A Snapshot of European Children’s Eating Habits: Results from the Fourth Round of the WHO European Childhood Obesity Surveillance Initiative (COSI)

 ,
,  , , , , , ,
, , , , , ,  , , , , add
Show full author list
, , , , add
Show full author list
Abstract
:1. Introduction
2. Materials and Methods
3. Results
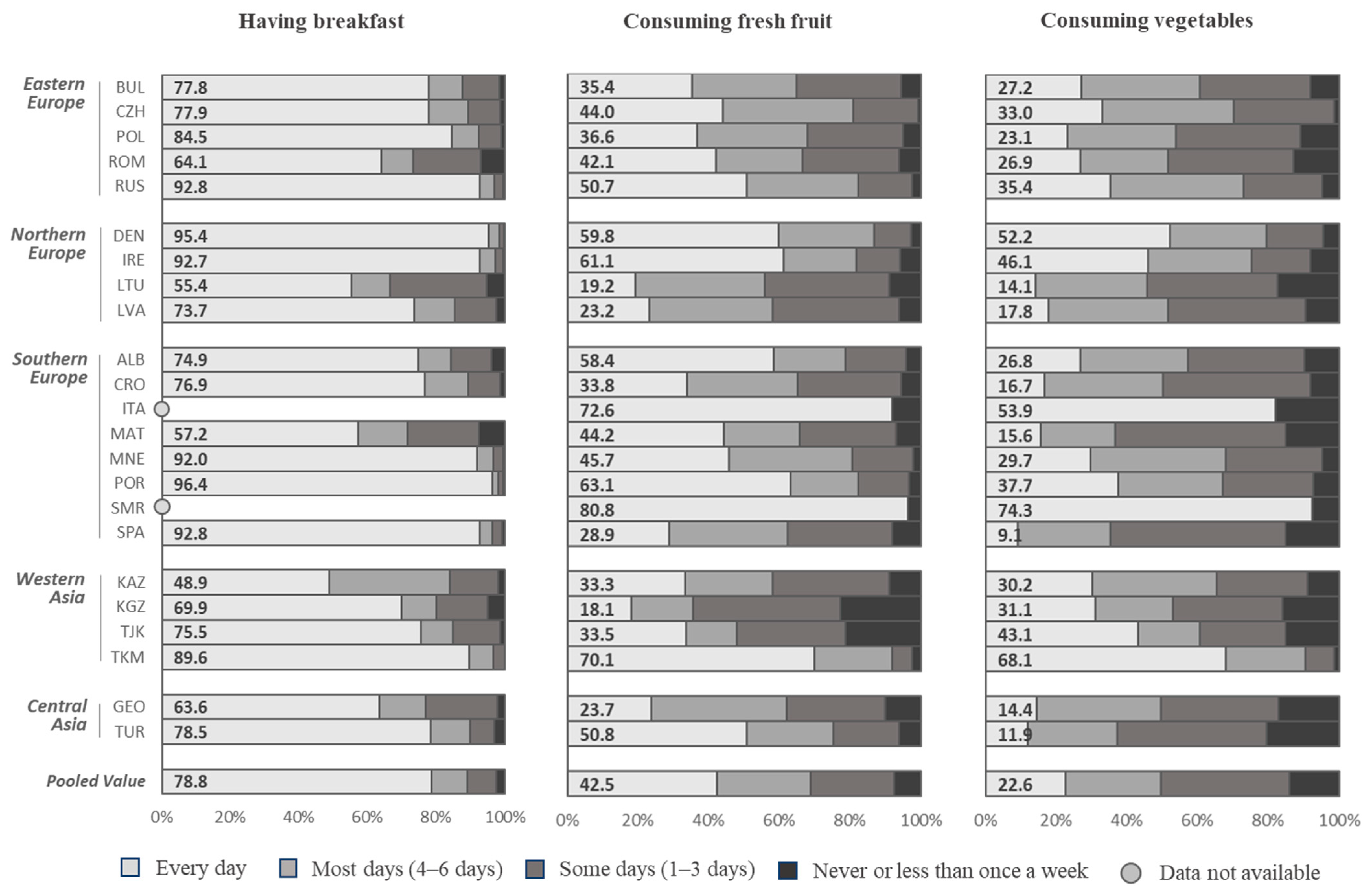
3.1. Consumption of Breakfast
3.2. Consumption of Fresh Fruit
3.3. Consumption of Vegetables
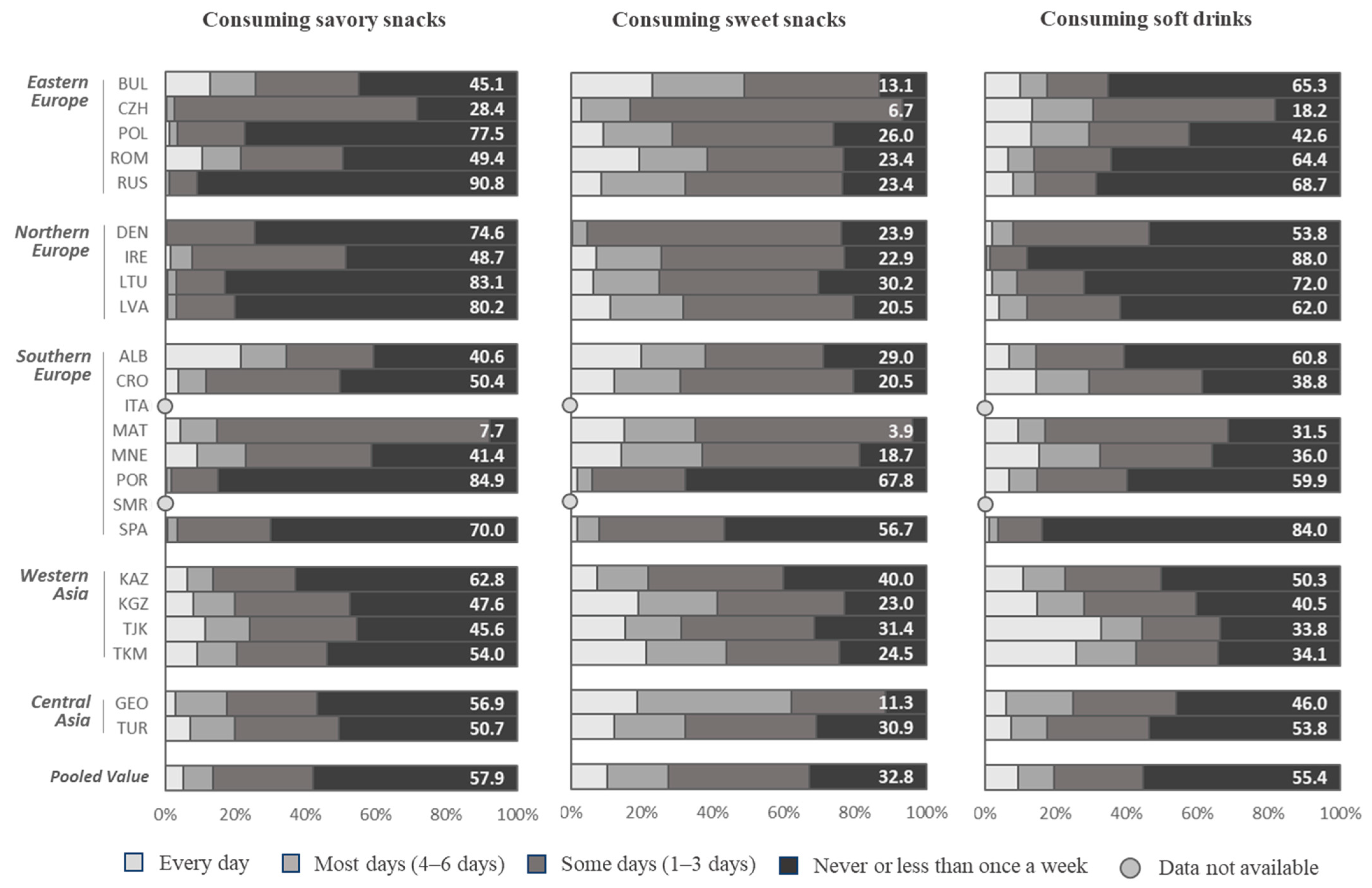
3.4. Consumption of Savory Snacks (Like Potato Crisps, Corn Chips, Popcorn, or Peanuts)
3.5. Consumption of Sweets (Like Candy Bars or Chocolate)
3.6. Consumption of Soft Drinks
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Disclaimer
References
- Park, M.H.; Falconer, C.; Viner, R.M.; Kinra, S. The impact of childhood obesity on morbidity and mortality in adulthood: A systematic review. Obes. Rev. 2012, 13, 985–1000. [Google Scholar] [CrossRef] [PubMed]
- Wijnhoven, T.M.; van Raaij, J.M.; Spinelli, A.; Starc, G.; Hassapidou, M.; Spiroski, I.; Rutter, H.; Martos, E.; Rito, A.I.; Hovengen, R.; et al. WHO European Childhood Obesity Surveillance Initiative: Body mass index and level of overweight among 6-9-year-old children from school year 2007/2008 to school year 2009/2010. BMC Public Health 2014, 14, 806. [Google Scholar] [CrossRef] [Green Version]
- Afshin, A.; Sur, P.J.; Fay, K.A.; Cornaby, L.; Ferrara, G.; Salama, J.S.; Mullany, E.C.; Abate, K.H.; Abbafati, C.; Abebe, Z. Health effects of dietary risks in 195 countries, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2019, 393, 1958–1972. [Google Scholar] [CrossRef] [Green Version]
- Freemark, M. Determinants of Risk for Childhood Obesity. N. Engl. J. Med. 2018, 379, 1371–1372. [Google Scholar] [CrossRef] [PubMed]
- Freemark, M. Childhood obesity in the modern age: Global trends, determinants, complications, and costs. In Pediatric Obesity; Springer: Berlin/Heidelberg, Germany, 2018; pp. 3–24. [Google Scholar]
- WHO. WHO European Childhood Obesity Surveillance Initiative: Report of the Fourth Round of Data Collection (2015–2017); WHO: Geneva, Switzerland, 2020. [Google Scholar]
- WHO. The Double Burden of Malnutrition. Available online: https://www.who.int/nutrition/double-burden-malnutrition/en/#:~:text=Double%20burden%20of%20malnutrition,populations%2C%20and%20across%20the%20lifecourse (accessed on 1 June 2020).
- Djordjic, V.; Jorga, J.; Radisavljevic, S.; Milanovic, I.; Bozic, P.; Ostojic, S.M. Thinness in young schoolchildren in Serbia: Another case of the double burden of malnutrition? Public Health Nutr. 2018, 21, 877–881. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Global Burden of Disease Collaborators Health effects of overweight and obesity in 195 countries over 25 years. N. Engl. J. Med. 2017, 377, 13–27. [CrossRef]
- WHO. World Health Organization Global Monitoring Framework for NCDs: Target 7: Halt the Rise in Obesity. Available online: https://www.who.int/nmh/ncd-tools/target7/en/ (accessed on 1 June 2020).
- United Nations. Sustainable Development Goals. Available online: https://sustainabledevelopment.un.org/?menu=1300 (accessed on 28 June 2020).
- Sachs, J.; Schmidt-Traub, G.; Kroll, C.; Lafortune, G.; Fuller, G. Sustainable Development Report 2019; Bertelsmann Stiftung and Sustainable Development Solutions Network (SDSN): New York, NY, USA, 2019; Volume 2. [Google Scholar]
- Mikkilä, V.; Räsänen, L.; Raitakari, O.T.; Pietinen, P.; Viikari, J. Longitudinal changes in diet from childhood into adulthood with respect to risk of cardiovascular diseases: The Cardiovascular Risk in Young Finns Study. Eur. J. Clin. Nutr. 2004, 58, 1038–1045. [Google Scholar] [CrossRef] [Green Version]
- WHO. Increasing Fruit and Vegetable Consumption to Reduce the Risk of Noncommunicable Diseases; World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- WHO. Diet, Nutrition and the Prevention of Chronic Diseases: Report of a Joint WHO/FAO Expert Consultation; WHO Technical Report Series, No. 916; World Health Organization: Geneva, Switzerland, 2003. [Google Scholar]
- WHO. Guideline: Sugars Intake for Adults and Children; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- Mozaffarian, D.; Fahimi, S.; Singh, G.M.; Micha, R.; Khatibzadeh, S.; Engell, R.E.; Lim, S.; Danaei, G.; Ezzati, M.; Powles, J.; et al. Global sodium consumption and death from cardiovascular causes. N. Engl. J. Med. 2014, 371, 624–634. [Google Scholar] [CrossRef] [Green Version]
- Malik, V.S.; Pan, A.; Willett, W.C.; Hu, F.B. Sugar-sweetened beverages and weight gain in children and adults: A systematic review and meta-analysis. Am. J. Clin. Nutr. 2013, 98, 1084–1102. [Google Scholar] [CrossRef] [Green Version]
- Moynihan, P.J.; Kelly, S.A.M. Effect on caries of restricting sugars intake: Systematic review to inform WHO guidelines. J. Dent. Res. 2014, 93, 8–18. [Google Scholar] [CrossRef] [Green Version]
- Wijnhoven, T.M.; van Raaij, J.; Breda, J. WHO European Childhood Obesity Surveillance Initiative. Implementation of Round 1 (2007/2008) and Round 2 (2009/2010); WHO Regional Office for Europe: Copenhagen, Denmark, 2014. [Google Scholar]
- Council for International Organizations of Medical Sciences, Council for International Organizations of Medical Sciences, World Health Organization. International Ethical Guidelines for Biomedical Research Involving Human Subjects; World Health Organization: Geneva, Switzerland, 2002. [Google Scholar]
- Wijnhoven, T.M.; van Raaij, J.M.; Spinelli, A.; Rito, A.I.; Hovengen, R.; Kunesova, M.; Starc, G.; Rutter, H.; Sjoberg, A.; Petrauskiene, A.; et al. WHO European Childhood Obesity Surveillance Initiative 2008: Weight, height and body mass index in 6-9-year-old children. Pediatr. Obes. 2013, 8, 79–97. [Google Scholar] [CrossRef] [PubMed]
- WHO. European Childhood Obesity Surveillance Initiative: Overweight and Obesity among 6–9-year-old Children. Report of the Third Round of Data Collection 2012–2013; WHO: Geneva, Switzerland, 2018. [Google Scholar]
- WHO. Healthy Diet: Key Facts. Available online: https://www.who.int/news-room/fact-sheets/detail/healthy-diet (accessed on 29 June 2020).
- United Nations. Statistical Division Standard Country or Area Codes for Statistical Use (M49). Available online: https://unstats.un.org/unsd/methodology/m49/ (accessed on 6 August 2020).
- Monzani, A.; Ricotti, R.; Caputo, M.; Solito, A.; Archero, F.; Bellone, S.; Prodam, F. A systematic review of the association of skipping breakfast with weight and cardiometabolic risk factors in children and adolescents. What should we better investigate in the future? Nutrients 2019, 11, 387. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Inchley, J.; Currie, D.B.; Budisavljevic, S.; Torsheim, T.; Jåstad, A.; Cosma, A.; Kelly, C.; Arnarsson, Á. Spotlight on Adolescent Health and Well-Being: Findings from the 2017/2018 Health Behaviour in School-Aged Children (HBSC) Survey in Europe and Canada; WHO Regional Office for Europe: Copenhagen, Denmark, 2020. [Google Scholar]
- Vereecken, C.; Pedersen, T.P.; Ojala, K.; Krølner, R.; Dzielska, A.; Ahluwalia, N.; Giacchi, M.; Kelly, C. Fruit and vegetable consumption trends among adolescents from 2002 to 2010 in 33 countries. Eur. J. Public Health 2015, 25, 16–19. [Google Scholar] [CrossRef] [Green Version]
- Rosi, A.; Paolella, G.; Biasini, B.; Scazzina, F.; Alicante, P.; De Blasio, F.; dello Russo, M.; Paolella, G.; Rendina, D.; Rosi, A. Dietary habits of adolescents living in North America, Europe or Oceania: A review on fruit, vegetable and legume consumption, sodium intake, and adherence to the Mediterranean Diet. Nutr. Metab. Cardiovasc. Dis. 2019, 29, 554–560. [Google Scholar] [CrossRef] [PubMed]
- Scaglioni, S.; De Cosmi, V.; Ciappolino, V.; Parazzini, F.; Brambilla, P.; Agostoni, C. Factors Influencing Children’s Eating Behaviours. Nutrients 2018, 10, 706. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, R.; Kelly, B.; Yeatman, H.; Boyland, E. Food marketing influences children’s attitudes, preferences and consumption: A systematic critical review. Nutrients 2019, 11, 875. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Micha, R.; Karageorgou, D.; Bakogianni, I.; Trichia, E.; Whitsel, L.P.; Story, M.; Penalvo, J.L.; Mozaffarian, D. Effectiveness of school food environment policies on children’s dietary behaviors: A systematic review and meta-analysis. PLoS ONE 2018, 13, e0194555. [Google Scholar] [CrossRef]
- European Commission. School Fruit, Vegetables and Milk Scheme. Available online: https://ec.europa.eu/info/food-farming-fisheries/key-policies/common-agricultural-policy/market-measures/school-fruit-vegetables-and-milk-scheme (accessed on 25 May 2020).
- WHO. Nutrition-Friendly Schools Initiative (NFSI). Available online: https://www.who.int/nutrition/topics/nutrition_friendly_schools_initiative/en/ (accessed on 25 May 2020).
- U.S. Department of Agriculture. School Breakfast Program. Available online: https://www.fns.usda.gov/sbp/school-breakfast-program (accessed on 26 May 2020).
- WHO. Taxes on Sugary Drinks: Why Do It? World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Colchero, M.A.; Rivera-Dommarco, J.; Popkin, B.M.; Ng, S.W. In Mexico, Evidence of Sustained Consumer Response two Years after Implementing a Sugar-Sweetened Beverage Tax. Health Aff. (Millwood) 2017, 36, 564–571. [Google Scholar] [CrossRef]
- van Raaij, J.; Hendriksen, M.; Verhagen, H. Potential for improvement of population diet through reformulation of commonly eaten foods. Public Health Nutr. 2009, 12, 325–330. [Google Scholar] [CrossRef] [Green Version]
- Goiana-da-Silva, F.; Cruz, E.S.D.; Gregorio, M.J.; Miraldo, M.; Darzi, A.; Araujo, F. The future of the sweetened beverages tax in Portugal. Lancet Public Health 2018, 3, e562. [Google Scholar] [CrossRef] [Green Version]
- Griffith, R.; O’Connell, M.; Smith, K. The Importance of Product Reformulation Versus Consumer Choice in Improving Diet Quality. Economica 2017, 84, 34–53. [Google Scholar] [CrossRef] [Green Version]
- Macgregor, G.A.; Hashem, K.M. Action on sugar--lessons from UK salt reduction programme. Lancet 2014, 383, 929–931. [Google Scholar] [CrossRef]
- Cairns, G.; Angus, K.; Hastings, G.; Caraher, M. Systematic reviews of the evidence on the nature, extent and effects of food marketing to children. A retrospective summary. Appetite 2013, 62, 209–215. [Google Scholar] [CrossRef] [PubMed]
- WHO. Monitoring and Restricting Digital Marketing of Unhealthy Products to Children and Adolescents; World Health Organization Regional Office for Europe: Copenhagen, Denmark, 2019. [Google Scholar]
- WHO. Noncommunicable Diseases Progress Monitor; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Hodder, R.K.; O’Brien, K.M.; Tzelepis, F.; Wyse, R.J.; Wolfenden, L. Interventions for increasing fruit and vegetable consumption in children aged five years and under. Cochrane Database Syst. Rev. 2018, 2018, CD008552. [Google Scholar] [CrossRef]
- Mazarello Paes, V.; Hesketh, K.; O’Malley, C.; Moore, H.; Summerbell, C.; Griffin, S.; Van Sluijs, E.M.F.; Ong, K.K.; Lakshman, R. Determinants of sugar-sweetened beverage consumption in young children: A systematic review. Obes. Rev. 2015, 16, 903–913. [Google Scholar] [CrossRef] [Green Version]
- Kairey, L.; Matvienko-Sikar, K.; Kelly, C.; McKinley, M.C.; O’Connor, E.M.; Kearney, P.M.; Woodside, J.V.; Harrington, J.M. Plating up appropriate portion sizes for children: A systematic review of parental food and beverage portioning practices. Obes. Rev. 2018, 19, 1667–1678. [Google Scholar] [CrossRef] [Green Version]
- WHO. Report of the Commission on Ending Childhood Obesity; World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- Crockett, R.A.; King, S.E.; Marteau, T.M.; Prevost, A.T.; Bignardi, G.; Roberts, N.W.; Stubbs, B.; Hollands, G.J.; Jebb, S.A. Nutritional labelling for healthier food or non-alcoholic drink purchasing and consumption. Cochrane Database Syst. Rev. 2018, 2, CD009315. [Google Scholar] [CrossRef] [Green Version]
- Monsivais, P.; Aggarwal, A.; Drewnowski, A. Are socio-economic disparities in diet quality explained by diet cost? J. Epidemiol. Community Health 2012, 66, 530–535. [Google Scholar] [CrossRef]
- Spinelli, A.; Buoncristiano, M.; Kovacs, V.A.; Yngve, A.; Spiroski, I.; Obreja, G.; Starc, G.; Pérez, N.; Rito, A.I.; Kunešová, M. Prevalence of severe obesity among primary school children in 21 European countries. Obes. Facts 2019, 12, 244–258. [Google Scholar] [CrossRef]
- Pérez-Rodrigo, C.; Artiach Escauriaza, B.; Artiach Escauriaza, J.; Polanco Allúe, I. Dietary assessment in children and adolescents: Issues and recommendations. Nutr. Hosp. 2015, 31 (Suppl. 3), 76–83. [Google Scholar] [CrossRef]
- Medin, A.C.; Hansen, B.H.; Astrup, H.; Ekelund, U.; Frost Andersen, L. Validation of energy intake from a web-based food recall for children and adolescents. PLoS ONE 2017, 12, e0178921. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheung, K.L.; Peter, M.; Smit, C.; de Vries, H.; Pieterse, M.E. The impact of non-response bias due to sampling in public health studies: A comparison of voluntary versus mandatory recruitment in a Dutch national survey on adolescent health. BMC Public Health 2017, 17, 276. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berg, C.; Jonsson, I.; Conner, M.T.; Lissner, L. Sources of bias in a dietary survey of children. Eur. J. Clin. Nutr. 1998, 52, 663–667. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Country a | Children Invited to Participate b | Children Included in the Analysis c | Percentage of Children Participating by Sex and Age (%) d | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Total Number | Proportion Whose Family Form Was Filled in (%) | Boys (n) | Girls (n) | Total (n) | Boys (%) | 6-Year-Olds | 7-Year-Olds | 8-Year-Olds | 9-Year-Olds | |
| Albania | 7113 | 36.2 | 1315 | 1212 | 2527 | 52.5 | 0.1 | 24.2 | 52.0 | 23.7 |
| Bulgaria | 4090 | 83.1 | 1702 | 1698 | 3400 | 51.5 | 0 | 100.0 | 0 | 0 |
| Croatia e | 7220 | 76.0 | 1318 | 1333 | 2651 | 51.1 | 0 | 0 | 100.0 | 0 |
| Czechia | n.a. | n.a. | 670 | 736 | 1406 | 50.7 | 49.5 | 50.5 | 0 | 0 |
| Denmark | 3202 | 29.9 | 511 | 446 | 957 | 52.7 | 27.4 | 70.2 | 2.4 | 0 |
| Georgia | 4143 | 78.4 | 1667 | 1579 | 3246 | 51.2 | 1.6 | 85.1 | 13.0 | 0.3 |
| Ireland | 2704 | 32.4 | 438 | 436 | 874 | 52.6 | 38.2 | 60.2 | 1.6 | 0 |
| Italy | 50,902 | 95.2 | 22,425 | 21,271 | 43,696 | 51.5 | 0 | 0.5 | 66.3 | 33.1 |
| Kazakhstan | 6026 | 82.3 | 2149 | 2162 | 4311 | 50.6 | 0 | 0.4 | 51.0 | 48.6 |
| Kyrgyzstan | 8773 | 86.6 | 3798 | 3769 | 7567 | 50.7 | 10.5 | 43.5 | 39.5 | 6.5 |
| Lithuania | 5527 | 69.8 | 1930 | 1882 | 3812 | 50.6 | 0.4 | 66.4 | 33.0 | 0.2 |
| Latvia | 8143 | 71.5 | 2752 | 2955 | 5707 | 48.2 | 7.9 | 43.8 | 9.1 | 39.3 |
| Malta | 4329 | 73.4 | 1589 | 1590 | 3179 | 50.0 | 0.1 | 69.7 | 30.1 | 0.1 |
| Montenegro | 4094 | 66.8 | 1441 | 1295 | 2736 | 52.8 | 31.2 | 48.4 | 20.1 | 0.2 |
| Poland | 3828 | 76.9 | 1451 | 1494 | 2945 | 50.2 | 0 | 0 | 100.0 | 0 |
| Portugal | 7475 | 85.6 | 3167 | 3224 | 6391 | 50.7 | 25.2 | 49.0 | 24.0 | 1.7 |
| Romania | 9094 | 73.6 | 3312 | 3298 | 6610 | 49.1 | 0.4 | 28.4 | 47.5 | 23.8 |
| Russian Federation | 3900 | 52.6 | 1006 | 1046 | 2052 | 50.2 | 18.8 | 72.8 | 8.3 | 0.1 |
| San Marino | 329 | 93.6 | 138 | 168 | 306 | 45.1 | 0 | 0 | 64.7 | 35.3 |
| Spain | 14,908 | 70.1 | 5290 | 5163 | 10,453 | 50.9 | 25.4 | 25.2 | 24.9 | 24.6 |
| Tajikistan | 3502 | 93.5 | 1623 | 1647 | 3270 | 51.6 | 7.7 | 90.8 | 1.4 | 0.2 |
| Turkmenistan | 4085 | 95.3 | 1944 | 1947 | 3891 | 49.9 | 0 | 79.9 | 20.1 | 0 |
| Turkey | 14,164 | 81.7 | 5335 | 5167 | 10,502 | 50.9 | 11.4 | 82.3 | 6.0 | 0.3 |
| Total | 198,683 | 79.5 | 66,971 | 65,518 | 132,489 | 51.3 | 0 | 75.2 | 18.2 | 6.6 |
© 2020 by World Health Organization. Licensee MDPI, Basel, Switzerland. This is an open access article distributed under the terms of the Creative Commons Attribution IGO License (http://creativecommons.org/licenses/by/3.0/igo/legalcode), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. In any reproduction of this article there should not be any suggestion that WHO or this article endorse any specific organisation or products. The use of the WHO logo is not permitted. This notice should be preserved along with the article’s original URL.
Share and Cite
Williams, J.; Buoncristiano, M.; Nardone, P.; Rito, A.I.; Spinelli, A.; Hejgaard, T.; Kierkegaard, L.; Nurk, E.; Kunešová, M.; Musić Milanović, S.; et al. A Snapshot of European Children’s Eating Habits: Results from the Fourth Round of the WHO European Childhood Obesity Surveillance Initiative (COSI). Nutrients 2020, 12, 2481. https://doi.org/10.3390/nu12082481
Williams J, Buoncristiano M, Nardone P, Rito AI, Spinelli A, Hejgaard T, Kierkegaard L, Nurk E, Kunešová M, Musić Milanović S, et al. A Snapshot of European Children’s Eating Habits: Results from the Fourth Round of the WHO European Childhood Obesity Surveillance Initiative (COSI). Nutrients. 2020; 12(8):2481. https://doi.org/10.3390/nu12082481
Chicago/Turabian StyleWilliams, Julianne, Marta Buoncristiano, Paola Nardone, Ana Isabel Rito, Angela Spinelli, Tatjana Hejgaard, Lene Kierkegaard, Eha Nurk, Marie Kunešová, Sanja Musić Milanović, and et al. 2020. "A Snapshot of European Children’s Eating Habits: Results from the Fourth Round of the WHO European Childhood Obesity Surveillance Initiative (COSI)" Nutrients 12, no. 8: 2481. https://doi.org/10.3390/nu12082481