A Protein/Lipid Preload Attenuates Glucose-Induced Endothelial Dysfunction in Individuals with Abnormal Glucose Tolerance

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Study Design
2.3. Metabolic Tests
2.4. Peripheral Arterial Tonometry (PAT)
2.5. Analytical Methods and Calculations
2.6. Statistical Analysis
3. Results
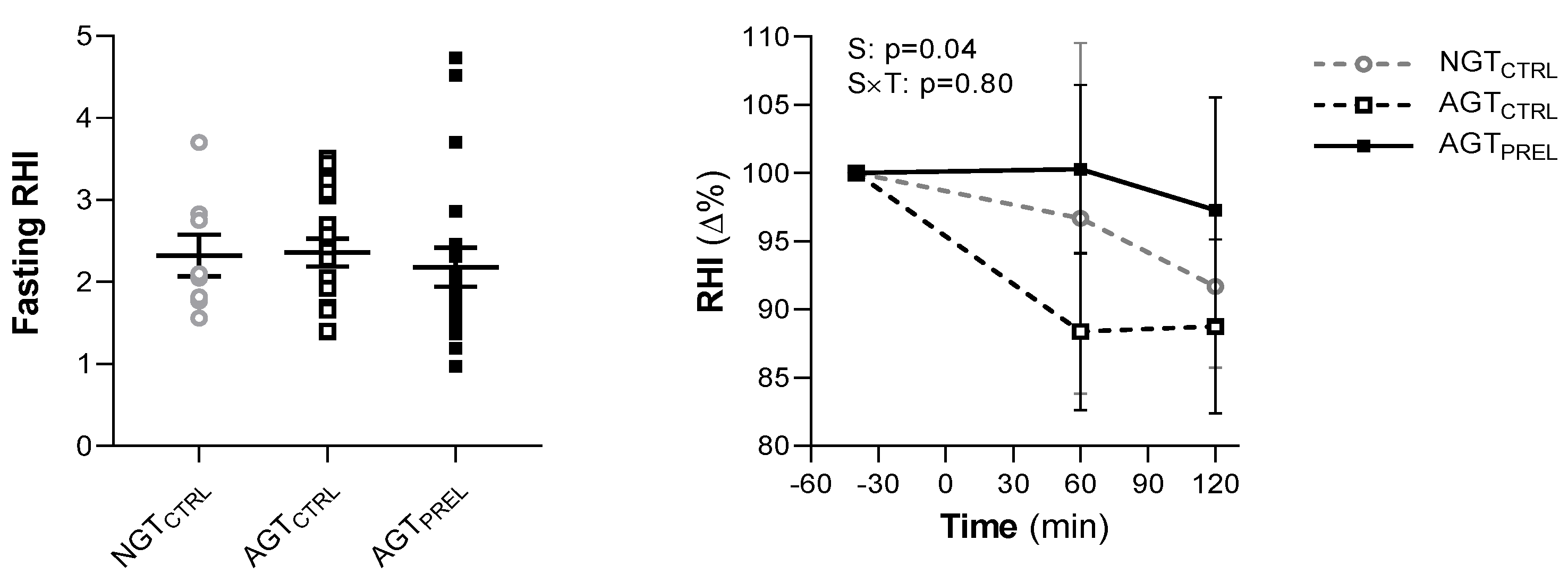
3.1. Fasting and Post-Glucose Endothelial Function
3.2. Effect of Nutrients on Post-Glucose Endothelial Dysfunction
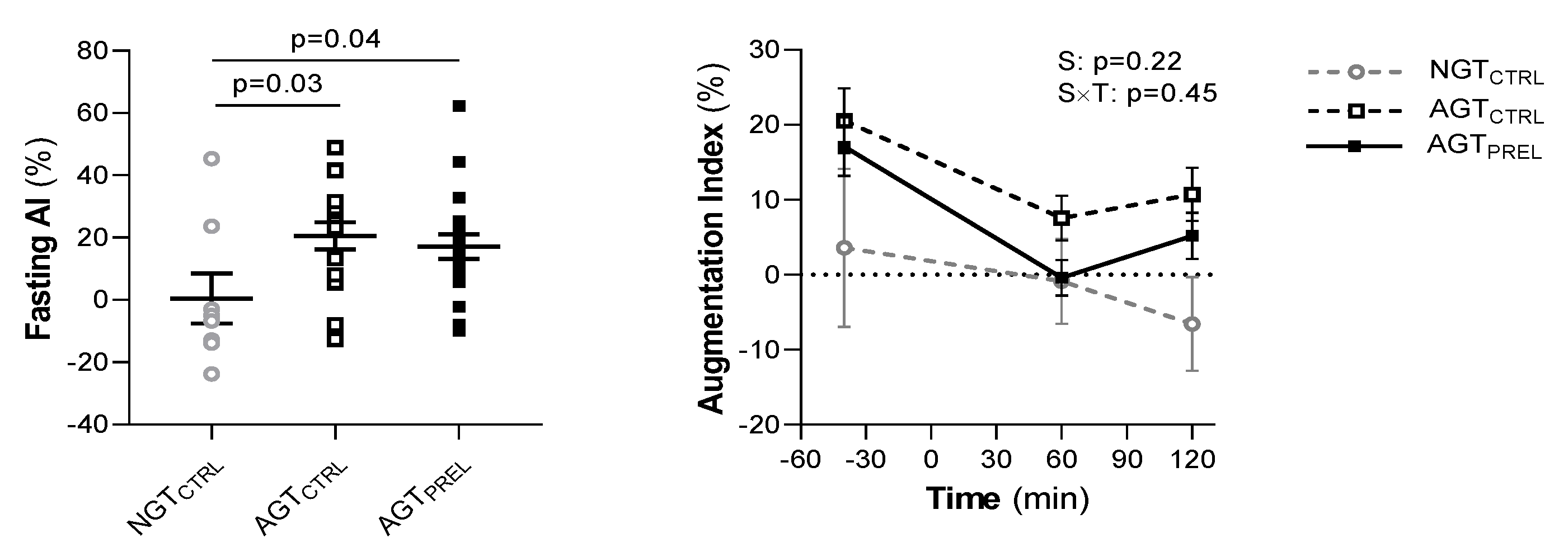
3.3. Fasting and Post-Glucose Arterial Stiffness
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| AA | Amino acid |
| AGT | Abnormal glucose tolerance |
| AI | Augmentation index |
| AI@75 | AI normalized to heart rate of 75 bpm |
| AUC | Area under the curve |
| BCAA | Branched-chain amino acid |
| eNOS | Endothelial nitric oxide synthase |
| FFA | Free fatty acid |
| FMD | Flow mediated dilation |
| GIP | Glucose-dependent insulinotropic polypeptide |
| GLP-1 | Glucagon-like peptide-1 |
| HbA1c | Glycated hemoglobin |
| HIRI | Hepatic insulin resistance index |
| HOMA-IR | Homeostatic model assessment for insulin resistance |
| IGT | Impaired glucose tolerance |
| NGT | Normal glucose tolerance |
| NO | Nitric oxide |
| OGIS | Oral glucose insulin sensitivity |
| OGTT | Oral glucose tolerance test |
| RHI | Reactive hyperemia index |
| T2D | Type 2 diabetes |
References
- Heintjes, E.M.; Houben, E.; Beekman-Hendriks, W.L.; Lighaam, E.; Cremers, S.M.; Penning van Beest, F.J.A.; Stehouwer, C.D.A.; Herings, R.M.C. Trends in mortality, cardiovascular complications, and risk factors in type 2 diabetes. Neth. J. Med. 2019, 77, 317–329. [Google Scholar] [PubMed]
- Williams, S.B.; Goldfine, A.B.; Timimi, F.K.; Ting, H.H.; Roddy, M.-A.; Simonson, D.C.; Creager, M.A. Acute hyperglycemia attenuates endothelium-dependent vasodilation in humans in vivo. Circulation 1998, 97, 1695–1701. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Su, Y.; Liu, X.-M.; Sun, Y.-M.; Jin, H.-B.; Fu, R.; Wang, Y.-Y.; Wu, Y.; Luan, Y. The relationship between endothelial dysfunction and oxidative stress in diabetes and prediabetes. Int. J. Clin. Pract. 2008, 62, 877–882. [Google Scholar] [CrossRef] [PubMed]
- Loader, J.; Montero, D.; Lorenzen, C.; Watts, R.; Méziat, C.; Reboul, C.; Stewart, S.; Walther, G. Acute hyperglycemia impairs vascular function in healthy and cardiometabolic diseased subjects. Arterioscler. Thromb. Vasc. Biol. 2015, 35, 2060–2072. [Google Scholar] [CrossRef] [Green Version]
- Mann, B.K.; Bhandohal, J.S.; Hong, J. An overall glance of evidence supportive of one-hour and two-hour postload plasma glucose levels as predictors of long-term cardiovascular events. Int. J. Endocrinol. 2019, 2019, 6048954. [Google Scholar] [CrossRef]
- Vita, J.A.; Treasure, C.B.; Nabel, E.G.; McLenachan, J.M.; Fish, R.D.; Yeung, A.C.; Vekshtein, V.I.; Selwyn, A.P.; Ganz, P. Coronary vasomotor response to acetylcholine relates to risk factors for coronary artery disease. Circulation 1990, 81, 491–497. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DECODE Study Group. Glucose tolerance and cardiovascular mortality. Arch. Intern. Med. 2001, 161, 397. [Google Scholar] [CrossRef] [PubMed]
- Costantino, S.; Paneni, F.; Battista, R.; Castello, L.; Capretti, G.; Chiandotto, S.; Tanese, L.; Russo, G.; Pitocco, D.; Lanza, G.A.; et al. Impact of glycemic variability on chromatin remodeling, oxidative stress, and endothelial dysfunction in patients with type 2 diabetes and with target HbA 1c levels. Diabetes 2017, 66, 2472–2482. [Google Scholar] [CrossRef] [Green Version]
- Kawano, H.; Motoyama, T.; Hirashima, O.; Hirai, N.; Miyao, Y.; Sakamoto, T.; Kugiyama, K.; Ogawa, H.; Yasue, H. Hyperglycemia rapidly suppresses flow-mediated endothelium- dependent vasodilation of brachial artery. J. Am. Coll. Cardiol. 1999, 34, 146–154. [Google Scholar] [CrossRef] [Green Version]
- Mah, E.; Noh, S.K.; Ballard, K.; Matos, M.E.; Volek, J.S.; Bruno, R.S. Postprandial hyperglycemia impairs vascular endothelial function in healthy men by inducing lipid peroxidation and increasing asymmetric dimethylarginine: Arginine. J. Nutr. 2011, 141, 1961–1968. [Google Scholar] [CrossRef]
- Romero, M.; Iddings, J.; Platt, D.H.; Ali, M.I.; Cederbaum, S.D.; Stepp, D.W.; Caldwell, R.B.; Caldwell, R.W. Diabetes-induced vascular dysfunction involves arginase I. Am. J. Physiol. Circ. Physiol. 2012, 302, H159–H166. [Google Scholar] [CrossRef] [Green Version]
- Zhenyukh, O.; González-Amor, M.; Rodrigues-Diez, R.R.; Esteban, V.; Ruiz-Ortega, M.; Salaices, M.; Mas, S.; Briones, A.M.; Egido, J. Branched-chain amino acids promote endothelial dysfunction through increased reactive oxygen species generation and inflammation. J. Cell. Mol. Med. 2018, 22, 4948–4962. [Google Scholar] [CrossRef] [PubMed]
- Vogel, R.A.; Corretti, M.C.; Plotnick, G.D. Effect of a single high-fat meal on endothelial function in healthy subjects. Am. J. Cardiol. 1997, 79, 350–354. [Google Scholar] [CrossRef]
- Ceriello, A.; Esposito, K.; Testa, R.; Bonfigli, A.; Marra, M.; Giugliano, D. The possible protective role of glucagon-like peptide 1 on endothelium during the meal and evidence for an “endothelial resistance” to glucagon-like peptide 1 in diabetes. Diabetes Care 2011, 34, 697–702. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muniyappa, R.; Sowers, J.R. Role of insulin resistance in endothelial dysfunction. Rev. Endocr. Metab. Disord. 2013, 14, 5–12. [Google Scholar] [CrossRef]
- Tricò, D.; Baldi, S.; Tulipani, A.; Frascerra, S.; Macedo, M.P.; Mari, A.; Ferrannini, E.; Natali, A. Mechanisms through which a small protein and lipid preload improves glucose tolerance. Diabetology 2015, 58, 2503–2512. [Google Scholar] [CrossRef]
- Tricò, D.; Filice, E.; Trifirò, S.; Natali, A. Manipulating the sequence of food ingestion improves glycemic control in type 2 diabetic patients under free-living conditions. Nutr. Diabetes 2016, 6, e226. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tricò, D.; Filice, E.; Baldi, S.; Frascerra, S.; Mari, A.; Natali, A. Sustained effects of a protein and lipid preload on glucose tolerance in type 2 diabetes patients. Diabetes Metab. 2016, 42, 242–248. [Google Scholar] [CrossRef]
- Jakubowicz, D.; Froy, O.; Ahren, B.; Boaz, M.; Landau, Z.; Bar-Dayan, Y.; Ganz, T.; Barnea, M.; Wainstein, J. Incretin, insulinotropic and glucose-lowering effects of whey protein pre-load in type 2 diabetes: A randomised clinical trial. Diabetology 2014, 57, 1807–1811. [Google Scholar] [CrossRef]
- Ma, J.; Jesudason, D.R.; Stevens, J.E.; Keogh, J.; Jones, K.L.; Clifton, P.M.; Horowitz, M.; Rayner, C.K. Sustained effects of a protein ‘preload’ on glycaemia and gastric emptying over 4 weeks in patients with type 2 diabetes: A randomized clinical trial. Diabetes Res. Clin. Pract. 2015, 108, e31–e34. [Google Scholar] [CrossRef]
- Shukla, A.P.; Iliescu, R.G.; Thomas, C.; Aronne, L.J. Food order has a significant impact on postprandial glucose and insulin levels: Table 1. Diabetes Care 2015, 38, e98–e99. [Google Scholar] [CrossRef] [Green Version]
- Wu, T.; Little, T.; Bound, M.J.; Borg, M.; Zhang, X.; Deacon, C.F.; Horowitz, M.; Jones, K.L.; Rayner, C.K. A protein preload enhances the glucose-lowering efficacy of vildagliptin in type 2 diabetes. Diabetes Care 2016, 39, 511–517. [Google Scholar] [CrossRef] [Green Version]
- Kuwata, H.; Iwasaki, M.; Shimizu, S.; Minami, K.; Maeda, H.; Seino, S.; Nakada, K.; Nosaka, C.; Murotani, K.; Kurose, T.; et al. Meal sequence and glucose excursion, gastric emptying and incretin secretion in type 2 diabetes: A randomised, controlled crossover, exploratory trial. Diabetology 2015, 59, 453–461. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tricò, D.; Natali, A. Modulation of postprandial glycemic responses by noncarbohydrate nutrients provides novel approaches to the prevention and treatment of type 2 diabetes. Am. J. Clin. Nutr. 2017, 106, 701–702. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nesti, L.; Mengozzi, A.; Tricò, D. Impact of nutrient type and sequence on glucose tolerance: Physiological insights and therapeutic implications. Front. Endocrinol. 2019, 10, 144. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association 2. Classification and diagnosis of diabetes: Standards of medical care in diabetes—2020. Diabetes Care 2019, 43, S14–S31. [Google Scholar] [CrossRef] [Green Version]
- Tricò, D.; Frascerra, S.; Baldi, S.; Mengozzi, A.; Nesti, L.; Mari, A.; Natali, A. The insulinotropic effect of a high-protein nutrient preload is mediated by the increase of plasma amino acids in type 2 diabetes. Eur. J. Nutr. 2018, 58, 2253–2261. [Google Scholar] [CrossRef]
- Bonetti, P.O.; Pumper, G.M.; Higano, S.T.; Holmes, D.R.; Kuvin, J.T.; Lerman, L.O. Noninvasive identification of patients with early coronary atherosclerosis by assessment of digital reactive hyperemia. J. Am. Coll. Cardiol. 2004, 44, 2137–2141. [Google Scholar] [CrossRef] [Green Version]
- Axtell, A.L.; Gomari, F.A.; Cooke, J.P. Assessing endothelial vasodilator function with the Endo-PAT 2000. J. Vis. Exp. 2010. [Google Scholar] [CrossRef] [Green Version]
- Venturi, E.; Pinnola, S.; Morizzo, C.; Boldrini, B.; Rossi, M.; Trifirò, S.; Tricò, D.; Natali, A.; The SUMMIT study group. Clinical phenotype and microvascular dynamics of subjects with endothelial dysfunction as assessed by peripheral tonometry. Microcirculation 2016, 23, 230–239. [Google Scholar] [CrossRef]
- Mari, A.; Pacini, G.; Murphy, E.; Ludvik, B.; Nolan, J.J. A model-based method for assessing insulin sensitivity from the oral glucose tolerance test. Diabetes Care 2001, 24, 539–548. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abdul-Ghani, M.A.; Matsuda, M.; Balas, B.; DeFronzo, R.A. Muscle and liver insulin resistance indexes derived from the oral glucose tolerance test. Diabetes Care 2006, 30, 89–94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Loader, J.; Meziat, C.; Watts, R.; Lorenzen, C.; Sigaudo-Roussel, D.; Stewart, S.; Reboul, C.; Meyer, G.; Walther, G. Effects of sugar-sweetened beverage consumption on microvascular and macrovascular function in a healthy population. Arter. Thromb. Vasc. Biol. 2017, 37, 1250–1260. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nohria, A.; Gerhard-Herman, M.; Creager, M.A.; Hurley, S.; Mitra, D.; Ganz, P. Role of nitric oxide in the regulation of digital pulse volume amplitude in humans. J. Appl. Physiol. 2006, 101, 545–548. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Green, D.J.; Dawson, E.A.; Groenewoud, H.M.; Jones, H.; Thijssen, D.H.J. Is flow-mediated dilation nitric oxide mediated? Hypertension 2014, 63, 376–382. [Google Scholar] [CrossRef] [Green Version]
- Kovac, J.R.; Gomez, L.; Smith, R.P.; Coward, R.M.; Gonzales, M.A.; Khera, M.; Lamb, L.J.; Lipshultz, L.I. Measurement of endothelial dysfunction via peripheral arterial tonometry predicts vasculogenic erectile dysfunction. Int. J. Impot. Res. 2014, 26, 218–222. [Google Scholar] [CrossRef] [Green Version]
- Meza, C.A.; La Favor, J.D.; Kim, D.-H.; Hickner, R.C. Endothelial dysfunction: Is there a hyperglycemia-induced Imbalance of NOX and NOS? Int. J. Mol. Sci. 2019, 20, 3775. [Google Scholar] [CrossRef] [Green Version]
- Stuehr, D.; Pou, S.; Rosen, G.M. Oxygen reduction by nitric-oxide synthases. J. Biol. Chem. 2001, 276, 14533–14536. [Google Scholar] [CrossRef] [Green Version]
- Tanaka, J.; Qiang, L.; Banks, A.S.; Welch, C.L.; Matsumoto, M.; Kitamura, T.; Ido-Kitamura, Y.; Depinho, R.A.; Accili, M. Foxo1 links hyperglycemia to LDL oxidation and endothelial nitric oxide synthase dysfunction in vascular endothelial cells. Diabetes 2009, 58, 2344–2354. [Google Scholar] [CrossRef] [Green Version]
- Gorin, Y.; Block, K. Nox as a target for diabetic complications. Clin. Sci. 2013, 125, 361–382. [Google Scholar] [CrossRef] [Green Version]
- Sibal, L.; Agarwal, S.C.; Home, P.D.; Boger, R.H. The role of Asymmetric Dimethylarginine (ADMA) in endothelial dysfunction and cardiovascular disease. Curr. Cardiol. Rev. 2010, 6, 82–90. [Google Scholar] [CrossRef]
- Thazhath, S.S.; Wu, T.; Bound, M.J.; Checklin, H.L.; Jones, K.L.; Willoughby, S.; Horowitz, M.; Rayner, C.K. Changes in meal composition and duration affect postprandial endothelial function in healthy humans. Am. J. Physiol. Liver Physiol. 2014, 307, G1191–G1197. [Google Scholar] [CrossRef] [Green Version]
- Westerbacka, J.; Vehkavaara, S.; Bergholm, R.; Wilkinson, I.; Cockcroft, J.; Yki-Jarvinen, H. Marked resistance of the ability of insulin to decrease arterial stiffness characterizes human obesity. Diabetes 1999, 48, 821–827. [Google Scholar] [CrossRef]
- Zheng, C.; Liu, Z. Vascular function, insulin action, and exercise: An intricate interplay. Trends Endocrinol. Metab. 2015, 26, 297–304. [Google Scholar] [CrossRef] [Green Version]
- Olver, T.D.; Grunewald, Z.I.; Ghiarone, T.; Restaino, R.M.; Sales, A.R.K.; Park, L.K.; Thorne, P.K.; Ganga, R.R.; Emter, C.A.; Lemon, P.W.R.; et al. Persistent insulin signaling coupled with restricted PI3K activation causes insulin-induced vasoconstriction. Am. J. Physiol. Circ. Physiol. 2019, 317, H1166–H1172. [Google Scholar] [CrossRef] [PubMed]
- Natali, A.; Baldi, S.; Vittone, F.; Muscelli, E.; Casolaro, A.; Morgantini, C.; Palombo, C.; Ferrannini, E. Effects of glucose tolerance on the changes provoked by glucose ingestion in microvascular function. Diabetology 2008, 51, 862–871. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nystrom, T.; Gutniak, M.K.; Zhang, Q.; Zhang, F.; Holst, J.J.; Ahren, B.; Sjöholm, Å. Effects of glucagon-like peptide-1 on endothelial function in type 2 diabetes patients with stable coronary artery disease. Am. J. Physiol. Metab. 2004, 287, E1209–E1215. [Google Scholar] [CrossRef] [PubMed]
- Torimoto, K.; Okada, Y.; Mori, H.; Otsuka, T.; Kawaguchi, M.; Matsuda, M.; Kuno, F.; Sugai, K.; Sonoda, S.; Hajime, M.; et al. Effects of exenatide on postprandial vascular endothelial dysfunction in type 2 diabetes mellitus. Cardiovasc. Diabetol. 2015, 14, 25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thengchaisri, N. Upregulation of arginase by H2O2 impairs endothelium-dependent nitric oxide-mediated dilation of coronary arterioles. Arter. Thromb. Vasc. Biol. 2006, 26, 2035–2042. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mahdi, A.; Kövamees, O.; Checa, A.; Wheelock, C.E.; Von Heijne, M.; Alvarsson, M.; Pernow, J. Arginase inhibition improves endothelial function in patients with type 2 diabetes mellitus despite intensive glucose-lowering therapy. J. Intern. Med. 2018, 284, 388–398. [Google Scholar] [CrossRef]
- McDonald, J.D.; Mah, E.; Chitchumroonchokchai, C.; Reverri, E.J.; Li, J.; Volek, J.S.; Villamena, F.A.; Bruno, R.S. Co-ingestion of whole eggs or egg whites with glucose protects against postprandial hyperglycaemia-induced oxidative stress and dysregulated arginine metabolism in association with improved vascular endothelial function in prediabetic men. Br. J. Nutr. 2018, 120, 901–913. [Google Scholar] [CrossRef]
- Konukoglu, D.; Fırtına, S.; Serin, O.; Konukoǧlu, D.; Firtina, S. The relationship between plasma asymmetrical dimethyl-l-arginine and inflammation and adhesion molecule levels in subjects with normal, impaired, and diabetic glucose tolerance. Metabolism 2008, 57, 110–115. [Google Scholar] [CrossRef] [PubMed]
- Steer, P.; Sarabi, D.M.; Karlström, B.; Basu, S.; Berne, C.; Vessby, B.; Lind, L.; Karlstrm, B. The effect of a mixed meal on endothelium-dependent vasodilation is dependent on fat content in healthy humans. Clin. Sci. 2003, 105, 81–87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bock, J.; E Hughes, W.; Casey, D.P. Age-associated differences in central artery responsiveness to sympathoexcitatory stimuli. Am. J. Hypertens. 2019, 32, 564–569. [Google Scholar] [CrossRef] [PubMed]
- Zhou, J.; Li, Y.-S.; Chien, S. Shear stress–initiated signaling and its regulation of endothelial function. Arter. Thromb. Vasc. Biol. 2014, 34, 2191–2198. [Google Scholar] [CrossRef] [Green Version]
- Taylor, J.L.; Curry, T.B.; Matzek, L.J.; Joyner, M.J.; Casey, D.P. Acute effects of a mixed meal on arterial stiffness and central hemodynamics in healthy adults. Am. J. Hypertens. 2013, 27, 331–337. [Google Scholar] [CrossRef] [Green Version]
- Pham, H.; Holen, I.S.; Phillips, L.; Hatzinikolas, S.; Huynh, L.Q.; Wu, T.; Hausken, T.; Rayner, C.K.; Horowitz, M.; Jones, K.L. The effects of a whey protein and guar gum-containing preload on gastric emptying, glycaemia, small intestinal absorption and blood pressure in healthy older subjects. Nutrients 2019, 11, 2666. [Google Scholar] [CrossRef] [Green Version]
- Mitchell, G.F.; Lacourcière, Y.; Arnold, J.M.O.; Dunlap, M.E.; Conlin, P.R.; Izzo, J.L. Changes in aortic stiffness and augmentation index after acute converting enzyme or vasopeptidase inhibition. Hypertension 2005, 46, 1111–1117. [Google Scholar] [CrossRef] [Green Version]
- Cheng, L.-T.; Tang, L.-J.; Cheng, L.; Huang, H.-Y.; Wang, T. Limitation of the augmentation index for evaluating arterial stiffness. Hypertens. Res. 2007, 30, 713–722. [Google Scholar] [CrossRef] [Green Version]
- Sakurai, M.; Yamakado, T.; Kurachi, H.; Kato, T.; Kuroda, K.; Ishisu, R.; Okamoto, S.; Isaka, N.; Nakano, T.; Ito, M. The relationship between aortic augmentation index and pulse wave velocity: An invasive study. J. Hypertens. 2007, 25, 391–397. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| AGT | NGT | p | |
|---|---|---|---|
| N | 22 | 8 | - |
| Age (years) | 50.0 ± 14.2 | 31.8 ± 11.9 | 0.004 |
| Sex (men/women; n (%)) | 14/8 (63.6/36.4) | 4/4 (50.0/50.0) | 0.68 |
| Body Mass Index (kg/m2) | 27.4 ± 5.5 | 26.6 ± 5.1 | 0.64 |
| Systolic Blood Pressure (mmHg) | 121 ± 9 | 109 ± 10 | 0.006 |
| Diastolic Blood Pressure (mmHg) | 78 ± 8 | 69 ± 8 | 0.01 |
| Heart Rate (bpm) | 63 ± 8 | 59 ± 10 | 0.45 |
| Non-smokers/Ex-smokers (n (%)) | 17/5 (77.3/22.7) | 7/1 (87.5/12.5) | 0.99 |
| Fasting Plasma Glucose (mmol/L) | 6.0 ± 1.0 | 5.1 ± 0.5 | 0.02 |
| 2-h Plasma Glucose (mmol/L) | 10.7 ± 2.6 | 6.3 ± 1.1 | <0.0001 |
| Plasma Glucose AUC (mmol × min/L) | 1,213 ± 203 | 852 ± 105 | 0.0002 |
| Glucose tolerance (IGT/T2D; n (%)) | 13/9 [59/41] | - | - |
| HbA1c (%) | 6.1 ± 0.6 | 5.3 ± 0.2 | 0.002 |
| Fasting Plasma Insulin (pmol/L) | 79 [42–120] | 52 [27–75] | 0.09 |
| 2-h Plasma Insulin (pmol/L) | 398 [299–703] | 192 [141–425] | 0.02 |
| Plasma Insulin AUC (nmol × min/L) | 38.9 [31.5–50.7] | 37.9 [30.6–59.8] | 0.96 |
| HOMA-IR (unit) | 3.0 [1.4–4.7] | 1.7 [0.8–2.7] | 0.049 |
| Matsuda Index (unit) | 5.3 [3.4–9.6] | 9.5 [5.1–14.1] | 0.07 |
| OGIS Index (unit) | 357 [313–406] | 416 [386–455] | 0.003 |
| HIRI (unit) | 3.5 [2.6–4.4] | 3.1 [2.4–6.5] | 0.99 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tricò, D.; Nesti, L.; Frascerra, S.; Baldi, S.; Mengozzi, A.; Natali, A. A Protein/Lipid Preload Attenuates Glucose-Induced Endothelial Dysfunction in Individuals with Abnormal Glucose Tolerance. Nutrients 2020, 12, 2053. https://doi.org/10.3390/nu12072053
Tricò D, Nesti L, Frascerra S, Baldi S, Mengozzi A, Natali A. A Protein/Lipid Preload Attenuates Glucose-Induced Endothelial Dysfunction in Individuals with Abnormal Glucose Tolerance. Nutrients. 2020; 12(7):2053. https://doi.org/10.3390/nu12072053
Chicago/Turabian StyleTricò, Domenico, Lorenzo Nesti, Silvia Frascerra, Simona Baldi, Alessandro Mengozzi, and Andrea Natali. 2020. "A Protein/Lipid Preload Attenuates Glucose-Induced Endothelial Dysfunction in Individuals with Abnormal Glucose Tolerance" Nutrients 12, no. 7: 2053. https://doi.org/10.3390/nu12072053