NUTRIC and Modified NUTRIC are Accurate Predictors of Outcome in End-Stage Liver Disease: A Validation in Critically Ill Patients with Liver Cirrhosis

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Blood Sampling and Laboratory Analyses
2.3. Calculation of NUTRIC and mNUTRIC
2.4. Data Collection
2.5. Statistical Analysis and Primary Endpoint
3. Results
3.1. Patients’ Characteristics and Laboratory Analyses
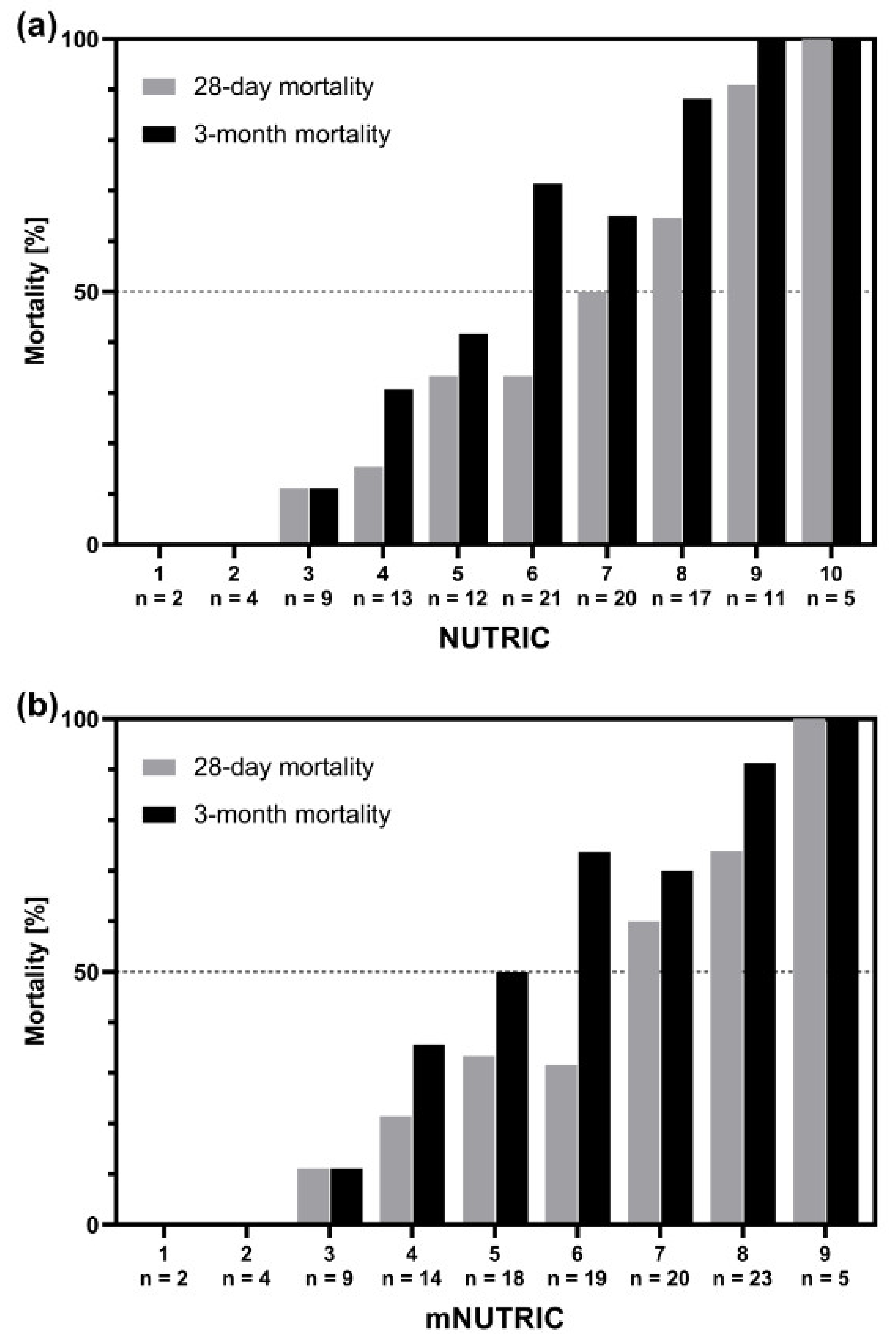
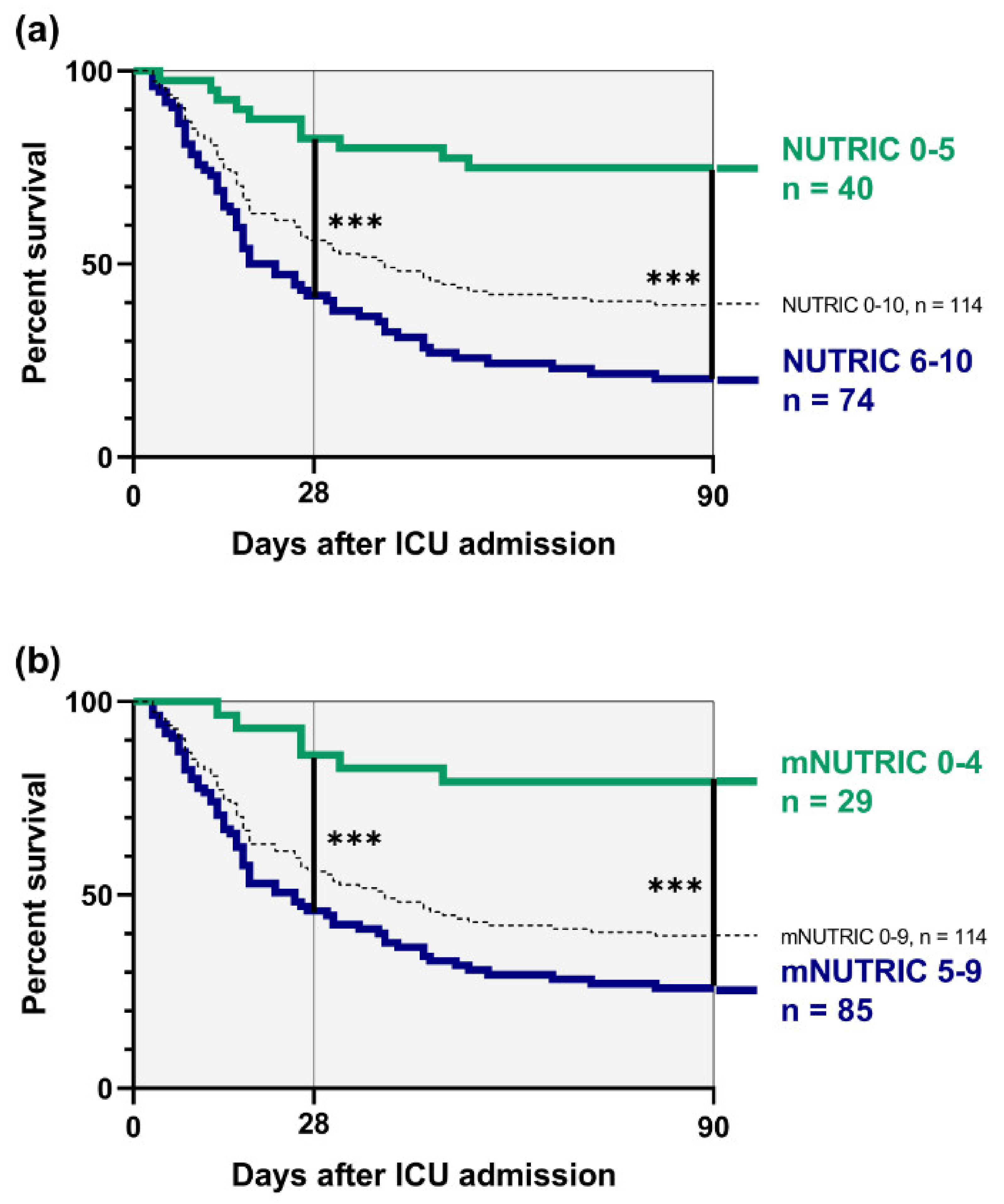
3.2. Mortality Risk Depending on NUTRIC and mNUTRIC
3.3. Patients with Discrepancy between NUTRIC and mNUTRIC
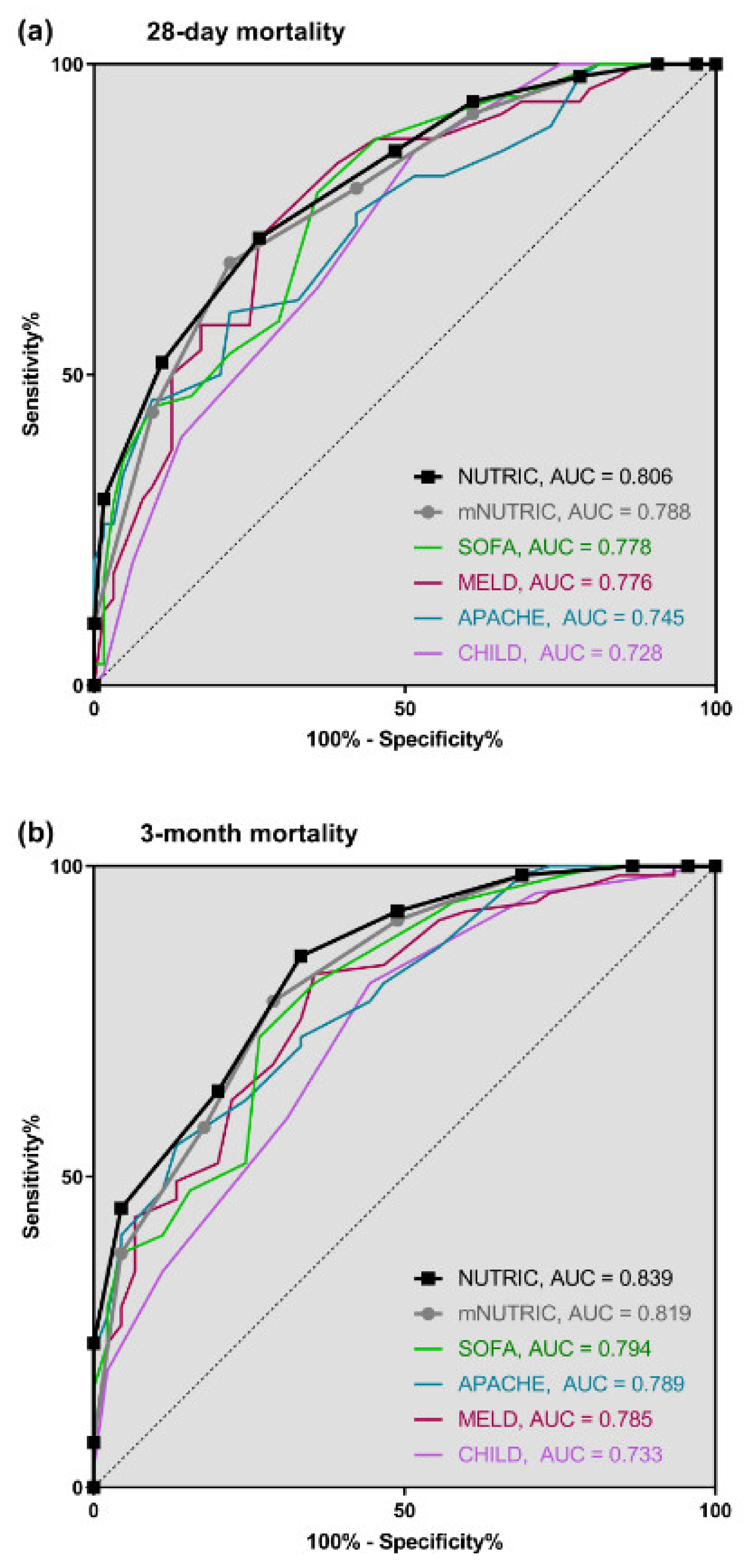
3.4. Prognostic Accuracy of NUTRIC and mNUTRIC
3.5. Correlation Analyses
4. Discussion
5. Limitations
6. Conclusions
Availability of Data and Material
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| ICU | Intensive care unit |
| NUTRIC | Nutrition Risk in Critically ill |
| APACHE | Acute and physiology chronic health evaluation |
| SOFA | Sequential organ failure assessment |
| IL6 | Interleukin 6 |
| mNUTRIC | Modified Nutrition Risk in Critically ill |
| MELD | Model of end-stage liver disease |
| ECLIA | Electrochemiluminescence immunoassay |
| IQR | Interquartile range |
| ROC | Receiver-operating-characteristic curves |
| AUC | Area under curve |
| PPV | Positive predictive value |
| NPV | Negative predictive value |
| HR | Hazard ratio |
| BMI | Body mass index |
| NAFLD | Non-alcoholic fatty liver disease |
| HRS | Hepato-renal syndrome |
| CI | Confidence interval |
| CAID | Cirrhosis associated immune dysfunction |
| CRP | C-reactive protein |
| PCT | Procalcitonin |
References
- Gines, P.; Quintero, E.; Arroyo, V.; Teres, J.; Bruguera, M.; Rimola, A.; Caballeria, J.; Rodes, J.; Rozman, C. Compensated cirrhosis: Natural history and prognostic factors. Hepatology 1987, 7, 122–128. [Google Scholar] [CrossRef]
- Iwakiri, Y.; Groszmann, R.J. The hyperdynamic circulation of chronic liver diseases: From the patient to the molecule. Hepatology 2006, 43, S121–S131. [Google Scholar] [CrossRef] [PubMed]
- Bernardi, M.; Moreau, R.; Angeli, P.; Schnabl, B.; Arroyo, V. Mechanisms of decompensation and organ failure in cirrhosis: From peripheral arterial vasodilation to systemic inflammation hypothesis. J. Hepatol. 2015, 63, 1272–1284. [Google Scholar] [CrossRef] [PubMed]
- Saliba, F.; Ichai, P.; Levesque, E.; Samuel, D. Cirrhotic patients in the ICU: Prognostic markers and outcome. Curr. Opin. Crit. Care 2013, 19, 154–160. [Google Scholar] [CrossRef] [PubMed]
- Alessandria, C.; Ozdogan, O.; Guevara, M.; Restuccia, T.; Jimenez, W.; Arroyo, V.; Rodes, J.; Gines, P. MELD score and clinical type predict prognosis in hepatorenal syndrome: Relevance to liver transplantation. Hepatology 2005, 41, 1282–1289. [Google Scholar] [CrossRef]
- Malbrain, M.L.; Chiumello, D.; Pelosi, P.; Bihari, D.; Innes, R.; Ranieri, V.M.; Del Turco, M.; Wilmer, A.; Brienza, N.; Malcangi, V.; et al. Incidence and prognosis of intraabdominal hypertension in a mixed population of critically ill patients: A multiple-center epidemiological study. Crit. Care Med. 2005, 33, 315–322. [Google Scholar] [CrossRef]
- D’Amico, G.; Pasta, L.; Morabito, A.; D’Amico, M.; Caltagirone, M.; Malizia, G.; Tine, F.; Giannuoli, G.; Traina, M.; Vizzini, G.; et al. Competing risks and prognostic stages of cirrhosis: A 25-year inception cohort study of 494 patients. Aliment. Pharmacol. Ther. 2014, 39, 1180–1193. [Google Scholar] [CrossRef] [Green Version]
- Jalan, R.; Fernandez, J.; Wiest, R.; Schnabl, B.; Moreau, R.; Angeli, P.; Stadlbauer, V.; Gustot, T.; Bernardi, M.; Canton, R.; et al. Bacterial infections in cirrhosis: A position statement based on the EASL Special Conference 2013. J. Hepatol. 2014, 60, 1310–1324. [Google Scholar] [CrossRef]
- Reverter, E.; Tandon, P.; Augustin, S.; Turon, F.; Casu, S.; Bastiampillai, R.; Keough, A.; Llop, E.; Gonzalez, A.; Seijo, S.; et al. A MELD-based model to determine risk of mortality among patients with acute variceal bleeding. Gastroenterology 2014, 146, 412–419. [Google Scholar] [CrossRef] [Green Version]
- Cholongitas, E.; Senzolo, M.; Patch, D.; Kwong, K.; Nikolopoulou, V.; Leandro, G.; Shaw, S.; Burroughs, A.K. Risk factors, sequential organ failure assessment and model for end-stage liver disease scores for predicting short term mortality in cirrhotic patients admitted to intensive care unit. Aliment. Pharmacol. Ther. 2006, 23, 883–893. [Google Scholar] [CrossRef]
- Das, V.; Boelle, P.Y.; Galbois, A.; Guidet, B.; Maury, E.; Carbonell, N.; Moreau, R.; Offenstadt, G. Cirrhotic patients in the medical intensive care unit: Early prognosis and long-term survival. Crit. Care Med. 2010, 38, 2108–2116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Drolz, A.; Jager, B.; Wewalka, M.; Saxa, R.; Horvatits, T.; Roedl, K.; Perkmann, T.; Zauner, C.; Kramer, L.; Ferenci, P.; et al. Clinical impact of arterial ammonia levels in ICU patients with different liver diseases. Intensive Care Med. 2013, 39, 1227–1237. [Google Scholar] [CrossRef]
- Levesque, E.; Saliba, F.; Ichai, P.; Samuel, D. Outcome of patients with cirrhosis requiring mechanical ventilation in ICU. J. Hepatol. 2014, 60, 570–578. [Google Scholar] [CrossRef]
- Scaglione, S.; Kliethermes, S.; Cao, G.; Shoham, D.; Durazo, R.; Luke, A.; Volk, M.L. The epidemiology of cirrhosis in the United States: A population-based study. J. Clin. Gastroenterol. 2015, 49, 690–696. [Google Scholar] [CrossRef]
- Fuhrmann, V.; Whitehouse, T.; Wendon, J. The ten tips to manage critically ill patients with acute-on-chronic liver failure. Intensive Care Med. 2018, 44, 1932–1935. [Google Scholar] [CrossRef] [PubMed]
- Muller, M.J.; Bottcher, J.; Selberg, O.; Weselmann, S.; Boker, K.H.; Schwarze, M.; von zur Muhlen, A.; Manns, M.P. Hypermetabolism in clinically stable patients with liver cirrhosis. Am. J. Clin. Nutr. 1999, 69, 1194–1201. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leevy, C.M. Moroianu SA: Nutritional aspects of alcoholic liver disease. Clin. Liver Dis. 2005, 9, 67–81. [Google Scholar] [CrossRef] [PubMed]
- Molfino, A.; Johnson, S.; Medici, V. The challenges of nutritional assessment in cirrhosis. Curr. Nutr. Rep. 2017, 6, 274–280. [Google Scholar] [CrossRef]
- Moriwaki, H.; Miwa, Y.; Tajika, M.; Kato, M.; Fukushima, H.; Shiraki, M. Branched-chain amino acids as a protein- and energy-source in liver cirrhosis. Biochem. Biophys. Res. Commun. 2004, 313, 405–409. [Google Scholar] [CrossRef]
- Hanai, T.; Shiraki, M.; Nishimura, K.; Ohnishi, S.; Imai, K.; Suetsugu, A.; Takai, K.; Shimizu, M.; Moriwaki, H. Sarcopenia impairs prognosis of patients with liver cirrhosis. Nutrition 2015, 31, 193–199. [Google Scholar] [CrossRef]
- Merli, M.; Riggio, O.; Dally, L. Does malnutrition affect survival in cirrhosis? PINC (Policentrica Italiana Nutrizione Cirrosi). Hepatology 1996, 23, 1041–1046. [Google Scholar] [CrossRef] [PubMed]
- Sam, J.; Nguyen, G.C. Protein-calorie malnutrition as a prognostic indicator of mortality among patients hospitalized with cirrhosis and portal hypertension. Liver Int. 2009, 29, 1396–1402. [Google Scholar] [CrossRef]
- Johnson, T.M.; Overgard, E.B.; Cohen, A.E.; DiBaise, J.K. Nutrition assessment and management in advanced liver disease. Nutr. Clin. Pract. 2013, 28, 15–29. [Google Scholar] [CrossRef] [PubMed]
- Thandassery, R.B.; Montano-Loza, A.J. Role of nutrition and muscle in cirrhosis. Curr. Treat. Options Gastroenterol. 2016, 14, 257–273. [Google Scholar] [CrossRef] [PubMed]
- Correia, M.I.; Waitzberg, D.L. The impact of malnutrition on morbidity, mortality, length of hospital stay and costs evaluated through a multivariate model analysis. Clin. Nutr. 2003, 22, 235–239. [Google Scholar] [CrossRef]
- Villet, S.; Chiolero, R.L.; Bollmann, M.D.; Revelly, J.P.; Cayeux, R.N.M.; Delarue, J.; Berger, M.M. Negative impact of hypocaloric feeding and energy balance on clinical outcome in ICU patients. Clin. Nutr. 2005, 24, 502–509. [Google Scholar] [CrossRef]
- Murray, M.J.; Marsh, H.M.; Wochos, D.N.; Moxness, K.E.; Offord, K.P.; Callaway, C.W. Nutritional assessment of intensive-care unit patients. Mayo Clin. Proc. 1988, 63, 1106–1115. [Google Scholar] [CrossRef]
- Preiser, J.C.; van Zanten, A.R.; Berger, M.M.; Biolo, G.; Casaer, M.P.; Doig, G.S.; Griffiths, R.D.; Heyland, D.K.; Hiesmayr, M.; Iapichino, G.; et al. Metabolic and nutritional support of critically ill patients: Consensus and controversies. Crit. Care 2015, 19, 35. [Google Scholar] [CrossRef] [Green Version]
- Heyland, D.K.; Dhaliwal, R.; Jiang, X.; Day, A.G. Identifying critically ill patients who benefit the most from nutrition therapy: The development and initial validation of a novel risk assessment tool. Crit. Care 2011, 15, R268. [Google Scholar] [CrossRef] [Green Version]
- Kondrup, J.; Allison, S.P.; Elia, M.; Vellas, B.; Plauth, M. Educational, clinical practice committee ESoP, Enteral N: ESPEN guidelines for nutrition screening 2002. Clin. Nutr. 2003, 22, 415–421. [Google Scholar] [CrossRef]
- Rahman, A.; Hasan, R.M.; Agarwala, R.; Martin, C.; Day, A.G.; Heyland, D.K. Identifying critically-ill patients who will benefit most from nutritional therapy: Further validation of the “modified NUTRIC” nutritional risk assessment tool. Clin. Nutr. 2016, 35, 158–162. [Google Scholar] [CrossRef] [PubMed]
- Plauth, M.; Bernal, W.; Dasarathy, S.; Merli, M.; Plank, L.D.; Schutz, T.; Bischoff, S.C. ESPEN guideline on clinical nutrition in liver disease. Clin. Nutr. 2019, 38, 485–521. [Google Scholar] [CrossRef] [Green Version]
- Garcia-Tsao, G. Bacterial infections in cirrhosis: Treatment and prophylaxis. J. Hepatol. 2005, 42, S85–S92. [Google Scholar] [CrossRef] [PubMed]
- Albillos, A.; Lario, M.; Alvarez-Mon, M. Cirrhosis-associated immune dysfunction: Distinctive features and clinical relevance. J. Hepatol. 2014, 61, 1385–1396. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wong, F.; Bernardi, M.; Balk, R.; Christman, B.; Moreau, R.; Garcia-Tsao, G.; Patch, D.; Soriano, G.; Hoefs, J.; Navasa, M. International ascites C: Sepsis in cirrhosis: Report on the 7th meeting of the International Ascites Club. Gut 2005, 54, 718–725. [Google Scholar] [CrossRef] [Green Version]
- Papp, M.; Vitalis, Z.; Altorjay, I.; Tornai, I.; Udvardy, M.; Harsfalvi, J.; Vida, A.; Kappelmayer, J.; Lakatos, P.L.; Antal-Szalmas, P. Acute phase proteins in the diagnosis and prediction of cirrhosis associated bacterial infections. Liver Int. 2012, 32, 603–611. [Google Scholar] [CrossRef]
- Ximenes, R.O.; Farias, A.Q.; Scalabrini Neto, A.; Diniz, M.A.; Kubota, G.T.; Ivo, M.M.; Colacique, C.G.; D’Albuquerque, L.A.; Daglius Dias, R. Patients with cirrhosis in the ED: Early predictors of infection and mortality. Am. J. Emerg. Med. 2016, 34, 25–29. [Google Scholar] [CrossRef]
- Navasa, M.; Follo, A.; Filella, X.; Jimenez, W.; Francitorra, A.; Planas, R.; Rimola, A.; Arroyo, V.; Rodes, J. Tumor necrosis factor and interleukin-6 in spontaneous bacterial peritonitis in cirrhosis: Relationship with the development of renal impairment and mortality. Hepatology 1998, 27, 1227–1232. [Google Scholar] [CrossRef]
- Connert, S.; Stremmel, W.; Elsing, C. Procalcitonin is a valid marker of infection in decompensated cirrhosis. Z Gastroenterol. 2003, 41, 165–170. [Google Scholar] [CrossRef]
- Prieto-Frias, C.; Conchillo, M.; Payeras, M.; Inarrairaegui, M.; Davola, D.; Fruhbeck, G.; Salvador, J.; Rodriguez, M.; Richter, J.A.; Mugueta, C.; et al. Factors related to increased resting energy expenditure in men with liver cirrhosis. Eur. J. Gastroenterol. Hepatol. 2016, 28, 139–145. [Google Scholar] [CrossRef]
- Jeong, D.H.; Hong, S.B.; Lim, C.M.; Koh, Y.; Seo, J.; Kim, Y.; Min, J.Y.; Huh, J.W. Comparison of accuracy of NUTRIC and modified NUTRIC scores in predicting 28-day mortality in patients with sepsis: A single center retrospective study. Nutrients 2018, 10, 911. [Google Scholar] [CrossRef] [Green Version]
- Mukhopadhyay, A.; Henry, J.; Ong, V.; Leong, C.S.; The, A.L.; van Dam, R.M.; Kowitlawakul, Y. Association of modified NUTRIC score with 28-day mortality in critically ill patients. Clin. Nutr. 2017, 36, 1143–1148. [Google Scholar] [CrossRef] [PubMed]
- De Vries, M.C.; Koekkoek, W.K.; Opdam, M.H.; van Blokland, D.; van Zanten, A.R. Nutritional assessment of critically ill patients: Validation of the modified NUTRIC score. Eur. J. Clin. Nutr. 2018, 72, 428–435. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mendes, R.; Policarpo, S.; Fortuna, P.; Alves, M.; Virella, D.; Heyland, D.K.; Portuguese, N.S.G. Nutritional risk assessment and cultural validation of the modified NUTRIC score in critically ill patients-A multicenter prospective cohort study. J. Crit. Care 2017, 37, 45–49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsai, M.H.; Huang, H.C.; Peng, Y.S.; Chen, Y.C.; Tian, Y.C.; Yang, C.W.; Lien, J.M.; Fang, J.T.; Hou, M.C.; Shen, C.H.; et al. Nutrition risk assessment using the modified NUTRIC score in cirrhotic patients with acute gastroesophageal variceal bleeding: Prevalence of high nutrition risk and its independent prognostic value. Nutrients 2019, 11, 2152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jensen, G.L.; Mirtallo, J.; Compher, C.; Dhaliwal, R.; Forbes, A.; Grijalba, R.F.; Hardy, G.; Kondrup, J.; Labadarios, D.; Nyulasi, I.; et al. Adult starvation and disease-related malnutrition: A proposal for etiology-based diagnosis in the clinical practice setting from the International Consensus Guideline Committee. JPEN J. Parenter. Enteral. Nutr. 2010, 34, 156–159. [Google Scholar] [CrossRef]
- Compher, C.; Chittams, J.; Sammarco, T.; Higashibeppu, N.; Higashiguchi, T.; Heyland, D.K. Greater nutrient intake is associated with lower mortality in western and eastern critically ill patients with low BMI: A multicenter, multinational observational study. JPEN J. Parenter. Enteral. Nutr. 2019, 43, 63–69. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variables | Scoring System (Points) | |||
|---|---|---|---|---|
| Included in NUTRIC | 0 | 1 | 2 | 3 |
| Ages, years | <50 | 50–74 | ≥75 | |
| Co-morbidities | 0–1 | ≥2 | ||
| Days from hospital to ICU | 0 | ≥1 | ||
| APACHE | <15 | 15–19 | 20–27 | ≥28 |
| SOFA | <6 | 6–9 | ≥10 | |
| Interleukin 6, pg/mL | <400 | ≥400 | ||
| Low NUTRIC | 0–5 Points | |||
| High NUTRIC | 6–10 Points | |||
| Modified NUTRIC | (without Interleukin 6) | |||
| Low mNUTRIC | 0–4 Points | |||
| High mNUTRIC | 5–9 Points | |||
| Male sex, n/total (%) | 72/114 (63%) |
| Age, years | 61 (52–67) |
| Body weight, kg | 75 (68–85) |
| Body height, cm | 175 (167–180) |
| BMI, kg/m2 | 24.8 (22.5–27.7) |
| APACHE II | 22 (17–28) |
| SOFA | 10 (8–13) |
| MELD | 26 (22–32) |
| Child-Pugh | 11 (10–13) |
| Child C, n/total (%) | 98/114 (86%) |
| Etiology of cirrhosis, n/total (%) | Alcoholic 78/114 (68%) |
| Viral 9/114 (8%) | |
| Autoimmune 5/114 (4%) | |
| Cryptogenic/NAFLD 22/114 (20%) | |
| Admission diagnoses, n/total (%) | Sepsis/Pneumonia 50/114 (44%) |
| Acute kidney failure/HRS 24/114 (21%) | |
| Gastrointestinal bleeding 20/114 (18%) | |
| Encephalopathy/delirium 20/114 (17%) | |
| Length of ICU stay, days | 13 (6–22) |
| 28-day mortality, n/total (%) | 50/114 (44%) |
| 3-month mortality, n/total (%) | 69/114 (61%) |
| Clinical cause of death, n/total (%) | Sepsis, Pneumonia 41/69 (61%) |
| Cardiocirculatory failure 13/69 (19%) | |
| Gastrointestinal bleeding 11/69 (16%) | |
| Central-nervous limitations 3/69 (4%) | |
| Baseline creatinine, mg/dL | 1.8 (1.2–2.7) |
| Dialysis before ICU, n/total (%) | 2/114 (1.8%) |
| Dialysis during ICU, n/total (%) | 66/112 (59%) |
| NUTRIC, n = 114 | mNUTRIC, n = 114 | |||||
|---|---|---|---|---|---|---|
| Low NUTRIC 0–5 n = 40 | High NUTRIC 6–10 n = 74 | p-Value | Low mNUTRIC 0–4 n = 29 | High mNUTRIC 5–9 n = 85 | p-Value | |
| Age, years | 55 (43–61) | 64 (55–68) | <0.001 | 54 (44–60) | 63 (55–68) | <0.001 |
| Height, cm | 175 (167–177) | 175 (167–180) | 0.449 | 174 (167–177) | 175 (168–180) | 0.155 |
| Weight, kg | 73 (65–81) | 76 (69–85) | 0.206 | 71 (64–79) | 76 (69–85) | 0.056 |
| BMI, kg/m2 | 23.8 (21.8–27.4) | 25.2 (22.7–28.0) | 0.200 | 23.7 (22.0–26.9) | 25.2 (22.5–28.3) | 0.134 |
| Albumin, g/dL | 3.3 (2.7–3.9) | 3.0 (2.5–3.5) | 0.048 | 3.4 (2.9–3.9) | 3.0 (2.5–3.6) | 0.050 |
| Co-morbidities | 2 (2–3) | 3 (3–4) | <0.001 | 2 (2–3) | 3 (3–4) | <0.001 |
| Days from hospital to ICU | 1 (0–3) | 3 (1–5) | 0.006 | 1 (0–3) | 3 (1–5) | 0.029 |
| Interleukin 6, pg/mL | 64 (32–160) | 246 (57–895) | <0.001 | 40 (23–127) | 204 (60–694) | <0.001 |
| Creatinine, mg/dL | 1.3 (1.0–1.9) | 2.2 (1.6–3.2) | <0.001 | 1.1 (0.8–1.7) | 2.1 (1.5–3.1) | <0.001 |
| APACHE | 17 (14–18) | 25 (22–29) | <0.001 | 15 (12–17) | 25 (22–28) | <0.001 |
| SOFA | 6 (5–8) | 12 (10–15) | <0.001 | 6 (4–7) | 11 (9–15) | <0.001 |
| MELD | 23 (20–28) | 28 (24–34) | <0.001 | 22 (20–26) | 27 (23–34) | <0.001 |
| CHILD | 9 (10–12) | 12 (11–13) | <0.001 | 10 (9–11) | 12 (11–13) | <0.001 |
| Length of ICU stay, days | 6 (3–17) | 16 (9–23) | <0.001 | 6 (3–14) | 15 (8–24) | <0.001 |
| 28-day mortality n/total (%) | 7/40 (18%) | 43/74 (58%) | <0.001 | 4/29 (14%) | 46/85 (54%) | <0.001 |
| 3-month mortality n/total (%) | 10/40 (25%) | 59/74 (80%) | <0.001 | 6/29 (21%) | 63/85 (74%) | <0.001 |
| Spearman’s Coefficient rs | Linear Regression R2 | p-Value | ||
|---|---|---|---|---|
| MELD | NUTRIC | 0.492 | 0.247 | <0.001 |
| mNUTRIC | 0.475 | 0.224 | <0.001 | |
| CHILD | NUTRIC | 0.441 | 0.203 | <0.001 |
| mNUTRIC | 0.413 | 0.180 | <0.001 | |
| IL6 | NUTRIC | 0.574 | 0.034 | <0.001 |
| mNUTRIC | 0.446 | 0.021 | <0.001 | |
| albumin | NUTRIC | −0.249 | 0.061 | 0.010 |
| mNUTRIC | −0.232 | 0.052 | 0.013 | |
| BMI | NUTRIC | 0.067 | 0.005 | 0.479 |
| mNUTRIC | 0.076 | 0.006 | 0.422 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mayr, U.; Pfau, J.; Lukas, M.; Bauer, U.; Herner, A.; Rasch, S.; Schmid, R.M.; Huber, W.; Lahmer, T.; Batres-Baires, G. NUTRIC and Modified NUTRIC are Accurate Predictors of Outcome in End-Stage Liver Disease: A Validation in Critically Ill Patients with Liver Cirrhosis. Nutrients 2020, 12, 2134. https://doi.org/10.3390/nu12072134
Mayr U, Pfau J, Lukas M, Bauer U, Herner A, Rasch S, Schmid RM, Huber W, Lahmer T, Batres-Baires G. NUTRIC and Modified NUTRIC are Accurate Predictors of Outcome in End-Stage Liver Disease: A Validation in Critically Ill Patients with Liver Cirrhosis. Nutrients. 2020; 12(7):2134. https://doi.org/10.3390/nu12072134
Chicago/Turabian StyleMayr, Ulrich, Julia Pfau, Marina Lukas, Ulrike Bauer, Alexander Herner, Sebastian Rasch, Roland M. Schmid, Wolfgang Huber, Tobias Lahmer, and Gonzalo Batres-Baires. 2020. "NUTRIC and Modified NUTRIC are Accurate Predictors of Outcome in End-Stage Liver Disease: A Validation in Critically Ill Patients with Liver Cirrhosis" Nutrients 12, no. 7: 2134. https://doi.org/10.3390/nu12072134