The Role of Dietary Fibre in Modulating Gut Microbiota Dysbiosis in Patients with Type 2 Diabetes: A Systematic Review and Meta-Analysis of Randomised Controlled Trials


Abstract
:1. Introduction
2. Description of the Intervention
3. How the Intervention Might Work
4. Why It Is Important to Do This Review
4.1. Aim
4.2. Methods
4.3. Types of Studies
4.4. Types of Participants
4.5. Types of Interventions
4.6. Types of Outcome Measures
4.7. Search Methods for Identification of Studies
4.8. Data Collection and Analysis
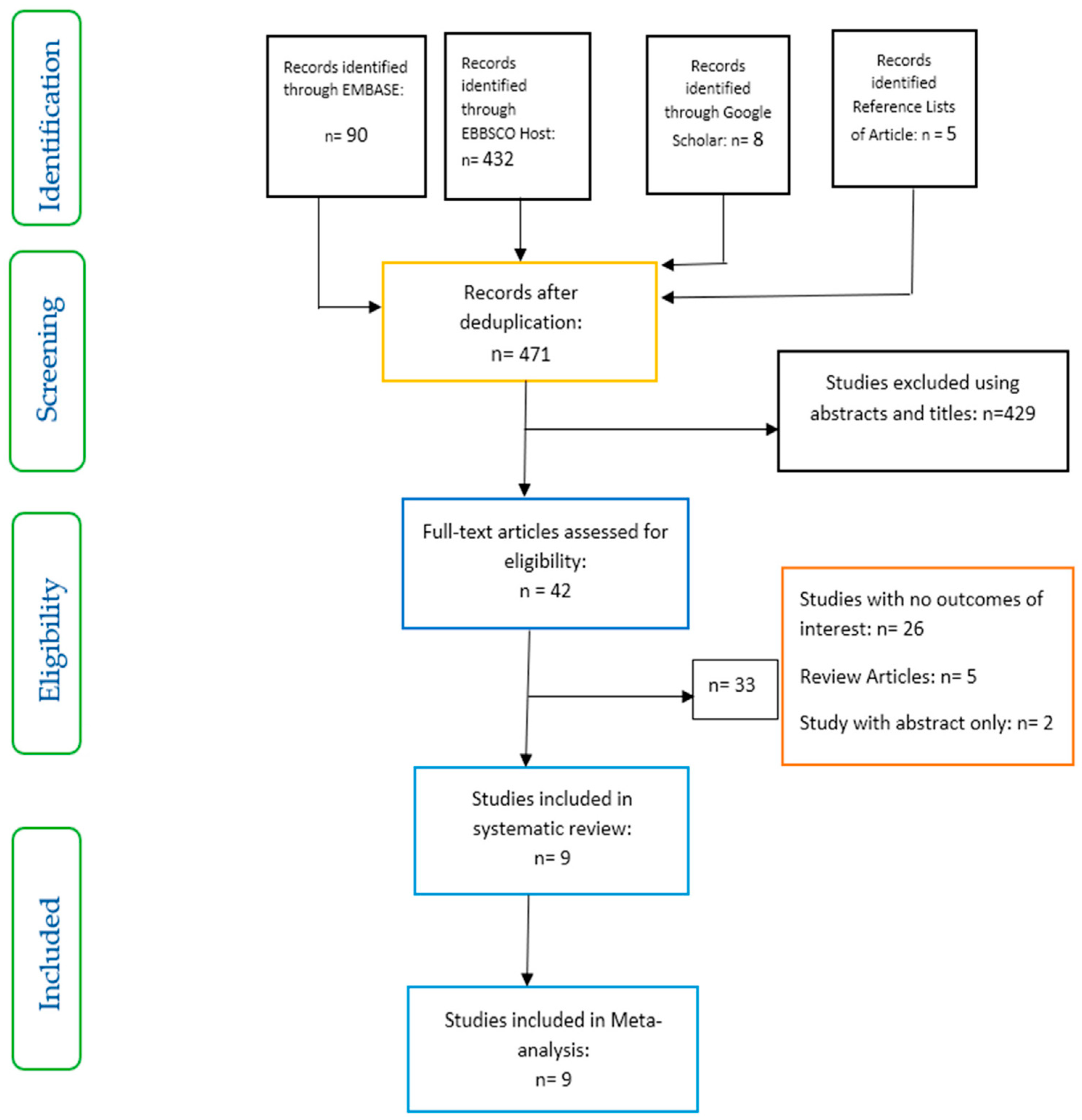
4.8.1. Selection of Studies
4.8.2. Data Extraction and Management
4.8.3. Assessment of Risk of Bias and Quality of Included Studies
4.8.4. Data Analysis
4.8.5. Effect Size
5. Results
5.1. Risk of Bias in Included Studies
5.2. Effects of Interventions
5.3. The Effect of Dietary Fibre on Gut Microbiota
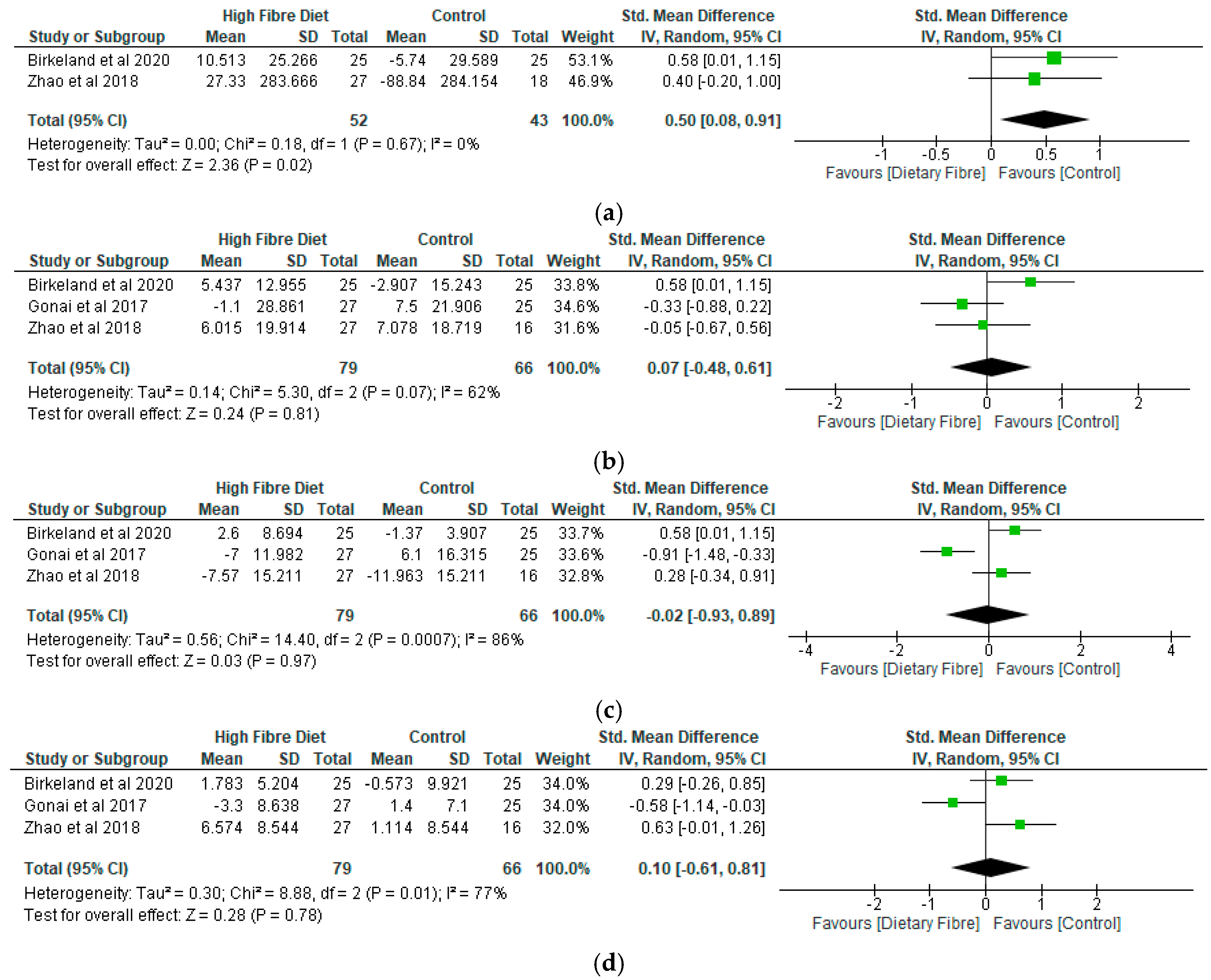
5.4. The Role of Dietary Fibre on Short-Chain Fatty Acids
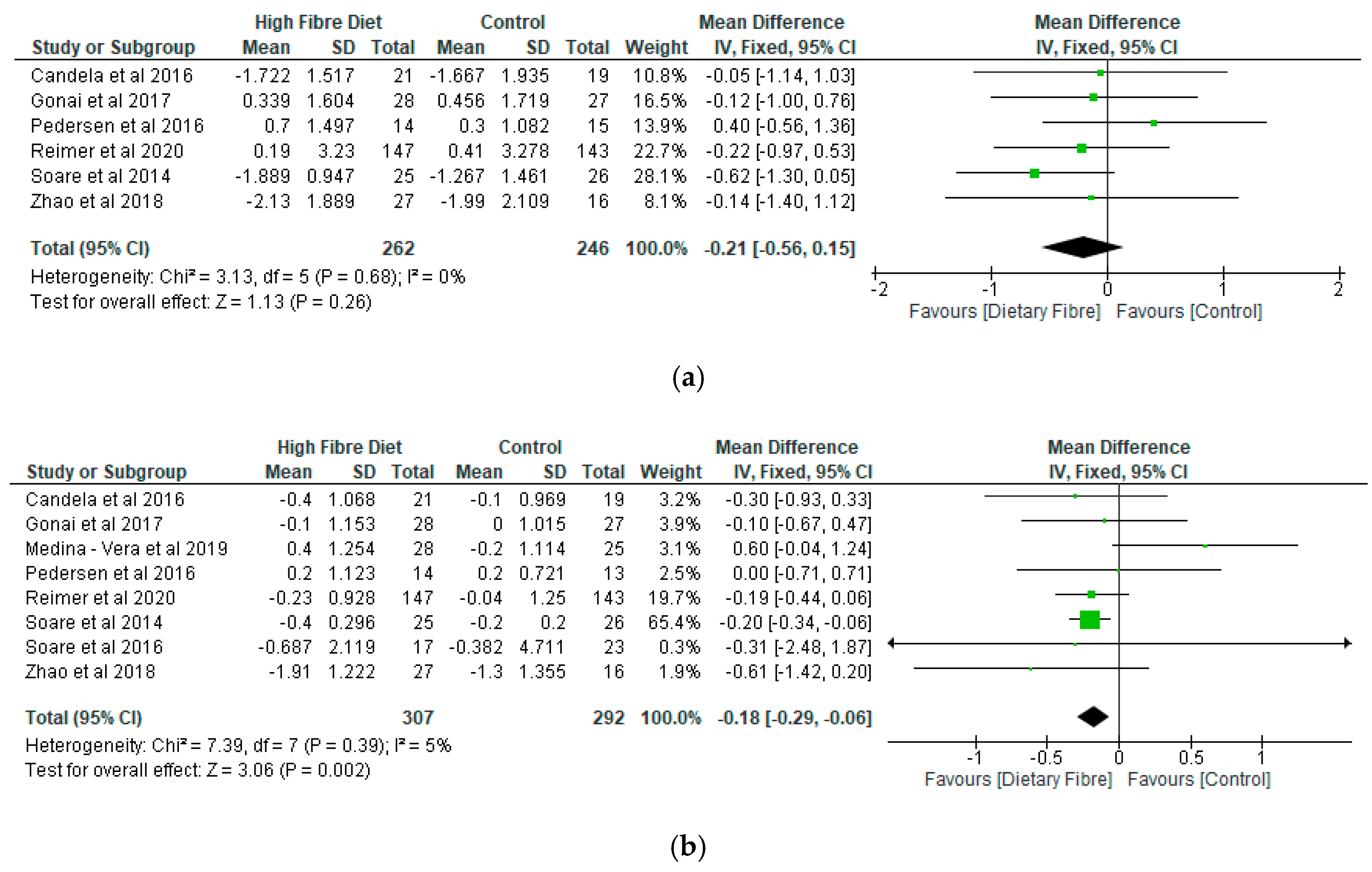
5.5. Glycaemic Control
5.6. Adverse Events
6. Discussion
7. Limitation of the Review
8. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- National Institute for Health and Care Excellence (NICE). Type 2 Diabetes in Adults: Management. 2015. Available online: https://www.nice.org.uk/guidance/ng28 (accessed on 1 August 2020).
- Woldeamlak, B.; Yirdaw, K.; Biadgo, B. Role of Gut Microbiota in Type 2 Diabetes Mellitus and Its Complications: Novel Insights and Potential Intervention Strategies. Korean J. Gastroenterol. Taehan Sohwagi Hakhoe Chi 2019, 74, 314–320. [Google Scholar] [CrossRef]
- World Health Organization. Global Report on Diabetes. 2016. Available online: https://apps.who.int/iris/bitstream/handle/10665/204871/9789241565257_eng.pdf;jsessionid=7EAFAD731DC646D9605E3539F423CDD0?sequence=1 (accessed on 1 August 2020).
- Roshanravan, N.; Alamdari, N.M.; Jafarabadi, M.A.; Mohammadi, A.; Shabestari, B.R.; Nasirzadeh, N.; Asghari, S.; Mansoori, B.; Akbarzadeh, M.; Ghavami, A.; et al. Effects of oral butyrate and inulin supplementation on inflammation-induced pyroptosis pathway in type 2 diabetes: A randomized, double-blind, placebo-controlled trial. Cytokine 2020, 131, 155101. [Google Scholar] [CrossRef]
- Ojo, O. An overview of diabetes and its complications. Diabetes Res. Open J. 2016, 2, e4–e6. [Google Scholar] [CrossRef]
- Ebrahimzadeh Leylabadlo, H.; Sanaie, S.; Sadeghpour Heravi, F.; Ahmadian, Z.; Ghotaslou, R. From role of gut microbiota to microbial-based therapies in type 2-diabetes. Infect. Genet. Evol. 2020, 81. [Google Scholar] [CrossRef] [PubMed]
- Makki, K.; Deehan, E.C.; Walter, J.; Bäckhed, F. The Impact of Dietary Fiber on Gut Microbiota in Host Health and Disease. Cell Host Microbe 2018, 23, 705–715. [Google Scholar] [CrossRef] [Green Version]
- Department of Health. Dietary Reference Values for Food Energy and Nutrients for the United Kingdom. 1991. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/743786/Dietary_Reference_Values_for_Food_Energy_and_Nutrients_for_the_United_Kingdom__1991_.pdf (accessed on 16 August 2020).
- Scientific Advisory Committee on Nutrition. Statement on Dietary Fibre. 2008. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/339367/SACN_Draft_position_statement_on_dietary_fibre_and_health_and_dietary_fibre_definition_2008.pdf (accessed on 16 August 2020).
- Scientific Advisory Committee on Nutrition. Carbohydrate and Health. 2015. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/445503/SACN_Carbohydrates_and_Health.pdf (accessed on 16 August 2020).
- Healey, G.; Murphy, R.; Butts, C.; Brough, L.; Whelan, K.; Coad, J. Habitual dietary fibre intake influences gut microbiota response to an inulin-type fructan prebiotic: A randomised, double-blind, placebo-controlled, cross-over, human intervention study. Br. J. Nutr. 2018, 119, 176–189. [Google Scholar] [CrossRef]
- Duvallet, C.; Gibbons, S.M.; Gurry, T.; Irizarry, R.A.; Alm, E.J. Meta-analysis of gut microbiome studies identifies disease-specific and shared responses. Nat. Commun. 2017, 8, 1784. [Google Scholar] [CrossRef] [Green Version]
- Zhao, L.; Zhang, F.; Ding, X.; Wu, G.; Lam, Y.Y.; Wang, X.; Fu, H.; Xue, X.; Lu, C.; Ma, J.; et al. Gut bacteria selectively promoted by dietary fibers alleviate type 2 diabetes. Science 2018, 359, 1151–1156. [Google Scholar] [CrossRef] [Green Version]
- Lee, S.E.; Choi, Y.; Jun, J.E.; Lee, Y.B.; Jin, S.M.; Hur, K.Y.; Ko, G.P.; Lee, M.K. Additional Effect of Dietary Fiber in Patients with Type 2 Diabetes Mellitus Using Metformin and Sulfonylurea: An Open-Label, Pilot Trial. Diabetes Metab. J. 2019, 43, 422–431. [Google Scholar] [CrossRef]
- Ahmad, A.; Yang, W.; Chen, G.; Shafiq, M.; Javed, S.; Ali Zaidi, S.S.; Shahid, R.; Liu, C.; Bokhari, H. Analysis of gut microbiota of obese individuals with type 2 diabetes and healthy individuals. PLoS ONE 2019, 14, e0226372. [Google Scholar] [CrossRef] [Green Version]
- Tsai, Y.-L.; Lin, T.-L.; Chang, C.-J.; Wu, T.-R.; Lai, W.-F.; Lu, C.-C.; Lai, H.-C. Probiotics, prebiotics and amelioration of diseases. J. Biomed. Sci. 2019, 26, 3. [Google Scholar] [CrossRef]
- Houghton, D.; Hardy, T.; Stewart, C.; Errington, L.; Day, C.P.; Trenell, M.I.; Avery, L. Systematic review assessing the effectiveness of dietary intervention on gut microbiota in adults with type 2 diabetes. Diabetologia 2018, 61, 1700–1711. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar]
- Methley, A.M.; Campbell, S.; Chew-Graham, C.; McNally, R.; Cheraghi-Sohi, S. PICO, PICOS and SPIDER: A comparison study of specificity and sensitivity in three search tools for qualitative systematic reviews. BMC Health Serv. Res. 2014, 14, 579. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.T.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions; Wiley-Blackwell: Hoboken, NJ, USA, 2009. [Google Scholar]
- Mitchell, M.; Muftakhidinov, B.; Winchen, T. Engauge Digitizer Software. 2020. Available online: http://markummitchell.github.io/engauge-digitizer (accessed on 21 September 2020).
- Medina-Vera, I.; Sanchez-Tapia, M.; Noriega-López, L.; Granados-Portillo, O.; Guevara-Cruz, M.; Flores-López, A.; Avila-Nava, A.; Fernández, M.L.; Tovar, A.R.; Torres, N. A dietary intervention with functional foods reduces metabolic endotoxaemia and attenuates biochemical abnormalities by modifying faecal microbiota in people with type 2 diabetes. Diabetes Metab. 2019, 45, 122–131. [Google Scholar] [CrossRef]
- Pedersen, C.; Wu, H.; Jaiyeola, E.; Diribe, O.; La Ragione, R.; Robertson, M.D.; Wright, J.; Gallagher, E.; Horton, F.; Hinton, P.; et al. Host–microbiome interactions in human type 2 diabetes following prebiotic fibre (galacto-oligosaccharide) intake. Br. J. Nutr. 2016, 116, 1869–1877. [Google Scholar] [CrossRef] [Green Version]
- The Nordic Cochrane Centre. Review Manager (RevMan) [Computer Program]; Version 5.3; The Nordic Cochrane Centre, The Cochrane Collaboration: Copenhagen, Denmark, 2014. [Google Scholar]
- Critical Appraisal Skills Programme (CASP). CASP Randomised Controlled Trial Checklist. Available online: https://casp-uk.net/wp-content/uploads/2018/03/CASP-Randomised-Controlled-Trial-Checklist-2018_fillable_form.pdf (accessed on 8 September 2020).
- Candela, M.; Biagi, E.; Soverini, M.; Consolandi, C.; Quercia, S.; Severgnini, M.; Peano, C.; Turroni, S.; Rampelli, S.; Pozzilli, P.; et al. Modulation of gut microbiota dysbioses in type 2 diabetic patients by macrobiotic Ma-Pi 2 diet. Br. J. Nutr. 2016, 116, 80–93. [Google Scholar] [CrossRef] [Green Version]
- Soare, A.; Khazrai, Y.M.; Del Toro, R.; Roncella, E.; Fontana, L.; Fallucca, S.; Angeletti, S.; Formisano, V.; Capata, F.; Ruiz, V.; et al. The effect of the macrobiotic Ma-Pi 2 diet vs. the recommended diet in the management of type 2 diabetes: The randomized controlled MADIAB trial. Nutr. Metab. 2014, 11, 39. [Google Scholar] [CrossRef] [Green Version]
- Soare, A.; Del Toro, R.; Khazrai, Y.M.; Di Mauro, A.; Fallucca, S.; Angeletti, S.; Skrami, E.; Gesuita, R.; Tuccinardi, D.; Manfrini, S.; et al. A 6-month follow-up study of the randomized controlled Ma-Pi macrobiotic dietary intervention (MADIAB trial) in type 2 diabetes. Nutr. Diabetes 2016, 6, e222. [Google Scholar] [CrossRef] [Green Version]
- Birkeland, E.; Gharagozlian, S.; Birkeland, K.I.; Valeur, J.; Måge, I.; Rud, I.; Aas, A.-M. Prebiotic effect of inulin-type fructans on faecal microbiota and short-chain fatty acids in type 2 diabetes: A randomised controlled trial. Eur. J. Nutr. 2020. [Google Scholar] [CrossRef]
- Gonai, M.; Shigehisa, A.; Kigawa, I.; Kurasaki, K.; Chonan, O.; Matsuki, T.; Yoshida, Y.; Aida, M.; Hamano, K.; Terauchi, Y. Galacto-oligosaccharides ameliorate dysbiotic Bifidobacteriaceae decline in Japanese patients with type 2 diabetes. Benef. Microbes 2017, 8, 705–716. [Google Scholar] [CrossRef]
- Reimer, R.A.; Wharton, S.; Green, T.J.; Manjoo, P.; Ramay, H.R.; Lyon, M.R.; Gahler, R.J.; Wood, S. Effect of a functional fibre supplement on glycemic control when added to a year-long medically supervised weight management program in adults with type 2 diabetes. Eur. J. Nutr. 2020. [Google Scholar] [CrossRef]
- Fallucca, F.; Fontana, L.; Fallucca, S.; Pianesi, M. Gut microbiota and Ma-Pi 2 macrobiotic diet in the treatment of type 2 diabetes. World J. Diabetes 2015, 6, 403–411. [Google Scholar] [CrossRef]
- Lozupone, C.A.; Stombaugh, J.; Gonzalez, A.; Ackermann, G.; Wendel, D.; Vázquez-Baeza, Y.; Jansson, J.K.; Gordon, J.I.; Knight, R. Meta-analyses of studies of the human microbiota. Genome Res. 2013, 23, 1704–1714. [Google Scholar] [CrossRef] [Green Version]
- Fallucca, F.; Porrata, C.; Fallucca, S.; Pianesi, M. Influence of diet on gut microbiota, inflammation and type 2 diabetes mellitus. First experience with macrobiotic Ma-Pi 2 diet. Diabetes/Metab. Res. Rev. 2014, 30, 48–54. [Google Scholar] [CrossRef]
- Gurung, M.; Li, Z.; You, H.; Rodrigues, R.; Jump, D.B.; Morgun, A.; Shulzhenko, N. Role of gut microbiota in type 2 diabetes pathophysiology. EBioMedicine 2020, 51, 102590. [Google Scholar] [CrossRef] [Green Version]
- Davison, K.M.; Temple, N.J. Cereal fiber, fruit fiber, and type 2 diabetes: Explaining the paradox. J. Diabetes Its Complicat. 2018, 32, 240–245. [Google Scholar] [CrossRef]
- Durrer Schutz, D.; Busetto, L.; Dicker, D.; Farpour-Lambert, N.; Pryke, R.; Toplak, H.; Widmer, D.; Yumuk, V.; Schutz, Y. European practical and patient-centred guidelines for adult obesity management in primary care. Obesity Facts 2019, 12, 40–66. [Google Scholar] [CrossRef]
- Wing, R.R.; Lang, W.; Wadden, T.A.; Saford, M.; Knowler, W.C.; Bertoni, A.G.; Hill, J.O.; Brancati, F.L.; Peters, A.; Wagenknecht, L.; et al. Benefts of modest weight loss in improving cardiovascular risk factors in overweight and obese individuals with type 2 diabetes. Diabetes Care 2011, 34, 1481–1486. [Google Scholar] [CrossRef] [Green Version]
- Diabetes Prevention Program Research Group. 10-year follow-up of diabetes incidence and weight loss in the Diabetes Prevention Program Outcomes Study. Lancet 2009, 374, 1677–1686. [Google Scholar] [CrossRef] [Green Version]
- McRorie, J.W.; McKeown, N.M. Understanding the physics of functional fibers in the gastrointestinal tract: An evidence-based approach to resolving enduring misconceptions about insoluble and soluble fiber. J. Acad. Nutr. Diet 2017, 117, 251–264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anderson, J.; Allgood, L.; Turner, C.; Oelgten, P.; Daggy, B. Effects of psyllium on glucose and serum lipid responses in men with type 2 diabetes and hypercholesterolemia. Am. J. Clin. Nutr. 1999, 70, 466–473. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Moran, M.; Guerrero-Romero, F.; Laczano-Burciaga, L. Lipid- and glucose-lowering efficacy of plantago psyllium in type II diabetes. J. Diabetes Complicat. 1998, 12, 273–278. [Google Scholar] [CrossRef]
- Grundy, M.M.; Edwards, C.H.; Mackie, A.R.; Gidley, M.J.; Butterworth, P.J.; Ellis, P.R. Re-evaluation of the mechanisms of dietary fibre and implications for macronutrient bioaccessibility, digestion and postprandial metabolism. Br. J. Nutr. 2016, 116, 816–833. [Google Scholar] [CrossRef] [Green Version]
- Brownlee, I.A. The physiological roles of dietary fibre. Food Hydrocoll. 2011, 25, 238–250. [Google Scholar] [CrossRef]
- Kendall, C.W.C.; Esfahani, A.; Jenkins, D.J.A. The link between dietary fibre and human health. Food Hydrocoll. 2010, 24, 42–48. [Google Scholar] [CrossRef]
- Gunness, P.; Gidley, M.J. Mechanisms underlying the cholesterol-lowering properties of soluble dietary fibre polysaccharides. Food Funct. 2010, 1, 149–155. [Google Scholar] [CrossRef]
- Mackie, A.; Bajka, B.; Rigby, N. Roles for dietary fibre in the upper GI tract: The importance of viscosity. Food Res. Int. 2016, 88, 234–238. [Google Scholar] [CrossRef]
- Feinglos, M.; Gibb, R.; Ramsey, D.; Surwit, R.; McRorie, J. Psyllium improves glycemic control in patients with type-2 diabetes mellitus. Bio. Carb. Diet. Fibre 2013, 1, 156–161. [Google Scholar] [CrossRef]
- Edwards, C.H.; Grundy, M.M.; Grassby, T.; Vasilopoulou, D.; Frost, G.S.; Butterworth, P.J.; Berry, S.E.; Sanderson, J.; Ellis, P.R. Manipulation of starch bioaccessibility in wheat endosperm to regulate starch digestion, postprandial glycemia, insulinemia, and gut hormone responses: A randomized controlled trial in healthy ileostomy participants. Am. J. Clin. Nutr. 2015, 102, 791–800. [Google Scholar] [CrossRef] [Green Version]
- Thomas, D.E.; Elliott, E.J. The use of low-glycaemic index diets in diabetes control. Br. J. Nutr. 2010, 104, 797–802. [Google Scholar] [CrossRef] [Green Version]
- Ojo, O.; Ojo, O.O.; Adebowale, F.; Wang, X.-H. The Effect of Dietary Glycaemic Index on Glycaemia in Patients with Type 2 Diabetes: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Nutrients 2018, 10, 373. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weickert, M.O.; Pfeiffer, A.F.H. Impact of Dietary Fiber Consumption on Insulin Resistance and the Prevention of Type 2 Diabetes. J. Nutr. 2018, 148, 7–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient/Population | Intervention | Outcome (Primary) | Study Designs | Combining Search Terms |
|---|---|---|---|---|
| Patients with diabetes | Dietary fibre | Gut microbiota | Randomised controlled trial | |
| Patients with diabetes OR type 2 diabetes OR Diabetes OR Diabetes complications OR diabetes mellitus, type 2 OR diabetes mellitus | Dietary fibre OR Dietary supplements OR Dietary carbohydrate OR Polysaccharide OR Wheat bran OR Fibre OR Supplement OR Prebiotics | Microbiota OR Gut microbiota OR Gastrointestinal microbiota OR Microbiome | #1 Randomised controlled trial OR controlled clinical trial OR randomized OR placebo OR drug therapy OR randomly OR trial OR groups #2 “Animals” NOT “Humans” #3 #1 NOT #2 | Column 1 AND Column 2 AND Column 3 AND Column 4 |
| Citation/Country of Study | Study Type | Sample Details | Mean Age (Years) | Aim | Interventions | Results |
|---|---|---|---|---|---|---|
| Birkeland et al. [29]. Norway | Randomised, placebo controlled, double-blind, cross-over study | n = 25 | 63.1 (41–73) | To evaluate the prebiotic effect of inulin-type fructans on faecal microbiota and SCFA in patients with T2D. | Inulin-type fructans (a mixture of oligofructose and inulin) versus placebo (maltodextrin). A 4-week washout separated the 6 weeks of treatment. | A daily supplement of inulin-type fructans induced a moderate, but significant increase in faecal levels of bifidobacteria, total SCFA, acetic acid and propionic acid in patients with T2D. |
| Candela et al. [26]. Italy | Open-label randomised controlled trial | Ma-Pi 2 diet: n = 21; Control diet: n = 19. | 66 | To explore the potential of two different energy-restricted dietary approaches—the fibre-rich macrobiotic Ma-Pi 2 diet or a control diet recommended by Italian professional societies for T2D treatment—to correct gut microbiota dysbiosis in T2D patients. | Fibre-rich macrobiotic Ma-Pi 2 diet versus control diet. 21 days of treatment. | The Ma-Pi 2 diet was associated with a greater reduction in FBG. Body weight changes (mean ± SD) kg: Ma-Pi 2 diet: −5.6 ± −1.0 Control diet: −2.7 ± −0.6 |
| Gonai et al. [30]. Japan | Randomized controlled, double-blind study | GOS: n = 27; Placebo: n = 25. | GOS: 55 ± 11 Placebo: 54 ± 12. | To assess the effects of GOS on glycaemic control and gut microbiotas and metabolites in patients with T2D. | Galacto-oligosaccharide (GOS) versus placebo (maltodextrin). Four weeks of treatment. | GOS restored the abundance of Bifidobacteriaceae. However, GOS did not have a significant effect on glucose tolerance. |
| Medina-Vera et al. [22]. Mexico | Single-centre, placebo-controlled, randomised double-blind | T2D: n = 81 (randomised: 9 subjects from each group discontinued study) final group numbers analysed: DF: n = 28 Placebo: n = 25 | DP: 50.4 ± 8.7 Placebo: 49.8 ± 10.6 | To study the effects of a functional food-based dietary intervention on faecal microbiota and biochemical parameters in patients with T2D. | A dietary portfolio (DP) versus placebo. A 3-month treatment period. | DP consumption stimulated the abundance of Bifidobacterium longum shown to improve insulin sensitivity. There were no significant differences in the levels of glucose between groups. Patients with T2D following the DP showed significant reductions in specific biochemical parameters compared with the placebo group: AUCs for glucose. |
| Pedersen et al. [23]. UK | Randomised, double-blind, placebo-controlled parallel study | GOS: n = 14; Placebo: n = 15. | GOS: 56.7 ± 1.6; Placebo: 58.1 ± 1.7. | To compare the effects of prebiotic supplementation with placebo treatment for 12 weeks on glucose control, intestinal permeability, intestinal bacterial composition, and endotoxaemia in patients with T2D. | Galacto-oligosaccharide (GOS) versus placebo (maltodextrin): 12 weeks of treatment. | Prebiotic fibre supplementation had no significant effects on clinical outcomes or bacterial abundances compared with placebo. Body weight changes (mean ± SEM) kg: GOS: 0.6 ± 0.1 Placebo: 0.1 ± 0 |
| Reimer et al. [31]. Canada | Placebo-controlled, double-blind, randomised controlled study | PGX®: n = 147 Placebo: n = 143. | PGX®: 56.2 ± 8.6 Placebo: 53.4 ± 9.9. | To examine the adjunct effect of the soluble viscous fibre PolyGlycopleX® (PGX®) on glycaemic control in adults with T2D. | PGX® versus placebo 52 weeks of treatment. | The butyrate producer (Roseburia) was significantly increased in the PGX® group. Adding PGX® to a weight management program for individuals with T2D provides a sustained reduction in HbA1c compared to placebo. Body weight changes: mean (95% CI) kg PGX®: −3.87 (−1.75 to −6.0) Placebo: −1.62 (0.56 to −3.80) |
| Soare et al. [27]. Italy | Randomized controlled, open-label trial | Ma-Pi 2 diet: n = 25; Control diet: n = 26 | Ma-Pi 2 diet: 67 ± 8.163 Control diet: 65 ± 7.284 | To evaluate the effect of different dietary approaches—the macrobiotic Ma-Pi 2 diet compared with standard diets recommended for patients with T2D. | Fibre-rich macrobiotic Ma-Pi 2 diet versus control diet: 21 days of treatment. | There was significantly greater reduction in fasting blood glucose, HbA1c, and insulin resistance in those patients receiving the Ma-Pi 2 diet compared with those in the control diet group. Body weight changes (mean ± SD) kg Ma-Pi 2 diet: −4.9 ± 0.4 Control diet: −3.97 ± 0.08 |
| Soare et al. [28]. Italy | Randomized controlled, open-label trial. 6-month follow-up study | Ma-Pi 2 diet: n = 17 Control diet: n = 23. | Ma-Pi 2 diet: 65 ± 8.89 Control diet: 64 ± 8.15 | To investigate whether the benefits of the original 21-day intensive dietary interventions extended beyond the original MADIAB trial duration and into everyday life. | Fibre-rich macrobiotic Ma-Pi 2 diet versus control diet: 6 months of treatment. | The Ma-Pi diet was associated with a higher percentage reduction in HbA1c. The Ma-Pi diet resulted in greater improvement in glycaemic control. Body weight changes: median (1st–3rd quartile) kg Ma-Pi 2 diet: −1.46 (−4.59; 0.78) Control diet: 0.72 (−2.4; 3.26) |
| Zhao et al. [13]. China | Randomized controlled trial, open-label, parallel-group study | High dietary fibre: n = 27, Control: n = 16. | High dietary fibre: 58.4 ± 6.2. Control: 59.7 ± 6.0; | To characterise the dynamics of the gut microbiota and its impact on glucose homeostasis in patients with T2D. | High dietary fibre versus control (usual care) | A select group of SCFA-producing strains was promoted by dietary fibres, and most other potential producers were either diminished or unchanged in patients with T2D. Body weight changes (mean ± SEM) kg: High dietary fibre: −2.99 ± −0.16 Control: −1.09 ± −0.13 |
| Citations | Bacteroides | Clostridium | Lactobacillus | Ruminococcus | Roseburia | Bifidobacterium |
|---|---|---|---|---|---|---|
| Birkeland et al. [29]. | There was also a positive effect on operational taxonomic units of Bacteroides. | Not Applicable | Not Applicable | Not Applicable | Not Applicable | A bifidogenic effect was most prominent, with the highest positive effect on operational taxonomic units (OTUs) of Bifidobacterium adolescentis |
| Candela et al. [26]. | Both diets increased the abundance of propionate and butyrate producers (i.e., Bacteroides) | Not Applicable | Not Applicable | Both diets consolidated a healthy-like abundance of Ruminococcus | Both diets consolidated a healthy-like abundance of Roseburia | Not Applicable |
| Gonai et al. [30]. | Not Applicable | Not Applicable | Not Applicable | Levels of Ruminococcaceae were significantly lower after intake of GOS compared with the baseline | Not Applicable | Bifidobacteriaceae abundance was considerably increased by intake of GOS compared with the baseline. |
| Medina-Vera et al. [22]. | Not Applicable | Not Applicable | Not Applicable | Not Applicable | Not Applicable | DP consumption stimulated the abundance of Bifidobacterium longum |
| Pedersen et al. [23]. | Not Applicable | Prebiotic treatment had no significant effect on Clostridium leptum or Clostridium coccoides groups. | Prebiotic treatment had no significant effect on total bacteria, Lactobacillus | Not Applicable | Prebiotic treatment had no significant effect on Roseburia | Prebiotic treatment had no significant effect on Bifidobacterium or any of the other bacteria measured |
| Reimer et al. [31]. | Not Applicable | Not Applicable | Not Applicable | Not Applicable | PGX® significantly increased the relative abundance of Roseburia | Not Applicable |
| Soare et al. [27]. | Not Applicable | Not Applicable | Not Applicable | Not Applicable | Not Applicable | Not Applicable |
| Soare et al. [28]. | Not Applicable | Not Applicable | Not Applicable | Not Applicable | Not Applicable | Not Applicable |
| Zhao et al. [13]. | Not Applicable | Not Applicable | Not Applicable | Not Applicable | Not Applicable | Bifidobacterium pseudocatenulatum was one of the most significantly promoted SCFA producers |
| PGX® (n = 103) | Placebo (n = 104) | |
|---|---|---|
| Total adverse events | 580 | 525 |
| Most common events: | ||
| Diarrhoea/loose stool | 150 | 61 |
| Cold/flu-like symptoms | 56 | 71 |
| Abdominal bloating | 35 | 29 |
| Abdominal pain/cramps | 35 | 37 |
| Constipation | 17 | 48 |
| Headache/sinus pain | 27 | 45 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ojo, O.; Feng, Q.-Q.; Ojo, O.O.; Wang, X.-H. The Role of Dietary Fibre in Modulating Gut Microbiota Dysbiosis in Patients with Type 2 Diabetes: A Systematic Review and Meta-Analysis of Randomised Controlled Trials. Nutrients 2020, 12, 3239. https://doi.org/10.3390/nu12113239
Ojo O, Feng Q-Q, Ojo OO, Wang X-H. The Role of Dietary Fibre in Modulating Gut Microbiota Dysbiosis in Patients with Type 2 Diabetes: A Systematic Review and Meta-Analysis of Randomised Controlled Trials. Nutrients. 2020; 12(11):3239. https://doi.org/10.3390/nu12113239
Chicago/Turabian StyleOjo, Omorogieva, Qian-Qian Feng, Osarhumwese Osaretin Ojo, and Xiao-Hua Wang. 2020. "The Role of Dietary Fibre in Modulating Gut Microbiota Dysbiosis in Patients with Type 2 Diabetes: A Systematic Review and Meta-Analysis of Randomised Controlled Trials" Nutrients 12, no. 11: 3239. https://doi.org/10.3390/nu12113239