1. Introduction
Sufficient intake of vitamins and minerals, preferably as part of our daily food intake, is generally recommended to prevent chronic diseases and promote health. Sodium, potassium, calcium and magnesium, also known as electrolytes, have numerous biological effects in the human body, whereas their imbalances have a strong impact on personal health. Electrolyte balance is essential for bone composition and function, muscular physiology, neuronal processes, oxygen transport, acid-base homeostasis and many other biological processes. Even small deviations in blood concentrations of electrolytes can lead to serious health problems and even increased mortality [
1].
Sodium (Na) is a cation in the extracellular fluid, which largely determines its volume and osmotic pressure. It is also present in the intracellular fluid, where it contributes to the cell membrane potential and enzymatic reactions. Together with chloride, dietary sodium is mostly consumed with table salt (NaCl) [
2,
3]. Potassium (K) is the most common cation of the intracellular fluid, where it is important for the regulation of membrane potential, maintenance of osmotic pressure, electrolyte homeostasis and acid-base-balance. Potassium also functions in controlling nerve impulses, protein biosynthesis and the conversion of blood sugar into glycogen. Although extracellular potassium only accounts for 2%, both increases and decreases of extracellular potassium concentration can lead to severe neuromuscular or muscular dysfunctions [
4,
5]. Calcium (Ca) plays a crucial role in the formation and maintenance of bone structures and in muscle physiology. It is involved in numerous intracellular signal transduction events and is indispensable for muscle contraction, blood coagulation, hormonal system regulation, nerve impulse transmission as well as energy and fat metabolism [
6]. Magnesium (Mg) is indispensable for various enzymatic reactions, protein/nucleic acid synthesis and energy metabolism [
7].
It was shown that the prevalence of electrolyte imbalances in the general population may reach up to 15% [
8]. Moreover, deviations in electrolyte concentrations can be associated with various diseases such as hypertension [
9,
10,
11,
12,
13], cardiovascular diseases (CVD) [
6,
14,
15,
16,
17], osteoporosis [
18] and diabetes mellitus type/insulin resistance [
19]. Interestingly, major differences in the geographic prevalence of these diseases have been observed in Europe, with higher rates in the eastern and north-eastern, and lower rates in the western and south-western European countries [
20,
21,
22,
23]. This “East–West gradient” was also reported for individual European countries including Germany, France and Austria [
23,
24,
25]. The east–west differences within Austria were also found to be apparent regarding food intake, nutrient profile and body composition. The Austrian Nutrition Report 2012 showed that BMI, waist circumference and body fat percentage in adults were significantly higher in eastern Austria compared to western regions. Additionally, east–west differences in energy and fat intake were also reported [
26].
In Austria, similarly to many other European countries, tradition plays an important role when it comes to food preferences [
27,
28]. The western Austrian region is covered by the central Alps; it is less densely populated and predominantly rural. Several traditional foods—such as typical milk products (e.g., Tyrolean cheese), meat and meat products (e.g., Tyrolean Speck), dumplings and sweet dishes (e.g., Kaiserschmarrn, Germknoedel), as well as soups and stews—are protected and registered in the Database of Origin and Registration by the European Commission [
29]. They are rooted in Austria’s food culture and, therefore, have an important impact on nutrient intake.
Numerous previous studies have suggested that correlations between specific foods or single nutrients with health outcomes can be inconsistent. Instead, analyses of dietary patterns may better reflect complex eating behaviors and enable correlations to be detected of food preferences with the prevalence of certain diseases. Therefore, it is important to recognize differences in dietary patterns and nutrient profiles within a certain population in order to understand possible associations with regional occurrence of nutritional deficits and diseases.
In our previous work, we identified three dietary patterns that are typical for our geographic area, with more than 60% of population following a traditional dietary pattern. This pattern was characterized by a high intake of animal products, traditional sweet dishes, dumplings, soups and stews with regular use of butter, cream and eggs. The second major dietary pattern in Western Austria, a health-conscious pattern (25% of studied population), was represented by high intake of health-promoting foods such as plant-based products. Only 10.8% of the study population followed a western dietary pattern characterized by low consumption of plant-based products, preferential intake of processed meat, fast food and high-sugar beverages [
30].
The aim of the present study was to evaluate the status of electrolyte nutritional intake in Tyrol, western Austria. We further compared electrolyte intake across various age and gender groups and combined data about individual electrolytes with food choices and dietary patterns. Our data relates electrolyte intake to actual food consumption in a tradition-rich region, and provides suggestions for future dietary improvements.
4. Discussion
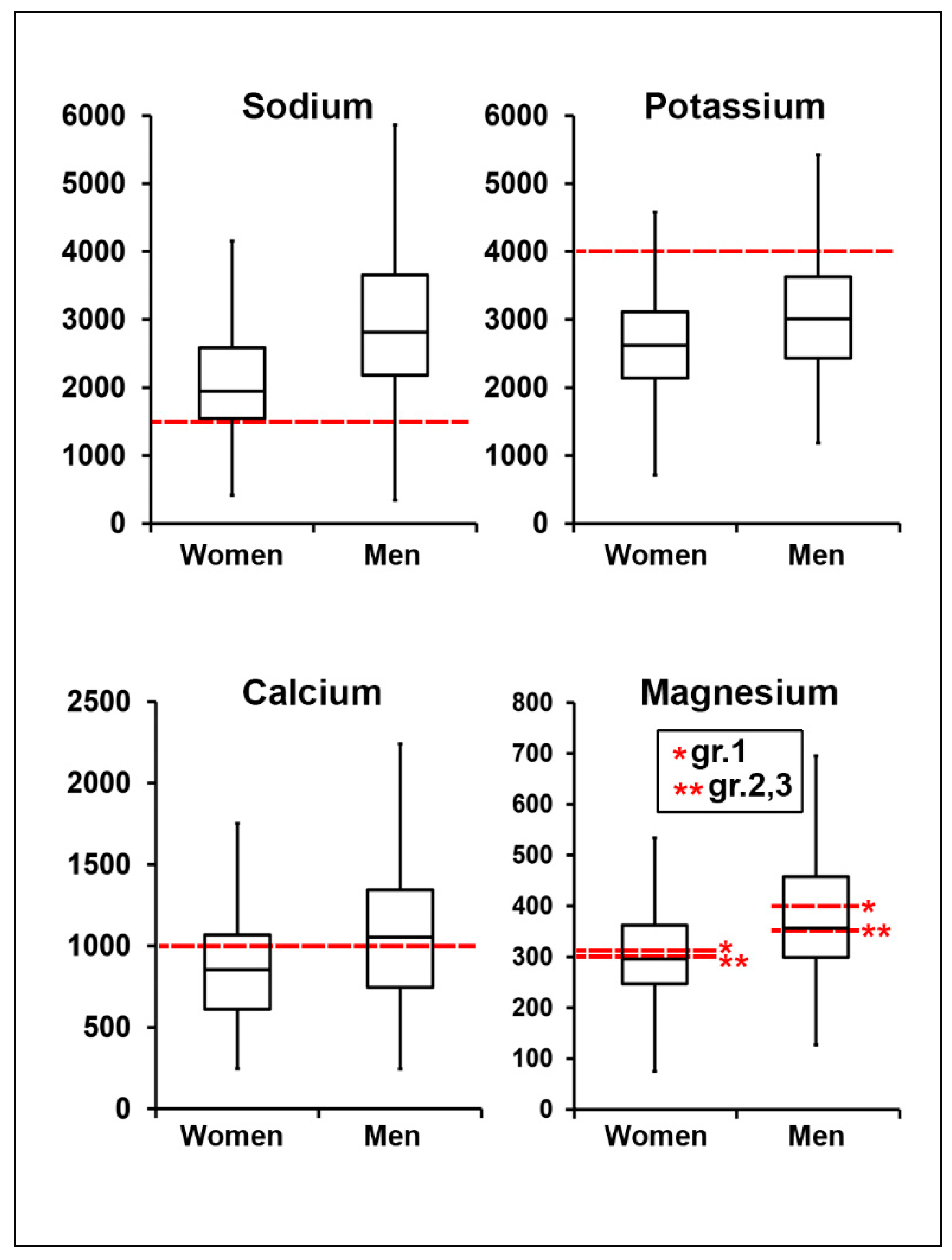
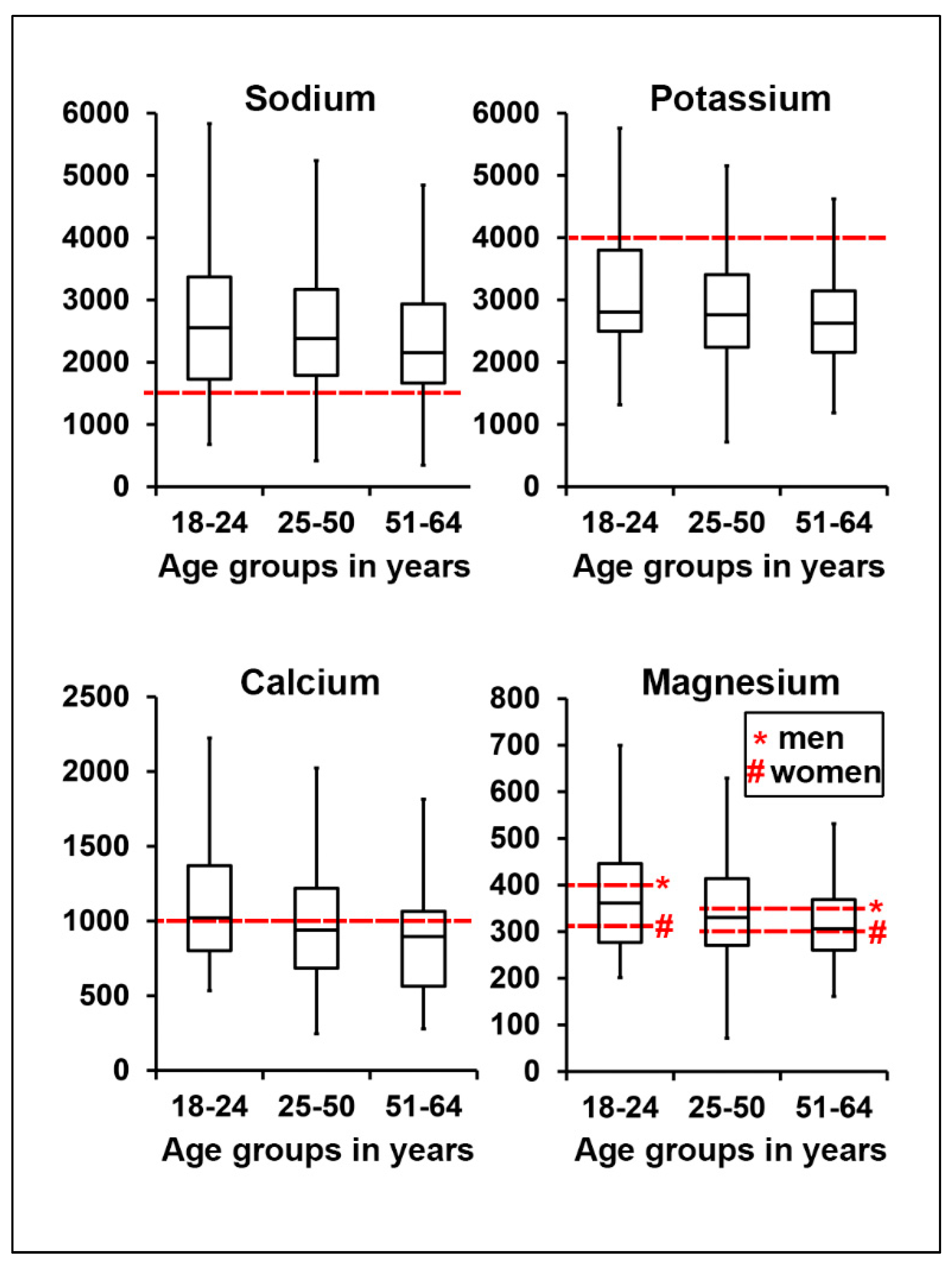
The present study is the first combined analysis of dietary sodium, potassium, calcium and magnesium intake in Austria. We compared nutritional intake of these four electrolytes in different gender/age groups, and described the main food sources of electrolytes according to regional dietary patterns.
It was previously shown that western dietary practices with a higher consumption of cereals and low-nutrient-density processed foods, and a lower consumption of fruits and vegetables, led to a diet high in sodium and low in potassium [
38,
39,
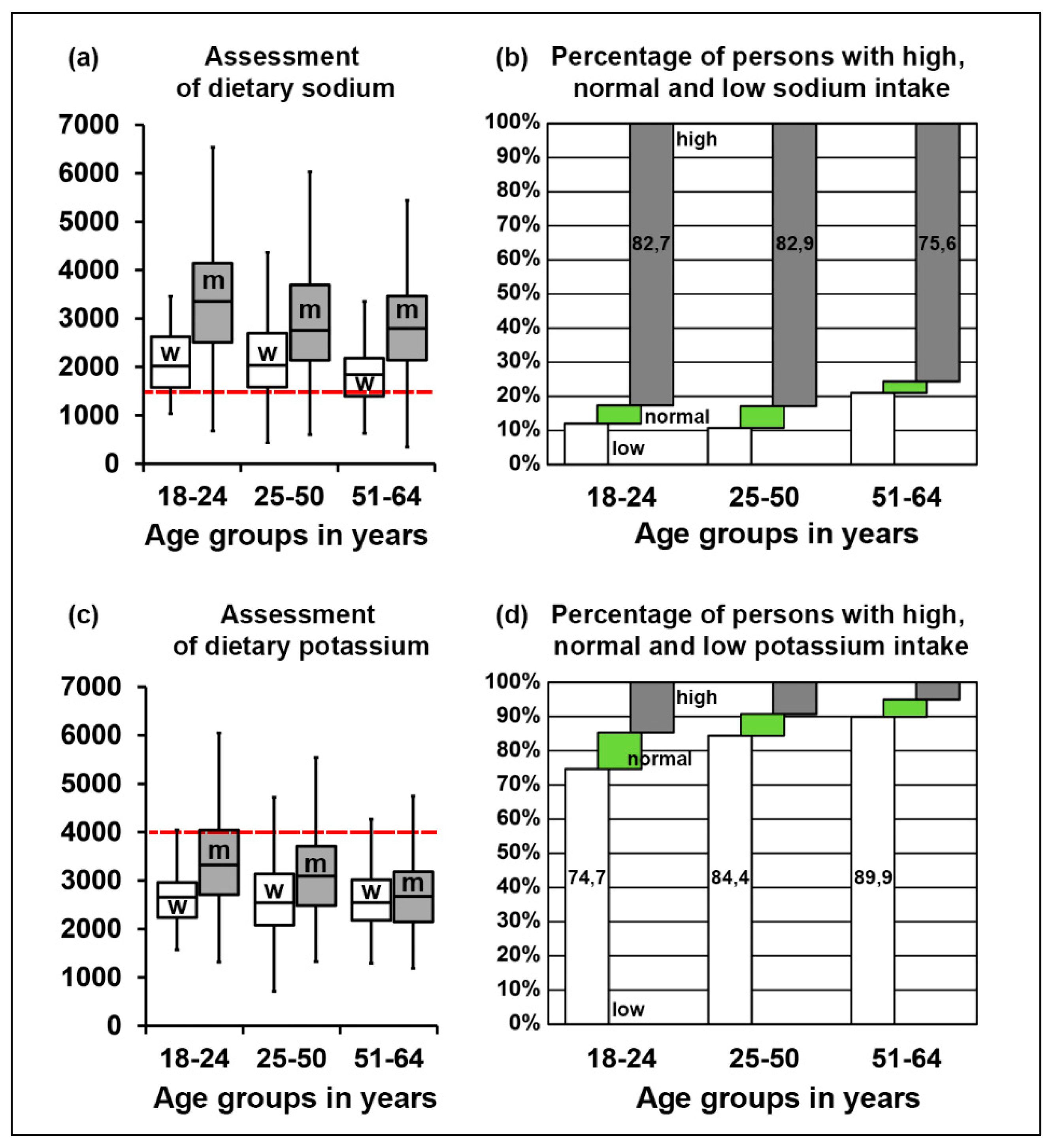
40]. Additionally, 99.4% of US adults were reported to consume excessive sodium, whereas less than 2% attained the recommended values for potassium [
39]. Additionally, meat products (including processed meats such as ham, bacon, etc.) contribute to a high proportion of salt intake worldwide [
41]. The reported potassium intakes below estimated average requirement (EAR) were 11–63% for women and 3–37% for men, and were highest in Spain, France, Poland and the UK, and lowest in The Netherlands [
42]. Deficits in magnesium intake in the adult population (18–60 years) were also previously reported in France (32% below EAR) and the UK (36% below EAR).
Our results confirm and extend previous studies in Austria, Germany, the UK and the US, where 50% or more of the participants did not reach the recommendations [
34,
36,
42,
43,
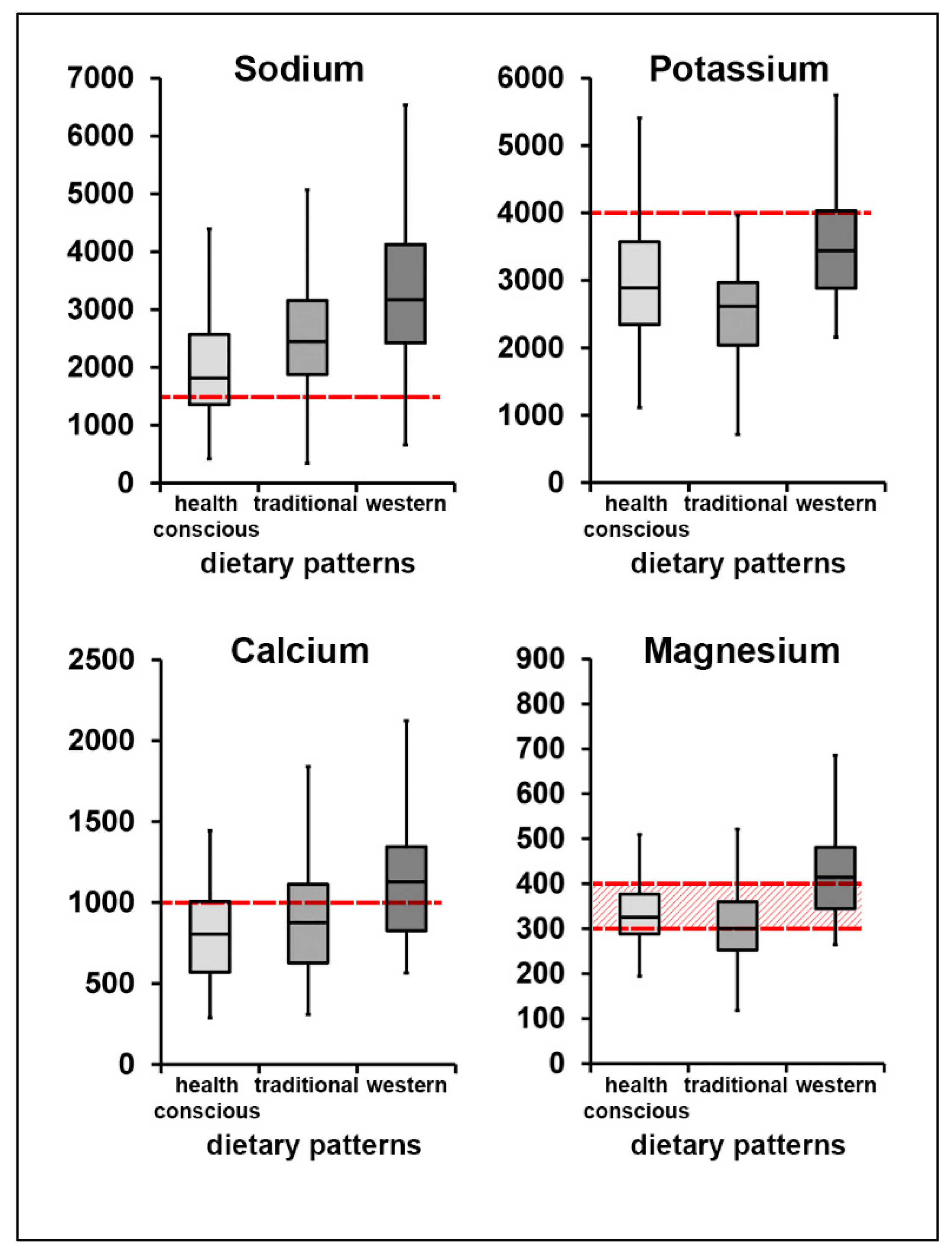
44]. In all three dietary patterns previously defined in Tyrol, the mean value of sodium intake was higher than the suggested consumption, which is also in line with our previous studies showing high consumption of salt in all regions of Austria [
44,
45]. Analyses of potassium, calcium and magnesium intake showed that the majority of our study population did not reach the normal intake range. When combining electrolyte intake values, only 1% of our study population reached D-A-CH recommended levels [
2], while 13% consumed adequate levels of three electrolytes. Analyses of food groups showed that these individuals preferred water/mineral water over sodas/energy drinks, consumed high amounts of fruits/vegetables/legumes and milk/cheese products, preferred vegetable oils over butter and at less sweets/cakes. Due to the low number of persons, we could not reliably correlate adequate electrolyte intake with previously defined dietary patterns, but our data may help to correct existing patterns by focusing on defined food groups.
Our data may extend the discussion about the practical applicability of reference values for individual electrolytes. Thus, the optimum calcium intake remains uncertain. According to the Austrian dietary guidelines [
46], three servings (about 500 g/day) of milk and dairy products (e.g., 1 glass of milk, 1 cup of yogurt, one piece of cheese) are recommended with a focus on covering calcium requirements. Guidelines from other geographic regions reduced their reference values for ecological reasons and taking into account plant-based calcium sources such as green vegetables, nuts and seeds, mineral water rich in calcium or milk alternatives [
47]. Although milk and dairy products often come under criticism by the media and the public, the current scientific literature suggests that the consumption of an appropriate amount of milk and dairy products may be beneficial at all ages, with the exception of individuals with specific medical conditions such as lactose intolerance or milk protein allergy [
48]. A recent review by Thorning et al. [
49] summarized data on the benefits of milk products, suggesting a protective effect against type 2 diabetes and CVD, and a positive effect on bone mineral density with very few adverse effects. At the same time, studies from Asian regions report calcium intakes of less than 500 mg/day [
50], and suggested that low intake of calcium is not associated with a higher risk of bone fractures, diabetes mellitus type 2, CVD [
51,
52] and hypertension [
35]. A recent publication by Willet et al. [
53] reviewed global healthy diets and suggested that among adults, the risk of fractures is not substantially reduced with calcium intakes greater than 500 mg/day. A clear association in this matter is difficult to assess, since other factors (e.g., genetics, calcium absorption, intolerances, etc.) have to be taken into account [
54]. However, higher intake of calcium or milk was not associated with CVD and other diseases [
17], which makes it even more difficult to establish connections between calcium intake and the aforementioned health issues. With this research background, our study population seems to be at low risk of calcium deficiency, despite their relatively low intake of milk and dairy products.
Evidence-based potassium recommendations have also been widely discussed in the literature. Current recommendations differ between China, the US and Europe, and are suggested to be considerably higher than current average intakes [
55]. The D-A-CH reference value for potassium was recently changed from 2000 mg/day to 4000 mg/day, which makes it more difficult to achieve [
2]. Thus, the large gap between recommended intake and the actual consumption of potassium, as we and other researchers have observed, has to be further evaluated, especially in the context of the whole diet including energy values and other minerals.
Inadequate magnesium status was previously observed in populations which consume processed-foods [
43]. Our data show that the magnesium intake mean value does not differ significantly from recommended intake levels. Still, 40% of our study population did not consume enough magnesium. Most of this mineral in our study came from bread, grains and potatoes (24.4%), fruits, vegetables, pulses, nuts and seeds (18.7%) and nonalcoholic drinks (18.4%). Interestingly, the average intake of whole grains, fruits, vegetables, legumes, nuts and seeds was still significantly lower than the nutritional guidelines suggest. According to the Austrian dietary guidelines [
31], three portions of vegetables (375–600 g/day) and two portions of fruits (250–300 g/day) should be consumed daily. In our study population, women only reached 36.9% (1.1 portions) of the recommended vegetable and 61.0% (1.22 portions) of the recommended fruit intake, while men reached 37.3% (1.1 portions) of the recommended vegetable and 43.9% (0.9 portions) of the recommended fruit intake (17). Although magnesium mean value intake in our study population was mostly within the recommended ranges, there was a clear need to optimize overall electrolyte intake by incorporating more fruits and (green) vegetables, legumes such as (soy) beans, peas, lenses and chick peas as well as whole grains such as whole grain bread, oats, or whole grain pasta. In addition, nuts and seeds such as pumpkin, sesame and sunflower seeds, as well as nuts, contribute to an adequate electrolyte intake. Taking into account that most participants follow a traditional dietary pattern, which does not include most of these products, diet optimization is challenging.
The results of our analysis allow several applicable conclusions to be made concerning the local population. Persons following traditional dietary patterns consume enough calcium and magnesium, but also eat too much salt and significantly less potassium, compared to the other dietary patterns in our study. It is therefore recommended that the consumption of plant-based foods that are widely accepted in Tyrolean cuisine be increased, e.g., white and red cabbage, potatoes, sauerkraut (pickled cabbage), seasonal local fruits and vegetables including spinach, leeks, radish, asparagus, broccoli, root vegetables, pears and apples. Persons in the group of the health-conscious dietary pattern had better sodium and potassium intakes, but did not reach the recommended calcium levels. Individuals following this dietary pattern often consume foods that are plant-based [
30]; thus, if it is not possible to increase calcium intake by consuming more dairy products, alternative products, such as fortified, plant-based milk, should be included.
Strengths and Limitations: The use of two nonconsecutive 24-h recalls is one of this study’s strengths, since we could consider seasonal differences and achieve the requirements of standardized conditions, as recommended by the EFSA [
17]. However, the results were limited by the cross-sectional design of the study, which only allowed judgements to be made regarding possible associations but not of casual relations. Also, we could only recruit participants from the central area of Tyrol, and therefore, the results are only representative of that area. Further limitations regarding our study design are described elsewhere [
14]. With lower response rates in men than in women, nonresponse bias is likely, and it was necessary to additionally recruit participants from regional companies to complete the missing gender and age groups. Therefore, these persons were not part of the original random sample. Furthermore, although known confounders were considered, residual confounding remains a possibility. In this study, the “migration background” of the person was considered when at least one of the parents was not born in Austria (23.5% of participants). We did not observe any significant differences in BMI or health parameters in this group of participants [
56].
Furthermore, dietary surveys are often not considered optimal for estimating a population’s electrolyte intake, due to the variability of electrolyte content in the food and the use of 24-h recalls. Additionally, no blood and urine samples were taken, and thus, actual electrolyte status could not be assessed.

 ,
, 





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}