Determinants of Sweetness Preference: A Scoping Review of Human Studies

Abstract
:1. Introduction
2. Materials and Methods
2.1. Literature Search Strategy
2.1.1. Inclusion and Exclusion Criteria
2.1.2. Data Extraction, Study Assessment, and Synthesis of Results
2.2. Additional Analyses
3. Results
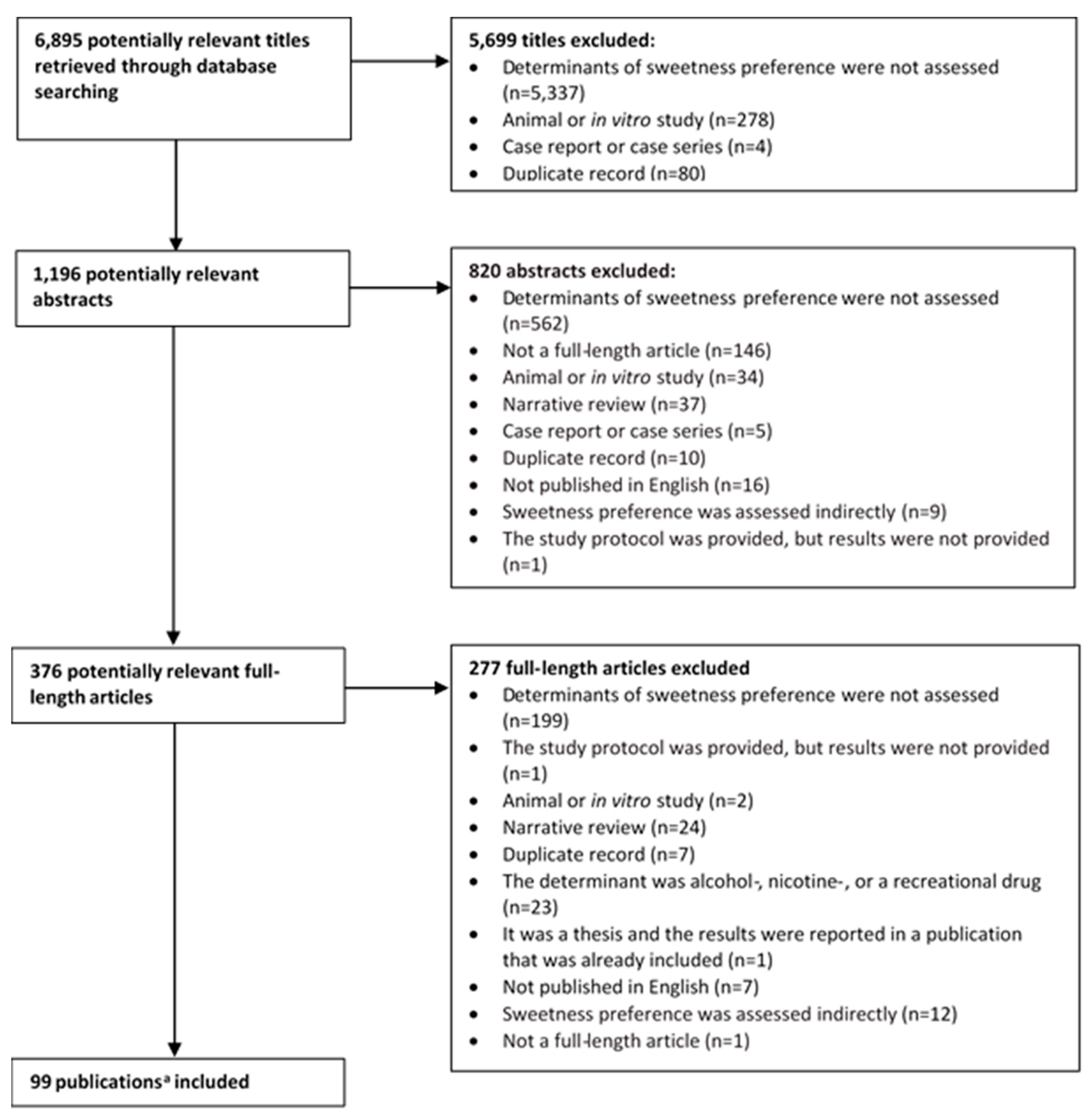
3.1. Literature Search Results
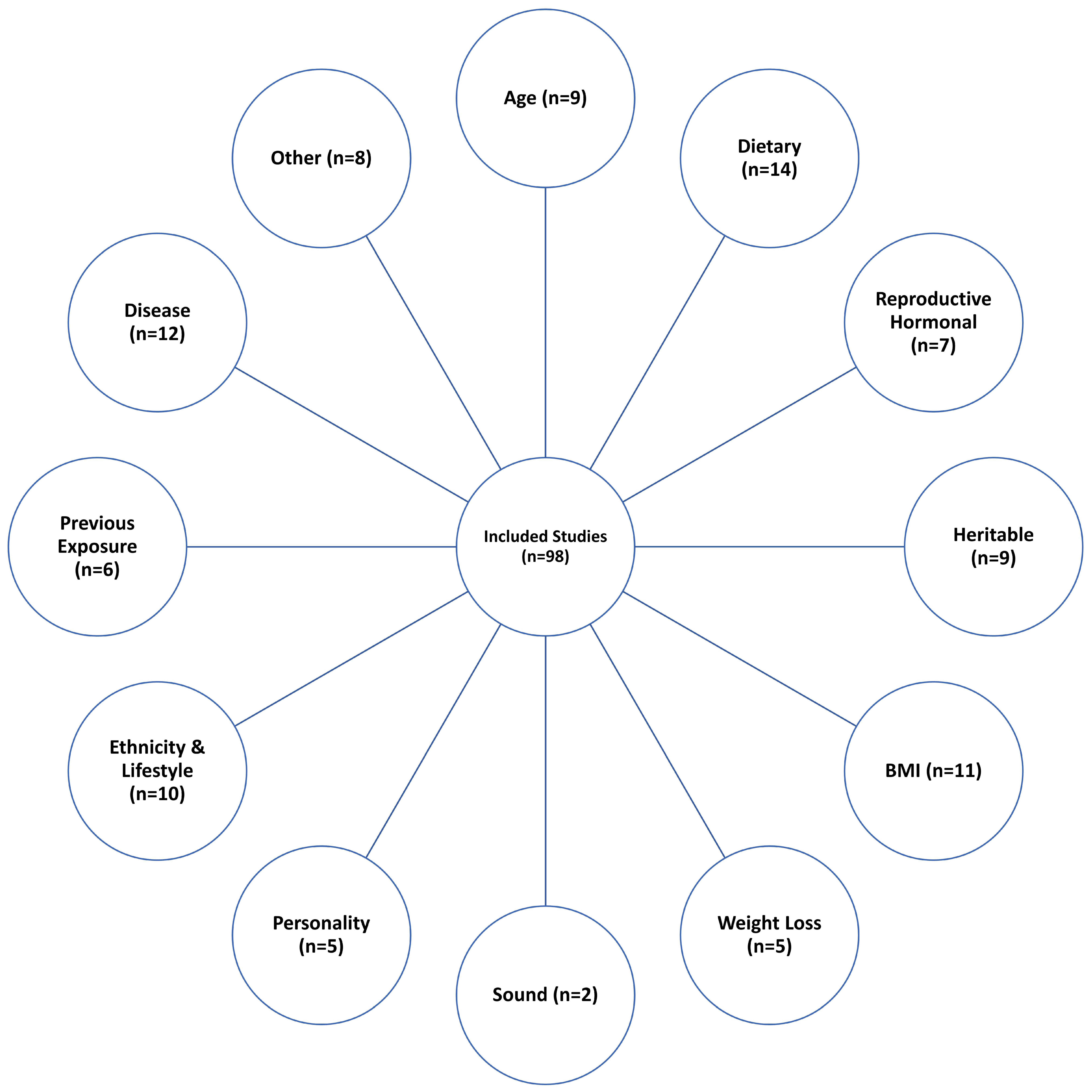
3.2. Categorization of Studies According to the Sweetness Preference Determinant Investigated
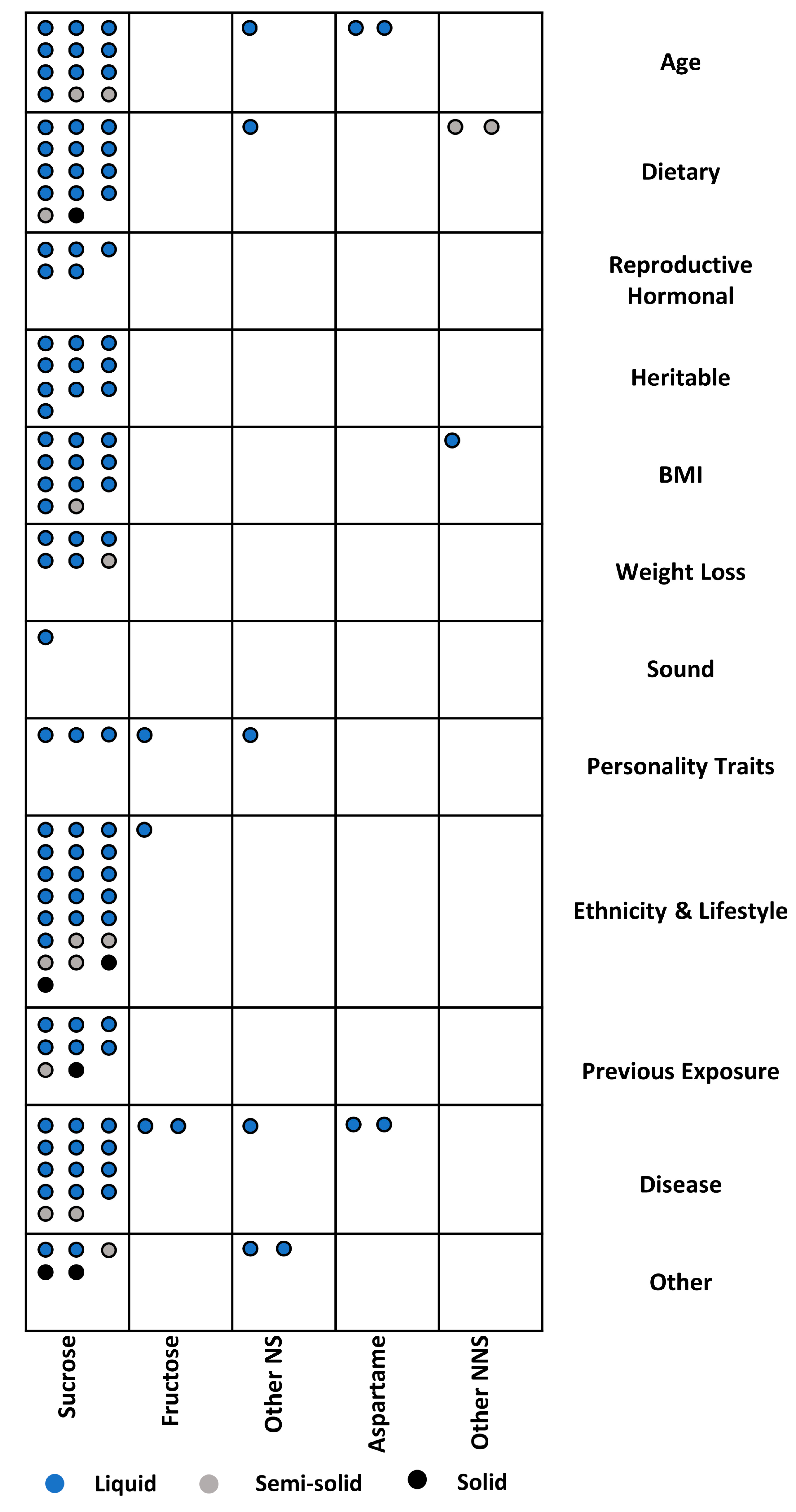
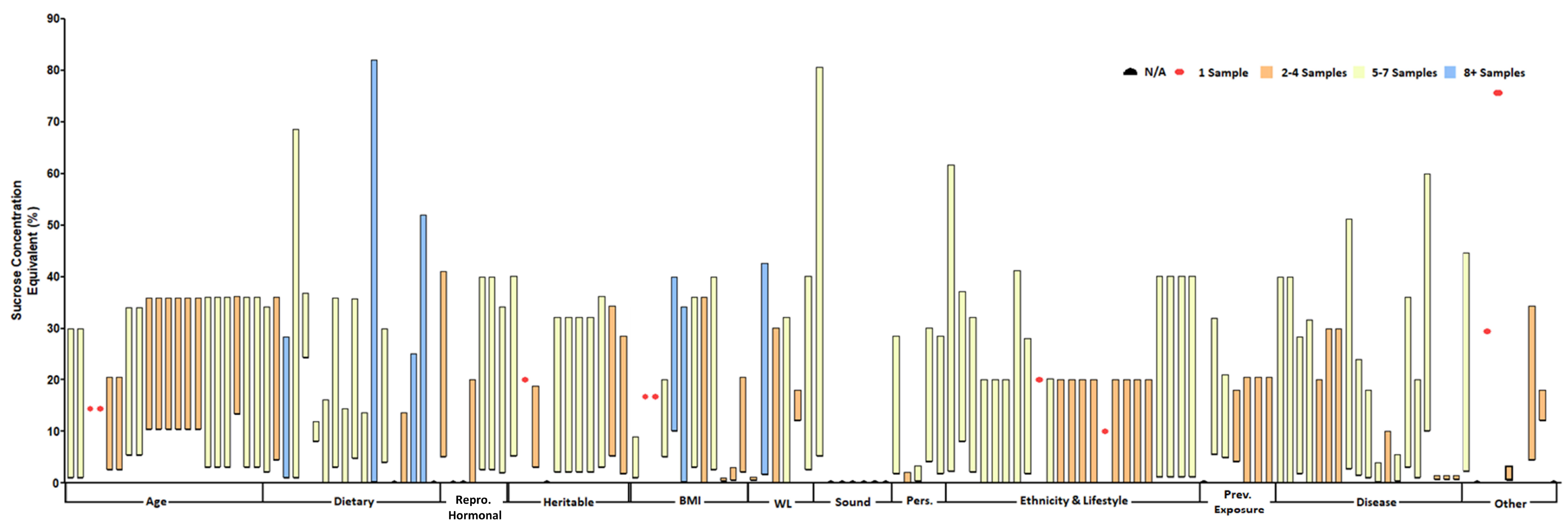
3.3. Key Study Characteristics
3.4. Study Results
3.4.1. Age and Sweetness Preference
3.4.2. Dietary/Nutritional Factors and Sweetness Preference
3.4.3. Reproductive Hormonal Factors and Sweetness Preference
3.4.4. Genetics and Sweetness Preference
3.4.5. Body Weight and Sweetness Preference
3.4.6. Weight Loss and Sweetness Preference
3.4.7. Sound and Sweetness Preference
3.4.8. Personality Traits and Sweetness Preference
3.4.9. Ethnicity and Lifestyle and Sweetness Preference
3.4.10. Previous Sweetness Exposure and Sweetness Preference
3.4.11. Disease and Sweetness Preference
Studies in Subjects with a Neurological or Psychological Disease
Studies in Individuals with T2DM or GDM
Studies in Patients with Other Diseases
3.4.12. Other Factors and Sweetness Preference
3.4.13. Summary of Findings
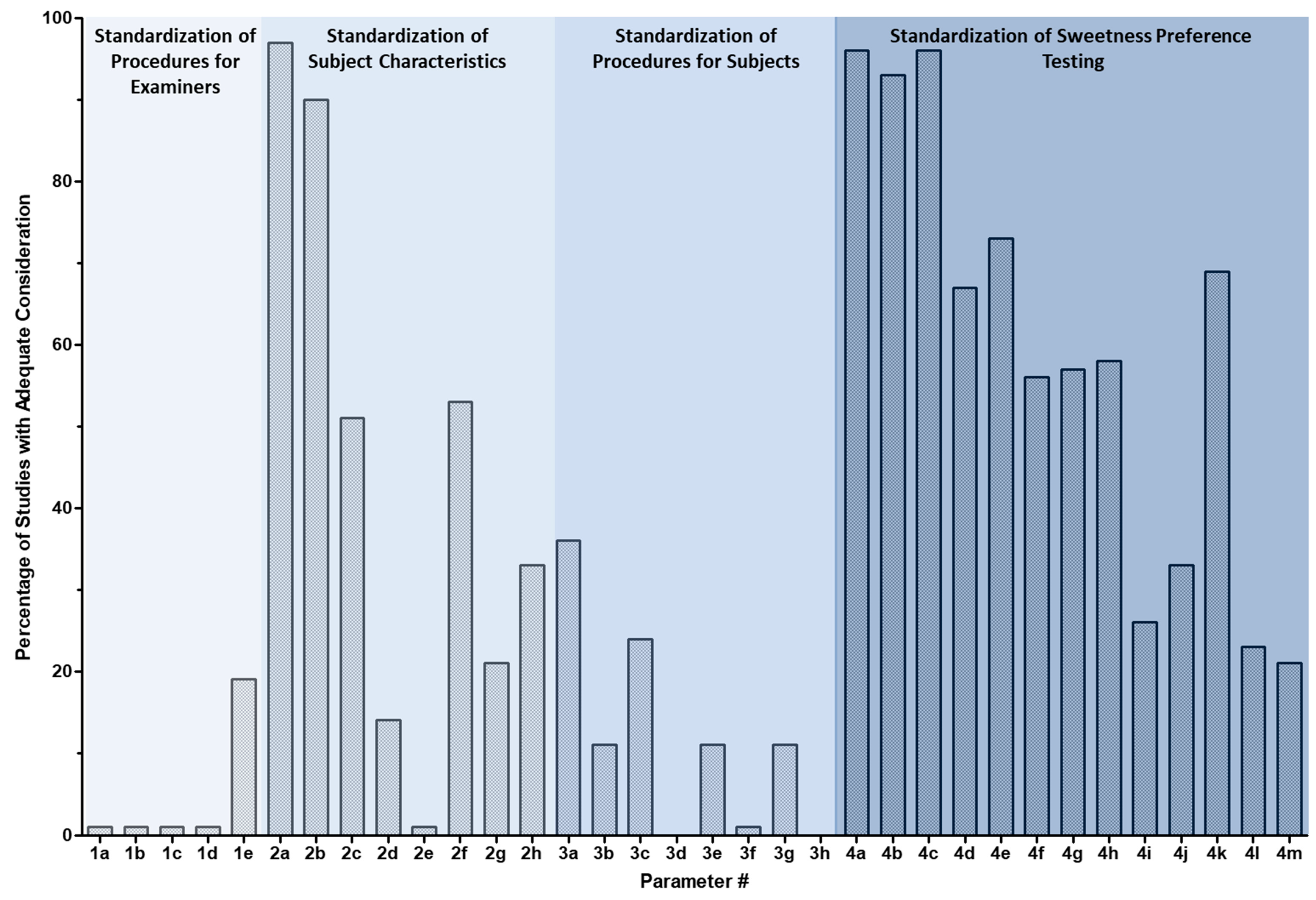
3.4.14. Findings related to the “investigator checklist”
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Ventura, A.K.; Mennella, J.A. Innate and learned preferences for sweet taste during childhood. Curr. Opin. Clin. Nutr. Metab. Care 2011, 14, 379–384. [Google Scholar] [CrossRef] [Green Version]
- Beauchamp, G.K. Why do we like sweet taste: A bitter tale? Physiol. Behav. 2016, 164, 432–437. [Google Scholar] [CrossRef] [Green Version]
- Shrayyef, M.Z.; Gerich, J.E. Normal glucose homeostasis. In Principles of Diabetes Mellitus; Poretsky, L., Ed.; Springer: Basel, Switzerland; New York, NY, USA, 2010; pp. 19–35. [Google Scholar]
- Lee, A.A.; Owyang, C. Sugars, sweet taste receptors, and brain responses. Nutrients 2017, 9, 653. [Google Scholar] [CrossRef] [Green Version]
- Bachmanov, A.A.; Beauchamp, G.K. Taste receptor genes. Annu. Rev. Nutr. 2007, 27, 389–414. [Google Scholar] [CrossRef] [Green Version]
- Margolskee, R.F.; Dyer, J.; Kokrashvili, Z.; Salmon, K.S.; Ilegems, E.; Daly, K.; Maillet, E.L.; Ninomiya, Y.; Mosinger, B.; Shirazi-Beechey, S.P. T1R3 and gustducin in gut sense sugars to regulate expression of Na+-glucose cotransporter 1. Proc. Natl. Acad. Sci. USA 2007, 104, 15075–15080. [Google Scholar] [CrossRef] [Green Version]
- Nelson, G.; Hoon, M.A.; Chandrashekar, J.; Zhang, Y.; Ryba, N.J.; Zuker, C.S. Mammalian sweet taste receptors. Cell 2001, 106, 381–390. [Google Scholar] [CrossRef] [Green Version]
- Zhao, G.Q.; Zhang, Y.; Hoon, M.A.; Chandrashekar, J.; Erlenbach, I.; Ryba, N.J.; Zuker, C.S. The receptors for mammalian sweet and umami taste. Cell 2003, 115, 255–266. [Google Scholar] [CrossRef] [Green Version]
- Fernstrom, J.D.; Munger, S.D.; Sclafani, A.; De Araujo, I.E.; Roberts, A.; Molinary, S. Mechanisms for sweetness. J. Nutr. 2012, 142, 1134S–1141S. [Google Scholar] [CrossRef]
- Hofer, D.; Asan, E.; Drenckhahn, D. Chemosensory perception in the gut. News Physiol. Sci. 1999, 14, 18–23. [Google Scholar] [CrossRef] [Green Version]
- Braun, T.; Voland, P.; Kunz, L.; Prinz, C.; Gratzl, M. Enterochromaffin cells of the human gut: Sensors for spices and odorants. Gastroenterology 2007, 132, 1890–1901. [Google Scholar] [CrossRef]
- Mace, O.J.; Lister, N.; Morgan, E.; Shepherd, E.; Affleck, J.; Helliwell, P.; Bronk, J.R.; Kellett, G.L.; Meredith, D.; Boyd, R.; et al. An energy supply network of nutrient absorption coordinated by calcium and T1R taste receptors in rat small intestine. J. Physiol. 2009, 587, 195–210. [Google Scholar] [CrossRef]
- Sylvetsky, A.C.; Conway, E.M.; Malhotra, S.; Rother, K.I. development of sweet taste perception: Implications for artificial sweetener use. Endocr. Dev. 2017, 32, 87–99. [Google Scholar] [CrossRef]
- Kojima, I.; Nakagawa, Y. The role of the sweet taste receptor in enteroendocrine cells and pancreatic beta-cells. Diabetes Metab. J. 2011, 35, 451–457. [Google Scholar] [CrossRef] [Green Version]
- Lee, R.J.; Kofonow, J.M.; Rosen, P.L.; Siebert, A.P.; Chen, B.; Doghramji, L.; Xiong, G.; Adappa, N.D.; Palmer, J.N.; Kennedy, D.W.; et al. Bitter and sweet taste receptors regulate human upper respiratory innate immunity. J. Clin. Investig. 2014, 124, 1393–1405. [Google Scholar] [CrossRef] [Green Version]
- Kyriazis, G.A.; Soundarapandian, M.M.; Tyrberg, B. Sweet taste receptor signaling in beta cells mediates fructose-induced potentiation of glucose-stimulated insulin secretion. Proc. Natl. Acad. Sci. USA 2012, 109, E524–E532. [Google Scholar] [CrossRef] [Green Version]
- Welcome, M.O.; Mastorakis, N.E.; Pereverzev, V.A. Sweet taste receptor signaling network: Possible implication for cognitive functioning. Neurol. Res. Int. 2015, 2015, 606479. [Google Scholar] [CrossRef] [Green Version]
- Sanematsu, K.; Yoshida, R.; Shigemura, N.; Ninomiya, Y. Structure, function, and signaling of taste G-protein-coupled receptors. Curr. Pharm. Biotechnol. 2014, 15, 951–961. [Google Scholar] [CrossRef]
- Jiang, P.; Cui, M.; Zhao, B.; Liu, Z.; Snyder, L.A.; Benard, L.M.; Osman, R.; Margolskee, R.F.; Max, M. Lactisole interacts with the transmembrane domains of human T1R3 to inhibit sweet taste. J. Biol. Chem. 2005, 280, 15238–15246. [Google Scholar] [CrossRef] [Green Version]
- Beauchamp, G.K.; Cowart, B.J. Development of sweet taste. In Sweetness; Dobbing, J., Ed.; Springer: Basel, Switzerland; New York, NY, USA, 1987; pp. 127–138. [Google Scholar]
- Ramirez, I. Why do sugars taste good? Neurosci. Biobehav. Rev. 1990, 14, 125–134. [Google Scholar] [CrossRef]
- Boers, H.M.; Seijen Ten Hoorn, J.; Mela, D.J. A systematic review of the influence of rice characteristics and processing methods on postprandial glycaemic and insulinaemic responses. Br. J. Nutr. 2015, 114, 1035–1045. [Google Scholar] [CrossRef]
- Drewnowski, A.; Henderson, S.A.; Shore, A.B.; Barratt-Fornell, A. Nontasters, tasters, and supertasters of 6-n-propylthiouracil (PROP) and hedonic response to sweet. Physiol. Behav. 1997, 62, 649–655. [Google Scholar] [CrossRef]
- Drewnowski, A.; Henderson, S.A.; Levine, A.; Hann, C. Taste and food preferences as predictors of dietary practices in young women. Public Health Nutr. 1999, 2, 513–519. [Google Scholar] [CrossRef] [Green Version]
- Bowen, D.J.; Grunberg, N.E. Variations in food preference and consumption across the menstrual cycle. Physiol. Behav. 1990, 47, 287–291. [Google Scholar] [CrossRef]
- Mizuta, E.; Kokubo, Y.; Yamanaka, I.; Miyamoto, Y.; Okayama, A.; Yoshimasa, Y.; Tomoike, H.; Morisaki, H.; Morisaki, T. Leptin gene and leptin receptor gene polymorphisms are associated with sweet preference and obesity. Hypertens. Res. 2008, 31, 1069–1077. [Google Scholar] [CrossRef] [Green Version]
- Tucci, S.A.; Murphy, L.E.; Boyland, E.J.; Dye, L.; Halford, J.C.G. Oral contraceptive effects on food choice during the follicular and luteal phases of the menstrual cycle. A laboratory based study. Appetite 2010, 55, 388–392. [Google Scholar] [CrossRef]
- Conroy, R.; Febres, G.; McMahon, D.J.; Thorner, M.O.; Gaylinn, B.D.; Conwell, I.; Aronne, L.; Korner, J. Recombinant human leptin does not alter gut hormone levels after gastric bypass but may attenuate sweet cravings. Int. J. Endocrinol. 2014, 2014, 120286. [Google Scholar] [CrossRef] [Green Version]
- Kontukoski, M.; Luomala, H.; Mesz, B.; Sigman, M.; Trevisa, M.; Rotola-Pukkila, M.; Inkeri, A. Sweet and sour: Music and taste associations. Nutr. Food Sci. 2015, 45, 357–376. [Google Scholar] [CrossRef]
- Lampuré, A.; Schlich, P.; Deglaire, A.; Castetbon, K.; Péneau, S.; Hercberg, S.; Méjean, C. Sociodemographic, psychological, and lifestyle characteristics are associated with a liking for salty and sweet tastes in French adults. J. Nutr. 2015, 145, 587–594. [Google Scholar] [CrossRef] [Green Version]
- Zhou, B.; Yamanaka-Okumura, H.; Adachi, C.; Kawakami, Y.; Katayama, T.; Takeda, E. High-fat diet-related stimulation of sweetness desire is greater in women than in men despite high vegetable intake. Public Health Nutr. 2015, 18, 1272–1281. [Google Scholar] [CrossRef]
- Tatano, H.; Yamanaka-Okumura, H.; Zhou, B.; Adachi, C.; Kawakami, Y.; Katayama, T.; Masuda, M.; Takeda, E.; Taketani, Y. Association of habitual high-fat intake and desire for protein and sweet food. J. Med. Investig. 2016, 63, 241–247. [Google Scholar] [CrossRef]
- Desor, J.A.; Greene, L.S.; Maller, O. Preferences for sweet and salty in 9- to 15-year-old and adult humans. Science 1975, 190, 686–687. [Google Scholar] [CrossRef] [PubMed]
- Desor, J.A.; Beauchamp, G.K. Longitudinal changes in sweet preferences in humans. Physiol. Behav. 1987, 39, 639–641. [Google Scholar] [CrossRef]
- De Graaf, C.; Zandstra, E.H. Sweetness intensity and pleasantness in children, adolescents, and adults. Physiol. Behav. 1999, 67, 513–520. [Google Scholar] [CrossRef]
- Liem, D.G.; de Graaf, C. Sweet and sour preferences in young children and adults: Role of repeated exposure. Physiol. Behav. 2004, 83, 421–429. [Google Scholar] [CrossRef] [PubMed]
- Mojet, J.; Christ-Hazelhof, E.; Heidema, J. Taste perception with age: Pleasantness and its relationships with threshold sensitivity and supra-threshold intensity of five taste qualities. Food Qual. Prefer. 2005, 16, 413–423. [Google Scholar] [CrossRef]
- Pepino, M.Y.; Mennella, J.A. Sucrose-induced analgesia is related to sweet preferences in children but not adults. Pain 2005, 119, 210–218. [Google Scholar] [CrossRef] [Green Version]
- Mennella, J.A.; Finkbeiner, S.; Reed, D.R. The proof is in the pudding: Children prefer lower fat but higher sugar than do mothers. Int. J. Obes. (Lond.) 2012, 36, 1285–1291. [Google Scholar] [CrossRef] [Green Version]
- Mennella, J.A.; Finkbeiner, S.; Lipchock, S.V.; Hwang, L.D.; Reed, D.R. Preferences for salty and sweet tastes are elevated and related to each other during childhood. PLoS ONE 2014, 9, e92201. [Google Scholar] [CrossRef] [Green Version]
- Bobowski, N.; Mennella, J.A. Personal variation in preference for sweetness: Effects of age and obesity. Child Obes. 2017, 13, 369–376. [Google Scholar] [CrossRef]
- Pangborn, R.M. Influence of hunger on sweetness preferences and taste thresholds. Am. J. Clin. Nutr. 1959, 7, 280–287. [Google Scholar] [CrossRef]
- Moskowitz, H.R.; Kumraiah, V.; Sharma, K.N.; Jacobs, H.L.; Sharma, S.D. Effects of hunger, satiety and glucose load upon taste intensity and taste hedonics. Physiol. Behav. 1976, 16, 471–475. [Google Scholar] [CrossRef]
- Fantino, M.; Baigts, F.; Cabanac, M.; Apfelbaum, M. Effects of an overfeeding regimen—The affective component of the sweet sensation. Appetite 1983, 4, 155–164. [Google Scholar] [CrossRef]
- Looy, H.; Weingarten, H.P. Effects of metabolic state on sweet taste reactivity in humans depend on underlying hedonic response profile. Chem. Senses 1991, 16, 123–130. [Google Scholar] [CrossRef]
- Laeng, B.; Berridge, K.C.; Butter, C.M. Pleasantness of a sweet taste during hunger and satiety: Effects of gender and “sweet tooth”. Appetite 1993, 21, 247–254. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martin, A.A.; Ferriday, D.; Rogers, P.J.; Brunstrom, J.M. Modulation of sweet preference by the actual and anticipated consequences of eating. Appetite 2016, 107, 575–584. [Google Scholar] [CrossRef] [PubMed]
- Wise, P.M.; Nattress, L.; Flammer, L.J.; Beauchamp, G.K. Reduced dietary intake of simple sugars alters perceived sweet taste intensity but not perceived pleasantness. Am. J. Clin. Nutr. 2016, 103, 50–60. [Google Scholar] [CrossRef]
- Pangborn, R.M.; Giovanni, M.E. Dietary intake of sweet foods and of dairy fats and resultant gustatory responses to sugar in lemonade and to fat in milk. Appetite 1984, 5, 317–327. [Google Scholar] [CrossRef]
- Garneau, N.L.; Nuessle, T.M.; Mendelsberg, B.J.; Shepard, S.; Tucker, R.M. Sweet liker status in children and adults: Consequences for beverage intake in adults. Food Qual. Prefer. 2018, 65, 175–180. [Google Scholar] [CrossRef]
- Divert, C.; Chabanet, C.; Schoumacker, R.; Martin, C.; Lange, C.; Issanchou, S.; Nicklaus, S. Relation between sweet food consumption and liking for sweet taste in French children. Food Qual. Prefer. 2017, 56, 18–27. [Google Scholar] [CrossRef]
- Ashi, H.; Campus, G.; Berteus Forslund, H.; Hafiz, W.; Ahmed, N.; Lingstrom, P. The influence of sweet taste perception on dietary intake in relation to dental caries and BMI in Saudi Arabian schoolchildren. Int. J. Dent. 2017, 2017, 4262053. [Google Scholar] [CrossRef]
- Vazquez, M.; Pearson, P.B.; Beauchamp, G.K. Flavor preferences in malnourished Mexican infants. Physiol. Behav. 1982, 28, 513–519. [Google Scholar] [CrossRef]
- Coldwell, S.E.; Oswald, T.K.; Reed, D.R. A marker of growth differs between adolescents with high vs. low sugar preference. Physiol. Behav. 2009, 96, 574–580. [Google Scholar] [CrossRef] [Green Version]
- Dippel, R.L.; Elias, J.W. Preferences for sweet in relationship to use of oral contraceptives and pregnancy. Horm. Behav. 1980, 14, 1–6. [Google Scholar] [CrossRef]
- Wright, P.; Crow, R.A. Menstrual cycle effect of sweetness preferences in women. Horm. Behav. 1973, 4, 387–391. [Google Scholar] [CrossRef]
- Plinerm, P.; Fleming, A.S. Food intake, body weight, and sweetness preferences over the menstrual cycle in humans. Physiol. Behav. 1983, 30, 663–666. [Google Scholar] [CrossRef]
- Brown, M.S.; Grunfeld, C.C. Taste preferences of infants for sweetened or unsweetened foods. Res. Nurs. Health 1980, 3, 11–17. [Google Scholar] [CrossRef] [PubMed]
- Frye, C.A.; Crystal, S.; Ward, K.D.; Kanarek, R.B. Menstrual cycle and dietary restraint influence taste preferences in young women. Physiol. Behav. 1994, 55, 561–567. [Google Scholar] [CrossRef]
- Bretz, W.A.; Corby, P.M.; Melo, M.R.; Coelho, M.Q.; Costa, S.M.; Robinson, M.; Schork, N.J.; Drewnowski, A.; Hart, T.C. Heritability estimates for dental caries and sucrose sweetness preference. Arch. Oral Biol. 2006, 51, 1156–1160. [Google Scholar] [CrossRef]
- Keskitalo, K.; Knaapila, A.; Kallela, M.; Palotie, A.; Wessman, M.; Sammalisto, S.; Peltonen, L.; Tuorila, H.; Perola, M. Sweet taste preferences are partly genetically determined: Identification of a trait locus on chromosome 16. Am. J. Clin. Nutr. 2007, 86, 55–63. [Google Scholar] [CrossRef] [Green Version]
- Keskitalo, K.; Tuorila, H.; Spector, T.D.; Cherkas, L.F.; Knaapila, A.; Silventoinen, K.; Perola, M. Same genetic components underlie different measures of sweet taste preference. Am. J. Clin. Nutr. 2007, 86, 1663–1669. [Google Scholar] [CrossRef]
- Bartoshuk, L.M.; Duffy, V.B.; Miller, I.J. PTC/PROP tasting: Anatomy, psychophysics, and sex effects. Physiol. Behav. 1994, 56, 1165–1171, Erratum in 1995, 58, 203. [Google Scholar] [CrossRef]
- Bartoshuk, L.M. Bitter taste of saccharin related to the genetic ability to taste the bitter substance 6-n-propylthiouracil. Science 1979, 205, 934–935. [Google Scholar] [CrossRef] [PubMed]
- Gent, J.F.; Bartoshuk, L.M. Sweetness of sucrose, neohesperidin dihydrochalcone, and saccharin is related to genetic ability to taste the bitter substance 6-n-propylthiouracil. Chem. Senses 1983, 7, 265–272. [Google Scholar] [CrossRef]
- Schiffman, S.S.; Crofton, V.A.; Beeker, T.G. Sensory evaluation of soft drinks with various sweeteners. Physiol. Behav. 1985, 34, 369–377. [Google Scholar] [CrossRef]
- Drewnowski, A.; Ahlstrom Henderson, S.; Barratt-Fornell, A. Genetic sensitivity to 6-n-propylthiouracil and sensory responses to sugar and fat mixtures. Physiol. Behav. 1998, 63, 771–777. [Google Scholar] [CrossRef]
- Nagy, A.; Steele, C.M.; Pelletier, C.A. Differences in swallowing between high and low concentration taste stimuli. Biomed. Res. Int. 2014, 2014, 813084. [Google Scholar] [CrossRef] [Green Version]
- Yeomans, M.R.; Tepper, B.J.; Rietzschel, J.; Prescott, J. Human hedonic responses to sweetness: Role of taste genetics and anatomy. Physiol. Behav. 2007, 91, 264–273. [Google Scholar] [CrossRef]
- Mennella, J.A.; Pepino, M.Y.; Reed, D.R. Genetic and environmental determinants of bitter perception and sweet preferences. Pediatrics 2005, 115, e216–e222. [Google Scholar] [CrossRef] [Green Version]
- Malcolm, R.; O’Neil, P.M.; Hirsch, A.A.; Currey, H.S.; Moskowitz, G. Taste hedonics and thresholds in obesity. Int. J. Obes. 1980, 4, 203–212. [Google Scholar]
- Ettinger, L.; Duizer, L.; Caldwell, T. Body fat, sweetness sensitivity, and preference: Determining the relationship. Can. J. Diet. Pract. Res. 2012, 73, 45–48. [Google Scholar] [CrossRef]
- Pepino, M.Y.; Mennella, J.A. Habituation to the pleasure elicited by sweetness in lean and obese women. Appetite 2012, 58, 800–805. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Connolly, L.; Coveleskie, K.; Kilpatrick, L.A.; Labus, J.S.; Ebrat, B.; Stains, J.; Jiang, Z.; Tillisch, K.; Raybould, H.E.; Mayer, E.A. Differences in brain responses between lean and obese women to a sweetened drink. Neurogastroenterol. Motil. 2013, 25, 579. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wooley, O.W.; Wooley, S.C.; Dunham, R.B. Calories and sweet taste: Effects on sucrose preference in the obese and nonobese. Physiol. Behav. 1972, 9, 765–768. [Google Scholar] [CrossRef]
- Von Atzingen, M.C.B.C.; Machado Pinto e Silva, E. Sweet and salt pleasantness are not related to nutritional status. Int. J. Food Sci. Nutr. Eng. 2012, 2, 39–43. [Google Scholar] [CrossRef]
- Pepino, M.Y.; Eisenstein, S.A.; Bischoff, A.N.; Klein, S.; Moerlein, S.M.; Perlmutter, J.S.; Black, K.J.; Hershey, T. Sweet dopamine: Sucrose preferences relate differentially to striatal D2 receptor binding and age in obesity. Diabetes 2016, 65, 2618–2623. [Google Scholar] [CrossRef] [Green Version]
- Hardikar, S.; Hochenberger, R.; Villringer, A.; Ohla, K. Higher sensitivity to sweet and salty taste in obese compared to lean individuals. Appetite 2017, 111, 158–165. [Google Scholar] [CrossRef] [Green Version]
- Alexy, U.T.E.; Schaefer, A.; Sailer, O.; Busch-Stockfisch, M.; Huthmacher, S.; Kunert, J.; Kersting, M. Sensory preferences and discrimination ability of children in relation to their body weight status. J. Sens. Stud. 2011, 26, 409–412. [Google Scholar] [CrossRef]
- Grinker, J.A.; Gropman-Rubin, J.; Bose, K. Sweet preference and body fatness: Neonatal data. Nutr. Behav. 1986, 3, 197–209. [Google Scholar]
- Lanfer, A.; Knof, K.; Barba, G.; Veidebaum, T.; Papoutsou, S.; de Henauw, S.; Soós, T.; Moreno, L.A.; Ahrens, W.; Lissner, L. Taste preferences in association with dietary habits and weight status in European children: Results from the IDEFICS study. Int. J. Obes. (Lond.) 2012, 36, 27–34. [Google Scholar] [CrossRef] [Green Version]
- Alexy, U.; Schaefer, A.; Sailer, O.; Busch-Stockfisch, M.; Reinehr, T.; Kunert, J.; Kersting, M. Sensory preferences and discrimination ability of children before and after an obesity intervention. Int. J. Pediatr. Obes. 2010, 5, 116–119. [Google Scholar] [CrossRef]
- Asao, K.; Rothberg, A.E.; Arcori, L.; Kaur, M.; Fowler, C.E.; Herman, W.H. Sweet taste preferences before and after an intensive medical weight loss intervention. Obes. Sci. Pract. 2016, 2, 189–195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burgess, B.; Rao, S.P.; Tepper, B.J. Changes in liking for sweet and fatty foods following weight loss in women are related to prop phenotype but not to diet. Obesity 2016, 24, 1867–1873. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Drewnowski, A.; Holden-Wiltse, J. Taste responses and food preferences in obese women: Effects of weight cycling. Int. J. Obes. Relat. Metab. Disord. 1992, 16, 639–648. [Google Scholar] [PubMed]
- Kleifield, E.I.; Lowe, M.R. Weight loss and sweetness preferences: The effects of recent versus past weight loss. Physiol. Behav. 1991, 49, 1037–1042. [Google Scholar] [CrossRef]
- Ferber, C.; Cabanac, M. Influence of noise on gustatory affective ratings and preference for sweet or salt. Appetite 1987, 8, 229–235. [Google Scholar] [CrossRef]
- Kampov-Polevoy, A.B.; Alterman, A.; Khalitov, E.; Garbutt, J.C. Sweet preference predicts mood altering effect of and impaired control over eating sweet foods. Eat. Behav. 2006, 7, 181–187. [Google Scholar] [CrossRef]
- Saliba, A.J.; Wragg, K.; Richardson, P. Sweet taste preference and personality traits using a white wine. Food Qual. Prefer. 2009, 20, 572–575. [Google Scholar] [CrossRef]
- Sena-Esteves, M.M.; Mota, M.; Malfeito-Ferreira, M. Patterns of sweetness preference in red wine according to consumer characterisation. Food Res. Int. 2018, 106, 38–44. [Google Scholar] [CrossRef] [Green Version]
- Weafer, J.; Burkhardt, A.; de Wit, H. Sweet taste liking is associated with impulsive behaviors in humans. Front. Behav. Neurosci. 2014, 8, 228. [Google Scholar] [CrossRef] [Green Version]
- Stone, L.J.; Pangborn, R.M. Preferences and intake measures of salt and sugar, and their relation to personality traits. Appetite 1990, 15, 63–79. [Google Scholar] [CrossRef]
- Bertino, M.; Beauchamp, G.K.; Jen, K.-l.C. Rated taste perception in two cultural groups. Chem. Senses 1983, 8, 3–15. [Google Scholar] [CrossRef]
- Jaafar, N.; Abdul Razak, I. Ethnic variations of sweet preferences in Malaysian children: A pilot study. J. Pedod. 1990, 14, 147–149. [Google Scholar] [PubMed]
- Holt, S.H.A.; Cobiac, L.; Beaumont-Smith, N.E.; Easton, K.; Best, D.J. Dietary habits and the perception and liking of sweetness among Australian and Malaysian students: A cross-cultural study. Food Qual. Prefer. 2000, 11, 299–312. [Google Scholar] [CrossRef]
- Takemi, Y.; Woo, T.J. Comparison of sweetness preference and motivational factors between Korean and Japanese children. J. Nutr. Health 2017, 50, 53–63. [Google Scholar] [CrossRef] [Green Version]
- Tuorila, H.; Keskitalo-Vuokko, K.; Perola, M.; Spector, T.; Kaprio, J. Affective responses to sweet products and sweet solution in British and Finnish adults. Food Qual. Prefer. 2017, 62, 128–136. [Google Scholar] [CrossRef] [Green Version]
- Jamel, H.A.; Sheiham, A.; Cowell, C.R.; Watt, R.G. Taste preference for sweetness in urban and rural populations in Iraq. J. Dent. Res. 1996, 75, 1879–1884. [Google Scholar] [CrossRef]
- Salbe, A.D.; DelParigi, A.; Pratley, R.E.; Drewnowski, A.; Tataranni, P.A. Taste preferences and body weight changes in an obesity-prone population. Am. J. Clin. Nutr. 2004, 79, 372–378. [Google Scholar] [CrossRef]
- Sorokowska, A.; Pellegrino, R.; Butovskaya, M.; Marczak, M.; Niemczyk, A.; Huanca, T.; Sorokowski, P. Dietary customs and food availability shape the preferences for basic tastes: A cross-cultural study among Polish, Tsimane’ and Hadza societies. Appetite 2017, 116, 291–296. [Google Scholar] [CrossRef]
- Martin, C.; Bellisle, F. Eating attitudes and taste responses in young ballerinas. Physiol. Behav. 1989, 46, 223–227. [Google Scholar] [CrossRef]
- Crystal, S.; Frye, C.A.; Kanarek, R.B. Taste preferences and sensory perceptions in female varsity swimmers. Appetite 1995, 24, 25–36. [Google Scholar] [CrossRef]
- Beauchamp, G.K.; Moran, M. Dietary experience and sweet taste preference in human infants. Appetite 1982, 3, 139–152. [Google Scholar] [CrossRef]
- Beauchamp, G.K.; Moran, M. Acceptance of sweet and salty tastes in 2-year-old children. Appetite 1984, 5, 291–305. [Google Scholar] [CrossRef]
- Liem, D.G.; Mennella, J.A. Sweet and sour preferences during childhood: Role of early experiences. Dev. Psychobiol. 2002, 41, 388–395. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liem, D.G.; Mars, M.; De Graaf, C. Sweet preferences and sugar consumption of 4- and 5-year-old children: Role of parents. Appetite 2004, 43, 235–245. [Google Scholar] [CrossRef] [PubMed]
- Fry Vennerød, F.F.; Lengard Almli, V.; Berget, I.; Lien, N. Do parents form their children’s sweet preference? The role of parents and taste sensitivity on preferences for sweetness in pre-schoolers. Food Qual. Prefer. 2017, 62, 172–182. [Google Scholar] [CrossRef] [Green Version]
- Sunday, S.R.; Halmi, K.A. Taste perceptions and hedonics in eating disorders. Physiol. Behav. 1990, 48, 587–594. [Google Scholar] [CrossRef]
- Travers, J.B.; Akey, L.R.; Chen, S.C.; Rosen, S.; Paulson, G.; Travers, S.P. Taste preferences in Parkinson’s disease patients. Chem. Senses 1993, 18, 47–55. [Google Scholar] [CrossRef]
- Franko, D.L.; Wolfe, B.E.; Jimerson, D.C. Elevated sweet taste pleasantness ratings in bulimia nervosa. Physiol. Behav. 1994, 56, 969–973. [Google Scholar] [CrossRef]
- Berlin, I.; Givry-Steiner, L.; Lecrubier, Y.; Puech, A.J. Measures of anhedonia and hedonic responses to sucrose in depressive and schizophrenic patients in comparison with healthy subjects. Eur. Psychiatry 1998, 13, 303–309. [Google Scholar] [CrossRef]
- Sienkiewicz-Jarosz, H.; Scinska, A.; Swiecicki, L.; Lipczynska-Lojkowska, W.; Kuran, W.; Ryglewicz, D.; Kolaczkowski, M.; Samochowiec, J.; Bienkowski, P. Sweet liking in patients with Parkinson’s disease. J. Neurol. Sci. 2013, 329, 17–22. [Google Scholar] [CrossRef]
- Swiecicki, L.; Scinska, A.; Bzinkowska, D.; Torbinski, J.; Sienkiewicz-Jarosz, H.; Samochowiec, J.; Bienkowski, P. Intensity and pleasantness of sucrose taste in patients with winter depression. Nutr. Neurosci. 2015, 18, 186–191. [Google Scholar] [CrossRef] [PubMed]
- Goodman, E.L.; Breithaupt, L.; Watson, H.J.; Peat, C.M.; Baker, J.H.; Bulik, C.M.; Brownley, K.A. Sweet taste preference in binge-eating disorder: A preliminary investigation. Eat. Behav. 2018, 28, 8–15. [Google Scholar] [CrossRef] [PubMed]
- Tepper, B.J.; Seldner, A.C. Sweet taste and intake of sweet foods in normal pregnancy and pregnancy complicated by gestational diabetes mellitus. Am. J. Clin. Nutr. 1999, 70, 277–284. [Google Scholar] [CrossRef] [PubMed]
- Tepper, B.J.; Hartfiel, L.M.; Schneider, S.H. Sweet taste and diet in type II diabetes. Physiol. Behav. 1996, 60, 13–18. [Google Scholar] [CrossRef]
- Yu, J.H.; Shin, M.S.; Lee, J.R.; Choi, J.H.; Koh, E.H.; Lee, W.J.; Park, J.Y.; Kim, M.S. Decreased sucrose preference in patients with type 2 diabetes mellitus. Diabetes Res. Clin. Pract. 2014, 104, 214–219. [Google Scholar] [CrossRef] [PubMed]
- Bellisle, F.; Dartois, A.M.; Kleinknecht, C.; Broyer, M. Perceptions of and preferences for sweet taste in uremic children. J. Am. Diet. Assoc. 1990, 90, 951–954. [Google Scholar]
- Prince, M.E.; Hoffman, C.J.; Pleasant, M.M. Sweetness thresholds and preferences of individuals with Prader-Willi syndrome. Top Clin. Nutr. 1999, 14, 58–63. [Google Scholar] [CrossRef]
- Frijters, J.E. Sweetness intensity perception and sweetness pleasantness in women varying in reported restraint of eating. Appetite 1984, 5, 103–108. [Google Scholar] [CrossRef]
- Habhab, S.; Sheldon, J.P.; Loeb, R.C. The relationship between stress, dietary restraint, and food preferences in women. Appetite 2009, 52, 437–444. [Google Scholar] [CrossRef]
- Kim, G.-H.; Hwang, J.-H.; Song, K.-H.; Kim, M.-J.; Lee, H.-M. The factors affecting sweet taste sensitivity and preference of the Korean middle-aged females. J. Community Nutr. 2006, 8, 107–113. [Google Scholar]
- Gawecki, J.; Urbanowicz, M.; Jeszka, J.; Mazur, B. Feeding habits and their physiological determinants. Relationships between consumer’s preference for sweetness of drinks and certain physiological parameters. Acta Physiol. Pol. 1976, 27, 455–460. [Google Scholar] [PubMed]
- Jayasinghe, S.N.; Kruger, R.; Walsh, D.C.I.; Cao, G.; Rivers, S.; Richter, M.; Breier, B.H. Is sweet taste perception associated with sweet food liking and intake? Nutrients 2017, 9, 750. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahrens, W. Sensory taste preferences and taste sensitivity and the association of unhealthy food patterns with overweight and obesity in primary school children in Europe—A synthesis of data from the IDEFICS study [on behalf of the IDEFICS consortium]. Flavour 2015, 4, 8. [Google Scholar] [CrossRef] [Green Version]
- Iatridi, V.; Hayes, J.E.; Yeomans, M.R. Reconsidering the classification of sweet taste liker phenotypes: A methodological review. Food Qual. Prefer. 2019, 72, 56–76. [Google Scholar] [CrossRef]
- Mennella, J.A.; Bobowski, N.K. The sweetness and bitterness of childhood: Insights from basic research on taste preferences. Physiol. Behav. 2015, 152, 502–507. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kremer, S.; Bult, J.H.; Mojet, J.; Kroeze, J.H. Compensation for age-associated chemosensory losses and its effect on the pleasantness of a custard dessert and a tomato drink. Appetite 2007, 48, 96–103. [Google Scholar] [CrossRef]
- Methven, L.; Allen, V.J.; Withers, C.A.; Gosney, M.A. Ageing and taste. Proc. Nutr. Soc. 2012, 71, 556–565. [Google Scholar] [CrossRef] [Green Version]
- Mojet, J.; Christ-Hazelhof, E.; Heidema, J. Taste perception with age: Generic or specific losses in threshold sensitivity to the five basic tastes? Chem. Senses 2001, 26, 845–860. [Google Scholar] [CrossRef] [Green Version]
- Fukunaga, A.; Uematsu, H.; Sugimoto, K. Influences of aging on taste perception and oral somatic sensation. J. Gerontol. A Biol. Sci. Med. Sci. 2005, 60, 109–113. [Google Scholar] [CrossRef]
- Arvidson, K. Location and variation in number of taste buds in human fungiform papillae. Scand. J. Dent. Res. 1979, 87, 435–442. [Google Scholar] [CrossRef]
- de Boer, A.; Ter Horst, G.J.; Lorist, M.M. Physiological and psychosocial age-related changes associated with reduced food intake in older persons. Ageing Res. Rev. 2013, 12, 316–328. [Google Scholar] [CrossRef] [PubMed]
- Fjell, A.M.; Walhovd, K.B.; Reinvang, I.; Lundervold, A.; Salat, D.; Quinn, B.T.; Fischl, B.; Dale, A.M. Selective increase of cortical thickness in high-performing elderly—Structural indices of optimal cognitive aging. Neuroimage 2006, 29, 984–994. [Google Scholar] [CrossRef] [PubMed]
- Hoogeveen, H.R.; Dalenberg, J.R.; Renken, R.J.; ter Horst, G.J.; Lorist, M.M. Neural processing of basic tastes in healthy young and older adults—An fMRI study. Neuroimage 2015, 119, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beauchamp, G.K.; Cowart, B.J. Congenital and experiential factors in the development of human flavor preferences. Appetite 1985, 6, 357–372. [Google Scholar] [CrossRef]
- Rolls, B.J.; Rowe, E.A.; Rolls, E.T. How sensory properties of foods affect human feeding behavior. Physiol. Behav. 1982, 29, 409–417. [Google Scholar] [CrossRef]
- Sørensen, L.B.; Møller, P.; Flint, A.; Martens, M.; Raben, A. Effect of sensory perception of foods on appetite and food intake: A review of studies on humans. Int. J. Obes. Relat. Metab. Disord. 2003, 27, 1152–1166. [Google Scholar] [CrossRef] [Green Version]
- Hill, W.F. Effects of mere exposure on preference in nonhuman mammals. Psychol. Bull. 1978, 85, 1177–1198, Cited in: Beauchamp and Moran, 1984. [Google Scholar] [CrossRef]
- Mennella, J.A.; Castor, S.M. Sensitive period in flavor learning: Effects of duration of exposure to formula flavors on food likes during infancy. Clin. Nutr. 2012, 31, 1022–1025. [Google Scholar] [CrossRef] [Green Version]
- Duncker, K. Experimental modification of children’s food preferences through social suggestion. J. Abnorm. Soc. Psychol. 1938, 33, 489–507. [Google Scholar] [CrossRef]
- Marino, H. Social influence in the formation of enduring preference. J. Abnorm. Soc. Psychol. 1942, 34, 449–468. [Google Scholar] [CrossRef]
- Kumar, P.; Magon, N. Hormones in pregnancy. Niger. Med. J. 2012, 53, 179–183. [Google Scholar] [CrossRef] [PubMed]
- Faas, M.M.; Melgert, B.N.; De Vos, P. A brief review on how pregnancy and sex hormones interfere with taste and food intake. Chemosens. Percept. 2010, 3, 51–56. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 1 | Standardization of Procedures for Examiners | |
| 1a | Smoking status | |
| 1b | Avoidance of scented personal products (i.e., perfume/cologne use) | |
| 1c | Avoidance of confectionary consumption (e.g., gums/mints) with strong flavors/scents | |
| 1d | Avoidance of foods with strong odors | |
| 1e | Standardization of questioning and information provided to subjects | |
| 2 | Standardization of Subject Characteristics | |
| 2a | Age | |
| 2b | Gender | |
| 2c | BMI/body weight | |
| 2d | Ethnicity/culture | |
| 2e | For females, stage of the menstrual cycle, and/or pregnancy status | |
| 2f | Health status (e.g., chronic disease state) | |
| 2g | Health status (e.g., acute disease/health condition that could affect sweetness preference) | |
| 2h | Medication use | |
| 3 | Standardization of Procedures for Subjects | |
| 3a | Fasting; satiation status | |
| 3b | Standardization of last meal consumed (NA: If subjects fasted overnight) | |
| 3c | Smoking (i.e., including vaping, snuff, chewing tobacco, e-cigarettes, etc.) | |
| 3d | Alcohol consumption/use of recreational drugs (e.g., cannabis) | |
| 3e | Avoidance of scented personal products (i.e., perfume/cologne use) | |
| 3f | Avoidance of confectionary (e.g., gums/mints) with strong flavors/scents; teeth brushing/use of mouthwash | |
| 3g | Physical activity | |
| 3h | Habitual use of non-caloric sweeteners (not applicable for caloric sweetener studies) | |
| 4 | Standardization of Sweetness Preference Testing | |
| 4a | Clear reporting of sweetener or sweetened product tested | |
| 4b | Clear reporting of sweetness concentrations tested | |
| 4c | Vehicle composition across challenges changes only with regards to sweetness | |
| 4d | Random order of challenges | |
| 4e | Consistent volume/amount of each challenge | |
| 4f | Consistent temperature of each challenge | |
| 4g | Consistent presentation of each challenge (e.g., in opaque cups) | |
| 4h | Consistent nature of each challenge (e.g., whole mouth rinse, complete ingestion, or swabbing of a particular area on the tongue) | |
| 4i | Consistent duration of each challenge | |
| 4j | Consistent time of day at which challenges were presented | |
| 4k | Rinsing of palate between challenges | |
| 4l | Consistent time interval between challenges | |
| 4m | Control of environmental stimuli during sweetness testing | |
| Sweetness Preference Determinant | Studies | Overall Findings | |
|---|---|---|---|
| No. | Consistent Findings? | ||
| 1. Age | 9 | Yes | •  in childhood and elderly populations. in childhood and elderly populations. |
| 2. Dietary/Nutritional Factors | 14 | Some | • in fasted vs. satiated state. |
| • Findings for sweetness preference based on dietary macronutrient composition or meal composition were inconsistent. | |||
| 3. Reproductive Hormonal Factors | 7 | Some | • Possible inverse relationship:  with higher levels of progesterone. with higher levels of progesterone. |
| 4. Genetics/Heritability | 9 | Some | • Heritability accounted for some of the variability in sweetness preference. |
| • Inconsistent findings with respect to sweetness preference and PROP sensitivity. | |||
| 5. Body Weight | 11 | Yes | • No association between sweetness preference and BMI status across age groups and genders. |
| 6. Weight Loss | 5 | No | • Inconsistent findings with respect to the effects of weight loss on sweetness preference. |
| 7. Sound | 2 | N/A | • Limited evidence to draw conclusions. |
| 8. Personality Traits | 5 | No | • Inconsistent findings. Limited evidence to draw conclusions. |
| 9. Ethnicity and Lifestyle | |||
| • Different Ethnic Groups | 5 | Yes | • among westernized cultures compared to their Asian counterparts. |
| • may be due to familiarization of foods. | |||
| • Traditional/Modern Lifestyles | 3 | Yes | • with a modern vs. traditional lifestyle. |
| • may be due to familiarization of foods. | |||
| • Physical Activity Levels | 2 | Yes | • in individuals who are more vs. less physically active. |
| 10. Previous Sweetness Exposure | 6 | No | • Inconsistent findings. |
| 11. Disease | |||
| • Neurological/Psychological | 7 | No | • Inconsistent findings among studies in subjects with a neurological or psychological disease. |
| • T2DM/GDM | 3 | No | • Limited evidence among studies in individuals with T2DM or GDM to draw conclusions. |
| Other | 2 | No | • Limited evidence among studies in individuals with other diseases (namely, PWS or end-stage renal disease) to draw conclusions. |
| 12. Other Factors | 8 | N/A | • Study objectives and results were too diverse to draw conclusions. |
= increased sweetness preference; = decreased sweetness preference; BMI = body mass index; b/w = between; GDM = gestational diabetes mellitus; N/A = not applicable; No. = number; PROP = 6-n-propylthiouracil; PWS = Prader-Willi Syndrome; T2DM = type 2 diabetes mellitus; GDM = Gestational Diabetes Mellitus; vs. = versus.© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Venditti, C.; Musa-Veloso, K.; Lee, H.Y.; Poon, T.; Mak, A.; Darch, M.; Juana, J.; Fronda, D.; Noori, D.; Pateman, E.; et al. Determinants of Sweetness Preference: A Scoping Review of Human Studies. Nutrients 2020, 12, 718. https://doi.org/10.3390/nu12030718
Venditti C, Musa-Veloso K, Lee HY, Poon T, Mak A, Darch M, Juana J, Fronda D, Noori D, Pateman E, et al. Determinants of Sweetness Preference: A Scoping Review of Human Studies. Nutrients. 2020; 12(3):718. https://doi.org/10.3390/nu12030718
Chicago/Turabian StyleVenditti, Carolina, Kathy Musa-Veloso, Han Youl Lee, Theresa Poon, Alastair Mak, Maryse Darch, Justine Juana, Dylan Fronda, Daniel Noori, Erika Pateman, and et al. 2020. "Determinants of Sweetness Preference: A Scoping Review of Human Studies" Nutrients 12, no. 3: 718. https://doi.org/10.3390/nu12030718