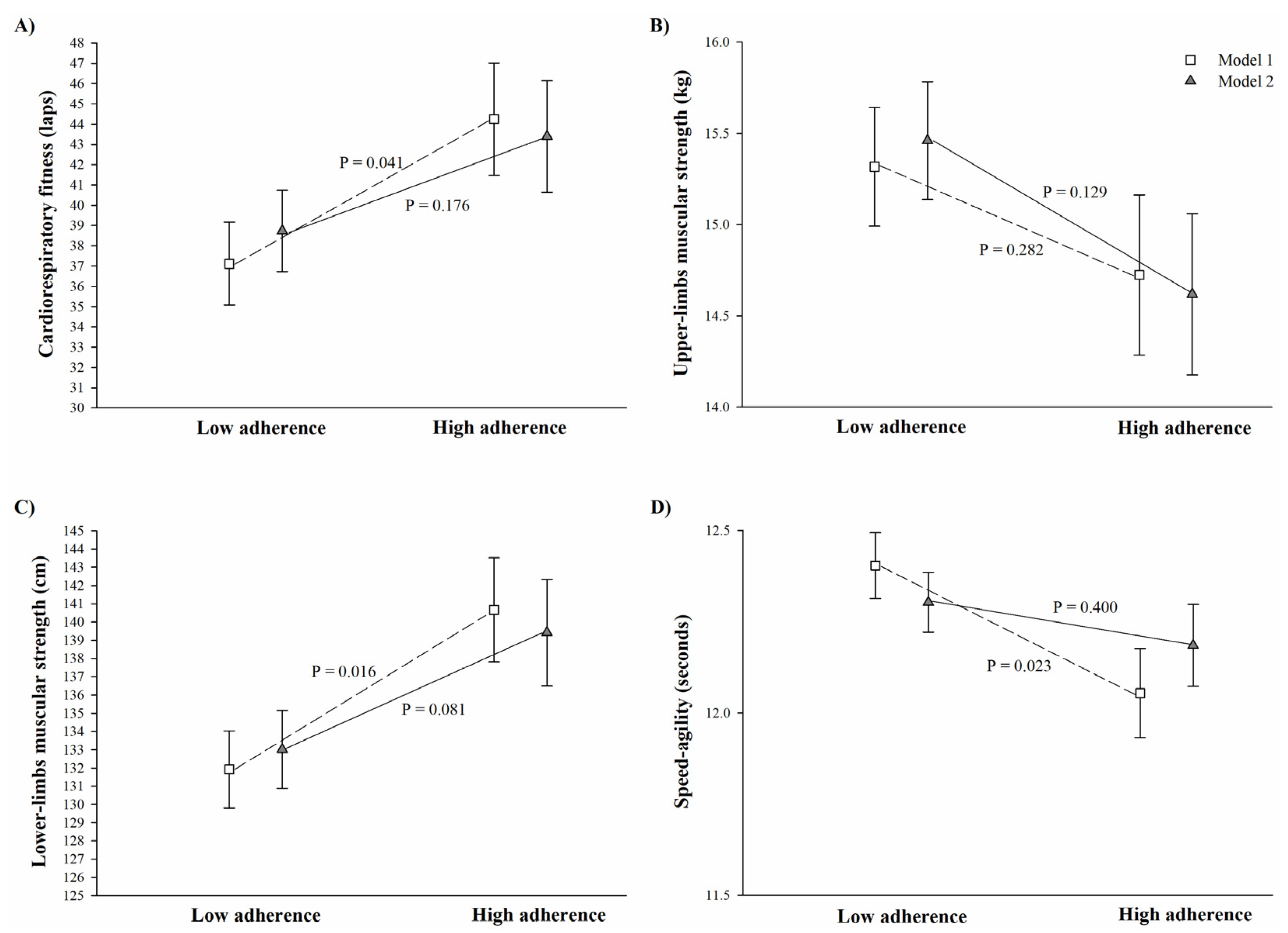
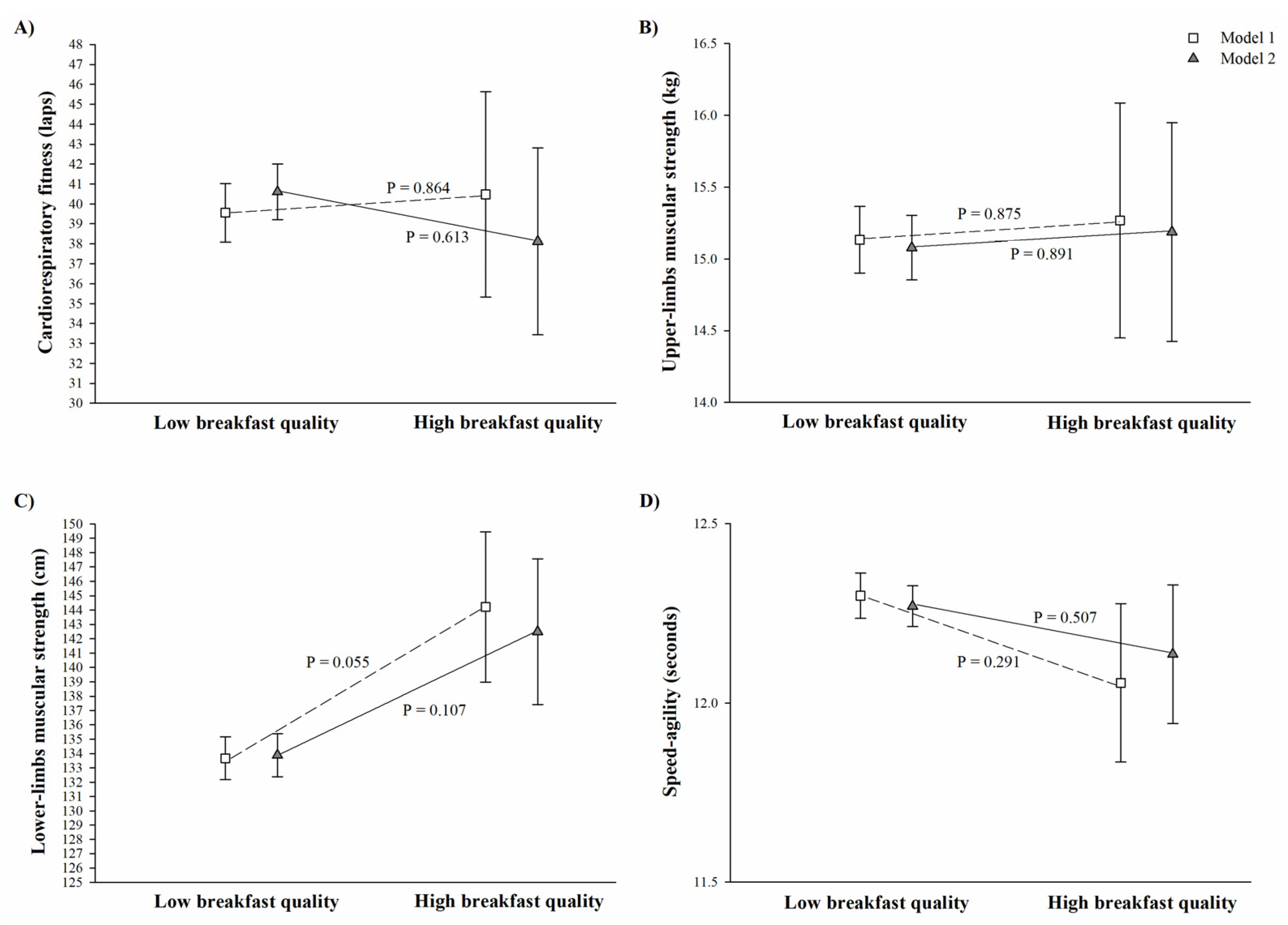
4.1. Mediterranean Dietary Pattern, Breakfast Quality, and Physical Fitness
4.2. Role of Physical Activity on the Association of Dietary Patterns with Physical Fitness
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Estruch, R.; Ros, E.; Salas-Salvadó, J.; Covas, M.-I.; Corella, D.; Arós, F.; Gómez-Gracia, E.; Ruiz-Gutiérrez, V.; Fiol, M.; Lapetra, J.; et al. Primary Prevention of Cardiovascular Disease with a Mediterranean Diet Supplemented with Extra-Virgin Olive Oil or Nuts. N. Engl. J. Med. 2018, 378, e34. [Google Scholar] [CrossRef]
- Dinu, M.; Pagliai, G.; Casini, A.; Sofi, F. Mediterranean diet and multiple health outcomes: An umbrella review of meta-analyses of observational studies and randomised trials. Eur. J. Clin. Nutr. 2018, 72, 30–43. [Google Scholar] [CrossRef] [PubMed]
- Sofi, F.; Cesari, F.; Abbate, R.; Gensini, G.F.; Casini, A. Adherence to Mediterranean diet and health status: Meta-analysis. BMJ 2008, 337. [Google Scholar] [CrossRef] [Green Version]
- Lydakis, C.; Stefanaki, E.; Stefanaki, S.; Thalassinos, E.; Kavousanaki, M.; Lydaki, D. Correlation of blood pressure, obesity, and adherence to the Mediterranean diet with indices of arterial stiffness in children. Eur. J. Pediatr. 2012, 171, 1373–1382. [Google Scholar] [CrossRef] [PubMed]
- Labayen Goñi, I.; Arenaza, L.; Medrano, M.; García, N.; Cadenas-Sanchez, C.; Ortega, F.B. Associations between the adherence to the Mediterranean diet and cardiorespiratory fitness with total and central obesity in preschool children: The PREFIT project. Eur. J. Nutr. 2018, 57, 2975–2983. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tognon, G.; Hebestreit, A.; Lanfer, A.; Moreno, L.A.; Pala, V.; Siani, A.; Tornaritis, M.; De Henauw, S.; Veidebaum, T.; Molnár, D.; et al. Mediterranean diet, overweight and body composition in children from eight European countries: Cross-sectional and prospective results from the IDEFICS study. Nutr. Metab. Cardiovasc. Dis. 2014, 24, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Rampersaud, G.C.; Pereira, M.A.; Girard, B.L.; Adams, J.; Metzl, J.D. Breakfast habits, nutritional status, body weight, and academic performance in children and adolescents. J. Am. Diet. Assoc. 2005, 105, 742–743. [Google Scholar] [CrossRef]
- Pereira, M.A.; Erickson, E.; McKee, P.; Schrankler, K.; Raatz, S.K.; Lytle, L.A.; Pellegrini, A.D. Breakfast frequency and quality may affect glycemia and appetite in adults and children. J. Nutr. 2011, 141, 163–168. [Google Scholar] [CrossRef] [Green Version]
- Arenaza, L.; Muñoz-Hernández, V.; Medrano, M.; Oses, M.; Amasene, M.; Merchán-Ramírez, E.; Cadenas-Sanchez, C.; Ortega, F.B.; Ruiz, J.R.; Labayen, I. Association of breakfast quality and energy density with cardiometabolic risk factors in overweight/obese children: Role of physical activity. Nutrients 2018, 10, 1066. [Google Scholar] [CrossRef] [Green Version]
- Raghuveer, G.; Hartz, J.; Lubans, D.R.; Takken, T.; Wiltz, J.L.; Mietus-Snyder, M.; Perak, A.M.; Baker-Smith, C.; Pietris, N.; Edwards, N.M.; et al. Cardiorespiratory Fitness in Youth: An Important Marker of Health: A Scientific Statement From the American Heart Association. Circulation 2020, 142, e101–e118. [Google Scholar] [CrossRef]
- Ortega, F.B.; Ruiz, J.R.; Castillo, M.J.; Sjöström, M. Physical fitness in childhood and adolescence: A powerful marker of health. Int. J. Obes. 2008, 32, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.-P.; Chastin, S.; Chou, R.; et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br. J. Sports Med. 2020, 54, 1451–1462. [Google Scholar] [CrossRef]
- Al-Jawaldeh, A.; Hammerich, A.; Doggui, R.; Engesveen, K.; Lang, K.; McColl, K. Implementation of WHO Recommended Policies and Interventions on Healthy Diet in the Countries of the Eastern Mediterranean Region: From Policy to Action. Nutrients 2020, 12, 3700. [Google Scholar] [CrossRef]
- Rosi, A.; Giopp, F.; Milioli, G.; Melegari, G.; Goldoni, M.; Parrino, L.; Scazzina, F. Weight Status, Adherence to the Mediterranean Diet, Physical Activity Level, and Sleep Behavior of Italian Junior High School Adolescents. Nutrients 2020, 12, 478. [Google Scholar] [CrossRef] [Green Version]
- García-Hermoso, A.; Ezzatvar, Y.; López-Gil, J.F.; Ramírez-Vélez, R.; Olloquequi, J.; Izquierdo, M. Is adherence to the Mediterranean diet associated with healthy habits and physical fitness? A systematic review and meta-analysis including 565 421 youths. Br. J. Nutr. 2020, 1–12. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.-G. Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cole, T.J.; Lobstein, T. Extended international (IOTF) body mass index cut-offs for thinness, overweight and obesity. Pediatr. Obes. 2012, 7, 284–294. [Google Scholar] [CrossRef] [PubMed]
- Serra-Majem, L.; Ribas, L.; Ngo, J.; Ortega, R.M.; García, A.; Pérez-Rodrigo, C.; Aranceta, J. Food, youth and the Mediterranean diet in Spain. Development of KIDMED, Mediterranean Diet Quality Index in children and adolescents. Public Health Nutr. 2004, 7, 931–935. [Google Scholar] [CrossRef]
- López, M.D.; Martín-Lagos, R. Guía para Estudios Dietéticos: Álbum Fotográfico de Alimentos; University of Granada: Granada, Spain, 2011. [Google Scholar]
- Monteagudo, C.; Palacín-Arce, A.; del Mar Bibiloni, M.; Pons, A.; Tur, J.A.; Olea-Serrano, F.; Mariscal-Arcas, M. Proposal for a Breakfast Quality Index (BQI) for children and adolescents. Public Health Nutr. 2013, 16, 639–644. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruiz, J.R.; Castro-Piñero, J.; España-Romero, V.; Artero, E.G.; Ortega, F.B.; Cuenca, M.M.; Jimenez-Pavón, D.; Chillón, P.; Girela-Rejón, M.J.; Mora, J.; et al. Field-based fitness assessment in young people: The ALPHA health-related fitness test battery for children and adolescents. Br. J. Sports Med. 2011, 45, 518–524. [Google Scholar] [CrossRef]
- Leger, L.A.; Mercier, D.; Gadoury, C.; Lambert, J. The multistage 20 metre shuttle run test for aerobic fitness. J. Sports Sci. 1988, 6, 93–101. [Google Scholar] [CrossRef] [PubMed]
- Migueles, J.H.; Cadenas-Sanchez, C.; Ekelund, U.; Delisle Nyström, C.; Mora-Gonzalez, J.; Löf, M.; Labayen, I.; Ruiz, J.R.; Ortega, F.B. Accelerometer Data Collection and Processing Criteria to Assess Physical Activity and Other Outcomes: A Systematic Review and Practical Considerations. Sport. Med. 2017, 47, 1821–1845. [Google Scholar] [CrossRef] [PubMed]
- Chandler, J.L.; Brazendale, K.; Beets, M.W.; Mealing, B.A. Classification of physical activity intensities using a wrist-worn accelerometer in 8–12-year-old children. Pediatr. Obes. 2016, 11, 120–127. [Google Scholar] [CrossRef] [PubMed]
- Cuenca-García, M.; Ruiz, J.R.; Ortega, F.B.; Labayen, I.; González-Gross, M.; Moreno, L.A.; Gomez-Martinez, S.; Ciarapica, D.; Hallström, L.; Wästlund, A.; et al. Association of breakfast consumption with objectively measured and self-reported physical activity, sedentary time and physical fitness in European adolescents: The HELENA (Healthy Lifestyle in Europe by Nutrition in Adolescence) Study. Public Health Nutr. 2014, 17, 2226–2236. [Google Scholar] [CrossRef] [Green Version]
- Corder, K.; van Sluijs, E.M.F.; Steele, R.M.; Stephen, A.M.; Dunn, V.; Bamber, D.; Goodyer, I.; Griffin, S.J.; Ekelund, U. Breakfast consumption and physical activity in British adolescents. Br. J. Nutr. 2011, 105, 316–321. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| All | Boys | Girls | ||||
|---|---|---|---|---|---|---|
| N | Mean ± SD | N | Mean ± SD | N | Mean ± SD | |
| Age (years) | 173 | 9.7 ± 0.3 | 86 | 9.7 ± 0.3 | 87 | 9.6 ± 0.3 |
| Weight (kg) | 173 | 33.2 ± 6.6 | 86 | 33.2 ± 7.1 | 87 | 33.2 ± 6.1 |
| Height (cm) | 173 | 137.7 ± 5.6 | 86 | 137.9 ± 5.8 | 87 | 137.4 ± 5.4 |
| Body mass index (kg/m2) | 173 | 17.4 ± 2.6 | 86 | 17.3 ± 2.7 | 87 | 17.5 ± 2.6 |
| Body fat percentage (%) | 173 | 18.7 ± 7.3 | 86 | 16.1 ± 5.1 | 87 | 21.3 ± 8.2 |
| Fat-free mass (kg) | 172 | 59.4 ± 5.8 | 85 | 61.3 ± 3.8 | 87 | 57.5 ± 6.8 |
| Weight status (%) *: | ||||||
| Normal weight | 126 | 72.8% | 63 | 73.3% | 63 | 72.4% |
| Overweight/Obese | 47 | 27.2% | 23 | 26.7% | 24 | 27.6% |
| Diet: | ||||||
| Mediterranean dietary pattern | 130 | 5.9 ± 1.6 | 63 | 6.1 ±1.6 | 67 | 5.8 ±1.7 |
| Breakfast quality index | 175 | 3.9 ± 1.1 | 86 | 3.9 ± 1.2 | 89 | 3.8 ± 1.0 |
| Physical fitness: | ||||||
| Cardiorespiratory fitness (laps) | 172 | 39.5 ± 20.3 | 84 | 48.5 ± 21.6 | 88 | 31.1 ± 14.6 |
| Upper-limbs muscular strength (kg) | 173 | 15.1 ± 3.0 | 85 | 15.7 ± 3.4 | 88 | 14.6 ± 2.5 |
| Lower-limbs muscular strength (cm) | 172 | 134.5 ± 19.8 | 84 | 141.0 ± 19.4 | 88 | 128.2 ± 18.6 |
| Speed–agility (sec) | 172 | 12.3 ± 0.8 | 84 | 12.0 ± 0.7 | 88 | 12.6 ± 0.8 |
| Physical activity (min/day) †: | ||||||
| Moderate-to-vigorous physical activity | 161 | 117.6 ± 28.8 | 79 | 121.0 ± 27.5 | 82 | 114.9 ± 29.6 |
| Wearing time (awake) | 161 | 828.3 ± 41.6 | 79 | 831.3 ± 43.1 | 82 | 825.2 ± 40.4 |
| Mediterranean Dietary Pattern | Breakfast Quality Index | |||||
|---|---|---|---|---|---|---|
| β | B | p | β | B | p | |
| Model 1: | ||||||
| Cardiorespiratory fitness | 0.189 | 2.416 | 0.019 | 0.058 | 1.062 | 0.406 |
| Upper-limbs muscular strength | −0.089 | −0.164 | 0.312 | 0.036 | 0.098 | 0.628 |
| Lower-limbs muscular strength | 0.196 | 2.542 | 0.017 | 0.115 | 2.058 | 0.116 |
| Speed–agility * | −0.210 | −0.117 | 0.010 | −0.050 | −0.038 | 0.494 |
| Model 2: | ||||||
| Cardiorespiratory fitness | 0.126 | 1.564 | 0.116 | 0.009 | 0.158 | 0.898 |
| Upper-limbs muscular strength | −0.160 | −0.289 | 0.071 | 0.089 | 0.231 | 0.247 |
| Lower-limbs muscular strength | 0.141 | 1.796 | 0.091 | 0.093 | 1.695 | 0.207 |
| Speed–agility * | −0.121 | −0.061 | 0.131 | −0.017 | −0.012 | 0.809 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cadenas-Sanchez, C.; Medrano, M.; Arenaza, L.; Amasene, M.; Osés, M.; Labayen, I. Association between Mediterranean Dietary Pattern and Breakfast Quality with Physical Fitness in School Children: The HIIT Project. Nutrients 2021, 13, 1353. https://doi.org/10.3390/nu13041353
Cadenas-Sanchez C, Medrano M, Arenaza L, Amasene M, Osés M, Labayen I. Association between Mediterranean Dietary Pattern and Breakfast Quality with Physical Fitness in School Children: The HIIT Project. Nutrients. 2021; 13(4):1353. https://doi.org/10.3390/nu13041353
Chicago/Turabian StyleCadenas-Sanchez, Cristina, María Medrano, Lide Arenaza, Maria Amasene, Maddi Osés, and Idoia Labayen. 2021. "Association between Mediterranean Dietary Pattern and Breakfast Quality with Physical Fitness in School Children: The HIIT Project" Nutrients 13, no. 4: 1353. https://doi.org/10.3390/nu13041353