Reproducibility of a Short-Form, Multicomponent Dietary Questionnaire to Assess Food Frequency Consumption, Nutrition Knowledge, and Lifestyle (SF-FFQ4PolishChildren) in Polish Children and Adolescents

 ,
,  ,
,  , ,
, ,  , , , ,
, , , ,  , ,
, ,  , , , , , ,
, , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Approval
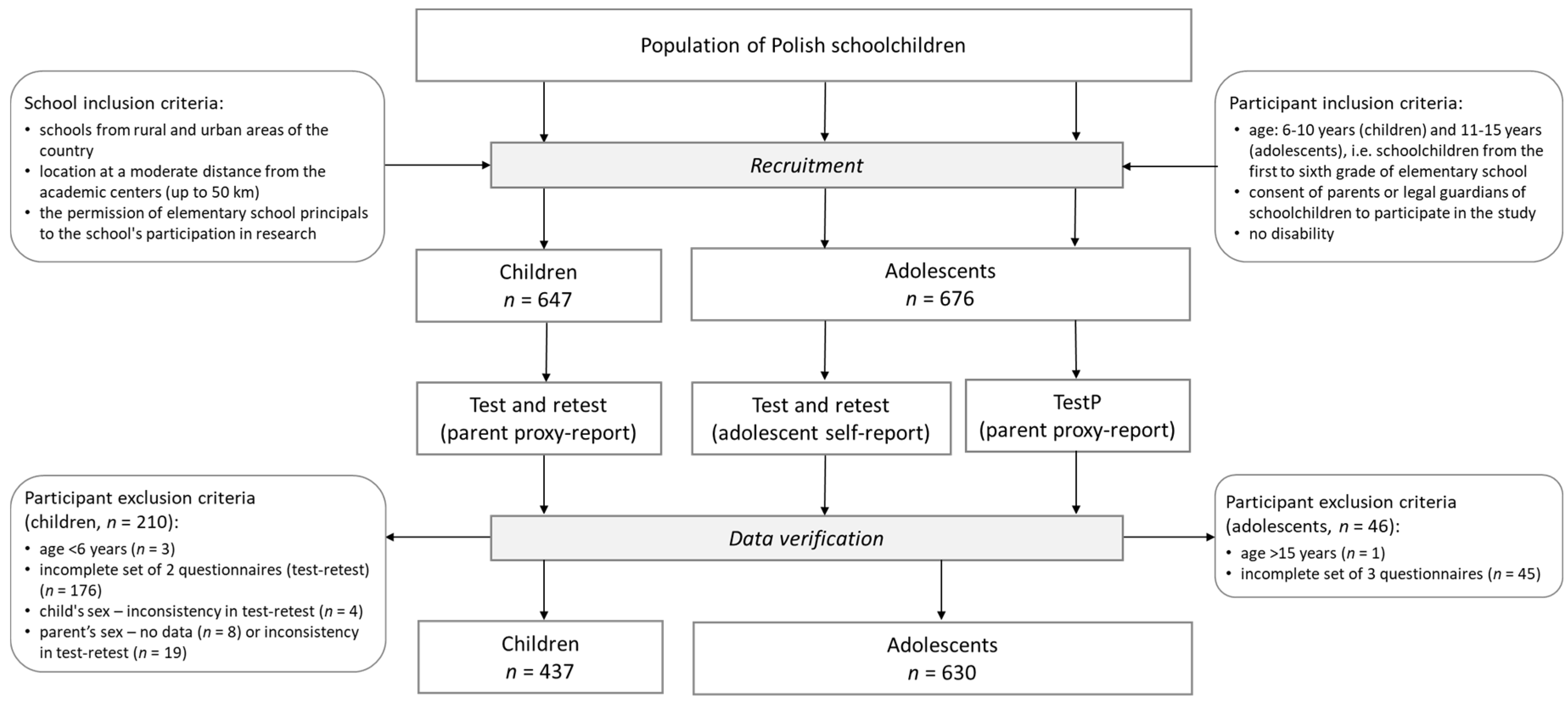
2.2. Study Design
2.3. Participants
2.4. A Short-Form, Multicomponent Dietary Questionnaire (SF-FFQ4PolishChildren)
2.5. Dietary Habits
2.6. Nutrition Knowledge
2.7. Active/Sedentary Lifestyle
2.8. The Family Affluence Scale Components
2.9. Anthropometric Data
2.10. Statistical Analysis
3. Results
3.1. Participant Characteristics
3.2. Nutrition Knowledge
3.3. Dietary Habits
3.4. Active/Sedentary Lifestyle
3.5. Socioeconomic Data
3.6. Anthropometric Data
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Craigie, A.M.; Lake, A.A.; Kelly, S.A.; Adamson, A.J.; Mathers, J.C. Tracking of obesity-related behaviours from childhood to adulthood: A systematic review. Maturitas 2011, 70, 266–284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Movassagh, E.Z.; Baxter-Jones, A.D.G.G.; Kontulainen, S.; Whiting, S.J.; Vatanparast, H. Tracking dietary patterns over 20 years from childhood through adolescence into young adulthood: The Saskatchewan Pediatric Bone Mineral Accrual Study. Nutrients 2017, 9, 990. [Google Scholar] [CrossRef] [PubMed]
- Suppli, C.H.; Due, P.; Henriksen, P.W.; Rayce, S.L.B.; Holstein, B.E.; Rasmussen, M. Low vigorous physical activity at ages 15, 19 and 27: Childhood socio-economic position modifies the tracking pattern. Eur. J. Public Health 2013, 23, 19–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thompson, F.; Subar, A. Dietary assessment methodology. In Nutrition in the Prevention and Treatment of Disease, 2nd ed.; Coulston, A.M., Boushey, C.J., Eds.; Academic Press: San Diego, CA, USA, 2008; pp. 3–39. [Google Scholar]
- Livingstone, M.B.E.; Robson, P.J.; Wallace, J.M.W. Issues in dietary intake assessment of children and adolescents. Br. J. Nutr. 2004, 92, S213–S222. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Rodrigo, C.; Escauriaza, B.A.; Bartrina, J.A.; Allúe, I.P. Dietary assessment in children and adolescents: Issues and recommendations. Nutr. Hosp. 2015, 31, 76–83. [Google Scholar] [PubMed]
- Food and Agriculture Organization (FAO). Dietary Assessment: A Resource Guide to Method Selection and Application in Low Resource Settings; FAO: Rome, Italy, 2018. [Google Scholar]
- Golley, R.K.; Bell, L.K.; Hendrie, G.A.; Rangan, A.M.; Spence, A.; McNaughton, S.A. Validity of short food questionnaire items to measure intake in children and adolescents: A systematic review. J. Hum. Nutr. Diet. 2017, 30, 36–50. [Google Scholar] [CrossRef] [Green Version]
- Lillegaard, I.T.L.; Øverby, N.C.; Andersen, L.F. Evaluation of a short food frequency questionnaire used among Norwegian children. Food Nutr. Res. 2012, 56, 6399–6407. [Google Scholar] [CrossRef] [Green Version]
- Cade, J.; Thompson, R.; Burley, V.; Warm, D. Development, validation and utilisation of food-frequency questionnaires—A review. Public Health Nutr. 2002, 5, 567–587. [Google Scholar] [CrossRef] [Green Version]
- Cade, J.E.; Burley, V.J.; Warm, D.L.; Thompson, R.L.; Margetts, B.M. Food-frequency questionnaires: A review of their design, validation and utilisation. Nutr. Res. Rev. 2004, 17, 5–22. [Google Scholar] [CrossRef] [Green Version]
- Gibson, R. Principles of Nutritional Assessment, 2nd ed.; Oxford University Press: New York, NY, USA, 2005. [Google Scholar]
- Tabacchi, G.; Filippi, A.R.; Amodio, E.; Jemni, M.; Bianco, A.; Firenze, A.; Mammina, C. A meta-analysis of the validity of FFQ targeted to adolescents. Public Health Nutr. 2016, 19, 1168–1183. [Google Scholar] [CrossRef] [Green Version]
- Sochacka-Tatara, E.; Pac, A. Relative validity of a semi-quantitative FFQ in 3-year-old Polish children. Public Health Nutr. 2014, 17, 1738–1744. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kowalkowska, J.; Wadolowska, L.; Czarnocinska, J.; Czlapka-Matyasik, M.; Galinski, G.; Jezewska-Zychowicz, M. Reproducibility of a Questionnaire for Dietary Habits, Lifestyle and Nutrition Knowledge Assessment (KomPAN) in Polish Adolescents and Adults. Nutrients 2018, 10, 1845. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Niedzwiedzka, E.; Wadolowska, L.; Kowalkowska, J. Reproducibility of A Non-Quantitative Food Frequency Questionnaire (62-Item FFQ-6) and PCA-Driven Dietary Pattern Identification in 13–21-Year-Old Females. Nutrients 2019, 11, 2183. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wong, J.E.; Parnell, W.R.; Howe, A.S.; Black, K.E.; Skidmore, P.M. Development and validation of a food-based diet quality index for New Zealand adolescents. BMC Public Health 2013, 13, 562–571. [Google Scholar] [CrossRef] [Green Version]
- Bjørnarå, H.B.; Hillesund, E.R.; Torstveit, M.K.; Stea, T.H.; Øverby, N.C.; Bere, E. An assessment of the test-retest reliability of the New Nordic Diet score. Food Nutr. Res. 2015, 59, 28397–28404. [Google Scholar] [CrossRef] [Green Version]
- Hoelscher, D.M.; Day, R.S.; Kelder, S.H.; Ward, J.L. Reproducibility and validity of the secondary level School-Based Nutrition Monitoring student questionnaire. J. Am. Diet. Assoc. 2003, 103, 186–194. [Google Scholar] [CrossRef]
- Vereecken, C.; De Pauw, A.; Van Cauwenbergh, S.; Maes, L. Development and test-retest reliability of a nutrition knowledge questionnaire for primary-school children. Public Health Nutr. 2012, 15, 1630–1638. [Google Scholar] [CrossRef] [Green Version]
- Grosso, G.; Mistretta, A.; Turconi, G.; Cena, H.; Roggi, C.; Galvano, F. Nutrition knowledge and other determinants of food intake and lifestyle habits in children and young adolescents living in a rural area of Sicily, South Italy. Public Health Nutr. 2013, 16, 1827–1836. [Google Scholar] [CrossRef] [Green Version]
- Hamulka, J.; Wadolowska, L.; Hoffmann, M.; Kowalkowska, J.; Gutkowska, K. Effect of an education program on nutrition knowledge, attitudes toward nutrition, diet quality, lifestyle, and body composition in polish teenagers. The ABC of healthy eating project: Design, protocol, and methodology. Nutrients 2018, 10, 1439. [Google Scholar] [CrossRef] [Green Version]
- Gawecki, J. Dietary Habits and Nutrition Beliefs Questionnaire and the Manual for Developing Nutritional Data; Gawecki, J., Ed.; Committee of Human Nutrition Science, Polish Academy of Sciences: Olsztyn, Poland, 2018; pp. 1–52. [Google Scholar]
- Whati, L.; Senekal, M.; Steyn, N.; Nel, J.; Lombard, C.; Norris, S. Development of a reliable and valid nutritional knowledge questionnaire for urban South African adolescents. Nutrition 2005, 21, 76–85. [Google Scholar] [CrossRef]
- National Food and Nutrition Institute (Poland). Pyramid of Healthy Nutrition and Physical Activity; National Food and Nutrition Institute: Warsaw, Poland, 2018; Available online: http://www.izz.waw.pl/attachments/article/555/Piramida IZZ 1.pdf (accessed on 18 January 2019).
- Mazur, J. Family Affluence Scale—Validation study and suggested modification. Hygeia Public Health 2013, 48, 211–217. [Google Scholar]
- Cole, T.J.; Lobstein, T. Extended international (IOTF) body mass index cut-offs for thinness, overweight and obesity. Pediatr. Obes. 2012, 7, 284–294. [Google Scholar] [CrossRef] [PubMed]
- Bland, J.M.; Altman, D.G. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986, 1, 307–310. [Google Scholar] [CrossRef]
- British Standards Institution. Precision of Test Methods 1: Guide for the Determination and Reproducibility for a Research Test Method (BS 597, Part 1); BSI: London, UK, 1975. [Google Scholar]
- Landis, J.R.; Koch, G.G. The measurement of observer agreement for categorical data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef] [Green Version]
- Bjerregaard, A.A.; Tetens, I.; Olsen, S.F.; Halldorsson, T.I. Reproducibility of a web-based FFQ for 13- to 15-year-old Danish adolescents. J. Nutr. Sci. 2016, 5, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Buch-Andersen, T.; Perez-Cueto Eulert, F.J.A.; Toft, U. Relative validity and reproducibility of a parent-administered semi-quantitative FFQ for assessing food intake in Danish children aged 3–9 years. Public Health Nutr. 2016, 19, 1184–1194. [Google Scholar] [CrossRef] [Green Version]
- Filippi, A.R.; Amodio, E.; Napoli, G.; Breda, J.; Bianco, A.; Jemni, M. The web-based ASSO-food frequency questionnaire for adolescents: Relative and absolute reproducibility assessment. Nutr. J. 2014, 13, 119–129. [Google Scholar] [CrossRef] [Green Version]
- Øverby, N.C.; Johannesen, E.; Jensen, G.; Skjaevesland, A.-K.; Haugen, M. Test-retest reliability and validity of a web-based food-frequency questionnaire for adolescents aged 13-14 to be used in the Norwegian Mother and Child Cohort Study (MoBa). Food Nutr. Res. 2014, 58, 23956–23966. [Google Scholar] [CrossRef] [Green Version]
- Saeedi, P.; Skeaff, S.A.; Wong, J.E.; Skidmore, P.M. Reproducibility and Relative Validity of a Short Food Frequency Questionnaire in 9-10 Year-Old Children. Nutrients 2016, 8, 271. [Google Scholar] [CrossRef] [Green Version]
- Vereecken, C.A.; Maes, L. A Belgian study on the reliability and relative validity of the Health Behaviour in School-Aged Children food-frequency questionnaire. Public Health Nutr. 2003, 6, 581–588. [Google Scholar] [CrossRef] [Green Version]
- Vioque, J.; Gimenez-Monzo, D.; Navarrete-Muñoz, E.M.; Garcia-de-la-Hera, M.; Gonzalez-Palacios, S.; Rebagliato, M. Reproducibility and validity of a food frequency questionnaire designed to assess diet in children aged 4-5 years. PLoS ONE 2016, 11, e0167338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wong, J.E.; Parnell, W.R.; Black, K.E.; Skidmore, P.M. Reliability and relative validity of a food frequency questionnaire to assess food group intakes in New Zealand adolescents. Nutr. J. 2012, 11, 65–73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lanfer, A.; Hebestreit, A.; Ahrens, W.; Krogh, V.; Sieri, S.; Lissner, L. Reproducibility of food consumption frequencies derived from the children’s eating habits questionnaire used in the IDEFICS study. Int. J. Obes. 2011, 35, S61–S68. [Google Scholar] [CrossRef] [Green Version]
- Handeland, K.; Kjellevold, M.; Markhus, M.W.; Graff, I.E.; Frøyland, L.; Lie, Ø. A diet score assessing Norwegian adolescents’ adherence to dietary recommendations—Development and test-retest reproducibility of the score. Nutrients 2016, 8, 467. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kant, A.K. Indexes of overall diet quality: A review. J. Am. Diet. Assoc. 1996, 96, 785–791. [Google Scholar] [CrossRef]
- McPherson, R.S.; Hoelscher, D.M.; Alexander, M.; Scanlon, K.S.; Serdula, M.K. Dietary assessment methods among school-aged children: Validity and reliability. Prev. Med. 2000, 31, S11–S33. [Google Scholar] [CrossRef]
- Kourlaba, G.; Kondaki, K.; Grammatikaki, E.; Roma-Giannikou, E.; Manios, Y. Diet quality of preschool children and maternal perceptions/misperceptions: The GENESIS study. Public Health 2009, 123, 738–742. [Google Scholar] [CrossRef]
- Huybrechts, I.; Vereecken, C.; De Bacquer, D.; Vandevijvere, S.; Van Oyen, H.; Maes, L. Reproducibility and validity of a diet quality index for children assessed using a FFQ. Br. J. Nutr. 2010, 104, 135–144. [Google Scholar] [CrossRef] [Green Version]
- Wilson, A.M.; Magarey, A.M.; Mastersson, N. Reliability and relative validity of a child nutrition questionnaire to simultaneously assess dietary patterns associated with positive energy balance and food behaviours, attitudes, knowledge and environments associated with healthy eating. Int. J. Behav. Nutr. Phys. Act. 2008, 5, 5–16. [Google Scholar] [CrossRef] [Green Version]
- Turconi, G.; Celsa, M.; Rezzani, C.; Biino, G.; Sartirana, M.A.; Roggi, C. Reliability of a dietary questionnaire on food habits, eating behaviour and nutritional knowledge of adolescents. Eur. J. Clin. Nutr. 2003, 57, 753–763. [Google Scholar] [CrossRef] [Green Version]
- Corder, K.; Crespo, N.C.; van Sluijs, E.M.; Lopez, N.V.; Elder, J.P. Parent awareness of young children’s physical activity. Prev. Med. 2012, 55, 201–205. [Google Scholar] [CrossRef] [Green Version]
- Gebremariam, M.K.; Totland, T.H.; Andersen, L.F.; Bergh, I.H.; Bjelland, M.; Grydeland, M. Stability and change in screen-based sedentary behaviours and associated factors among Norwegian children in the transition between childhood and adolescence. BMC Public Health 2012, 12, 104–112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lien, N.; Bjelland, M.; Bergh, I.H.; Grydeland, M.; Anderssen, S.A.; Ommundsen, Y. Design of a 20-month comprehensive, multicomponent school-based randomised trial to promote healthy weight development among 11–13 year olds: The Health in Adolescents study. Scand. J. Public Health 2010, 38, 38–51. [Google Scholar] [CrossRef] [PubMed]
- Andersen, A.; Krølner, R.; Currie, C.; Dallago, L.; Due, P.; Richter, M. High agreement on family affluence between children’s and parents’ reports: International study of 11-year-old children. J. Epidemiol. Community Health 2008, 62, 1092–1094. [Google Scholar] [CrossRef]
- Brettschneider, A.-K.; Ellert, U.; Schaffrath Rosario, A. Comparison of BMI derived from parent-reported height and weight with measured values: Results from the German KiGGS study. Int. J. Environ. Res. Public Health 2012, 9, 632–647. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huybrechts, I.; Himes, J.H.; Ottevaere, C.; De Vriendt, T.; De Keyzer, W.; Cox, B. Validity of parent-reported weight and height of preschool children measured at home or estimated without home measurement: A validation study. BMC Pediatr. 2011, 11, 63–70. [Google Scholar] [CrossRef] [Green Version]
- Niedźwiedzka, E.; Wądołowska, L.; Słowińska, M.; Cichon, R.; Przybyłowicz, K. Self-reported and measured values of body weight and height vs. evaluation of the nutritional status of youth. Pol. J. Environ. Stud. 2006, 15, 716–722. [Google Scholar]
- Statistics Poland. Regions of Poland. Warsaw, Poland. 2016. Available online: https://stat.gov.pl/obszary-tematyczne/inne-opracowania/miasta-wojewodztwa/regiony-polski-2016,6,10.html (accessed on 18 December 2018).
- Field, A.E.; Peterson, K.E.; Gortmaker, S.L.; Cheung, L.; Rockett, H.; Fox, M.K. Reproducibility and validity of a food frequency questionnaire among fourth to seventh grade inner-city school children: Implications of age and day-to-day variation in dietary intake. Public Health Nutr. 1999, 2, 293–300. [Google Scholar] [CrossRef] [Green Version]
- Ortiz-Andrellucchi, A.; Henríquez-Sánchez, P.; Sánchez-Villegas, A.; Peña-Quintana, L.; Mendez, M.; Serra-Majem, L. Dietary assessment methods for micronutrient intake in infants, children and adolescents: A systematic review. Br. J. Nutr. 2009, 102, S87–S117. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Physical Activity at School | Physical Activity at Leisure Time | ||
|---|---|---|---|
| Low | Moderate | High | |
| Low | Low (0 points) | Low (1 points) | Moderate (2 points) |
| Moderate | Low (1 points) | Moderate (3 points) | Moderate (4 points) |
| High | Moderate (2 points) | Moderate (4 points) | High (5 points) |
| Question | Response Categories | |
|---|---|---|
| 1. | How many computers, laptops, or tablets does your family own? | none (0 points); one (1 point); two (2 points); more than two (2 points) |
| 2. | Does your family own a car, van, or truck? | no (0 points); yes, one (1 point); yes, two or more (2 points) |
| 3. | Does your family have a dishwasher? | no (0 points); yes (1 point) |
| 4. | Do you have your own bedroom? | no (0 points); yes (1 point) |
| 5. | How many bathrooms (room with a bath or shower) are in your home? | none (0 points); one (1 point); two (2 points); more than two (2 points) |
| 6. | Does your home have an outdoor space attached (e.g., garden)? | no (0 points); yes (1 point) |
| Variables | Children Aged 6–10 Years (Questionnaire Filled Out by A Parent) | Adolescents Aged 11–15 Years (Questionnaire Filled Out by An Adolescent) | ||
|---|---|---|---|---|
| n | % | n | % | |
| Sample size | 437 | 630 | ||
| Sex | ||||
| boys | 211 | 48.3 | 325 | 51.6 |
| girls | 226 | 51.7 | 305 | 48.4 |
| Age (years) 1 | 437 | 8.0 (7.9; 8.1) | 630 | 12.5 (12.4; 12.6) |
| Residence | 437 | 630 | ||
| rural | 231 | 52.9 | 293 | 46.5 |
| urban 2 | 206 | 47.1 | 337 | 53.5 |
| FAS (points) 1 | 431 | 6.2 (6.0; 6.4) | 622 | 6.8 (6.7; 6.9) |
| Nutrition knowledge score (points) 1,3 | 436 | 10.4 (10.1; 10.6) | 626 | 7.2 (6.9; 7.4) |
| Nutrition knowledge level 3 | 436 | 626 | ||
| low | 28 | 6.4 | 191 | 30.5 |
| moderate | 310 | 71.1 | 417 | 66.6 |
| high | 98 | 22.5 | 18 | 2.9 |
| pHDI (%points) 1 | 433 | 31.5 (30.3; 32.8) | 628 | 29.0 (27.9; 30.1) |
| pHDI category | 433 | 628 | ||
| low | 252 | 58.2 | 417 | 66.4 |
| moderate | 175 | 40.4 | 204 | 32.5 |
| high | 6 | 1.4 | 7 | 1.1 |
| nHDI (%points) 1 | 436 | 13.0 (12.2; 13.9) | 627 | 15.1 (14.2; 16.0) |
| nHDI category | 436 | 627 | ||
| low | 416 | 95.4 | 577 | 92.0 |
| moderate | 20 | 4.6 | 49 | 7.8 |
| high | 0 | 0.0 | 1 | 0.2 |
| Screen time score (points) 1 | 437 | 0.4 (0.4; 0.5) | 629 | 0.9 (0.8; 1.0) |
| Screen time category | 437 | 629 | ||
| <2 h/day | 278 | 63.6 | 262 | 41.7 |
| 2 to <4 h/day | 134 | 30.7 | 238 | 37.8 |
| 4 to <6 h/day | 22 | 5.0 | 90 | 14.3 |
| 6 to <8 h/day | 0 | 0.0 | 19 | 3.0 |
| 8 to <10 h/day | 2 | 0.5 | 10 | 1.6 |
| ≥10 h/day | 1 | 0.2 | 10 | 1.6 |
| Physical activity score (points) 1 | 437 | 3.2 (3.0; 3.3) | 629 | 3.4 (3.3; 3.5) |
| Physical activity level | 437 | 629 | ||
| low | 73 | 16.7 | 99 | 15.7 |
| moderate | 304 | 69.6 | 378 | 60.1 |
| high | 60 | 13.7 | 152 | 24.2 |
| Physical activity at school | 437 | 629 | ||
| low | 74 | 16.9 | 68 | 10.8 |
| moderate | 284 | 65.0 | 316 | 50.2 |
| high | 79 | 18.1 | 245 | 39.0 |
| Physical activity at leisure time | 437 | 629 | ||
| low | 31 | 7.1 | 81 | 12.9 |
| moderate | 219 | 50.1 | 284 | 45.2 |
| high | 187 | 42.8 | 264 | 42.0 |
| BMI-for-age | 415 | 595 | ||
| thinness | 76 | 18.3 | 81 | 13.6 |
| normal weight | 263 | 63.4 | 425 | 71.4 |
| overweight | 76 | 18.3 | 89 | 15.0 |
| Variables | Cat. 1 | Children Aged 6–10 Years | Adolescents Aged 11–15 years | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Parent (Test–Retest) | Adolescent (Test–Retest) | Adolescent (Test) & Parent (TestP) | |||||||||||
| n | Total Agreement | Misclassification | n | Total Agreement | Misclassification | n | Total Agreement | Misclassification | |||||
| ±1 Cat. | ±2 Cat. or More | ±1 Cat. | ±2 Cat. or More | ±1 Cat. | ±2 Cat. or More | ||||||||
| Nutrition knowledge level 2 | 3 | 432 | 85.0 | 14.8 | 0.2 | 615 | 72.7 | 27.3 | 0.0 | 628 | NA | ||
| Dietary habits | |||||||||||||
| Breakfast | 4 | 436 | 88.8 | 7.8 | 3.4 | 629 | 77.3 | 17.8 | 4.9 | 628 | 80.3 | 12.6 | 7.2 |
| Meal at school | 4 | 435 | 95.4 | 3.9 | 0.7 | 629 | 79.8 | 16.2 | 4.0 | 626 | 81.6 | 14.7 | 3.7 |
| Dairy products | 7 | 435 | 68.0 | 24.8 | 7.1 | 630 | 51.3 | 33.8 | 14.9 | 627 | 44.3 | 34.4 | 21.2 |
| Fish | 7 | 436 | 77.1 | 19.3 | 3.7 | 628 | 57.3 | 31.5 | 11.1 | 627 | 50.9 | 37.0 | 12.1 |
| Fast food | 7 | 436 | 80.7 | 16.7 | 2.5 | 628 | 61.8 | 30.9 | 7.3 | 627 | 58.9 | 27.8 | 13.4 |
| Sweetened soft drinks | 7 | 436 | 64.9 | 23.4 | 11.7 | 628 | 50.8 | 26.8 | 22.5 | 628 | 41.1 | 32.0 | 26.9 |
| Fruit or mixed fruit and vegetable juices | 7 | 434 | 59.0 | 26.7 | 14.3 | 629 | 42.9 | 33.7 | 23.4 | 628 | 43.5 | 30.7 | 25.8 |
| Energy drinks | 7 | 437 | 98.4 | 1.4 | 0.2 | 629 | 80.1 | 12.4 | 7.5 | 628 | 83.9 | 8.4 | 7.6 |
| Vegetables | 7 | 437 | 66.6 | 19.9 | 13.5 | 628 | 45.9 | 32.3 | 21.8 | 627 | 46.3 | 26.3 | 27.4 |
| Fruit | 7 | 432 | 66.2 | 22.7 | 11.1 | 629 | 44.5 | 34.0 | 21.5 | 627 | 42.9 | 28.9 | 28.2 |
| Sweets | 7 | 433 | 70.2 | 21.5 | 8.3 | 629 | 49.4 | 36.1 | 14.5 | 628 | 43.8 | 31.1 | 25.2 |
| pHDI | 3 | 430 | 79.5 | 20.5 | 0 | 625 | 75.8 | 23.5 | 0.6 | 622 | 69.0 | 30.5 | 0.5 |
| nHDI | 3 | 432 | 96.8 | 3.2 | 0.0 | 625 | 92.0 | 7.7 | 0.3 | 623 | 92.3 | 7.7 | 0.0 |
| Active/sedentary lifestyle | |||||||||||||
| Screen time | 6 | 434 | 86.9 | 11.5 | 1.6 | 623 | 64.8 | 24.9 | 10.3 | 625 | 60.0 | 29.9 | 10.1 |
| Physical activity level | 3 | 432 | 86.3 | 13.4 | 0.2 | 622 | 74.8 | 24.6 | 0.6 | 626 | 65.3 | 32.1 | 2.6 |
| Physical activity at school | 3 | 435 | 84.4 | 14.5 | 1.1 | 622 | 74.6 | 24.0 | 1.4 | 627 | 64.6 | 29.8 | 5.6 |
| Physical activity at leisure time | 3 | 432 | 83.8 | 15.3 | 0.9 | 623 | 71.3 | 27.0 | 1.8 | 626 | 59.9 | 37.9 | 2.2 |
| FAS components | |||||||||||||
| How many computers, laptops, or tablets does your family own? | 4 | 433 | 87.1 | 11.5 | 1.4 | 626 | 83.7 | 15.2 | 1.1 | 623 | 75.6 | 20.5 | 3.9 |
| Does your family own a car, van, or truck? | 3 | 433 | 91.9 | 7.6 | 0.5 | 627 | 86.3 | 11.5 | 2.2 | 622 | 83.6 | 13.0 | 3.4 |
| Does your family have a dishwasher? | 2 | 435 | 97.5 | 2.5 | 625 | 95.8 | 4.2 | 622 | 95.5 | 4.5 | |||
| Do you have your own bedroom? | 2 | 435 | 96.1 | 3.9 | 622 | 95.8 | 4.2 | 620 | 92.9 | 7.1 | |||
| How many bathrooms (room with a bath or shower) are in your home? | 4 | 434 | 95.2 | 4.1 | 0.7 | 628 | 90.9 | 7.5 | 1.6 | 624 | 89.4 | 9.9 | 0.6 |
| Does your home have an outdoor space attached (e.g., garden)? | 2 | 432 | 95.1 | 4.9 | 625 | 95.2 | 4.8 | 622 | 95.2 | 4.8 | |||
| BMI-for-age | 3 | 407 | 89.4 | 10.6 | 0.0 | 583 | 90.2 | 9.6 | 0.2 | 585 | 92.1 | 7.7 | 0.2 |
| Variables | Cat. 1 | Children Aged 6–10 Years | Adolescents Aged 11–15 Years | |
|---|---|---|---|---|
| Parent (Test–Retest) | Adolescent (Test–Retest) | Adolescent (Test) & Parent (TestP) | ||
| Sample size | 437 | 630 | 628 | |
| Nutrition knowledge level 2 | 3 | 0.62 | 0.36 | NA |
| Dietary habits | ||||
| Breakfast | 4 | 0.70 | 0.54 | 0.56 |
| Meal at school | 4 | 0.78 | 0.53 | 0.46 |
| Dairy products | 7 | 0.54 | 0.37 | 0.27 |
| Fish | 7 | 0.67 | 0.42 | 0.32 |
| Fast food | 7 | 0.68 | 0.43 | 0.33 |
| Sweetened soft drinks | 7 | 0.56 | 0.39 | 0.28 |
| Fruit or mixed fruit and vegetable juices | 7 | 0.46 | 0.30 | 0.30 |
| Energy drinks | 7 | 0.81 | 0.44 | 0.45 |
| Vegetables | 7 | 0.56 | 0.31 | 0.31 |
| Fruit | 7 | 0.53 | 0.31 | 0.27 |
| Sweets | 7 | 0.59 | 0.36 | 0.27 |
| pHDI | 3 | 0.55 | 0.44 | 0.31 |
| nHDI | 3 | 0.45 | 0.35 | 0.26 |
| Active/sedentary lifestyle | ||||
| Screen time | 6 | 0.72 | 0.46 | 0.35 |
| Physical activity level | 3 | 0.68 | 0.52 | 0.36 |
| Physical activity at school | 3 | 0.69 | 0.54 | 0.40 |
| Physical activity at leisure time | 3 | 0.69 | 0.51 | 0.31 |
| FAS components | ||||
| How many computers, laptops, or tablets does your family own? | 4 | 0.79 | 0.69 | 0.55 |
| Does your family own a car, van, or truck? | 3 | 0.84 | 0.76 | 0.70 |
| Does your family have a dishwasher? | 2 | 0.93 | 0.89 | 0.87 |
| Do you have your own bedroom? | 2 | 0.90 | 0.83 | 0.74 |
| How many bathrooms (room with a bath or shower) are in your home? | 4 | 0.88 | 0.84 | 0.79 |
| Does your home have an outdoor space attached (e.g., garden)? | 2 | 0.85 | 0.85 | 0.84 |
| BMI-for-age | 3 | 0.67 | 0.64 | 0.65 |
| Variables (All in Points) | Range of Points | Children Aged 6–10 Years (n = 437) | Adolescents Aged 11–15 Years (n = 630) | |
|---|---|---|---|---|
| Parent (Test–Retest) | Adolescent (Test–Retest) | Adolescent (Test) & Parent (TestP) | ||
| Nutrition knowledge score 2 | 0–18 | 0.80 | 0.68 | NA |
| pHDI | 0–100 | 0.76 | 0.63 | 0.52 |
| nHDI | 0–100 | 0.83 | 0.68 | 0.53 |
| Screen time score | 0–5 | 0.78 | 0.58 | 0.45 |
| Physical activity score | 0–5 | 0.77 | 0.71 | 0.51 |
| FAS | 0–9 | 0.93 | 0.91 | 0.90 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kowalkowska, J.; Wadolowska, L.; Hamulka, J.; Wojtas, N.; Czlapka-Matyasik, M.; Kozirok, W.; Bronkowska, M.; Sadowska, J.; Naliwajko, S.; Dziaduch, I.; et al. Reproducibility of a Short-Form, Multicomponent Dietary Questionnaire to Assess Food Frequency Consumption, Nutrition Knowledge, and Lifestyle (SF-FFQ4PolishChildren) in Polish Children and Adolescents. Nutrients 2019, 11, 2929. https://doi.org/10.3390/nu11122929
Kowalkowska J, Wadolowska L, Hamulka J, Wojtas N, Czlapka-Matyasik M, Kozirok W, Bronkowska M, Sadowska J, Naliwajko S, Dziaduch I, et al. Reproducibility of a Short-Form, Multicomponent Dietary Questionnaire to Assess Food Frequency Consumption, Nutrition Knowledge, and Lifestyle (SF-FFQ4PolishChildren) in Polish Children and Adolescents. Nutrients. 2019; 11(12):2929. https://doi.org/10.3390/nu11122929
Chicago/Turabian StyleKowalkowska, Joanna, Lidia Wadolowska, Jadwiga Hamulka, Natalia Wojtas, Magdalena Czlapka-Matyasik, Witold Kozirok, Monika Bronkowska, Joanna Sadowska, Sylwia Naliwajko, Izabela Dziaduch, and et al. 2019. "Reproducibility of a Short-Form, Multicomponent Dietary Questionnaire to Assess Food Frequency Consumption, Nutrition Knowledge, and Lifestyle (SF-FFQ4PolishChildren) in Polish Children and Adolescents" Nutrients 11, no. 12: 2929. https://doi.org/10.3390/nu11122929