Global Leadership Initiative on Malnutrition Criteria Predict Pulmonary Complications and 90-Day Mortality after Major Abdominal Surgery in Cancer Patients

 , , ,
, , ,
Abstract
:1. Introduction
2. Methods
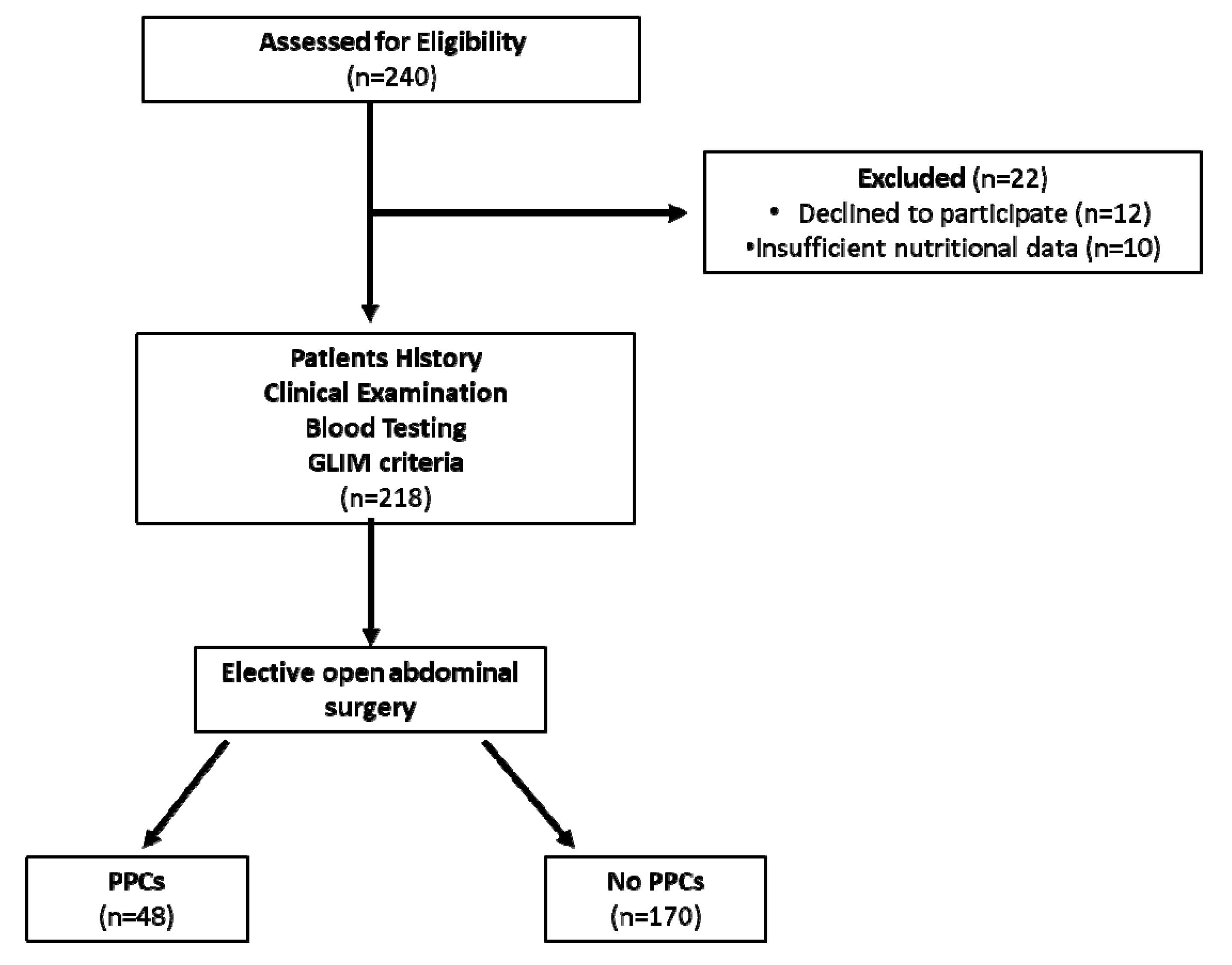
2.1. Study Participants and Design
2.2. Measures and Data Collection
- (1)
- Unintentional weight loss (>5% in 6 months);
- (2)
- Patient had low BMI (<20 kg/m2 if <70 years and<22 kg/m2 if ≥70years); or
- (3)
- Reductionof muscle mass based on calf circumference wasused as phenotypic criteria. For this test, knee was flexed to 90° with the feet and ankles relaxed, and the largest calf circumference was measured using a standard tape measure with 0.1 cm increment. Values lower than 31 cm were considered as low [26].
- (4)
- Reduced intake (>50% of energy intake during the last pre-admission week) orinflammatory response of the disease (chronic disease-related inflammation was evaluated using C reactive protein (CRP) values >5mg/dL) was used as etiologic criteria.
2.3. Outcomes
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| GLIM | Global Leadership Initiative on Malnutrition |
| BMI | Body Mass Index |
| PPCs | Postoperative pulmonary complications |
| ESPEN | European Society for Clinical Nutrition and Metabolism |
| LOS | Length of Hospital Stay |
| CRM | Cancer related malnutrition |
References
- Kirkland, L.L.; Shaughnessy, E. Recognition and Prevention of Nosocomial Malnutrition: A Review and A Call to Action! Am. J. Med. 2017, 130, 1345–1350. [Google Scholar] [CrossRef] [Green Version]
- Bullock, A.F.; Greenley, S.L.; McKenzie, G.A.G.; Paton, L.W.; Johnson, M.J. Relationship between markers of malnutrition and clinical outcomes in older adults with cancer: Systematic review, narrative synthesis and meta-analysis. Eur. J. Clin. Nutr. 2020, 74, 1519–1535. [Google Scholar] [CrossRef]
- Söderström, L.; Rosenblad, A.; Adolfsson, E.T.; Bergkvist, L. Malnutrition is associated with increased mortality in older adults regardless of the cause of death. Br. J. Nutr. 2017, 117, 532–540. [Google Scholar] [CrossRef] [Green Version]
- Lim, S.L.; Ong, K.C.B.; Chan, Y.H.; Loke, W.C.; Ferguson, M.; Daniels, L. Malnutrition and its impact on cost of hospitalization, length of stay, readmission and 3-year mortality. Clin. Nutr. 2012, 31, 345–350. [Google Scholar] [CrossRef] [Green Version]
- Barker, L.A.; Gout, B.S.; Crowe, T.C. Hospital Malnutrition: Prevalence, Identification and Impact on Patients and the Healthcare System. Int. J. Environ. Res. Public Health 2011, 8, 514–527. [Google Scholar] [CrossRef] [Green Version]
- Arends, J.; Baracos, V.V.; Bertz, H.H.; Bozzetti, F.; Calder, P.P.; Deutz, N.E.P.; Erickson, N.N.; Laviano, A.A.; Lisanti, M.M.; Lobo, D.N.D.; et al. ESPEN expert group recommendations for action against cancer-related malnutrition. Clin. Nutr. 2017, 36, 1187–1196. [Google Scholar] [CrossRef] [Green Version]
- Ryan, A.M.; Power, D.G.; Daly, L.; Cushen, S.J.; Bhuachalla, Ē.N.; Prado, C.M. Cancer-associated malnutrition, cachexia and sarcopenia: The skeleton in the hospital closet 40 years later. Proc. Nutr. Soc. 2016, 75, 199–211. [Google Scholar] [CrossRef] [Green Version]
- D’Almeida, C.A.; Peres, W.; De Pinho, N.B.; Martucci, R.B.; Rodrigues, V.D.; Ramalho, A. Prevalence of Malnutrition in Older Hospitalized Cancer Patients: A Multicenter and Multiregional Study. J. Nutr. Health Aging 2020, 24, 166–171. [Google Scholar] [CrossRef]
- Martin, L.; Gioulbasanis, I.; Senesse, P.; Baracos, V.E. Cancer-Associated Malnutrition and CT-Defined Sarcopenia and Myosteatosis Are Endemic in Overweight and Obese Patients. J. Parenter. Enter. Nutr. 2020, 44, 227–238. [Google Scholar] [CrossRef]
- Cederholm, T.; Jensen, G.L.; Correia, M.I.T.; Gonzalez, M.C.; Fukushima, R.; Higashiguchi, T.; Baptista, G.; Barazzoni, R.; Blaauw, R.; Coats, A.; et al. GLIM criteria for the diagnosis of malnutrition—A consensus report from the global clinical nutrition community. Clin. Nutr. 2019, 38, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Kondrup, J.; Allison, S.; Elia, M.; Vellas, B.; Plauth, M. ESPEN Guidelines for Nutrition Screening 2002. Clin. Nutr. 2003, 22, 415–421. [Google Scholar] [CrossRef]
- Gamaletsou, M.; Poulia, K.-A.; Karageorgou, D.; Yannakoulia, M.; Ziakas, P.; Zampelas, A.; Sipsas, N. Nutritional risk as predictor for healthcare-associated infection among hospitalized elderly patients in the acute care setting. J. Hosp. Infect. 2012, 80, 168–172. [Google Scholar] [CrossRef]
- Sierzega, M.; Niekowal, B.; Kulig, J.; Popiela, T. Nutritional Status Affects the Rate of Pancreatic Fistula after Distal Pancreatectomy: A Multivariate Analysis of 132 Patients. J. Am. Coll. Surg. 2007, 205, 52–59. [Google Scholar] [CrossRef]
- Correia, M.I.; Waitzberg, D.L. The impact of malnutrition on morbidity, mortality, length of hospital stay and costs evaluated through a multivariate model analysis. Clin. Nutr. 2003, 22, 235–239. [Google Scholar] [CrossRef]
- Skeie, E.; Tangvik, R.J.; Nymo, L.S.; Harthug, S.; Lassen, K.; Viste, A. Weight loss and BMI criteria in GLIM’s definition of malnutrition is associated with postoperative complications following abdominal resections—Results from a National Quality Registry. Clin. Nutr. 2020, 39, 1593–1599. [Google Scholar] [CrossRef] [Green Version]
- Haines, K.L.; Lao, W.; Nguyen, B.P.; Krishnamoorthy, V.; Williams, D.; Gallagher, S.; Agarwal, S.; Wischmeyer, P.E. Evaluation of Malnutrition via Modified GLIM Criteria for in Patients Undergoing Emergent Gastrointestinal Surgery. Clin. Nutr. 2020. [Google Scholar] [CrossRef]
- Patel, K.; Hadian, F.; Ali, A.; Broadley, G.; Evans, K.; Horder, C.; Johnstone, M.; Langlands, F.; Matthews, J.; Narayan, P.; et al. Postoperative pulmonary complications following major elective abdominal surgery: A cohort study. Perioper. Med. 2016, 5, 10. [Google Scholar] [CrossRef] [Green Version]
- Miskovic, A.; Lumb, A.B. Postoperative pulmonary complications. Br. J. Anaesth. 2017, 118, 317–334. [Google Scholar] [CrossRef] [Green Version]
- Arozullah, A.M.; Daley, J.; Henderson, W.G.; Khuri, S.F. Multifactorial Risk Index for Predicting Postoperative Respiratory Failure in Men After Major Noncardiac Surgery. The national veterans administration surgical quality improvement program. Ann. Surg. 2000, 232, 242–253. [Google Scholar] [CrossRef]
- Canet, J.; Sabaté, S.; Mazo, V.; Gallart, L.; De Abreu, M.G.; Belda, F.J.; Langeron, O.; Hoeft, A.A.; Pelosi, P. Development and validation of a score to predict postoperative respiratory failure in a multicentre European cohort: A prospective, observational study. Eur. J. Anaesthesiol. 2015, 32, 458–470. [Google Scholar] [CrossRef]
- Li, Y.S.; Meng, F.C.; Lin, J.K. Procedural and post-operative complications associated with laparoscopic versus open abdominal surgery for right-sided colonic cancer resection: A systematic review and meta-analysis. Medicine 2020, 99, e22431. [Google Scholar] [CrossRef]
- Yang, C.K.; Teng, A.; Lee, D.Y.; Rose, K. Pulmonary complications after major abdominal surgery: National Surgical Quality Improvement Program analysis. J. Surg. Res. 2015, 198, 441–449. [Google Scholar] [CrossRef]
- Lu, K.; Li, H.; Chen, Y.; Wu, B.; Zhang, J.; Huang, M.; Chen, J. Can the preoperative nutritional risk score be a predictor of the outcomes in critically ill patients of lung transplantation: A retrospective study. Ann. Transl. Med. 2020, 8, 40. [Google Scholar] [CrossRef]
- Karl, A.; Rittler, P.; Buchner, A.; Fradet, V.; Speer, R.; Walther, S.; Stief, G.C. Prospective Assessment of Malnutrition in Urologic Patients. Urology 2009, 73, 1072–1076. [Google Scholar] [CrossRef]
- Leong, D.T.K.; Yusuf, S. Reference ranges of handgrip strength from 125,462 healthy adults in 21 countries: A prospective urban rural epidemilogic (pure) study. J. Cachexia Sarcopenia Muscle 2016, 7, 535–546. [Google Scholar] [CrossRef]
- Rolland, Y.; Lauwers-Cances, V.; Cournot, M.; Nourhashémi, F.; Reynish, W.; Riviere, D.; Vellas, B.; Grandjean, H. Sarcopenia, Calf Circumference, and Physical Function of Elderly Women: A Cross-Sectional Study. J. Am. Geriatr. Soc. 2003, 51, 1120–1124. [Google Scholar] [CrossRef]
- Jammer, I.; Wickboldt, N.; Sander, M.; Smith, A.; Schultz, M.J.; Pelosi, P.; Leva, B.; Rhodes, A.; Hoeft, A.; Walder, B.; et al. Standards for definitions and use of outcome measures for clinical effectiveness research in perioperative medicine: European perioperative clinical outcome (epco) definitions: A statement from the esa-esicm. Joint taskforce on perioperative outcome measures. Eur. J. Anaesthesiol. 2015, 32, 88–105. [Google Scholar] [CrossRef] [Green Version]
- Bosaeus, I. Nutritional support in multimodal therapy for cancer cachexia. Support. Care Cancer 2008, 16, 447–451. [Google Scholar] [CrossRef]
- Frasson, M.; Granero-Castro, P.; Rodríguez, J.L.R.; Flor-Lorente, B.; Braithwaite, M.; Martínez, E.M.; Pérez, J.A.Á.; Cazador, A.C.; Espí, A.; Garcia-Granero, E. Risk factors for anastomotic leak and postoperative morbidity and mortality after elective right colectomy for cancer: Results from a prospective, multicentric study of 1102 patients. Int. J. Color. Dis. 2016, 31, 105–114. [Google Scholar] [CrossRef]
- Hu, W.-H.; Eisenstein, S.; Parry, L.; Ramamoorthy, S. Preoperative malnutrition with mild hypoalbuminemia associated with postoperative mortality and morbidity of colorectal cancer: A propensity score matching study. Nutr. J. 2019, 18, 1–7. [Google Scholar] [CrossRef]
- Al-Refaie, W.B.; Parsons, H.M.; Markin, A.; Abrams, J.; Habermann, E.B. Blood transfusion and cancer surgery outcomes: A continued reason for concern. Surgery 2012, 152, 344–354. [Google Scholar] [CrossRef]
- Neto, A.S.; Da Costa, L.G.V.; Hemmes, S.N.; Canet, J.; Hedenstierna, G.; Jaber, S.; Hiesmayr, M.; Hollmann, M.W.; Mills, G.H.; Melo, M.F.V.; et al. The LAS VEGAS risk score for prediction of postoperative pulmonary complications: An observational study. Eur. J. Anaesthesiol. 2018, 35, 691–701. [Google Scholar] [CrossRef]
- Sun, Z.; Kong, X.-J.; Jing, X.; Deng, R.-J.; Tian, Z.-B. Nutritional Risk Screening 2002 as a Predictor of Postoperative Outcomes in Patients Undergoing Abdominal Surgery: A Systematic Review and Meta-Analysis of Prospective Cohort Studies. PLoS ONE 2015, 10, e0132857. [Google Scholar] [CrossRef] [Green Version]
- Okazaki, T.; Ebihara, S.; Mori, T.; Izumi, S.; Ebihara, T. Association between sarcopenia and pneumonia in older people. Geriatr. Gerontol. Int. 2020, 20, 7–13. [Google Scholar] [CrossRef] [Green Version]
- Ginsburg, A.S.; Izadnegahdar, R.; A Berkley, J.; Walson, J.L.; Rollins, N.; Klugman, K.P. Undernutrition and pneumonia mortality. Lancet Glob. Health 2015, 3, e735–e736. [Google Scholar] [CrossRef] [Green Version]
- Xiao, J.; Caan, B.J.; Feliciano, E.M.C.; Meyerhardt, J.A.; Peng, P.D.; Baracos, V.E.; Lee, V.S.; Ely, S.; Gologorsky, R.C.; Weltzien, E.; et al. Association of Low Muscle Mass and Low Muscle Radiodensity with Morbidity and Mortality for Colon Cancer Surgery. JAMA Surg. 2020, 155, 942. [Google Scholar] [CrossRef]
- Chiang, J.; Chang, C.-J.; Jiang, S.; Yeh, C.; You, J.; Hsieh, P.; Huang, H. Pre-operative serum albumin level substantially predicts post-operative morbidity and mortality among patients with colorectal cancer who undergo elective colectomy. Eur. J. Cancer Care 2015, 26, e12403. [Google Scholar] [CrossRef]
- Mullen, J.T.; Moorman, D.W.; Davenport, D.L. The obesity paradox: Body mass index and outcomes in patients undergoing nonbariatric general surgery. Ann. Surg. 2009, 250, 166–172. [Google Scholar] [CrossRef]
- Ramachandran, S.; Nafiu, O.O.; Ghaferi, A.; Tremper, K.K.; Shanks, A.; Kheterpal, S. Independent Predictors and Outcomes of Unanticipated Early Postoperative Tracheal Intubation after Nonemergent, Noncardiac Surgery. Anesthesiology 2011, 115, 44–53. [Google Scholar] [CrossRef] [Green Version]
- Arozullah, A.M.; Khuri, S.F.; Henderson, W.G.; Daley, J. Development and Validation of a Multifactorial Risk Index for Predicting Postoperative Pneumonia after Major Noncardiac Surgery. Ann. Intern. Med. 2001, 135, 847–857. [Google Scholar] [CrossRef]
- Weimann, A.; Braga, M.; Carli, F.; Higashiguchi, T.T.; Hübner, M.; Klek, S.; Laviano, A.; Ljungqvist, O.; Lobo, D.N.; Martindale, R.; et al. ESPEN guideline: Clinical nutrition in surgery. Clin. Nutr. 2017, 36, 623–650. [Google Scholar] [CrossRef] [Green Version]
- Contreras-Bolívar, V.; Torralvo, F.J.S.; Ruiz-Vico, M.; González-Almendros, I.; Barrios, M.; Padín, S.; Alba, E.; Olveira, G. GLIM Criteria Using Hand Grip Strength Adequately Predict Six-Month Mortality in Cancer Inpatients. Nutrients 2019, 11, 2043. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Characteristic | Total (n = 218) | PPCs (n = 48) | No PPCs (n = 170) | p-Value |
|---|---|---|---|---|
| Age (years) | 70.1 ± 13.1 | 73.9 ± 9 | 69 ± 13.9 | 0.23 |
| Sex, male, n (%) | 90 (49) | 21 (43.7) | 69 (40.5) | 0.30 |
| Albumin (g/dL) | 3.87 ± 0.6 | 3.34 ± 0.58 | 3.93 ± 0.59 | <0.05 |
| CRP (mg/dL) | 2.46 ± 3.7 | 3.4 ± 4.5 | 2.2 ± 3.5 | 0.13 |
| Hb (g/dL) | 11.5 ± 1.9 | 10.9 ± 1.8 | 11.7 ± 1.9 | 0.07 |
| Urea (mg/dL) | 42.9 ± 18 | 55.2 ± 23.6 | 39.5 ± 14.6 | <0.001 |
| Creatinine (mg/dL) | 0.95 ± 0.6 | 1.25 ± 1.2 | 0.86 ± 2.4 | <0.05 |
| Comorbidities *, n (%) | 68 (31.1) | 30 (62.5) | 38 (22.3) | <0.001 |
| Respiratory comorbidities | 22 (10) | 14 (29) | 8 (4.7) | <0.001 |
| Cardiovascular comorbidities | 34 (15.6) | 18 (37.5) | 16 (9.4) | <0.01 |
| Metabolic comorbidities | 32 (14.7) | 24 (50) | 8 (4.8) | <0.001 |
| BMI <20 if <70 years or <22 if >70 years | 36 (16.5) | 8 (16.6) | 28 (16.5) | 0.98 |
| Weight loss in past 3–6 months, n (%) | 122 (56) | 36 (75) | 86 (50.6) | <0.01 |
| <5% | 96 (44) | 12 (25) | 84 (49.4) | |
| 5–10% | 74 (34) | 24 (50) | 50 (29.4) | |
| >10% | 48 (22) | 12 (25) | 36 (21.2) | |
| Reduced dietary intake in past week | 118 (54) | 28 (58.3) | 90 (53) | 0.64 |
| Diagnosis of Malnutrition, n (%) | 72 (33.0) | 30 (62.5) | 42 (24.7) | <0.001 |
| Moderate Malnutrition, n (%) | 38 (17.4) | 16 (33.3) | 22 (12.9) | <0.01 |
| Severe Malnutrition, n (%) | 30 (13.7) | 14 (29.1) | 16 (9.5) | <0.01 |
| Underlying condition, n (%) | 0.76 | |||
| Gastric cancer | 44 (20) | 14 (29.2) | 30 (17.6) | |
| Pancreatic cancer | 22 (10) | 8 (16.6) | 14 (8.2) | |
| Hepatic cancer | 12 (5.5) | 4 (8.3) | 8 (4.7) | |
| Colorectal cancer | 128 (59) | 26 (54.2) | 102 (60) | |
| Type of surgical procedure | 0.29 | |||
| Conventional | 168 (77.0) | 38 (80.5) | 130 (74.1) | |
| Laparoscopic | 50 (23.0) | 9 (19.5) | 41 (24.1) | |
| Colorectal resection | 78 (35.7) | 18 (38.5) | 60 (35.2) | |
| Gastric Resection | 30 (13.8) | 4 (9.6) | 26 (17.2) | |
| Small bowel resection | 29 (13.3) | 7 (14.4) | 22 (12.8) | |
| Hepatobiliary resection | 26 (11.9) | 7 (14.4) | 19 (8.7) | |
| Other ** | 55 (25.3) | 13 (27.1) | 42 (24.7) | |
| Length of hospital stay (days) | 20.2 (10.2–30.7) | 26.7 (11.3–31.5) | 18.2 (7.3–32.3) | 0.02 |
| In hospital death, n (%) | 12 (5.5) | 8 (16.6) | 4 (2.3) | <0.01 |
| 90-day all-cause mortality, n (%) | 44 (20.1) | 24 (50) | 20 (11.7) | <0.01 |
| PPCs | 90-Day All-Cause Mortality | |||||
|---|---|---|---|---|---|---|
| Variables | Relative Risk | 95% CI | p | Relative Risk | 95% CI | p |
| Sex (Male vs. Female) | 1.61 | 0.64–4.00 | 0.30 | 1.42 | 1.08–1.76 | 0.02 |
| Age (years) | 1.03 | 0.99–1.08 | 0.11 | 1.75 | 1.09–2.42 | 0.03 |
| Albumin (g/dL) | 0.44 | 0.20–0.94 | 0.03 | 4.24 | 2.20–6.19 | 0.01 |
| C-reactive protein (mg/dL) | 1.07 | 0.96–1.20 | 0.18 | 1.07 | 0.96–1.20 | 0.18 |
| Hb (g/dL) | 0.81 | 0.63–1.03 | 0.08 | 0.82 | 0.58–1.06 | 0.13 |
| Urea (mg/dL) | 1.04 | 1.02–1.07 | <0.01 | 1.52 | 0.76–2.27 | 0.32 |
| Creatinine (mg/dL) | 5.80 | 1.25–26.96 | 0.02 | 3.90 | 0.65–7.45 | 0.27 |
| Respiratory comorbidities (Yes vs. No) | 4.77 | 1.83–12.44 | <0.01 | 4.52 | 1.25–9.85 | <0.01 |
| Malnutrition (Yes vs. No) | 2.34 | 1.66–3.04 | 0.01 | 3.24 | 1.52–5.14 | <0.001 |
| BMI < 20 kg/m2 | 1.01 | 0.30–3.42 | 0.98 | 1.23 | 0.60–1.93 | 0.11 |
| Preoperative weight loss (%) | 1.57 | 0.88–2.79 | 0.12 | 1.85 | 0.44–3.29 | 0.42 |
| Reduced dietary intake in past week (Yes vs. No) | 1.24 | 0.49–3.11 | 0.64 | 1.65 | 0.62–2.68 | 0.32 |
| Variables | Relative Risk | 95% CI | p Value |
|---|---|---|---|
| PPCs * | |||
| Moderate Malnutrition | |||
| Model I | 1.72 | 1.26–2.18 | <0.01 |
| Model II | 1.61 | 1.13–2.09 | <0.01 |
| Severe Malnutrition | |||
| Model I | 1.95 | 1.32–2.56 | <0.01 |
| Model II | 1.82 | 1.21–2.73 | <0.01 |
| Mortality ** | |||
| Moderate Malnutrition | |||
| Model I | 1.92 | 1.25–2.69 | <0.01 |
| Model II | 1.78 | 1.15–2.41 | <0.001 |
| Severe Malnutrition | |||
| Model I | 2.03 | 1.39–2.72 | <0.01 |
| Model II | 1.97 | 1.28–2.63 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kakavas, S.; Karayiannis, D.; Bouloubasi, Z.; Poulia, K.A.; Kompogiorgas, S.; Konstantinou, D.; Vougas, V. Global Leadership Initiative on Malnutrition Criteria Predict Pulmonary Complications and 90-Day Mortality after Major Abdominal Surgery in Cancer Patients. Nutrients 2020, 12, 3726. https://doi.org/10.3390/nu12123726
Kakavas S, Karayiannis D, Bouloubasi Z, Poulia KA, Kompogiorgas S, Konstantinou D, Vougas V. Global Leadership Initiative on Malnutrition Criteria Predict Pulmonary Complications and 90-Day Mortality after Major Abdominal Surgery in Cancer Patients. Nutrients. 2020; 12(12):3726. https://doi.org/10.3390/nu12123726
Chicago/Turabian StyleKakavas, Sotirios, Dimitrios Karayiannis, Zoi Bouloubasi, Kalliopi Anna Poulia, Steven Kompogiorgas, Dimitrios Konstantinou, and Vasileios Vougas. 2020. "Global Leadership Initiative on Malnutrition Criteria Predict Pulmonary Complications and 90-Day Mortality after Major Abdominal Surgery in Cancer Patients" Nutrients 12, no. 12: 3726. https://doi.org/10.3390/nu12123726