Binge Drinking and Risk of Breast Cancer: Results from the SUN (‘Seguimiento Universidad de Navarra’) Project

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
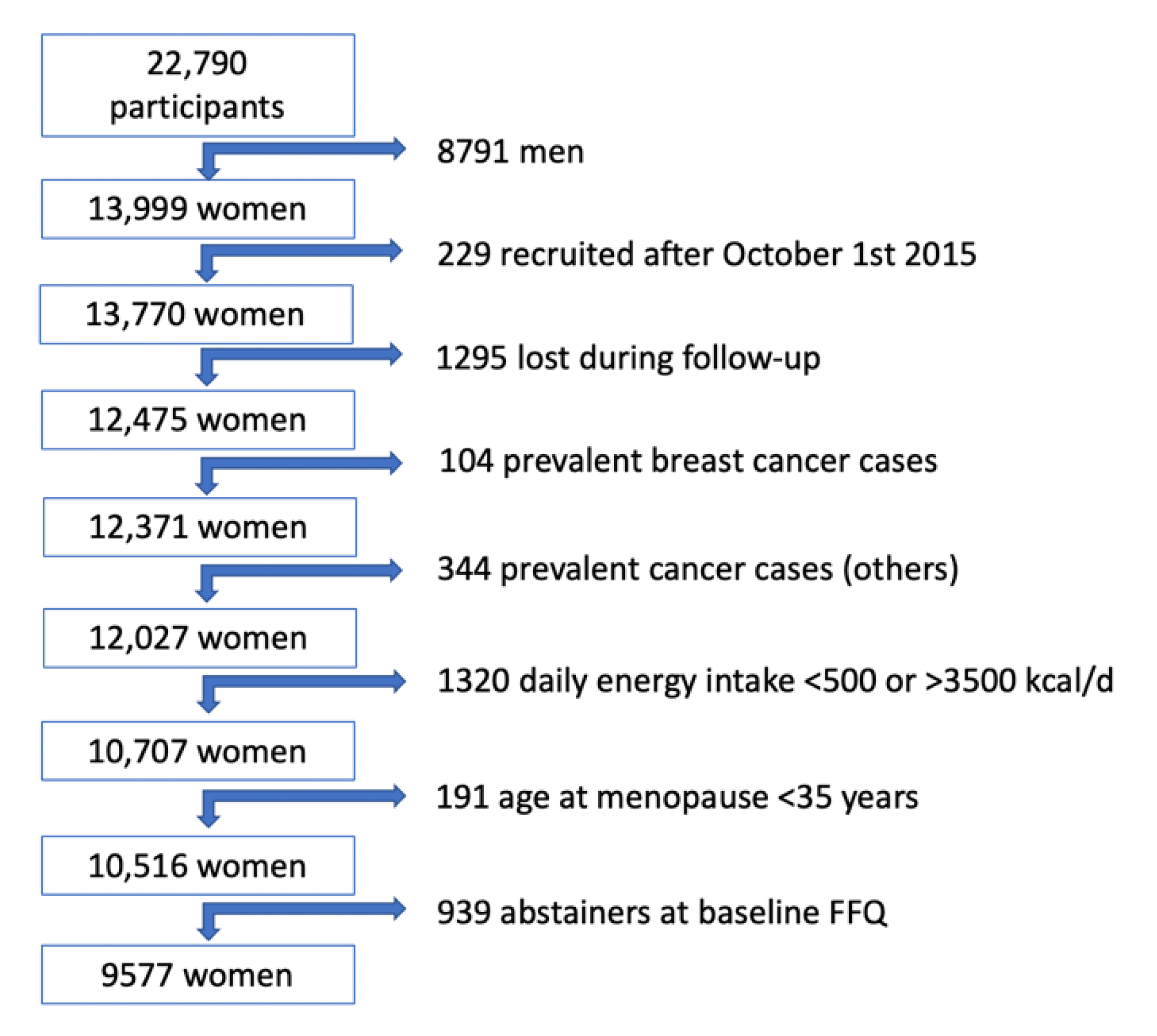
2.1. Study Population
2.2. Assessment of Alcohol Consumption
2.3. Breast Cancer Assessment
2.4. Covariate Assessment
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Kanny, D.; Naimi, T.S.; Liu, Y.; Brewer, R.D. Trends in Total Binge Drinks per Adult Who Reported Binge Drinking—United States, 2011–2017. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 30–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eaton, D.K.; Kann, L.; Kinchen, S.A.; Shanklin, S.; Flint, K.H.; Hawkins, J.; Harris, W.A.; Lowry, R.; McManus, T.; Chyen, D.; et al. Youth Risk Behavior Surveillance—United States, 2011. CDC Morb. Mortal. Surveil. Summ. 2012, 61, 1–162. [Google Scholar]
- National Institute on Alcohol Abuse and Alcoholism (NIAAA). Alcohol’s Effects on Health. United States: NIH. Available online: https://www.niaaa.nih.gov/alcohol-health/overview-alcohol-consumption/moderate-binge-drinking (accessed on 4 March 2020).
- World Health Organization. Global Health Observatory (GHO) Data. Heavy Episodic Drinking among Drinkers; WHO: Geneva, Switzerland, 2020; Available online: http://www.who.int/gho/alcohol/consumption_patterns/heavy_episodic_drinkers_text/en/ (accessed on 4 March 2020).
- Heath, D.B. Cultural variations among drinking patterns. In Drinking Patterns and their Consequences; Grant, M., Litvak, J., Eds.; Taylor & Francis: Washington, DC, USA, 1997; pp. 103–128. [Google Scholar]
- Gea, A.; Bes-Rastrollo, M.; Toledo, E.; Garcia-Lopez, M.; Beunza, J.J.; Estruch, R.; Martinez-Gonzalez, M.A. Mediterranean alcohol-drinking pattern and mortality in the SUN (Seguimiento Universidad de Navarra) Project: A prospective cohort study. Br. J. Nutr. 2014, 111, 1871–1880. [Google Scholar] [CrossRef] [Green Version]
- International Agency for Research on Cancer. Alcohol Consumption and Ethyl Carbamate. In IARC Monographs on the Evaluation of Carcinogenic Risks to Humans; International Agency for Research on Cancer: Lyon, France, 2010; Volume 96. [Google Scholar]
- Room, R.; Babor, T.; Rehm, J. Alcohol and public health. Lancet 2005, 365, 519–530. [Google Scholar] [CrossRef]
- Chen, W.Y.; Rosner, B.; Hankinson, S.E.; Colditz, G.A.; Willett, W.C. Moderate alcohol consumption during adult life, drinking patterns, and breast cancer risk. JAMA 2011, 306, 1884–1890. [Google Scholar] [CrossRef] [Green Version]
- Sun, Q.; Xie, W.; Wang, Y.; Chong, F.; Song, M.; Li, T.; Xu, L.; Song, C. Alcohol consumption by beverage type and risk of breast cancer: A dose-response meta-analysis of prospective cohort studies. Alcohol Alcohol. 2020. [Google Scholar] [CrossRef]
- Mørch, L.S.; Johansen, D.; Thygesen, L.C.; Tjønneland, A.; Løkkegaard, E.; Stahlberg, C.; Grønbaek, M. Alcohol drinking, consumption patterns and breast cancer among Danish nurses: A cohort study. Eur. J. Public Health 2007, 17, 624–629. [Google Scholar] [CrossRef]
- White, A.J.; DeRoo, L.A.; Weinberg, C.R.; Sandler, D.P. Lifetime Alcohol Intake, Binge Drinking Behaviors, and Breast Cancer Risk. Am. J. Epidemiol. 2017, 186, 541–549. [Google Scholar] [CrossRef]
- Lindtner, C.; Scherer, T.; Zielinski, E.; Filatova, N.; Fasshauer, M.; Tonks, N.K.; Puchowicz, M.; Buettner, C. Binge drinking induces whole-body insulin resistance by impairing hypothalamic insulin action. Sci. Transl. Med. 2013, 5, 170ra14. [Google Scholar] [CrossRef] [Green Version]
- De Pergola, G.; Silvestris, F. Obesity as a major risk factor for cancer. J. Obes. 2013, 2013, 291546. [Google Scholar] [CrossRef] [Green Version]
- Carlos, S.; De La Fuente-Arrillaga, C.; Bes-Rastrollo, M.; Razquin, C.; Rico-Campà, A.; Martínez-González, M.A.; Ruiz-Canela, M. Mediterranean Diet and Health Outcomes in the SUN Cohort. Nutrients 2018, 10, 439. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Willett, W.C. Nutritional Epidemiology, 3rd ed.; Oxford University Press: New York, NY, USA, 2013. [Google Scholar]
- Martinez-Gonzalez, M.A.; Lopez-Fontana, C.; Varo, J.J.; Sánchez-Villegas, A.; Martinez, J.A. Validation of the Spanish version of the physical activity questionnaire used in the Nurses’ Health Study and the Health Professionals’ Follow-up Study. Public Health Nutr. 2005, 8, 920–927. [Google Scholar] [CrossRef] [PubMed]
- Trichopoulou, A.; Costacou, T.; Bamia, C.; Trichopoulos, D. Adherence to a Mediterranean diet and survival in a Greek population. N. Engl. J. Med. 2003, 348, 2599–2608. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shivappa, N.; Sandin, S.; Löf, M.; Hébert, J.R.; Adami, H.O.; Weiderpass, E. Prospective study of dietary inflammatory index and risk of breast cancer in Swedish women. Br. J. Cancer 2015, 113, 1099–1103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Romanos-Nanclares, A.; Toledo, E.; Gardeazabal, I.; Jimenez-Moleón, J.J.; Martinez-González, M.A.; Gea, A. Sugar-sweetened beverage consumption and incidence of breast cancer: The Seguimiento Universidad de Navarra (SUN) Project. Eur. J. Nutr. 2019, 58, 2875–2886. [Google Scholar] [CrossRef] [PubMed]
- Chan, D.S.M.; Abar, L.; Cariolou, M.; Nanu, N.; Greenwood, D.C.; Bandera, E.V.; McTiernan, A.; Norat, T. World Cancer Research Fund International: Continuous Update Project—Systematic literature review and meta-analysis of observational cohort studies on physical activity, sedentary behavior, adiposity, and weight change and breast cancer risk. Cancer Causes Control 2019, 30, 1183–1200. [Google Scholar] [CrossRef] [Green Version]
- Smith-Warner, S.A.; Spiegelman, D.; Yaun, S.S.; van den Brandt, P.A.; Folsom, A.R.; Goldbohm, R.A.; Graham, S.; Holmberg, L.; Howe, G.R.; Marshall, J.R.; et al. Alcohol and Breast Cancer in Women. A Pooled Analysis of Cohort Studies. JAMA 1998, 279, 535–540. [Google Scholar] [CrossRef] [Green Version]
- Petri, A.L.; Tjonneland, A.; Gamborg, M.; Johansen, D.; Høidrup, S.; Sørensen, T.I.; Grønbaek, M. Alcohol Intake, Type of Beverage, and Risk of Breast Cancer in Pre- and Postmenopausal Women. Alcohol. Clin. Exp. Res. 2004, 7, 1084–1090. [Google Scholar] [CrossRef]
- Lew, J.Q.; Freedman, N.D.; Leitzmann, M.F.; Brinton, L.A.; Hoover, R.N.; Hollenbeck, A.R.; Schatzkin, A.; Park, Y. Alcohol and Risk of Breast Cancer by Histologic Type and Hormone Receptor Status in Postmenopausal Women. The NIH-AARP Diet and Health Study. Am. J. Epidemiol. 2009, 170, 308–317. [Google Scholar] [CrossRef] [Green Version]
- Li, C.I.; Chlebowski, R.T.; Freiberg, M.; Johnson, K.C.; Kuller, L.; Lane, D.; Lessin, L.; O’Sullivan, M.J.; Wactawski-Wende, J.; Yasmeen, S.; et al. Alcohol Consumption and Risk of Postmenopausal Breast Cancer by Subtype: The Women’s Health Initiative Observational Study. J. Natl. Cancer Inst. 2010, 102, 1422–1431. [Google Scholar] [CrossRef] [Green Version]
- Romieu, I.; Scoccianti, C.; Chajès, V.; de Batlle, J.; Biessy, C.; Dossus, L.; Baglietto, L.; Clavel-Chapelon, F.; Overvad, K.; Olsen, A.; et al. Alcohol Intake and Breast Cancer in the European Prospective Investigation into Cancer and Nutrition. Int. J. Cancer 2015, 137, 1921–1930. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scoccianti, C.; Lauby-Secretan, B.; Bello, P.Y.; Chajes, V.; Romieu, I. Female breast cancer and alcohol consumption: A review of the literature. Am. J. Prev. Med. 2014, 46 (Suppl. 1), S16–S25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Toledo, E.; Salas-Salvadó, J.; Donat-Vargas, C.; Buil-Cosiales, P.; Estruch, R.; Ros, E.; Corella, D.; Fitó, M.; Hu, F.B.; Arós, F.; et al. Mediterranean Diet and invasive breast cancer among women at high cardiovascular risk in the PREDIMED Trial: A Randomized Clinical Trial. JAMA Intern. Med. 2015, 175, 1752–1760. [Google Scholar] [CrossRef] [PubMed]
- Rohan, T.E.; Cook, M.G. Alcohol consumption and risk of benign proliferative epithelial disorders of the breast in women. Int. J. Cancer 1989, 43, 631–636. [Google Scholar] [CrossRef]
- Friedenreich, C.; Bryant, H.; Alexander, F.; Hugh, J.; Danyluk, J.; Page, D. Risk factors for benign proliferative breast disease. Int. J. Epidemiol. 2000, 29, 637–644. [Google Scholar] [CrossRef]
- Longnecker, M.P.; Newcomb, P.A.; Mittendorf, R.; Greenberg, E.R.; Clapp, R.W.; Bogdan, G.F.; Baron, J.; MacMahon, B.; Willett, W.C. Risk of breast cancer in relation to lifetime alcohol consumption. J. Natl. Cancer Inst. 1995, 87, 923–929. [Google Scholar] [CrossRef]
- Fan, S.; Meng, Q.; Gao, B.; Grossman, J.; Yadegari, M.; Goldberg, I.D.; Rosen, E.M. Alcohol stimulates estrogen receptor signaling in human breast cancer cell lines. Cancer Res. 2000, 60, 5635–5639. [Google Scholar]
- Baglia, M.L.; Cook, L.S.; Mei-Tzu, C.; Wiggins, C.; Hill, D.; Porter, P.; Li, C.I. Alcohol, smoking, and risk of Her2-overexpressing and triple-negative breast cancer relative to estrogen receptor-positive breast cancer. Int. J. Cancer 2018, 143, 1849–1857. [Google Scholar] [CrossRef] [Green Version]
- Ellingjord-Dale, M.; Vos, L.; Hjerkind, K.V.; Hjartaker, A.; Russnes, H.G.; Tretli, S.; Hofvind, S.; Dos-Santos-Silva, I.; Ursin, G. Alcohol, Physical Activity, Smoking, and Breast Cancer Subtypes in a Large, Nested Case-Control Study from the Norwegian Breast Cancer Screening Program. Cancer Epidemiol. Biomark. Prev. 2017, 26, 1736–1744. [Google Scholar] [CrossRef] [Green Version]
- Seitz, H.K.; Maurer, B. The relationship between alcohol metabolism, estrogen levels, and breast cancer risk. Alcohol Res. Health 2007, 30, 42–43. [Google Scholar]
- Lorenti Garcia, C.; Mechilli, M.; Proietti De Santis, L.; Schinoppi, A.; Kobos, K.; Palitti, F. Relationship between DNA lesions, DNA repair and chromosomal damage induced by acetaldehyde. Mutat. Res. 2009, 662, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Fan, A.Z.; Russell, M.; Naimi, T.; Li, Y.; Liao, Y.; Jiles, R.; Mokdad, A.H. Patterns of alcohol consumption and the metabolic syndrome. J. Clin. Endocrinol. Metab. 2008, 93, 3833–3838. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galceran, J.; Ameijide, A.; Carulla, M.; Mateos, A.; Quirós, J.R.; Rojas, D.; Alemán, A.; Torrella, A.; Chico, M.; Vicente, M.; et al. Cancer incidence in Spain, 2015. Clin. Transl. Oncol. 2017, 19, 799–825. [Google Scholar] [CrossRef] [PubMed]
- Shaper, A.G.; Wannamethee, G.; Walker, M. Alcohol and mortality in British men: Explaining the U-shaped curve. Lancet 1988, 2, 1267–1273. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | No Binge Drinking | Binge Drinking |
|---|---|---|
| n (%) * | 7285 (76.1) | 2292 (23.9) |
| Age (years) | 36 (10.6) | 29.8 (7.8) |
| Body-mass index (kg/m2) | 22.3 (3.0) | 22 (2.9) |
| Height (cm) | 163 (6) | 165 (5.9) |
| Physical activity (MET-h/week) | 20 (18.5) | 20.9 (19.7) |
| Total energy intake (kcal/day) | 2303 (574) | 2304 (563) |
| Alcohol intake (g/day) | 6.5 (10.7) | 9.7 (12.7) |
| Sugar-sweetened beverages (servings/day) | 0.16 (0.33) | 0.22 (0.32) |
| Lifetime breast-feeding (months) | 3.1 (5.5) | 1.2 (3.2) |
| Adherence to Mediterranean diet score | 4.1 (1.7) | 4.1 (1.7) |
| Time of university education (years) | 4.8 (1.4) | 4.7 (1.2) |
| Age of menarche (%) | ||
| <10 years | 20.3 | 19.4 |
| 10–16 years | 71.7 | 72.5 |
| >16 years | 8 | 8.1 |
| Menopause (%) | 12.8 | 2.9 |
| Obstetric history (including age at first pregnancy) (%) | ||
| Age < 25 years & nulliparous | 15.2 | 28.2 |
| Age ≥ 25 years & nulliparous | 47.5 | 53.8 |
| First pregnancy before 25 years | 5.3 | 1.6 |
| First pregnancy between 25 & 30 years of age | 16.7 | 7 |
| First pregnancy being 30 years old or older | 15.3 | 9.4 |
| Time of hormone-replacement therapy (months) | 1.2 (2.3) | 1.6 (2.4) |
| Smoking (%) | ||
| Never | 55.5 | 37.5 |
| Current | 23 | 43.5 |
| Former | 21.5 | 19 |
| Lifetime tobacco exposure (pack-years) | 4 (7.7) | 4.7 (7.2) |
| Family history of Breast Cancer (%) | ||
| None | 89.2 | 90.2 |
| Before the age of 45 years | 8.8 | 8.2 |
| After the age of 45 years | 2 | 1.6 |
| Confirmed Breast Cancer Cases | No Binge Drinking | Binge Drinking |
|---|---|---|
| Overall | ||
| Cases/women-years | 67/80,452 | 21/24,479 |
| Age adjusted | 1 (Ref.) | 1.82 (1.09–3.03) |
| Multivar. adjusted * | 1 (Ref.) | 1.76 (1.03–2.99) |
| Premenopausal | ||
| Cases/women-years | 33/61,155 | 18/22,796 |
| Age adjusted | 1 (Ref.) | 2.29 (1.27–4.13) |
| Multivar. adjusted * | 1 (Ref.) | 2.06 (1.11–3.82) |
| Postmenopausal | ||
| Cases/women-years | 28/16,405 | 2/1377 |
| Age adjusted | 1 (Ref.) | 0.84 (0.20–3.53) |
| Multivar. adjusted * | 1 (Ref.) | 1.13 (0.26–4.95) |
| Probable Breast Cancer Cases | No Binge Drinking | Binge Drinking |
|---|---|---|
| Overall | ||
| Cases/women-years | 135/80,452 | 32/24,479 |
| Age adjusted | 1 (Ref.) | 1.29 (0.87–1.94) |
| Multivar. adjusted * | 1 (Ref.) | 1.22 (0.81–1.85) |
| Premenopausal | ||
| Cases/women-years | 72/61,155 | 26/22,796 |
| Age adjusted | 1 (Ref.) | 1.45 (0.92–2.30) |
| Multivar. adjusted * | 1 (Ref.) | 1.28 (0.79–2.06) |
| Postmenopausal | ||
| Cases/women-years | 52/16,405 | 5/1377 |
| Age adjusted | 1 (Ref.) | 1.10 (0.44–2.79) |
| Multivar. adjusted * | 1 (Ref.) | 1.27 (0.49–3.30) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sánchez-Bayona, R.; Gea, A.; Gardeazabal, I.; Romanos-Nanclares, A.; Martínez-González, M.Á.; Bes-Rastrollo, M.; Santisteban, M.; Toledo, E. Binge Drinking and Risk of Breast Cancer: Results from the SUN (‘Seguimiento Universidad de Navarra’) Project. Nutrients 2020, 12, 731. https://doi.org/10.3390/nu12030731
Sánchez-Bayona R, Gea A, Gardeazabal I, Romanos-Nanclares A, Martínez-González MÁ, Bes-Rastrollo M, Santisteban M, Toledo E. Binge Drinking and Risk of Breast Cancer: Results from the SUN (‘Seguimiento Universidad de Navarra’) Project. Nutrients. 2020; 12(3):731. https://doi.org/10.3390/nu12030731
Chicago/Turabian StyleSánchez-Bayona, Rodrigo, Alfredo Gea, Itziar Gardeazabal, Andrea Romanos-Nanclares, Miguel Ángel Martínez-González, Maira Bes-Rastrollo, Marta Santisteban, and Estefanía Toledo. 2020. "Binge Drinking and Risk of Breast Cancer: Results from the SUN (‘Seguimiento Universidad de Navarra’) Project" Nutrients 12, no. 3: 731. https://doi.org/10.3390/nu12030731