
Potential Immunomodulatory Effects from Consumption of Nutrients in Whole Foods and Supplements on the Frequency and Course of Infection: Preliminary Results


Abstract
:1. Introduction
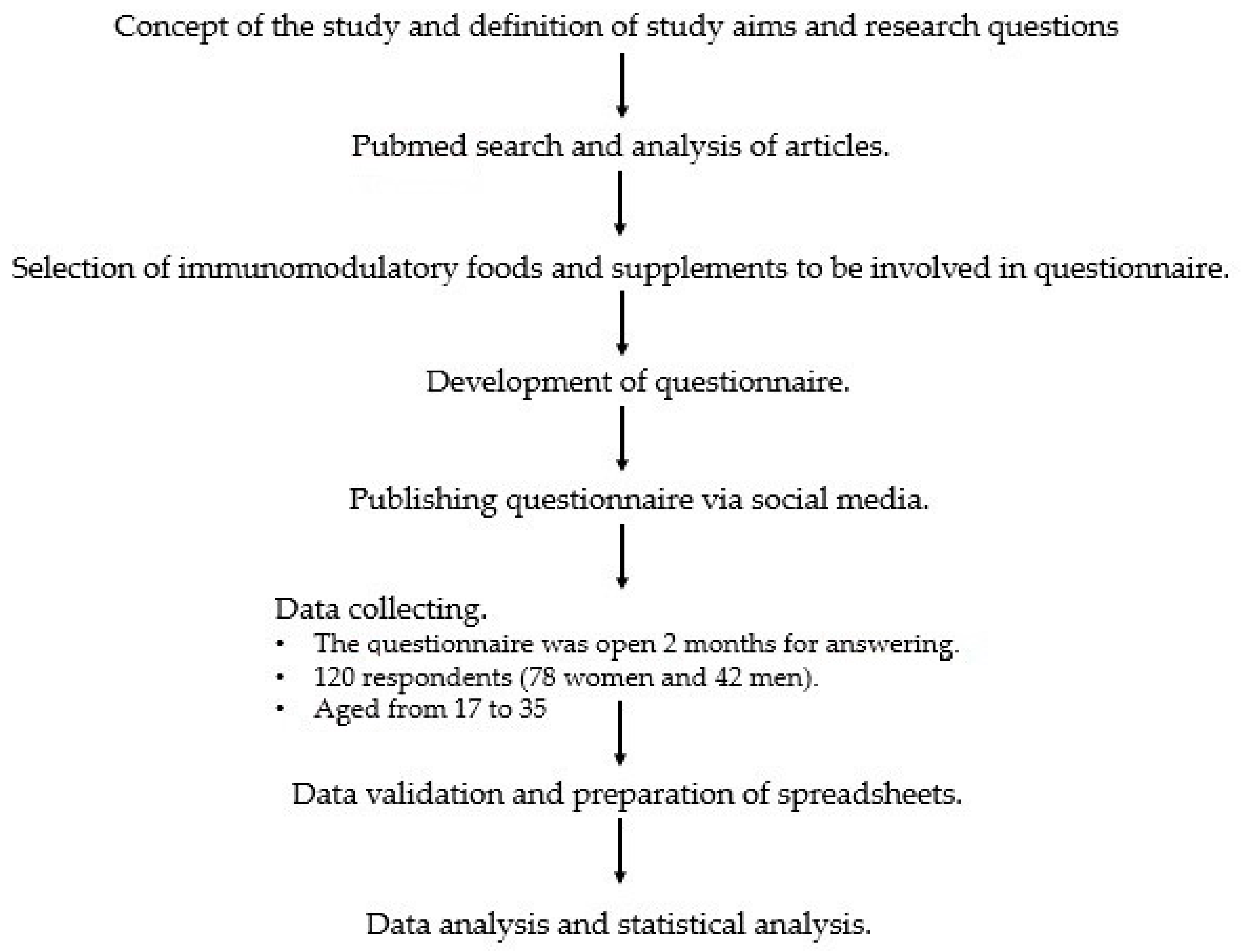
2. Materials and Methods
2.1. Study Design
2.2. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dymarska, E.; Grochowska, A.; Krauss, H. Wpływ sposobu odżywiania na układ odpornościowy. Immunomodulacyjne działanie kwasów tłuszczowych, witamin, składników mineralnych oraz przeciwutleniaczy. Now. Lek. 2013, 82, 222–231. [Google Scholar]
- Krzysik, M.; Biernat, J.; Grajeta, H. The Influence of Nutrients on Immune System Functioning–Part I. Immunomodulatory Effects of Fatty Acids on the Human Body. Adv. Clin. Exp. Med. 2007, 16, 123–133. [Google Scholar]
- Toti, E.; Chen, O.C.-Y.; Palmery, M.; Valencia, D.V.; Peluso, I. Non-Provitamin A and Provitamin a Carotenoids as Immunomodulators: Recommended Dietary Allowance, Therapeutic Index, or Personalized Nutrition? Oxid. Med. Cell. Longev. 2018, 2018, 4637861. [Google Scholar] [CrossRef]
- Rutkowski, M.; Matuszewski, T.; Kędziora, J.; Witaminy, A. E i C jako antyoksydanty. Pol. Merk. Lek. 2010, 174, 377–381. [Google Scholar]
- Całkosiński, I.; Rosińczuk-Tonderys, J.; Szopa, M. Zastosowanie wysokich dawek tokoferolu w prewencji i potencjalizacji działania dioksyn. Postepy Hig. Med. Dosw. 2011, 65, 143–157. [Google Scholar] [CrossRef]
- Maćkowiak, K.; Torliński, L. Współczesne poglądy na rolę witaminy. Now. Lek. 2007, 76, 349–356. [Google Scholar]
- Myszka, M.; Klinger, M. Immunomodulacyjne działanie witaminy D. Postępy Hig. Med. Dosw. 2014, 68, 865–878. [Google Scholar] [CrossRef]
- Baeke, F.; Korf, H.; Overbergh, L.; van Etten, E.; Verstuyf, A.; Gysemans, C.; Mathieu, C. Human T lymphocytes are direct targets of 1,25-dihydroxyvitamin D3 in the immune system. J. Steroid Biochem. Mol. Biol. 2010, 121, 221–227. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.; Sims, G.P.; Chen, X.X.; Gu, Y.Y.; Chen, S.; Lipsky, P.E. Modulatory effects of 1,25-dihydroxyvitamin D3 on human B cell differentiation. J. Immunol. 2007, 179, 1634–1647. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Artym, J.; Zimecki, M. Organizm gospodarza kontra drobnoustroje w walce o żelazo. Rola Żelaza w Zakażeniach. Kosmos 2014, 63, 345–366. [Google Scholar]
- Arytm, J.; Udział laktoferryny w gospodarce żelazem w organizmie; Część, I. Wpływ laktoferryny na wchłanianie, transport i magazynowanie żelaza. Postępy Hig. Med. Dosw. 2008, 62, 599–611. [Google Scholar]
- Klecha, B.; Bukowska, B. Selen w organizmie człowieka–charakterystyka pierwiastka i potencjalne zastosowanie terapeutyczne. Bromat. Cem. Toksykol. 2016, 4, 825–826. [Google Scholar]
- Maggini, S.; Wintergerst, E.S.; Beveridge, S.; Hornig, D.H. Selected vitamins and trace elements support immune function bystrengthening epithelial barriers and cellular and humoral immune responses. Br. J. Nutr. 2007, 98, S29–S35. [Google Scholar] [CrossRef] [PubMed]
- Calder, P.C.; Carr, A.C.; Gombart, A.F.; Eggersdorfer, M. Optimal nutritional status for a well-functioning immune system is an important factor to protect against viral infections. Nutrients 2020, 12, 1181. [Google Scholar] [CrossRef] [Green Version]
- Kościej, A.; Skotnicka-Graca, U.; Ozga, I. Importance of selected nutritional factors for children’s immunity. Probl. Hig. Epidemiol. 2017, 98, 110–117. [Google Scholar]
- Maciorowska, E.; Ryszczuk, E. Rola probiotyków i prebiotyków w procesie immunomodulacji w przewodzie pokarmowym. Zakażenia 2012, 1, 33–39. [Google Scholar]
- Kaźmierska, A. Probiotyki–recepta na zdrowie? Kosmos. Probl. Nauk Biol. 2014, 63, 455–472. [Google Scholar]
- Parvez, S.; Malik, K.A.; Kang, S.A.; Kim, Y.H. Probiotics and their fermented food products are beneficial for health. Food Sci. Nutr. 2017, 59, 506–527. [Google Scholar] [CrossRef]
- Giugliano, D.; Ceriello, A.; Esposisto, K. The Effects of Diet on Inflammation. J. Am. Coll. Cardiol. 2006, 48, 678–685. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grzelak, T.; Suliga, K.; Pelczyńska, M.; Sperling, M.; Czyżewska, K. Ocena częstości stosowania suplementów diety wśród wegetarian oraz osób odżywiających się tradycyjnie. Probl. Hig. Epidemiol. 2017, 98, 170–176. [Google Scholar]
- Bińkowska-Bury, M.; Więch, P.; Januszewicz, P. The use of dietary supplementation among university students. Zdr. Publ. 2010, 102, 144–149. [Google Scholar] [CrossRef] [Green Version]
- Zegan, M.; Michota-Katulska, E.; Gałązka, M.; Sińska, B.; Kucharska, A. Suplementy diety i żywność stosowana w celu wspomagania odporności–badania pilotażowe. Probl. Hig. Epidemiol. 2013, 94, 910–914. [Google Scholar]
- Skop-Lewandowska, A.; Małek, A.; Gmur, M.; Kolarzyk, E. Mode of nutrition and popularity of dietary supplements and food supplements among young people attending fitness clubs. Probl. Hig. Epidemiol. 2013, 94, 786–793. [Google Scholar]
- Stang, J.; Story, M.T.; Harnack, L.; Neumark-Sztainer, D. Relationships between vitamin and mineral supplement use, dietary intake, and dietary adequacy among adolescents. J. Am. Diet. Assoc. 2000, 100, 905–910. [Google Scholar] [CrossRef]
- Millen, A.E.; Dodd, K.W.; Subar, A.F. Use of vitamin, mineral, nonvitamin, and nonmineral supplements in the United States: The 1987, 1992, and 2000 National Health Interview Survey results. J. Am. Diet. Assoc. 2004, 104, 942–950. [Google Scholar] [CrossRef]
- Iddir, M.; Brito, A.; Dingeo, G.; Fernandez Del Campo, S.S.; Samouda, H.; La Frano, M.R.; Bohn, T. Strengthening the Immune System and Reducing Inflammation and Oxidative Stress through Diet and Nutrition: Considerations during theCOVID-19 Crisis. Nutrients 2020, 12, 1562. [Google Scholar] [CrossRef] [PubMed]
- Hemilä, H. Vitamin C and infections. Nutrients 2017, 9, 339. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wannamethee, S.G.; Lowe, G.D.; Rumley, A.; Bruckdorfer, K.R.; Whincup, P.H. Associations of vitamin C status, fruit and vegetable intakes, and markers of inflammation and hemostasis. Am. J. Clin. Nutr. 2006, 83, 567–574. [Google Scholar] [CrossRef] [PubMed]
- Misiorowski, W.; Misiorowska, J.; Dębski, R.; Głuszko, P.; Tłustochowicz, W.; Zgliczyński, W. Stanowisko Zespołu Ekspertów w sprawie stosowania wysokich dawek witaminy D w zapobieganiu i leczeniu jej niedoboru. Medycyna po Dyplomie 2017, 9, 36–45. [Google Scholar]
- Hansdottir, S.; Monick, M.M. Vitamin D effects on lung immunity and respiratory diseases. Vitam. Horm. 2011, 86, 217–237. [Google Scholar] [CrossRef] [Green Version]
- Martineau, A.R.; Jolliffe, D.A.; Hooper, R.L.; Greenberg, L.; Aloia, J.F.; Bergman, P.; Dubnov-Raz, G.; Esposito, S.; Ganmaa, D.; Ginde, A.A.; et al. Vitamin D supplementation to prevent acute respiratory tract infections: Systematic review and meta-analysis of individual participant data. BMJ 2017, 356, i6583. [Google Scholar] [CrossRef] [Green Version]
- Cannell, J.J.; Vieth, R.; Umhau, J.C.; Holick, M.F.; Grant, W.B.; Madronich, S.; Garland, C.F.; Giovannucci, E. Epidemic influenza and vitamin D. Epidemiol. Infect. 2006, 134, 1129–1140. [Google Scholar] [CrossRef]
- Jolliffe, D.A.; Griffiths, C.J.; Martineau, A.R. Vitamin D in the prevention of acute respiratory infection: Systematic review of clinical studies. J. Steroid Biochem. Mol. Biol. 2013, 136, 321–329. [Google Scholar] [CrossRef]
- Rhodes, J.M.; Subramanian, S.; Laird, E.; Kenny, R.A. Low population mortality from COVID-19 in countries south of latitude 35 degrees north supports vitamin D as a factor determining severity. Aliment Pharmacol Ther. 2020, 51, 1434–1437. [Google Scholar] [CrossRef] [Green Version]
- Calder, P.C. Omega-3 polyunsaturated fatty acids and inflammatory processes: Nutrition or pharmacology?: Omega-3 fatty acids and inflammation. Br. J. Clin. Pharmacol. 2012, 75, 645–662. [Google Scholar] [CrossRef] [Green Version]
- Basil, M.C.; Levy, B.D. Specialized pro-resolving mediators: Endogenous regulators of infection and inflammation. Nat. Rev. Immunol. 2016, 16, 51–67. [Google Scholar] [CrossRef]
- Calder, P.C. n-3 polyunsaturated fatty acids, inflammationand immunity: Pouring oil on troubled waters or anotherfishytale? Nutr. Res. 2001, 21, 309–341. [Google Scholar] [CrossRef]
- Calder, P.C.; Grimble, R.F. Polyunsaturated fatty acids, inflammation andimmunity. Eur. J. Clin. Nutr. 2002, 56, S14–S19. [Google Scholar] [CrossRef] [Green Version]
- Artym, J. The role of lactoferrin in the iron metabolism. Part II. Antimicrobial and antiinflammatory effect of lactoferrin by chelation of iron. Adv. Hyg. Exp. Med. 2010, 64, 604–616. [Google Scholar]
- Bowman, B.A.; Russell, R.M. Present Knowledge in Nutrition, 9th ed.; ILSI Press: Washington, DC, USA, 2006. [Google Scholar]
- Beard, J.L. Iron biology in immune function, muscle metabolism and neuronal functioning. J. Nutr. 2001, 131, 568S–579S. [Google Scholar] [CrossRef]
- Cassat, J.E.; Skaar, E.P. Iron in infection and immunity. Cell Host Microbe 2013, 13, 509–519. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saeed, F.; Nadeem, M.; Ahmed, R.; Nadeem, M.; Arshad, M.; Ullah, A. Studying the impact of nutritional immunology underlying the modulation of immune responses by nutritional compounds—A review. Food Agric. Immunol. 2016, 27, 205–229. [Google Scholar] [CrossRef] [Green Version]
- Broome, C.S.; McArdle, F.; Kyle, J.A.; Andrews, F.; Lowe, N.M.; Hart, C.A.; Arthur, J.R.; Jackson, M.J. An increase in selenium intake improves immune function and poliovirus handling in adults with marginal selenium status. Am. J. Clin. Nutr. 2004, 80, 154–162. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, P.R.; Berry, M.J. The influence of selenium on immune responses. Mol. Nutr. Food Res. 2008, 52, 1273–1280. [Google Scholar] [CrossRef]
- Avery, J.C.; Hoffmann, P.R. Selenium, Selenoproteins, and Immunity. Nutrients 2018, 10, 1203. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stephensen, C.B. Vitamin A, infection, and immune function. Annu. Rev. Nutr. 2001, 21, 167–192. [Google Scholar] [CrossRef]
- Semba, R.D. Vitamin A and immunity to viral, bacterial and proto-zoan infections. Proc. Nutr. Soc. 1999, 58, 719–727. [Google Scholar] [CrossRef] [Green Version]
- Coutsoudis, A.; Kiepiela, P.; Coovadia, H.M.; Broughton, M. Vitamin A supplementation enhances specificIgG antibody levels and total lymphocyte numbers while improvingmorbidity in measles. Pediatric Infect. Dis. J. 1992, 11, 203–209. [Google Scholar] [CrossRef]
- Gombart, A.F.; Pierre, A.; Maggini, S. A review of micronu-trients and the immune system-working in harmony to reduce therisk of infection. Nutrients 2020, 12, 236. [Google Scholar] [CrossRef] [Green Version]
- Prasad, A.S.; Beck, F.W.; Bao, B.; Fitzgerald, J.T.; Snell, D.C.; Steinberg, J.D.; Cardozo, L.J. supplementation decreases incidence of infections in the elderly: Effect of zinc on generation of cytokines and oxidative stress. Am. J. Clin. Nutr. 2007, 85, 837–844. [Google Scholar] [CrossRef] [Green Version]
- Kahmann, L.; Uciechowski, P.; Warmuth, S.; Plümäkers, B.; Gressner, A.M.; Malavolta, M.; Mocchegiani, E.; Rink, L. Zinc supplementation in the elderly reduces spontaneous inflammatory cytokine release and restores T cell functions. Rejuvenation Res. 2008, 11, 227–237. [Google Scholar] [CrossRef] [PubMed]
- Boukaiba, N.; Flament, C.; Acher, S.; Chappuis, P.; Piau, A.; Fusselier, M.; Dardenne, M.; Lemonnier, D. A physiological amount of zinc supplementation: Effects on nutritional, lipid, and thymic status in an elderly population. Am. J. Clin. Nutr. 1993, 57, 566–572. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine. Dietary Reference Intakes for Vitamin A, Vitamin K, Arsenic, Boron, Chromium, Copper, Iodine, Iron, Manganese, Molybdenum, Nickel, Silicon, Vanadium, and Zinc; The National Academies Press: Washington, DC, USA, 2001; Volume 44. [Google Scholar] [CrossRef] [Green Version]
- Maggini, S.; Beveridge, S.; Sorbara, J.P.; Senatore, G. Feeding the immune system: The role of micronutrients in restoring resistance to infections. CAB. Rev. 2008, 3, 1–21. [Google Scholar] [CrossRef]
- Vieira, A.T.; Teixeira, M.M.; Martins, F.S. The role of probiotics and prebiotics in inducing gut immunity. Front. Immunol. 2013, 4, 445. [Google Scholar] [CrossRef] [PubMed]
- Haywooda, A.B.; Blacka, E.K.; Bakerb, D.; Mc Garveyb, J.; Healey, P. Probiotic supplementation reduces the duration and incidence of infections but not severity in elite rugby union players. J. Sci. Med. Sport 2014, 17, 356–360. [Google Scholar] [CrossRef]
- Winkler, P.; de Vrese, M.; Laue, C.H.; Schrezenmeir, J. Effect of a dietary supplement containing probiotic bacteria plus vitamins and minerals on common cold infections and cellular immune parameters. Int. J. Clin. Pharmacol. Ther. 2005, 43, 318–326. [Google Scholar] [CrossRef] [PubMed]
- Steinert, E.R.; Lee, Y.K.; Sybesma, W. Vitamins for the Gut Microbiome. Trends Mol. Med. 2020, 26, 137–140. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Incidence of Infection | Viral Infections | Bacterial Infections | Fungal Infections |
|---|---|---|---|
| Never | 10.0 | 52.5 | 79.2 |
| Occasionally (1–3 times a year) | 80.0 | 40.8 | 18.3 |
| Often (4–6 times a year) | 9.2 | 6.7 | 2.5 |
| Very often (more than 7 times a year) | 0.8 | 0.0 | 0.0 |
| The course of infection | Number of respondents reporting the course of infection | ||
| Severe, but without complications | 38.4 | ||
| Mild | 60.8 | ||
| Severe, and with complications | 0.8 | ||
| Duration of infection | Number of respondents reporting the duration of infection | ||
| >7 days | 17.5 | ||
| 4–6 days | 36.7 | ||
| 1–3 days | 45.8 | ||
| Product or Supplement/ Frequency of Consumption | Daily | A Few Times a Week | Once a Week or Several Times a Month | Several Times a Year | Never |
|---|---|---|---|---|---|
| foods rich in omega-3 | 7.5 | 25.8 | 45.8 | 18.4 | 2.5 |
| supplements rich in omega-3 | 7.5 | 9.2 | 10.0 | 22.5 | 50.8 |
| foods rich in vitamin A | 28.3 | 45.0 | 25.0 | 0.8 | 0.8 |
| supplements rich in vitamin A | 8.3 | 10.0 | 11.7 | 19.2 | 40.8 |
| products rich in β-carotene | 31.7 | 40.8 | 26.7 | 0.0 | 0.8 |
| supplements rich in β-carotene | 3.3 | 4.2 | 17.5 | 15.0 | 60.0 |
| products rich in vitamin E | 16.7 | 26.7 | 45.0 | 9.2 | 2.5 |
| supplements rich in vitamin E | 6.7 | 3.3 | 21.6 | 16.7 | 51.7 |
| products rich in vitamin C | 39.2 | 40.0 | 16.7 | 2.5 | 1.7 |
| supplements rich in vitamin C | 12.5 | 10.8 | 27.5 | 19.2 | 30.0 |
| products rich in vitamin D | 2.5 | 13.3 | 56.7 | 20.8 | 6.7 |
| supplements rich in vitamin D | 11.7 | 11.7 | 15.8 | 15.8 | 45.0 |
| products rich in iron | 39.2 | 35.0 | 22.5 | 2.5 | 53.3 |
| supplements rich in iron | 4.2 | 7.5 | 21.7 | 13.3 | 0.8 |
| products rich in zinc | 15.8 | 19.2 | 48.4 | 15.0 | 1.6 |
| supplements rich in zinc | 3.3 | 5.8 | 14.2 | 16.7 | 60.0 |
| products rich in selenium | 19.2 | 25.8 | 48.4 | 5.8 | 0.8 |
| supplements rich in selenium | 2.5 | 1.7 | 16.7 | 11.7 | 67.5 |
| products rich in probiotic bacteria | 25.0 | 38.3 | 30.8 | 5.0 | 0.8 |
| supplements rich in probiotic bacteria | 5.0 | 5.8 | 15.0 | 26.7 | 47.5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Polak, E.; Stępień, A.E.; Gol, O.; Tabarkiewicz, J. Potential Immunomodulatory Effects from Consumption of Nutrients in Whole Foods and Supplements on the Frequency and Course of Infection: Preliminary Results. Nutrients 2021, 13, 1157. https://doi.org/10.3390/nu13041157
Polak E, Stępień AE, Gol O, Tabarkiewicz J. Potential Immunomodulatory Effects from Consumption of Nutrients in Whole Foods and Supplements on the Frequency and Course of Infection: Preliminary Results. Nutrients. 2021; 13(4):1157. https://doi.org/10.3390/nu13041157
Chicago/Turabian StylePolak, Ewelina, Agnieszka Ewa Stępień, Olga Gol, and Jacek Tabarkiewicz. 2021. "Potential Immunomodulatory Effects from Consumption of Nutrients in Whole Foods and Supplements on the Frequency and Course of Infection: Preliminary Results" Nutrients 13, no. 4: 1157. https://doi.org/10.3390/nu13041157