High Salt Diet Impacts the Risk of Sarcopenia Associated with Reduction of Skeletal Muscle Performance in the Japanese Population


 ,
,
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Data Collection
2.2.1. Blood Test and Urinalysis
2.2.2. Anthropometric Measurements
2.2.3. Assessment of Physical Performance
2.3. Statistical Analysis
3. Results
3.1. Comparison with Estimated Daily Salt Intake
3.2. Correlation with Estimated Salt Intake
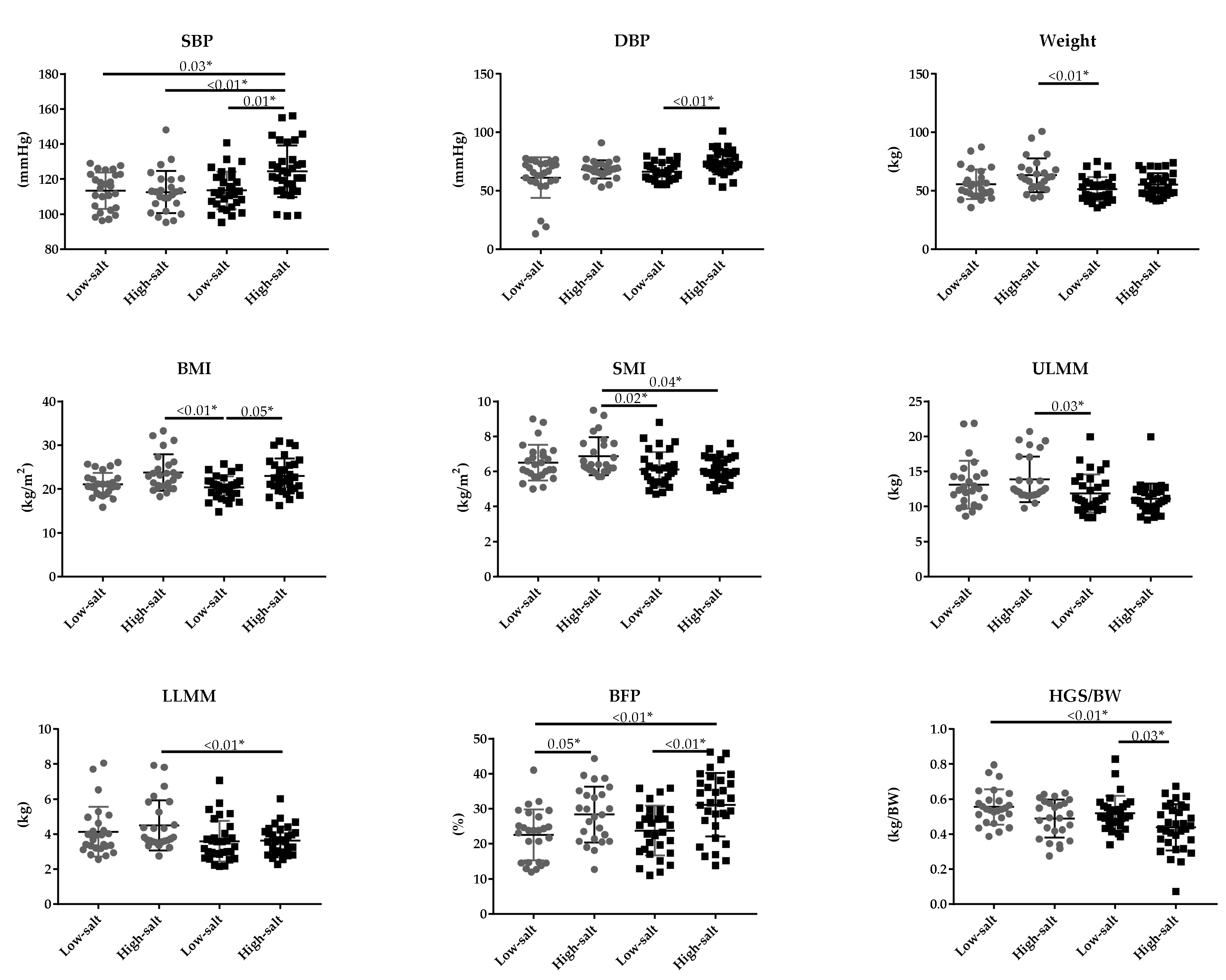
3.3. Comparison of Estimated Salt Intake and Age
3.4. Multivariate Analysis of Estimated Salt Intake and Sarcopenia Parameters
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Aging Society White Paper. 2019. Available online: https://www8.cao.go.jp/kourei/whitepaper/index-w.html (accessed on 31 July 2020).
- Cruz-Jentoft, A.J.; Baeyens, J.P.; Bauer, J.M.; Boirie, Y.; Cederholm, T.; Landi, F.; Martin, F.C.; Michel, J.P.; Rolland, Y.; Schneider, S.M.; et al. Sarcopenia: European consensus on definition and diagnosis: Report of the European Working Group on Sarcopenia in Older People. Age Ageing 2010, 39, 412–423. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, L.K.; Liu, L.K.; Woo, J.; Assantachai, P.; Auyeung, T.W.; Bahyah, K.S.; Chou, M.Y.; Chen, L.Y.; Hsu, P.S.; Krairit, O.; et al. Sarcopenia in Asia: Consensus report of the Asian Working Group for Sarcopenia. J. Am. Med. Dir. Assoc. 2014, 15, 95–101. [Google Scholar] [CrossRef] [PubMed]
- Nishikawa, H.; Shiraki, M.; Hiramatsu, A.; Moriya, K.; Hino, K.; Nishiguchi, S. Japan Society of Hepatology guidelines for sarcopenia in liver disease (1st edition): Recommendation from the working group for creation of sarcopenia assessment criteria. Hepatol. Res. 2016, 46, 951–963. [Google Scholar] [CrossRef] [PubMed]
- Arai, H. Clinical Management of Sarcopenia: Secondary Publication of Geriatrics & Gerontology International 2018;18 S1:1-44. JMA J. 2020, 3, 95–100. [Google Scholar]
- Larsson, L.; Degens, H.; Li, M.; Salviati, L.; Lee, Y.I.; Thompson, W.; Kirkland, J.L.; Sandri, M. Sarcopenia: Aging-Related Loss of Muscle Mass and Function. Physiol. Rev. 2019, 99, 427–511. [Google Scholar] [CrossRef]
- Marzetti, E.; Calvani, R.; Tosato, M.; Cesari, M.; Di Bari, M.; Cherubini, A.; Broccatelli, M.; Savera, G.; D’Elia, M.; Pahor, M.; et al. Physical activity and exercise as countermeasures to physical frailty and sarcopenia. Aging Clin. Exp. Res. 2017, 29, 35–42. [Google Scholar] [CrossRef]
- Beaudart, C.; Dawson, A.; Shaw, S.C.; Harvey, N.C.; Kanis, J.A.; Binkley, N.; Reginster, J.Y.; Chapurlat, R.; Chan, D.C.; Bruyère, O.; et al. Nutrition and physical activity in the prevention and treatment of sarcopenia: Systematic review. Osteoporos. Int. 2017, 28, 1817–1833. [Google Scholar] [CrossRef] [Green Version]
- Steffl, M.; Bohannon, R.W.; Sontakova, L.; Tufano, J.J.; Shiells, K.; Holmerova, I. Relationship between sarcopenia and physical activity in older people: A systematic review and meta-analysis. Clin. Interv. Aging 2017, 12, 835–845. [Google Scholar] [CrossRef] [Green Version]
- Bosaeus, I.; Rothenberg, E. Nutrition and physical activity for the prevention and treatment of age-related sarcopenia. Proc. Nutr. Soc. 2016, 75, 174–180. [Google Scholar] [CrossRef] [Green Version]
- Montero-Fernández, N.; Serra-Rexach, J.A. Role of exercise on sarcopenia in the elderly. Eur. J. Phys. Rehabil. Med. 2013, 49, 131–143. [Google Scholar]
- Cruz-Jentoft, A.J.; Sayer, A.A. Sarcopenia. Lancet 2019, 393, 2636–2646. [Google Scholar] [CrossRef]
- Sieber, C.C. Malnutrition and sarcopenia. Aging Clin. Exp. Res. 2019, 31, 793–798. [Google Scholar] [CrossRef] [PubMed]
- Sinclair, A.J.; Abdelhafiz, A.H.; Rodríguez-Mañas, L. Frailty and sarcopenia newly emerging and high impact complications of diabetes. J. Diabetes Complicat. 2017, 31, 1465–1473. [Google Scholar] [CrossRef] [PubMed]
- Moorthi, R.N.; Avin, K.G. Clinical relevance of sarcopenia in chronic kidney disease. Curr. Opin. Nephrol. Hypertens. 2017, 26, 219–228. [Google Scholar] [CrossRef] [Green Version]
- Watanabe, H.; Enoki, Y.; Maruyama, T. Sarcopenia in Chronic Kidney Disease: Factors, Mechanisms, and Therapeutic Interventions. Biol. Pharm. Bull. 2019, 42, 1437–1445. [Google Scholar] [CrossRef] [Green Version]
- Ponziani, F.R.; Gasbarrini, A. Sarcopenia in Patients with Advanced Liver Disease. Curr. Protein Peptide Sci. 2018, 19, 681–691. [Google Scholar] [CrossRef]
- Kim, J.A.; Choi, K.M. Sarcopenia and fatty liver disease. Hepatol. Int. 2019, 13, 674–687. [Google Scholar] [CrossRef]
- Dasarathy, S.; Merli, M. Sarcopenia from mechanism to diagnosis and treatment in liver disease. J. Hepatol. 2016, 65, 1232–1244. [Google Scholar] [CrossRef] [Green Version]
- Garcia, M.; Seelaender, M.; Sotiropoulos, A.; Coletti, D.; Lancha, A.H., Jr. Vitamin D, muscle recovery, sarcopenia, cachexia, and muscle atrophy. Nutrition 2019, 60, 66–69. [Google Scholar] [CrossRef]
- Naseeb, M.A.; Volpe, S.L. Protein and exercise in the prevention of sarcopenia and aging. Nutr. Res. 2017, 40, 1–20. [Google Scholar] [CrossRef]
- Sodium Intake for Adults and Children Guideline WHO. 2012. Available online: http://apps.who.int/iris/bitstream/10665/77985/1/9789241504836_eng.pdf?ua=1&ua=1 (accessed on 31 July 2020).
- National Health and Nutrition Survey. 2018. Available online: https://www.mhlw.go.jp/stf/newpage_08789.html (accessed on 31 July 2020).
- Rust, P.; Ekmekcioglu, C. Impact of Salt Intake on the Pathogenesis and Treatment of Hypertension. Adv. Exp. Med. Biol. 2017, 956, 61–84. [Google Scholar]
- Aaron, K.J.; Sanders, P.W. Role of dietary salt and potassium intake in cardiovascular health and disease: A review of the evidence. Mayo Clin. Proc. 2013, 88, 987–995. [Google Scholar] [CrossRef] [Green Version]
- Kopp, C.; Linz, P.; Dahlmann, A.; Hammon, M.; Jantsch, J.; Müller, D.N.; Schmieder, R.E.; Cavallaro, A.; Eckardt, K.U.; Uder, M.; et al. 23Na magnetic resonance imaging-determined tissue sodium in healthy subjects and hypertensive patients. Hypertension 2013, 61, 635–640. [Google Scholar] [CrossRef] [Green Version]
- Mandai, S.; Furukawa, S.; Kodaka, M.; Hata, Y.; Mori, T.; Nomura, N.; Ando, F.; Mori, Y.; Takahashi, D.; Yoshizaki, Y.; et al. Loop diuretics affect skeletal myoblast differentiation and exercise-induced muscle hypertrophy. Sci. Rep. 2017, 7, 46369. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsuchiya, Y.; Nakashima, S.; Banno, Y.; Suzuki, Y.; Morita, H. Effect of high-NaCl or high-KCl diet on hepatic Na+- and K+-receptor sensitivity and NKCC1 expression in rats. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2004, 286, R591–R596. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Desir, G.V. Regulation of blood pressure and cardiovascular function by renalase. Kidney Int. 2009, 76, 366–370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Y.; Liu, F.Q.; Wang, D.; Mu, J.J.; Ren, K.Y.; Guo, T.S.; Chu, C.; Wang, L.; Geng, L.K.; Yuan, Z.Y. Effect of salt intake and potassium supplementation on serum renalase levels in Chinese adults: A randomized trial. Medicine 2014, 93, e44. [Google Scholar] [CrossRef] [PubMed]
- Desir, G.V. Renalase deficiency in chronic kidney disease, and its contribution to hypertension and cardiovascular disease. Curr. Opin. Nephrol. Hypertens. 2008, 17, 181–185. [Google Scholar] [CrossRef] [PubMed]
- Desir, G.V. Role of renalase in the regulation of blood pressure and the renal dopamine system. Curr. Opin. Nephrol. Hypertens. 2011, 20, 31–36. [Google Scholar] [CrossRef]
- Tokinoya, K.; Yoshida, Y.; Sugasawa, T.; Takekoshi, K. Moderate-intensity exercise increases renalase levels in the blood and skeletal muscle of rats. FEBS Open Bio 2020. [Google Scholar] [CrossRef] [Green Version]
- Tokinoya, K.; Shiromoto, J.; Sugasawa, T.; Yoshida, Y.; Aoki, K.; Nakagawa, Y.; Ohmori, H.; Takekoshi, K. Influence of acute exercise on renalase and its regulatory mechanism. Life Sci. 2018, 210, 235–242. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, Y.; Sugasawa, T.; Hoshino, M.; Tokinoya, K.; Ishikura, K.; Ohmori, H.; Takekoshi, K. Transient changes in serum renalase concentration during long-distance running: The case of an amateur runner under continuous training. J. Phys. Fit. Sports Med. 2017, 6, 159–166. [Google Scholar] [CrossRef] [Green Version]
- Tokinoya, K.; Shirai, T.; Ota, Y.; Takemasa, T.; Takekoshi, K. Denervation-induced muscle atrophy suppression in renalase-deficient mice via increased protein synthesis. Physiol. Rep. 2020, 8, e14475. [Google Scholar] [CrossRef] [PubMed]
- Sato, S.; Shirato, K.; Tachiyashiki, K.; Imaizumi, K. Muscle plasticity and β₂-adrenergic receptors: Adaptive responses of β₂-adrenergic receptor expression to muscle hypertrophy and atrophy. J. Biomed. Biotechnol. 2011, 2011, 729598. [Google Scholar] [CrossRef]
- Sugiura, T.; Takase, H.; Ohte, N.; Dohi, Y. Dietary Salt Intake is a Significant Determinant of Impaired Kidney Function in the General Population. Kidney Blood Press. Res. 2018, 43, 1245–1254. [Google Scholar] [CrossRef]
- Wang, Y.; Xie, B.Q.; Gao, W.H.; Yan, D.Y.; Zheng, W.L.; Lv, Y.B.; Cao, Y.M.; Hu, J.W.; Yuan, Z.Y.; Mu, J.J. Effects of Renin-Angiotensin System Inhibitors on Renal Expression of Renalase in Sprague-Dawley Rats Fed With High Salt Diet. Kidney Blood Press. Res. 2015, 40, 605–613. [Google Scholar] [CrossRef]
- Horio, M. [Development of evaluation of kidney function and classification of chronic kidney disease (CKD)--including CKD clinical practice guide 2012]. Rinsho Byori. Jpn. J. Clin. Pathol. 2013, 61, 616–621. [Google Scholar]
- Koo, H.S.; Kim, Y.C.; Ahn, S.Y.; Oh, S.W.; Kim, S.; Chin, H.J.; Park, J.H. Estimating 24-hour urine sodium level with spot urine sodium and creatinine. J. Korean Med. Sci. 2014, 29 (Suppl. S2), S97–S102. [Google Scholar] [CrossRef] [Green Version]
- Tanaka, T.; Okamura, T.; Miura, K.; Kadowaki, T.; Ueshima, H.; Nakagawa, H.; Hashimoto, T. A simple method to estimate populational 24-h urinary sodium and potassium excretion using a casual urine specimen. J. Hum. Hypertens. 2002, 16, 97–103. [Google Scholar] [CrossRef] [Green Version]
- Fang, W.H.; Yang, J.R.; Lin, C.Y.; Hsiao, P.J.; Tu, M.Y.; Chen, C.F.; Tsai, D.J.; Su, W.; Huang, G.S.; Chang, H.; et al. Accuracy augmentation of body composition measurement by bioelectrical impedance analyzer in elderly population. Medicine 2020, 99, e19103. [Google Scholar] [CrossRef]
- Wang, H.; Hai, S.; Cao, L.; Zhou, J.; Liu, P.; Dong, B.R. Estimation of prevalence of sarcopenia by using a new bioelectrical impedance analysis in Chinese community-dwelling elderly people. BMC Geriatr. 2016, 16, 216. [Google Scholar] [CrossRef] [Green Version]
- Hiraki, K.; Yasuda, T.; Hotta, C.; Izawa, K.P.; Morio, Y.; Watanabe, S.; Sakurada, T.; Shibagaki, Y.; Kimura, K. Decreased physical function in pre-dialysis patients with chronic kidney disease. Clin. Exp. Nephrol. 2013, 17, 225–231. [Google Scholar] [CrossRef]
- Abro, A.; Delicata, L.A.; Vongsanim, S.; Davenport, A. Differences in the prevalence of sarcopenia in peritoneal dialysis patients using hand grip strength and appendicular lean mass: Depends upon guideline definitions. Eur. J. Clin. Nutr. 2018, 72, 993–999. [Google Scholar] [CrossRef] [PubMed]
- Yeung, S.S.Y.; Reijnierse, E.M.; Trappenburg, M.C.; Blauw, G.J.; Meskers, C.G.M.; Maier, A.B. Knee extension strength measurements should be considered as part of the comprehensive geriatric assessment. BMC Geriatr. 2018, 18, 130. [Google Scholar] [CrossRef] [PubMed]
- Ratkevicius, A.; Joyson, A.; Selmer, I.; Dhanani, T.; Grierson, C.; Tommasi, A.M.; DeVries, A.; Rauchhaus, P.; Crowther, D.; Alesci, S.; et al. Serum concentrations of myostatin and myostatin-interacting proteins do not differ between young and sarcopenic elderly men. J. Gerontol. Ser. A 2011, 66, 620–626. [Google Scholar] [CrossRef] [PubMed]
- Hofmann, M.; Halper, B.; Oesen, S.; Franzke, B.; Stuparits, P.; Tschan, H.; Bachl, N.; Strasser, E.M.; Quittan, M.; Ploder, M.; et al. Serum concentrations of insulin-like growth factor-1, members of the TGF-beta superfamily and follistatin do not reflect different stages of dynapenia and sarcopenia in elderly women. Exp. Gerontol. 2015, 64, 35–45. [Google Scholar] [CrossRef] [PubMed]
- Vieira, N.D.; Testa, D.; Ruas, P.C.; Salvini, T.F.; Catai, A.M.; De Melo, R.C. The effects of 12 weeks Pilates-inspired exercise training on functional performance in older women: A randomized clinical trial. J. Bodyw. Mov. Ther. 2017, 21, 251–258. [Google Scholar] [CrossRef] [PubMed]
- Krupp, S.; Kasper, J.; Hermes, A.; Balck, F.; Ralf, C.; Schmidt, T.; Weisser, B.; Willkomm, M. The "Lübeck Worlds of Movement Model"-results of the effects evaluation. Bundesgesundheitsblatt Gesundh. Gesundh 2019, 62, 274–281. [Google Scholar] [CrossRef]
- Mijnarends, D.M.; Meijers, J.M.; Halfens, R.J.; Ter Borg, S.; Luiking, Y.C.; Verlaan, S.; Schoberer, D.; Cruz Jentoft, A.J.; Van Loon, L.J.; Schols, J.M. Validity and reliability of tools to measure muscle mass, strength, and physical performance in community-dwelling older people: A systematic review. J. Am. Med. Dir. Assoc. 2013, 14, 170–178. [Google Scholar] [CrossRef]
- Jones, C.J.; Rikli, R.E.; Beam, W.C. A 30-s chair-stand test as a measure of lower body strength in community-residing older adults. Res. Q. Exerc. Sport 1999, 70, 113–119. [Google Scholar] [CrossRef]
- Asakura, K.; Uechi, K.; Sasaki, Y.; Masayasu, S.; Sasaki, S. Estimation of sodium and potassium intakes assessed by two 24 h urine collections in healthy Japanese adults: A nationwide study. Br. J. Nutr. 2014, 112, 1195–1205. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, B.F.; Stamler, J.; Dennis, B.; Moag-Stahlberg, A.; Okuda, N.; Robertson, C.; Zhao, L.; Chan, Q.; Elliott, P. Nutrient intakes of middle-aged men and women in China, Japan, United Kingdom, and United States in the late 1990s: The INTERMAP study. J. Hum. Hypertens. 2003, 17, 623–630. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, L.; Stamler, J.; Chan, Q.; Van Horn, L.; Daviglus, M.L.; Dyer, A.R.; Miura, K.; Okuda, N.; Wu, Y.; Ueshima, H.; et al. Salt intake and prevalence of overweight/obesity in Japan, China, the United Kingdom, and the United States: The INTERMAP Study. Am. J. Clin. Nutr. 2019, 110, 34–40. [Google Scholar] [CrossRef] [PubMed]
- Lanaspa, M.A.; Kuwabara, M.; Andres-Hernando, A.; Li, N.; Cicerchi, C.; Jensen, T.; Orlicky, D.J.; Roncal-Jimenez, C.A.; Ishimoto, T.; Nakagawa, T.; et al. High salt intake causes leptin resistance and obesity in mice by stimulating endogenous fructose production and metabolism. Proc. Natl. Acad. Sci. USA 2018, 115, 3138–3143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ma, Y.; He, F.J.; MacGregor, G.A. High salt intake: Independent risk factor for obesity? Hypertension 2015, 66, 843–849. [Google Scholar] [CrossRef]
- Wannamethee, S.G.; Atkins, J.L. Muscle loss and obesity: The health implications of sarcopenia and sarcopenic obesity. Proc. Nutr. Soc. 2015, 74, 405–412. [Google Scholar] [CrossRef]
- Oku, Y.; Tanabe, R.; Nakaoka, K.; Yamada, A.; Noda, S.; Hoshino, A.; Haraikawa, M.; Goseki-Sone, M. Influences of dietary vitamin D restriction on bone strength, body composition and muscle in rats fed a high-fat diet: Involvement of mRNA expression of MyoD in skeletal muscle. J. Nutr. Biochem. 2016, 32, 85–90. [Google Scholar] [CrossRef]
- Conte, M.; Vasuri, F.; Trisolino, G.; Bellavista, E.; Santoro, A.; Degiovanni, A.; Martucci, E.; D’Errico-Grigioni, A.; Caporossi, D.; Capri, M.; et al. Increased Plin2 expression in human skeletal muscle is associated with sarcopenia and muscle weakness. PLoS ONE 2013, 8, e73709. [Google Scholar] [CrossRef] [Green Version]
- Majid, H.; Masood, Q.; Khan, A.H. Homeostatic Model Assessment for Insulin Resistance (HOMA-IR): A Better Marker for Evaluating Insulin Resistance than Fasting Insulin in Women with Polycystic Ovarian Syndrome. JCPSP 2017, 27, 123–126. [Google Scholar]
- Kim, H.K.; Lee, Y.J.; Lee, Y.K.; Kim, H.; Koo, K.H. Which Index for Muscle Mass Represents an Aging Process? J. Bone Metab. 2018, 25, 219–226. [Google Scholar] [CrossRef] [PubMed]
- Dodds, R.M.; Granic, A.; Robinson, S.M.; Sayer, A.A. Sarcopenia, long-term conditions, and multimorbidity: Findings from UK Biobank participants. J. Cachexia Sarcopenia Muscle 2020, 11, 62–68. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
{kind=link}
| Low—Salt | High—Salt | Normality p value | T Test | |
|---|---|---|---|---|
| p Value | ||||
| Sample size (n) | 57 | 57 | - | - |
| Salt intake (g/day) | 7.62(1.31) | 11.11(1.16) | 0.63 | <0.01 * |
| Male/Female (n/n) | 11/46 | 8/49 | - | 0.45 ✝ |
| Age (year) § | 56.00[49.00–63.00] | 56.00[50.5–65.00] | <0.01 * | 0.60 |
| SBP (mmHg) § | 113.00[104.33–122.00] | 117.33[110.33–128.00] | <0.01 * | 0.05 * |
| DBP (mmHg) § | 65.67[60.00–73.00] | 70.33[66.17–76.00] | 0.04 * | 0.01 * |
| Height (m) § | 1.59 [1.53–1.66] | 1.57[1.52–1.61] | <0.01 * | 0.28 |
| Weight (kg) § | 51.20[45.30–58.30] | 57.60[48.75–66.25] | <0.01 * | 0.01 * |
| BMI (kg/m2) § | 20.61[18.88–21.89] | 22.69[20.28–25.58] | <0.01 * | <0.01 * |
| SMI (kg/m2) § | 6.10[5.50–6.90] | 6.20[5.80–6.85] | <0.01 * | 0.34 |
| ULMM (kg) § | 3.56[2.95–4.32] | 3.67[3.24–4.35] | <0.01 * | 0.24 |
| LLMM (kg) § | 11.69[10.04–14.19] | 11.78[10.44–12.82] | <0.01 * | 0.88 |
| BFP (%) | 23.21(7.15) | 29.91(8.65) | 0.10 | <0.01 * |
| HGS/BW (kg/BW) | 0.54(0.10) | 0.46(0.12) | 0.23 | <0.01 * |
| KES/BW (kg/BW) | 0.62(0.17) | 0.57(0.16) | 0.16 | 0.13 |
| SLT (sec) § | 60.00[48.05–60.00] | 60.00[38.24–60.00] | <0.01 * | 0.72 |
| MGS (m/sec) § | 2.28[2.04–2.61] | 2.18[1.99–2.44] | <0.01 * | 0.14 |
| Flex (m) | 0.39(9.08) | 0.36(7.54) | 0.75 | 0.04 * |
| 30CS (time) § | 24.00[19.00–29.00] | 18.00[16.00–23.00] | <0.01 * | <0.01 * |
| Renalase (mg/L) § | 4.26[2.93–5.46] | 4.24[3.30–5.38] | <0.01 * | 0.90 |
| IL-6 (pg/mL) § | 1.00[0.65–1.20] | 1.20[0.90–1.90] | <0.01 * | <0.01 * |
| UN (mg/dL) | 14.04(2.81) | 13.07(2.61) | 0.10 | 0.06 |
| CysC (mg/L) § | 0.65[0.61–0.69] | 0.67[0.62–0.70] | <0.01 * | 0.27 |
| TG (mg/dL) § | 61.00[46.00–78.00] | 83.00[59.50–100.50] | <0.01 * | <0.01 * |
| Alb (g/dL) | 4.53(0.30) | 4.51(0.26) | 0.10 | 0.77 |
| Glu (mg/dL) § | 96.00[91.00–106.00] | 99.00[92.50–104.00] | <0.01 * | 0.28 |
| Insulin (μU/mL) § | 3.90[2.90–6.10] | 4.90[3.75–7.15] | <0.01 * | 0.02 * |
| HbA1c (%) | 5.61(0.33) | 5.69(0.38) | 0.11 | 0.27 |
| AST (U/L) | 22.93(4.93) | 24.11(5.03) | 0.70 | 0.21 |
| ALT (U/L) § | 17.00[14.00–19.00] | 18.00[15.00–27.00] | <0.01 * | 0.05 * |
| Correlation Coefficient | ||
|---|---|---|
| p value | r value | |
| Age (year) § | 0.54 | - |
| SBP (mmHg) § | 0.03 * | 0.21 |
| DBP (mmHg) § | 0.07 | - |
| Height (m) § | 0.74 | - |
| Weight (kg) § | <0.01 * | 0.39 |
| BMI (kg/m2) § | <0.01 * | 0.49 |
| SMI (kg/m2) § | 0.03 * | 0.21 |
| ULMM (kg) § | 0.01 * | 0.24 |
| LLMM (kg) § | 0.42 | |
| BFP (%) | <0.01 * | 0.49 |
| HGS/BW (kg/BW) | <0.01 * | −0.38 |
| KES/BW (kg/BW) | 0.14 | − |
| SLT (sec)§ | 0.46 | − |
| MGS (m/sec) § | 0.24 | − |
| Flex (m) | 0.03 * | −0.20 |
| 30CS (time) § | <0.01 * | −0.32 |
| Renalase (mg/L) § | 0.67 | − |
| IL-6 (pg/mL) § | <0.01 * | 0.31 |
| UN (mg/dL) | 0.25 | − |
| CysC (mg/L) § | 0.15 | − |
| TG (mg/dL) § | <0.01 | 0.34 |
| Alb (g/dL) | 0.67 | − |
| Glu (mg/dL) § | 0.11 | − |
| Insulin (μU/mL) § | <0.01 * | 0.27 |
| HbA1c (%) | 0.12 | − |
| AST (U/L) | 0.51 | − |
| ALT (U/L) § | 0.02 * | 0.21 |
| Younger Low—Salt | Younger High—Salt | Older Low—Salt | Older High—Salt | p value | |
|---|---|---|---|---|---|
| Sample size (n) | 26 | 25 | 31 | 32 | – |
| Salt intake (g/day) | 7.56(1.19) | 11.01(1.08) | 7.67(1.42) | 11.19(1.23) | – |
| Male/Female (n) | 5/21 | 6/19 | 6/25 | 2/30 | – |
| Age (year) § | 48.50[37.75–53.00] | 50.00[44.50–54.00] | 62.00[58.00–71.00] | 65.00[60.25–67.00] | – |
| SBP (mmHg) § | 115.33[103.33–122.67] | 112.67[103.83–119.83] | 112.33[105.75–121.00] | 122.50[113.67–130.75] | <0.01 * |
| DBP (mmHg) § | 68.17[60.50–73.75] | 68.33[64.17–72.50] | 65.33[59.67–71.67] | 72.67[67.83–81.50] | <0.01 * |
| Weight (kg) § | 52.50[46.23–62.33] | 61.50[52.80–69.00] | 47.00[44.80–56.80] | 51.15[47.83–62.13] | <0.01 * |
| BMI (kg/m2) § | 20.61[19.00–22.50] | 23.10[20.50–25.86] | 20.45[18.27–21.83] | 22.20[20.00–25.61] | <0.01 * |
| SMI (kg/m2) § | 6.25[5.78–7.10] | 6.40[6.05–7.60] | 6.00[5.40–6.70] | 5.95[5.63–6.78] | 0.01 * |
| ULMM (kg) § | 3.81[3.19–4.71] | 3.82[3.56–5.55] | 3.28[2.86–4.04] | 3.61[2.90–4.13] | 0.03 * |
| LLMM (kg) § | 12.44[10.21–14.43] | 12.27[11.67–17.10] | 11.04[9.92–13.63] | 10.86[9.91–12.15] | <0.01 * |
| BFP (%) | 22.54(7.31) | 28.38(7.98) | 23.76(7.08) | 31.12(9.07) | <0.01 * |
| HGS/BW (kg/BW) | 0.56(0.10) | 0.49(0.11) | 0.52(0.10) | 0.44(0.13) | <0.01 * |
| KES/BW (kg/BW) | 0.64(0.20) | 0.62(0.16) | 0.60(0.14) | 0.53(0.16) | 0.08 |
| SLT (sec) § | 60.00[60.00–60.00] | 60.00[48.35–60.00] | 60.00[25.12–60.00] | 60.00[37.51–60.00] | 0.23 |
| MGS (m/sec) § | 2.34[2.13–2.79] | 2.25[2.05–2.73] | 2.24[1.95–2.59] | 2.13[1.81–2.33] | 0.05 |
| Flex (m) | 0.39(0.10) | 0.36(0.09) | 0.38(0.11) | 0.35(0.07) | 0.44 |
| 30CS (time) § | 24.00[19.75–29.00] | 20.00[16.00–23.00] | 21.00[18.00–29.00] | 17.50[16.00–22.00] | <0.01 * |
| Renalase (mg/L) § | 3.71[2.78–6.30] | 4.85[2.71–6.28] | 4.40[3.37–5.12] | 4.13[3.45–4.95] | 0.73 |
| IL-6 (pg/mL) § | 0.80[0.60–1.03] | 0.90[0.75–1.45] | 1.00[0.70–1.30] | 1.70[1.10–2.08] | <0.01 * |
| UN (mg/dL) | 13.23(2.87) | 12.54(2.29) | 14.72(2.62) | 13.49(2.79) | 0.02 * |
| CysC (mg/L) § | 0.63[0.61–0.68] | 0.66[0.61–0.69] | 0.65[0.62–0.70] | 0.68[0.61–0.70] | 0.43 |
| TG (mg/dL) § | 65.50[46.50–81.75] | 84.00[52.50–95.00] | 58.00[43.00–78.00] | 82.50[66.25–105.75] | 0.01 * |
| Alb (g/dL) | 4.50(0.29) | 4.54(0.24) | 4.55(0.32) | 4.49(0.27) | 0.74 |
| Glu (mg/dL) § | 93.00[87.50–99.25] | 97.00[90.50–100.50] | 99.00[94.00–108.00] | 100.00[94.25–107.75] | 0.02 * |
| insulin (μU/mL) § | 4.05[2.98–5.95] | 4.90[3.55–6.55] | 3.70[2.70–6.80] | 5.00[3.98–7.45] | 0.10 |
| HbA1c (%) | 5.48(0.29) | 5.55(0.31) | 5.73(0.32) | 5.79(0.39) | <0.01 * |
| AST (U/L) | 21.19(4.50) | 23.36(5.06) | 24.39(4.87) | 24.69(5.01) | 0.04 * |
| ALT (U/L) § | 16.00[12.00–17.25] | 19.00[15.00–29.50] | 18.00[15.00–21.00] | 16.00[15.00–26.75] | 0.05 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yoshida, Y.; Kosaki, K.; Sugasawa, T.; Matsui, M.; Yoshioka, M.; Aoki, K.; Kuji, T.; Mizuno, R.; Kuro-o, M.; Yamagata, K.; et al. High Salt Diet Impacts the Risk of Sarcopenia Associated with Reduction of Skeletal Muscle Performance in the Japanese Population. Nutrients 2020, 12, 3474. https://doi.org/10.3390/nu12113474
Yoshida Y, Kosaki K, Sugasawa T, Matsui M, Yoshioka M, Aoki K, Kuji T, Mizuno R, Kuro-o M, Yamagata K, et al. High Salt Diet Impacts the Risk of Sarcopenia Associated with Reduction of Skeletal Muscle Performance in the Japanese Population. Nutrients. 2020; 12(11):3474. https://doi.org/10.3390/nu12113474
Chicago/Turabian StyleYoshida, Yasuko, Keisei Kosaki, Takehito Sugasawa, Masahiro Matsui, Masaki Yoshioka, Kai Aoki, Tomoaki Kuji, Risuke Mizuno, Makoto Kuro-o, Kunihiro Yamagata, and et al. 2020. "High Salt Diet Impacts the Risk of Sarcopenia Associated with Reduction of Skeletal Muscle Performance in the Japanese Population" Nutrients 12, no. 11: 3474. https://doi.org/10.3390/nu12113474