Analysis of the Impact of a Multi-Strain Probiotic on Body Composition and Cardiorespiratory Fitness in Long-Distance Runners

 , ,
, ,
Abstract
:1. Introduction
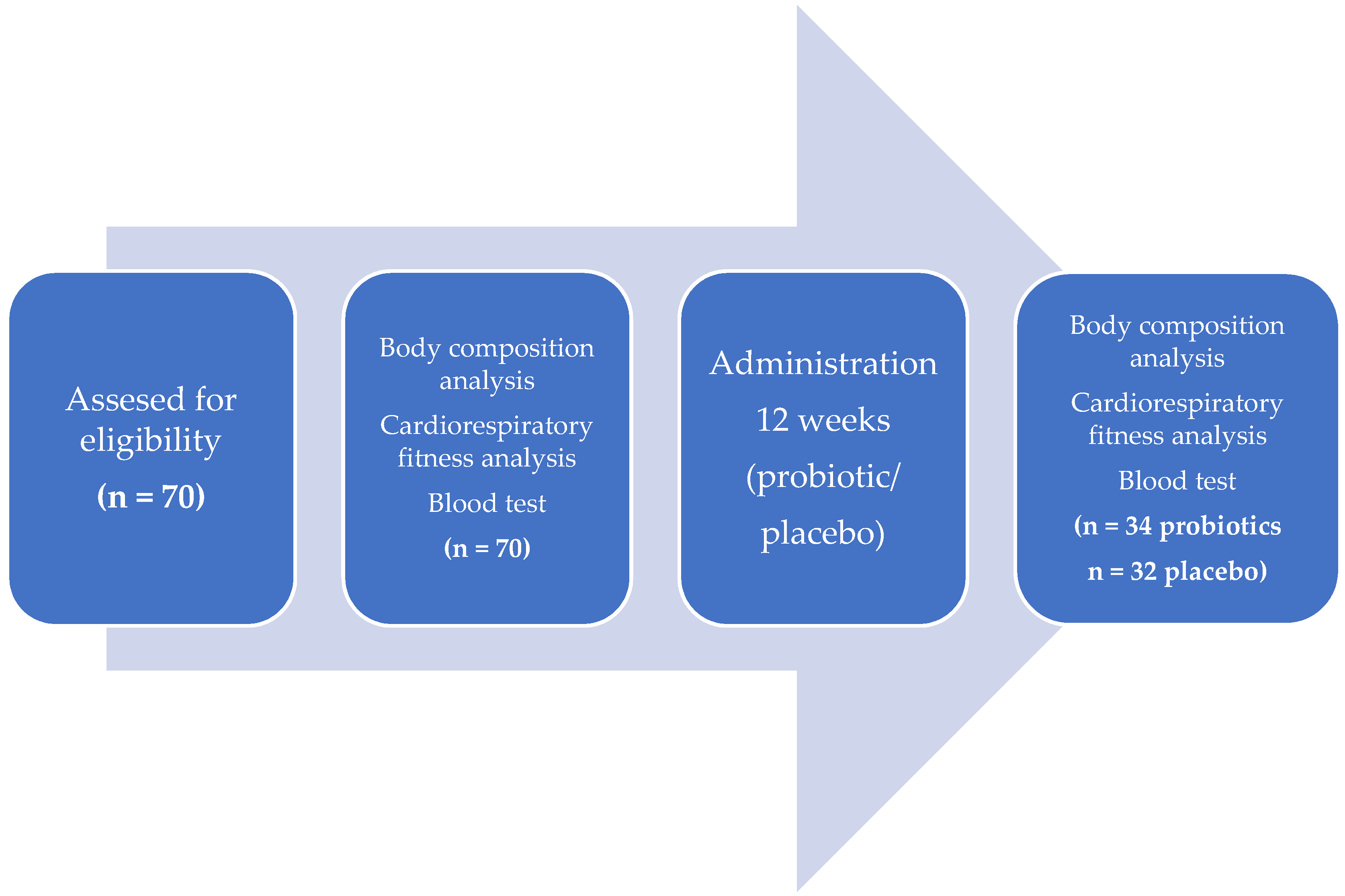
2. Materials and Methods
2.1. Body Composition
2.2. Cardiorespiratory Fitness Analysis
2.3. Inflammation
2.4. Statistics
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Trial Registration
Conflicts of Interest
References
- Videbæk, S.; Bueno, A.M.; Nielsen, R.O.; Rasmussen, S. Incidence of running-related injuries per 1000 h of running in different types of runners: A systematic review and meta-analysis. Sports Med. 2015, 45, 1017–1026. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benjamin, I.; Rapoport, B.I. Metabolic factors limiting performance in marathon runners. PLoS Comput. Biol. 2010, 6, e1000960. [Google Scholar]
- Polish Running Report 2014. Available online: http://polskabiega.sport.pl/pdf/nsb_raport.pdf (accessed on 3 February 2020).
- Cureton, K.J.; Sparling, P.B. Distance running, performance and metabolic responses to running in men and women with excess weight experimentally equated. Med. Sci. Sports Exerc. 1980, 12, 288–294. [Google Scholar] [CrossRef] [PubMed]
- Maughan, R.J.; Burke, L.M. Żywienie a Zdolność do Wysiłku; Medicina Sportiva: Krakow, Poland, 2000. [Google Scholar]
- Manore, M.M. Dietary supplements for improving body composition and reducing body weight: Where is the evidence? Int. J. Sport Nutr. Exerc. Metab. 2012, 22, 139–154. [Google Scholar] [CrossRef] [PubMed]
- Chlíbková, D.; Knechtle, B.; Rosemann, T.; Žákovská, A.; Tomášková, I.; Shortall, M.; Tomášková, I. Changes in foot volume, body composition, and hydration status in male and female 24-hour ultra-mountain bikers. J. Int. Soc. Sports Nutr. 2014, 11, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andrzejewska, J.; Burdukiewicz, A.; Stachoń, A.; Pietraszewska, J. Influence of physical activity on body composition and podometric features of young men. JKES 2013, 23, 53–62. [Google Scholar] [CrossRef] [Green Version]
- Hoffman, M.D. Anthropometric characteristics of ultramarathoners. Int. J. Sports Med. 2008, 29, 808–811. [Google Scholar] [CrossRef]
- Hoffman, M.D.; Lebus, D.K.; Ganong, A.C.; Casazza, G.A.; Van Loan, M. Body composition of 161-km ultramarathoners. Int. J. Sports Med. 2010, 31, 106–109. [Google Scholar] [CrossRef]
- Adach, Z.; Brzenczek-Owczarzak, W.; Celejowa, I. Fizjologia wysiłku i treningu fizycznego. Wydaw. Lek. PZWL 2011, 30–75. [Google Scholar]
- Joyner, M.J.; Coyle, E.F. Endurance exercise performance: The physiology of champions. J. Physiol. 2008, 586 Pt 1, 35–44. [Google Scholar] [CrossRef]
- Durkalec-Michalski, K. Ocena Wpływu Suplementacji Kwasem Beta-Hydroksy-Beta-Metylomasłowym (HMB) na Wskaźniki Wydolności Fizycznej Zawodników Wybranych Dyscyplin Sportowych. Ph.D Thesis, Uniwersytet Medyczny im. Karola Marcinkowskiego w Poznaniu, Poznań, Poland, 2012. [Google Scholar]
- Legaz-Arrese, A.; Munguia-Izquierdo, D.; Nuviala, A.N.; Serveto-Galindo, O.; Urdiales, D.M.; Masia, J.R. Average VO2max as a function of running performances on different distances. Sci. Sport 2007, 22, 43–49. [Google Scholar] [CrossRef]
- Jäger, R.; Mohr, A.E.; Carpenter, K.C.; Kerksick, C.M.; Purpura, M.; Moussa, A.; Townsend, J.R.; Lamprecht, M.; West, N.P.; Black, K.; et al. International society of sports nutrition position stand: Probiotics. J. Int. Soc. Sports Nutr. 2019, 16, 62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- West, N.P.; Pyne, D.B.; Peake, J.M.; Cripps, A.W. Probiotics, immunity and exercise: A review. Exerc. Immunol. Rev. 2009, 15, 107–126. [Google Scholar] [PubMed]
- West, N.P.; Pyne, D.B.; Cripps, A.W.; Hopkins, W.G.; Eskesen, D.C.; Jairath, A.; Christophersen, C.T.; Conlon, M.A.; Fricker, P.A. Lactobacillus fermentum (PCC®) supplementation and gastrointestinal and respiratory-tract illness symptoms: A randomized control trial in athletes. Nutr. J. 2011, 10, 30. [Google Scholar] [CrossRef] [Green Version]
- Leite, G.S.F.; Resende Master Student, A.S.; West, N.P.; Lancha, A.H., Jr. Probiotics and sports: A new magic bullet? Nutrition 2019, 60, 152–160. [Google Scholar] [CrossRef] [Green Version]
- Jang, L.G.; Choi, G.; Kim, S.W.; Kim, B.Y.; Lee, S.; Park, H. The combination of sport and sport-specific diet is associated with characteristics of gut microbiota: An observational study. J. Int. Soc. Sports Nutr. 2019, 16, 21. [Google Scholar] [CrossRef] [Green Version]
- Zanuso, S.; Jimenez, A.; Pugliese, G.; Corigliano, G.; Balducci, S. Exercise for the management of type 2 diabetes: A review of the evidence. Acta Diabetol. 2010, 47, 15–22. [Google Scholar] [CrossRef] [Green Version]
- Li, J.; Siegrist, J. Physical activity and risk of cardiovascular disease—A meta-analysis of prospective cohort studies. Int. J. Environ. Res. Public Health 2012, 9, 391–407. [Google Scholar] [CrossRef]
- Carek, P.J.; Laibstain, S.E.; Carek, S.M. Exercise for the treatment of depression and anxiety. Int. J. Psychiatry Med. 2011, 41, 15–28. [Google Scholar] [CrossRef]
- Cartee, G.D.; Hepple, R.T.; Bamman, M.M.; Zierath, J.R. Exercise promotes healthy aging of skeletal muscle. Cell Metab. 2016, 23, 1034–1047. [Google Scholar] [CrossRef] [Green Version]
- Huang, W.C.; Lee, M.C.; Lee, C.C.; Ng, K.S.; Hsu, Y.J.; Tsai, T.Y.; Young, S.L.; Lin, J.S.; Huang, C.C. Effect of Lactobacillus plantarum TWK10 on exercise physiological Adaptation, PERFORMANCE, and body composition in healthy humans. Nutrients 2019, 11, 2836. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hottenrott, K.; Ludyga, S.; Schulze, S. Effects of high intensity training and continuous endurance training on aerobic capacity and body composition in recreationally active runners. J. Sports Sci. Med. 2012, 11, 483–488. [Google Scholar] [PubMed]
- Szulińska, M.; Łoniewski, I.; van Hemert, S.; Sobieska, M.; Bogdański, P. Dose-dependent effects of multispecies probiotic supplementation on the lipopolysaccharide (LPS) level and cardiometabolic profile in obese postmenopausal women: A 12-week randomized clinical trial. Nutrients 2018, 10, E773. [Google Scholar]
- Engin, A. The definition and prevalence of obesity and metabolic syndrome. Adv. Exp. Med. Biol. 2017, 960, 1–17. [Google Scholar] [PubMed]
- Kim, J.; Yun, J.M.; Kim, M.K.; Kwon, O.; Cho, B. Lactobacillus gasseri BNR17 supplementation reduces the visceral fat accumulation and waist circumference in obese adults: A randomized, double-blind, placebo-controlled trial. J. Med. Food 2018, 21, 454–461. [Google Scholar] [CrossRef] [PubMed]
- Wosinska, L.; Cotter, P.D.; O’Sullivan, O.; Guinane, C. The potential impact of probiotics on the gut microbiome of athletes. Nutrients 2019, 11, 2270. [Google Scholar] [CrossRef] [Green Version]
- Shing, C.M.; Peake, J.M.; Lim, C.L.; Briskey, D.; Walsh, N.P.; Fortes, M.B.; Ahuja, K.D.K.; Vitetta, L. Effects of probiotics supplementation on gastrointestinal permeability, inflammation and exercise performance in the heat. Eur. J. Appl. Physiol. 2014, 114, 93–103. [Google Scholar] [CrossRef] [PubMed]
- Huang, W.C.; Wei, C.C.; Huang, C.C.; Chen, W.L.; Huang, H.Y. The beneficial effects of Lactobacillus plantarum PS128 on high-intensity, exercise-induced oxidative stress, inflammation, and performance in triathletes. Nutrients 2019, 11, 353. [Google Scholar] [CrossRef] [Green Version]
- Vitale, K.; Getzin, A. Nutrition and supplement update for the endurance athlete: Review and recommendations. Nutrients 2019, 11, 1289. [Google Scholar] [CrossRef] [Green Version]
- Fedewa, M.V.; Hathaway, E.D.; Ward-Ritacco, C.L. Effect of exercise training on C reactive protein: A systematic review and meta-analysis of randomised and non-randomised controlled trials. Br. J. Sports Med. 2017, 51, 670–676. [Google Scholar] [CrossRef] [PubMed]
- Kostrzewa-Nowak, D.; Nowak, R.; Chamera, T.; Buryta, R.; Moska, W.; Cięszczyk, P. Post-effort chances in C-reactive protein level among soccer players at the end of the training season. J. Strength Cond. Res. 2015, 29, 1399–1405. [Google Scholar] [CrossRef] [PubMed]
- Lamprecht, M.; Bogner, S.; Schippinger, G. Probiotic supplementation affects markers of intestinal barrier, oxidation, and inflammation in trained men; a randomized, double-blinded, placebo-controlled trial. J. Int. Soc. Sports Nutr. 2012, 9, 45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zuhl, M.N.; Lanphere, K.R.; Kravitz, L.; Mermier, C.M.; Schneider, S.; Dokladny, K.; Moseley, P.L. Effects of oral glutamine supplementation on exercise-induced gastrointestinal permeability and tight junction protein expression. J. Appl. Physiol. 2014, 116, 183–191. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hackney, A.C.; Koltun, K.J. The immune system and overtraining in athletes: Clinical implications. Acta Clin. Croat. 2012, 51, 633–641. [Google Scholar] [PubMed]
- De Oliveira, E.P.; Burini, R.C. Food-dependent, exercise-induced gastrointestinal distress. J. Int. Soc. Sports Nutr. 2011, 8, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Probiotic Women (n = 14) | Placebo Women (n = 6) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Initial Stage (P) | Final Stage (F) | Initial Stage (P) | Final Stage (F) | ||||||||
| Parameter | Mean ± SD | Median | Mean ± SD | Median | p * | Mean ± SD | Median | Mean ± SD | Median | p * | p ** |
| TBW (kg) | 34.82 ± 3.30 | 34.25 | 35.24 ± 3.58 | 35.10 | 0.504 | 36.18 ± 2.02 | 35.90 | 37.03 ± 2.00 | 36.65 | 0.248 | 0.535 |
| LBM (kg) | 47.61 ± 4.50 | 46.90 | 48.18 ± 4.92 | 48.10 | 0.600 | 49.48 ± 2.76 | 48.95 | 50.71 ± 2.71 | 50.25 | 0.172 | 0.482 |
| BFM (kg) | 15.00 ± 3.98 | 14.80 | 14.57 ± 4.34 | 13.80 | 0.600 | 17.01 ± 8.12 | 16.40 | 17.11 ± 9.35 | 17.10 | 0.916 | 0.836 |
| PBF (%) | 23.82 ± 5.12 | 24.25 | 23.28 ± 5.59 | 23.05 | 0.916 | 24.65 ± 8.59 | 25.60 | 24.18 ± 10.26 | 26.10 | 0.600 | 0.772 |
| VAT (cm2) | 62.13 ± 21.04 | 60.50 | 59.37 ± 22.62 | 56.05 | 0.247 | 61.33 ± 27.20 | 70.00 | 61.18 ± 26.20 | 70.70 | 0.833 | 0.679 |
| SMM (kg) | 26.29 ± 2.72 | 25.90 | 26.57 ± 2.92 | 26.35 | 0.779 | 27.35 ± 1.61 | 26.85 | 28.10 ± 1.73 | 27.85 | 0.248 | 0.322 |
| Probiotic Men (n = 20) | Placebo Men (n = 26) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Initial Stage (P) | Final Stage (F) | Initial Stage (P) | Final Stage (F) | ||||||||
| Parameter | Mean ± SD | Median | Mean ± SD | Median | p * | Mean ± SD | Median | Mean ± SD | Median | p * | p ** |
| TBW (kg) | 47.43 ± 3.56 | 47.80 | 48.14 ± 3.82 | 48.60 | 0.019 | 49.20 ± 6.05 | 50.70 | 49.65 ± 6.00 | 50.55 | 0.061 | 0.327 |
| FFM (kg) | 64.73 ± 4.81 | 65.20 | 67.74 ± 5.23 | 66.40 | 0.019 | 67.15 ± 8.33 | 69.35 | 67.79 ± 8.29 | 69.00 | 0.063 | 0.338 |
| BFM (kg) | 14.62 ± 4.88 | 14.55 | 15.39 ± 4.64 | 14.60 | 0.184 | 13.83 ± 5.00 | 12.40 | 13.56 ± 4.88 | 13.15 | 0.431 | 0.067 |
| PBF (%) | 18.17 ± 5.05 | 17.95 | 18.76 ± 4.67 | 18.40 | 0.286 | 16.86 ± 4.86 | 15.65 | 16.54 ± 5.13 | 16.15 | 0.242 | 0.118 |
| VAT (cm2) | 61.80 ± 22.25 | 61.00 | 63.14 ±2 1.51 | 61.50 | 0.460 | 59.05 ± 21.33 | 59.05 | 58.06 ± 20.82 | 57.50 | 0.594 | 0.306 |
| SMM (kg) | 36.65 ± 2.86 | 37.35 | 37.29 ± 3.10 | 38.00 | 0.022 | 38.07 ± 4.98 | 39.45 | 38.46 ± 4.95 | 39.15 | 0.056 | 0.212 |
| Probiotic Women (n = 14) | Placebo Women (n = 6) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Initial Stage (P) | Final Stage (F) | Initial Stage (P) | Final Stage (F) | ||||||||
| Parameter | Mean ± SD | Median | Mean ± SD | Median | p * | Mean ± SD | Median | Mean ± SD | Median | p * | p ** |
| VO2max (mL/kg/min) | 34.02 ± 5.30 | 32.60 | 35.90 ± 6.16 | 35.25 | 0.140 | 36.98 ± 11.34 | 31.95 | 36.06 ± 8.85 | 33.00 | 0.600 | 0.302 |
| Ve (L/min) | 57.24 ± 10.54 | 56.00 | 61.24 ± 14.2 | 58.15 | 0.271 | 63.51 ± 15.25 | 60.15 | 63.48 ± 9.92 | 62.05 | 0.753 | 0.433 |
| Rf (1/min) | 30.25 ± 7.50 | 30.70 | 31.91 ± 8.57 | 32.05 | 0.300 | 30.06 ± 4.05 | 29.85 | 33.48 ± 4.02 | 34.15 | 0.027 | 0.386 |
| HR (bpm) | 150.28 ± 10.38 | 152.00 | 155.50 ± 9.1 | 158.00 | 0.208 | 153.50 ± 12.14 | 156.00 | 157.83 ± 13.16 | 161.00 | 0.093 | 0.967 |
| FeO2 (%) | 16.24 ± 0.47 | 16.19 | 16.25 ± 0.34 | 16.21 | 0.875 | 16.12 ± 0.36 | 16.12 | 16.17 ± 0.47 | 16.26 | 0.600 | 0.836 |
| FC (METS) | 9.72 ± 1.52 | 9.35 | 10.25 ± 1.7 | 10.05 | 0.151 | 10.56 ± 3.25 | 9.15 | 10.30 ± 2.53 | 9.40 | 0.600 | 0.248 |
| Max VO2/HR (mL/beat) | 14.10 ± 2.08 | 13.95 | 14.46 ± 2.47 | 13.98 | 0.432 | 15.63 ± 2.06 | 15.15 | 15.03 ± 2.25 | 14.70 | 0.401 | 0.247 |
| Breathing reserve (%) | 53.42 ± 8.95 | 56.00 | 50.50 ± 12.63 | 51.50 | 0.363 | 51.16 ± 9.32 | 53.00 | 50.66 ± 5.64 | 52.00 | 0.600 | 0.804 |
| Exercise capacity (mL/kg/min) | 34.02 ± 5.30 | 32.60 | 35.90 ± 6.16 | 35.25 | 0.934 | 36.98 ± 11.34 | 31.95 | 36.06 ± 8.85 | 33.00 | 0.710 | 0.302 |
| AT (mL/kg/min) | 19.97 ± 4.49 | 19.75 | 19.27 ± 3.02 | 18.65 | 0.868 | 21.40 ± 6.59 | 19.00 | 20.08 ± 6.81 | 18.05 | 0.772 | 0.868 |
| Probiotic Men (n = 20) | Placebo Men (n = 26) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Initial Stage (P) | Final Stage (F) | Initial Stage (P) | Final Stage (F) | ||||||||
| Parameter | Mean ± SD | Median | Mean± SD | Median | p * | Mean ± SD | Median | Mean ± SD | Median | p * | p ** |
| VO2max (mL/kg/min) | 38.22 ± 5.99 | 37.15 | 41.05 ± 8.02 | 41.10 | 0.017 | 42.34 ± 706 | 42.65 | 43.86 ± 7.58 | 43.40 | 0.286 | 0.313 |
| Ve (L/min) | 79.78 ± 17.11 | 79.65 | 87.78 ± 20.52 | 84.90 | 0.013 | 93.50 ± 23.54 | 92.15 | 97.94 ± 28.85 | 92.95 | 0.258 | 0.253 |
| Rf (1/min) | 30.37 ± 5.87 | 30.25 | 31.61 ± 6.62 | 32.10 | 0.232 | 34.30 ± 9.15 | 35.95 | 33.92 ± 9.18 | 36.85 | 0.892 | 0.277 |
| HR (bpm) | 150.20 ± 7.77 | 151.00 | 152.10 ± 7.68 | 151.00 | 0.156 | 152.23 ± 7.45 | 152.00 | 155.19 ± 9.55 | 155.00 | 0.119 | 0.876 |
| FeO2 (%) | 16.10 ± 0.49 | 16.19 | 16.18 ± 0.45 | 16.18 | 0.121 | 16.21 ± 0.66 | 16.31 | 16.21 ± 0.78 | 16.30 | 0.706 | 0.363 |
| FC (METS) | 10.91 ± 1.70 | 10.60 | 11.67 ± 2.32 | 11.70 | 0.036 | 12.10 ± 1.98 | 12.15 | 12.56 ± 2.20 | 12.40 | 0.170 | 0.340 |
| Max VO2/HR (mL/beat) | 20.21 ± 3.49 | 20.30 | 21.27 ± 4.29 | 22.15 | 0.102 | 22.51 ± 3.67 | 22.30 | 23.08 ± 3.92 | 23.70 | 0.492 | 0.287 |
| Breathing reserve (%) | 50.70 ± 10.13 | 50.00 | 45.75 ± 12.63 | 47.50 | 0.020 | 45.07 ± 15.41 | 51.00 | 45.26 ± 13.75 | 48.00 | 0.558 | 0.128 |
| Exercise capacity (mL/kg/min) | 38.21 ± 6.01 | 37.15 | 40.86 ± 8.14 | 41.10 | 0.036 | 42.42 ± 7.18 | 42.65 | 44.07 ± 7.87 | 43.40 | 0.196 | 0.363 |
| AT (mL/kg/min) | 21.05 ± 4.21 | 20.40 | 20.35 ± 3.33 | 20.75 | 0.346 | 21.85 ± 4.06 | 21.55 | 20.13 ± 3.58 | 20.45 | 0.850 | 0.340 |
| Probiotic Women(n = 14) | Placebo Women(n = 6) | ||||||||||
| Initial Stage(P) | Final Stage (F) | Initial Stage(P) | Final Stage (F) | ||||||||
| Parameter | Mean ± SD | Median | Mean ± SD | Median | p * | Mean ± SD | Median | Mean ± SD | Median | p * | p ** |
| CRP (mg/L) | 2.17 ± 3.50 | 0.85 | 0.87 ± 1.14 | 0.50 | 0.151 | 1.81 ± 2.17 | 0.95 | 1.21 ± 1.09 | 0.85 | 0.916 | 0.433 |
| TNF-alpha (pg/mL) | 10.82 ± 1.61 | 10.50 | 9.39 ± 1.43 | 9.48 | 0.003 | 10.57 ± 1.45 | 11.27 | 8.85 ± 1.21 | 8.36 | 0.074 | 0.693 |
| Probiotics Men(n = 20) | Placebo Men(n = 26) | ||||||||||
| Initial Stage(P) | Final Stage (F) | Initial Stage(P) | Final Stage (F) | ||||||||
| CRP (mg/L) | 1.75 ± 2.27 | 0.85 | 1.63 ± 2.81 | 1.00 | 0.459 | 1.40 ± 2.26 | 0.70 | 1.09 ± 1.31 | 0.70 | 0.330 | 0.334 |
| TNF-alpha (pg/mL) | 11.30 ± 0.85 | 11.21 | 9.68 ± 1.46 | 9.43 | 0.001 | 10.66 ± 0.95 | 10.71 | 9.78 ±1.69 | 8.87 | 0.016 | 0.327 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Smarkusz-Zarzecka, J.; Ostrowska, L.; Leszczyńska, J.; Orywal, K.; Cwalina, U.; Pogodziński, D. Analysis of the Impact of a Multi-Strain Probiotic on Body Composition and Cardiorespiratory Fitness in Long-Distance Runners. Nutrients 2020, 12, 3758. https://doi.org/10.3390/nu12123758
Smarkusz-Zarzecka J, Ostrowska L, Leszczyńska J, Orywal K, Cwalina U, Pogodziński D. Analysis of the Impact of a Multi-Strain Probiotic on Body Composition and Cardiorespiratory Fitness in Long-Distance Runners. Nutrients. 2020; 12(12):3758. https://doi.org/10.3390/nu12123758
Chicago/Turabian StyleSmarkusz-Zarzecka, Joanna, Lucyna Ostrowska, Joanna Leszczyńska, Karolina Orywal, Urszula Cwalina, and Damian Pogodziński. 2020. "Analysis of the Impact of a Multi-Strain Probiotic on Body Composition and Cardiorespiratory Fitness in Long-Distance Runners" Nutrients 12, no. 12: 3758. https://doi.org/10.3390/nu12123758