Association between Dietary Intake and Lipid-Lowering Therapy: Prospective Analysis of Data from Australian Diabetes, Obesity, and Lifestyle Study (AusDiab) Using a Quantile Regression Approach

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Outcome Measures
2.3. Covariates
2.4. Statistical Analysis
3. Results
3.1. Participant Characteristics
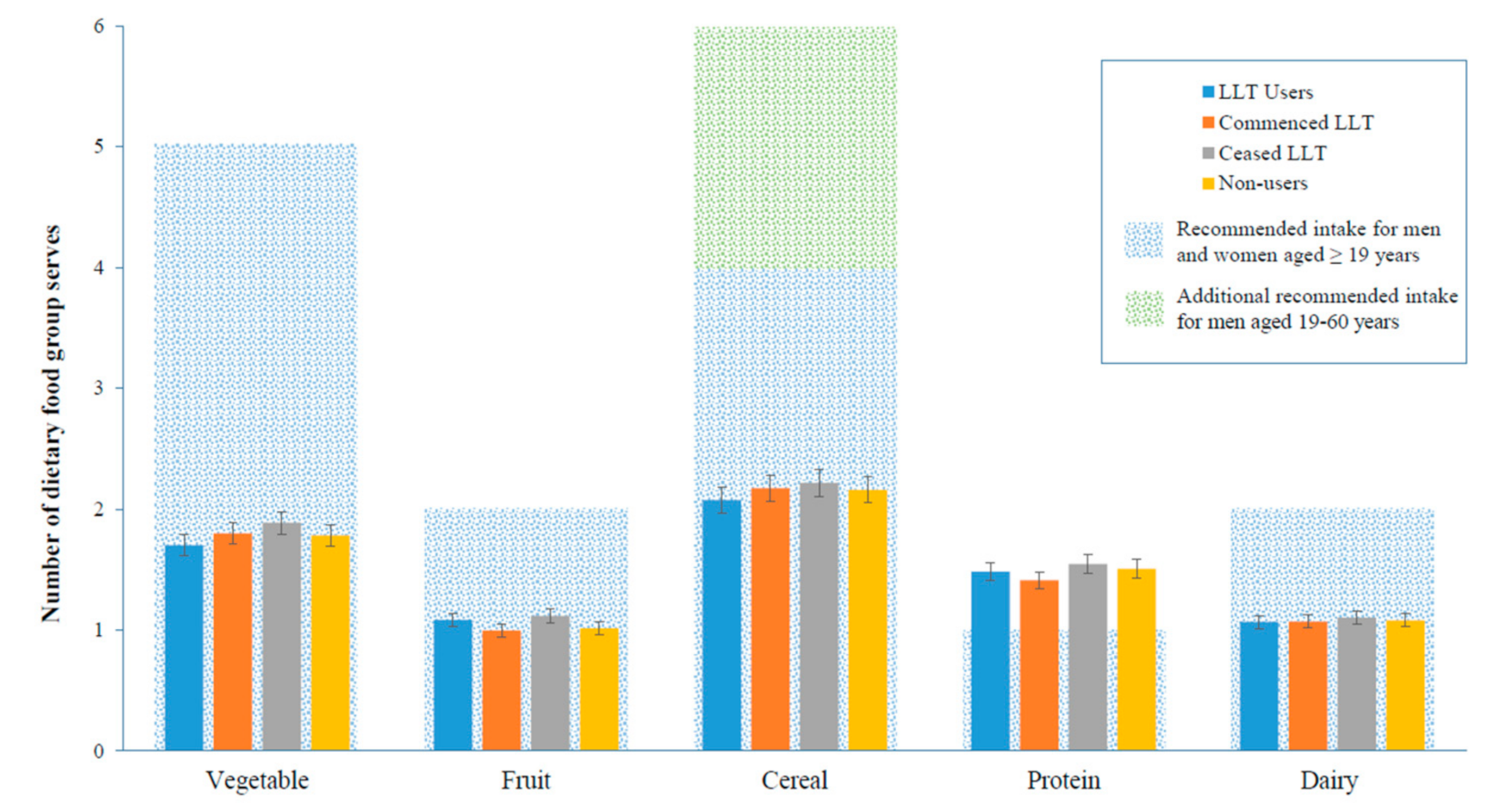
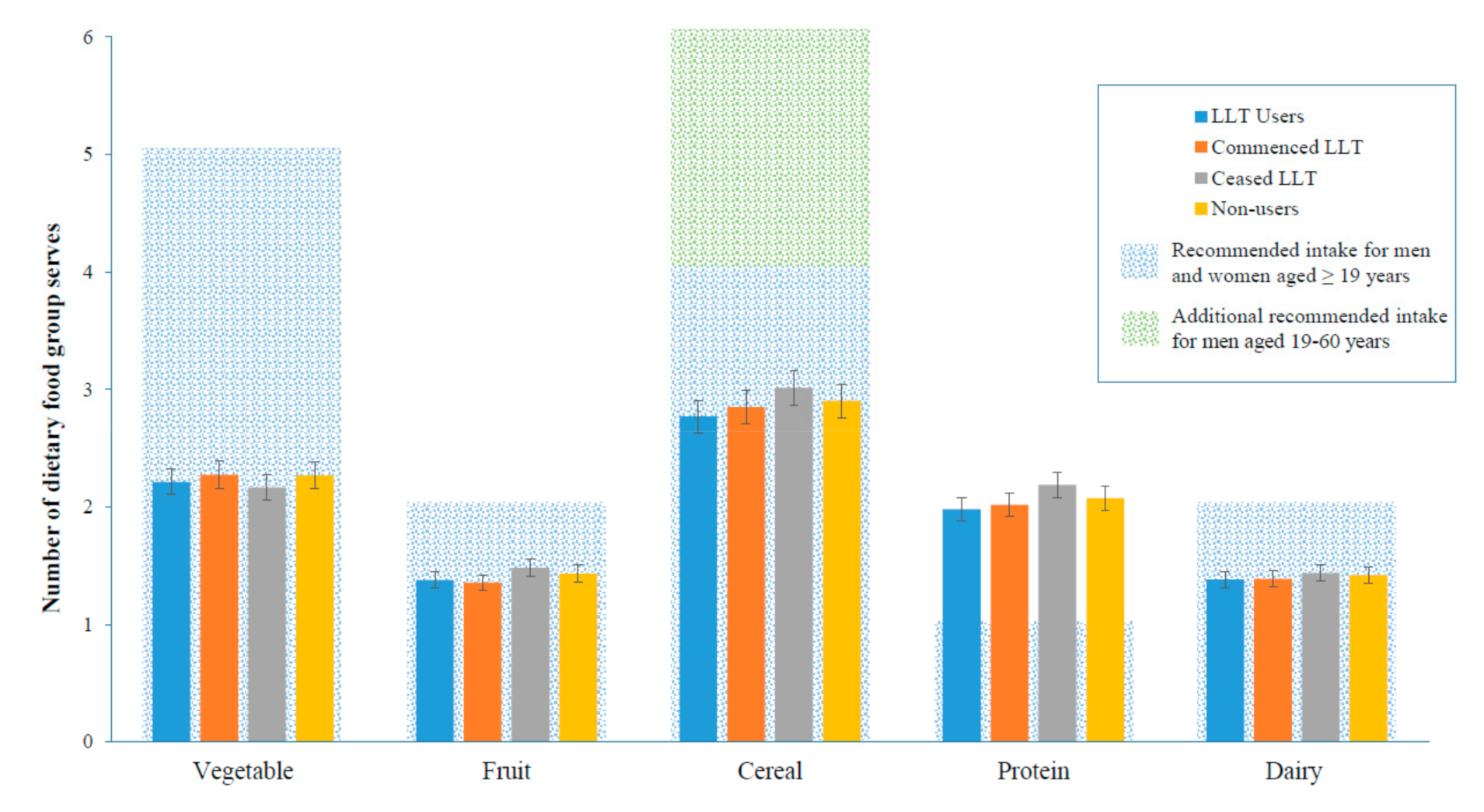
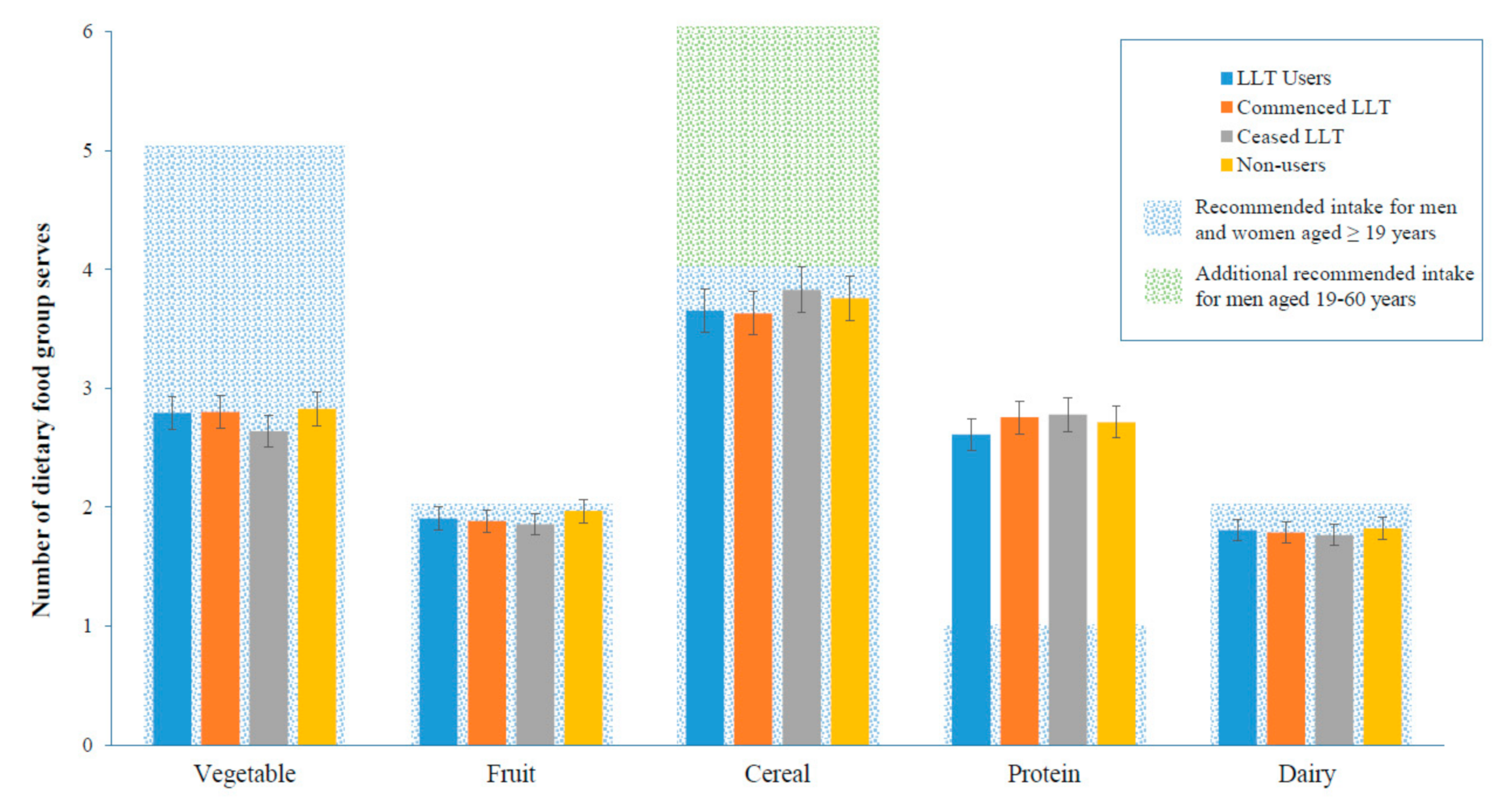
3.2. Dietary Intake
3.3. Quantile Regression
3.4. Subgroup Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Abubakar, I.; Tillmann, T.; Banerjee, A. Global, regional, and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, 1990–2013: A systematic analysis for the global burden of disease study 2013. Lancet 2015, 385, 117–171. [Google Scholar]
- American Heart Association. Cardiovascular Disease: A Costly Burden for America Projections through 2035; American Heart Association: Washington, DC, USA, 2017. [Google Scholar]
- Yusuf, S.; Reddy, S.; Ôunpuu, S.; Anand, S. Global burden of cardiovascular diseases: Part I: General considerations, the epidemiologic transition, risk factors, and impact of urbanization. Circulation 2001, 104, 2746–2753. [Google Scholar] [CrossRef] [PubMed]
- Megson, I.L.; Whitfield, P.D.; Zabetakis, I. Lipids and cardiovascular disease: Where does dietary intervention sit alongside statin therapy? Food Funct. 2016, 7, 2603–2614. [Google Scholar] [CrossRef] [PubMed]
- Poli, A.; Visioli, F. Pharmacology of nutraceuticals with lipid lowering properties. High Blood Press. Cardiovasc. Prev. 2019, 26, 113–118. [Google Scholar] [CrossRef] [PubMed]
- Cicero, A.F.; Colletti, A.; Bajraktari, G.; Descamps, O.; Djuric, D.M.; Ezhov, M.; Fras, Z.; Katsiki, N.; Langlois, M.; Latkovskis, G. Lipid-lowering nutraceuticals in clinical practice: Position paper from an international lipid expert panel. Nutr. Rev. 2017, 75, 731–767. [Google Scholar] [CrossRef] [PubMed]
- Hamilton-Craig, I.R. Prescribing statins: The real issues. Med. J. Aust. 2014, 200, 440–441. [Google Scholar] [CrossRef]
- Simons, L.A.; Levis, G.; Simons, J. Apparent discontinuation rates in patients prescribed lipid-lowering drugs. Med. J. Aust. 1996, 164, 208–211. [Google Scholar] [CrossRef]
- Ellis, J.J.; Erickson, S.R.; Stevenson, J.G.; Bernstein, S.J.; Stiles, R.A.; Fendrick, A.M. Suboptimal statin adherence and discontinuation in primary and secondary prevention populations. J. Gen. Intern. Med. 2004, 19, 638–645. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deambrosis, P.; Saramin, C.; Terrazzani, G.; Scaldaferri, L.; Debetto, P.; Giusti, P.; Chinellato, A. Evaluation of the prescription and utilization patterns of statins in an italian local health unit during the period 1994–2003. Eur. J. Clin. Pharmacol. 2007, 63, 197–203. [Google Scholar] [CrossRef]
- Vinker, S.; Shani, M.; Baevsky, T.; Elhayany, A. Adherence with statins over 8 years in a usual care setting. Am. J. Manag. Care 2008, 14, 388–392. [Google Scholar]
- Ofori-Asenso, R.; Jakhu, A.; Zomer, E.; Curtis, A.J.; Korhonen, M.J.; Nelson, M.; Gambhir, M.; Tonkin, A.; Liew, D.; Zoungas, S. Adherence and persistence among statin users aged 65 years and over: A systematic review and meta-analysis. J. Gerontol. A Biol. Sci. Med. Sci. 2017, 73, 813–819. [Google Scholar] [CrossRef]
- Hu, F.B.; Rimm, E.B.; Stampfer, M.J.; Ascherio, A.; Spiegelman, D.; Willett, W.C. Prospective study of major dietary patterns and risk of coronary heart disease in men. Am. J. Clin. Nutr. 2000, 72, 912–921. [Google Scholar] [CrossRef] [PubMed]
- Jacques, P.F.; Tucker, K.L. Are dietary patterns useful for understanding the role of diet in chronic disease? Am. J. Clin. Nutr. 2001, 73, 1–2. [Google Scholar] [CrossRef] [Green Version]
- Panagiotakos, D.B.; Georgousopoulou, E.N.; Georgiopoulos, G.A.; Pitsavos, C.; Chrysohoou, C.; Skoumas, I.; Ntertimani, M.; Laskaris, A.; Papadimitriou, L.; Tousoulis, D. Adherence to mediterranean diet offers an additive protection over the use of statin therapy: Results from the attica study (2002–2012). Curr. Vasc. Pharmacol. 2015, 13, 778–787. [Google Scholar] [CrossRef]
- Wang, H.; Blumberg, J.B.; Chen, C.Y.O.; Choi, S.W.; Corcoran, M.P.; Harris, S.S.; Jacques, P.F.; Kristo, A.S.; Lai, C.Q.; Lamon-Fava, S. Dietary modulators of statin efficacy in cardiovascular disease and cognition. Mol. Asp. Med. 2014, 38, 1–53. [Google Scholar] [CrossRef] [PubMed]
- Sugiyama, T.; Tsugawa, Y.; Tseng, C.H.; Kobayashi, Y.; Shapiro, M.F. Is there gluttony in the time of statins? Different time trends of caloric and fat intake between statin-users and non-users among us adults. JAMA Intern. Med. 2014, 174, 1038–1045. [Google Scholar] [CrossRef] [PubMed]
- Barter, P.; Best, J.; Boyden, A.; Cooper, C.; Gillam, I.; Mansfield, P. Lipid management guidelines—2001. Med. J. Aust. 2001, 175, 57–85. [Google Scholar]
- Barnard, R.J.; DiLauro, S.C.; Inkeles, S.B. Effects of intensive diet and exercise intervention in patients taking cholesterol-lowering drugs. Am. J. Cardiol. 1997, 79, 1112–1114. [Google Scholar] [CrossRef]
- National Health and Medical Research Council. Dietary Guidelines for Australian Adults; Australian Government Printing Service: Canberra, Australia, 2003.
- National Health and Medical Research Council. Dietary Guidelines for Older Australians; Commonwealth of Australia: Canberra, Australia, 1999. Available online: http://www.nhmrc.gov.au/publications/synopses/n23syn.htm (accessed on 24 May 2019).
- Australian Institute of Health and Welfare 2014. Australia’s Health 2014; Australia’s Health Series No. 14. Cat. No. AUS 178; AIHW: Canberra, Australia, 2014.
- Australian Bureau of Statistics. Australian Health Survey: First Results, 2011–2012; Australian Bureau of Statistics: Canberra, Australia, 2012.
- Dunstan, D.W.; Zimmet, P.Z.; Welborn, T.A.; Cameron, A.J.; Shaw, J.; De Courten, M.; Jolley, D.; McCarty, D.J.; Committee, A.S. The Australian Diabetes, Obesity and Lifestyle Study (AusDiab)—Methods and response rates. Diabetes Res. Clin. Pract. 2002, 57, 119–129. [Google Scholar] [CrossRef]
- Australian Institute of Health and Welfare. The Active Australia Survey: A Guide and Manual for Implementation, Analysis and Reporting; Australian Institute of Health and Welfare: Canberra, Australia, 2003.
- Subar, A.F.; Thompson, F.E.; Kipnis, V.; Midthune, D.; Hurwitz, P.; McNutt, S.; McIntosh, A.; Rosenfeld, S. Comparative validation of the block, willett, and national cancer institute food frequency questionnaires: The eating at America’s table study. Am. J. Epidemiol. 2001, 154, 1089–1099. [Google Scholar] [CrossRef]
- Koenker, R.; Bassett, G., Jr. Regression quantiles. Econometrica 1978, 46, 33–50. [Google Scholar] [CrossRef]
- Lofgren, I.; Greene, G.; Schembre, S.; Delmonico, M.J.; Riebe, D.; Clark, P. Comparison of diet quality, physical activity and biochemical values of older adults either reporting or not reporting use of lipid-lowering medication. J. Nutr. Health Aging 2010, 14, 168–172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johal, S.; Jamsen, K.M.; Bell, J.S.; Mc Namara, K.P.; Magliano, D.J.; Liew, D.; Ryan-Atwood, T.E.; Anderson, C.; Ilomäki, J. Do statin users adhere to a healthy diet and lifestyle? The Australian diabetes, obesity and lifestyle study. Eur. J. Prev. Cardiol. 2017, 24, 621–627. [Google Scholar] [CrossRef] [PubMed]
- Lytsy, P.; Burell, G.; Westerling, R. Cardiovascular risk factor assessments and health behaviours in patients using statins compared to a non-treated population. Int. J. Behav. Med. 2012, 19, 134–142. [Google Scholar] [CrossRef] [PubMed]
- Van Horn, L.; McCoin, M.; Kris-Etherton, P.M.; Burke, F.; Carson, J.A.S.; Champagne, C.M.; Karmally, W.; Sikand, G. The evidence for dietary prevention and treatment of cardiovascular disease. J. Am. Diet. Assoc. 2008, 108, 287–331. [Google Scholar] [CrossRef] [PubMed]
- Blumenthal, J.A.; Babyak, M.A.; Hinderliter, A.; Watkins, L.L.; Craighead, L.; Lin, P.H.; Caccia, C.; Johnson, J.; Waugh, R.; Sherwood, A. Effects of the dash diet alone and in combination with exercise and weight loss on blood pressure and cardiovascular biomarkers in men and women with high blood pressure: The encore study. Arch. Intern. Med. 2010, 170, 126–135. [Google Scholar] [CrossRef]
- Liu, L.; Ikeda, K.; Sullivan, D.H.; Ling, W.; Yamori, Y. Epidemiological evidence of the association between dietary protein intake and blood pressure: A meta-analysis of published data. Hypertens. Res. 2002, 25, 689–695. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.M.; Ho, S.C.; Chen, Y.M.; Woo, J. Effect of soy protein and isoflavones on blood pressure and endothelial cytokines: A 6-month randomized controlled trial among postmenopausal women. J. Hypertens. 2013, 31, 384–392. [Google Scholar] [CrossRef]
- Turpeinen, O. Effect of cholesterol-lowering diet on mortality from coronary heart disease and other causes. Circulation 1979, 59, 1–7. [Google Scholar] [CrossRef]
- Guo, J.; Astrup, A.; Lovegrove, J.A.; Gijsbers, L.; Givens, D.I.; Soedamah-Muthu, S.S. Milk and dairy consumption and risk of cardiovascular diseases and all-cause mortality: Dose–response meta-analysis of prospective cohort studies. Eur. J. Epidemiol. 2017, 32, 269–287. [Google Scholar] [CrossRef]
- Goldbohm, R.A.; Chorus, A.M.; Galindo Garre, F.; Schouten, L.J.; van den Brandt, P.A. Dairy consumption and 10-y total and cardiovascular mortality: A prospective cohort study in the Netherlands. Am. J. Clin. Nutr. 2011, 93, 615–627. [Google Scholar] [CrossRef]
- Alexander, D.D.; Bylsma, L.C.; Vargas, A.J.; Cohen, S.S.; Doucette, A.; Mohamed, M.; Irvin, S.R.; Miller, P.E.; Watson, H.; Fryzek, J.P. Dairy consumption and CVD: A systematic review and meta-analysis. Br. J. Nutr. 2016, 115, 737–750. [Google Scholar] [CrossRef]
- McAleer, S.; Cupples, M.; Neville, C.; McKinley, M.; Woodside, J.; Tully, M. Statin prescription initiation and lifestyle behaviour: A primary care cohort study. BMC Fam. Pract. 2016, 17, 77. [Google Scholar] [CrossRef]
- Buttar, H.S.; Li, T.; Ravi, N. Prevention of cardiovascular diseases: Role of exercise, dietary interventions, obesity and smoking cessation. Exp. Clin. Cardiol. 2005, 10, 229–249. [Google Scholar]
- Hebert, J.R.; Ma, Y.; Clemow, L.; Ockene, I.S.; Saperia, G.; Stanek, E.J., III; Merriam, P.A.; Ockene, J.K. Gender differences in social desirability and social approval bias in dietary self-report. Am. J. Epidemiol. 1997, 146, 1046–1055. [Google Scholar] [CrossRef]
- Reeves, R.S.; Foreyt, J.P.; Scott, L.W.; Mitchell, R.E.; Wohlleb, J.; Gotto, A., Jr. Effects of a low cholesterol eating plan on plasma lipids: Results of a three-year community study. Am. J. Public Health 1983, 73, 873–877. [Google Scholar] [CrossRef]
- Jula, A.; Marniemi, J.; Huupponen, R.; Virtanen, A.; Rastas, M.; Rönnemaa, T. Effects of diet and simvastatin on serum lipids, insulin, and antioxidants in hypercholesterolemic men: A randomized controlled trial. JAMA 2002, 287, 598–605. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | LLT Users (n = 446) | Commenced LLT (n = 565) | Ceased LLT (n = 71) | Non-Users (n = 4813) | p Value |
|---|---|---|---|---|---|
| Age, mean (SD) | 62.54 (9.29) a | 57.92 (10.20) bc | 61.72 (11.0) ac | 49.67 (12.34) d | <0.01 |
| Sex, n (%) | |||||
| Male | 233 (52.2) a | 313 (50.4) b | 33 (46.5) abc | 2113 (43.9) c | <0.01 |
| Education, n (%) | |||||
| Higher than secondary level education | 131 (29.4) a | 195 (34.5) b | 21 (29.6) c | 2073 (43.1) d | <0.01 |
| BMI kg/m2, mean (SD) | 28.46 (4.73) a | 28.03 (4.75) a | 28.46 (4.67) a | 26.56 (4.76) b | <0.01 |
| Diabetes, n (%) | |||||
| Yes | 227 (50.9) a | 219 (38.8) b | 32 (45.1) abc | 987 (20.5) d | <0.01 |
| Prior CVD, n (%) | |||||
| Yes | 156 (35.0) a | 66 (11.7) b | 18 (25.4) ac | 163 (3.4) d | <0.01 |
| Hypertension, n (%) | |||||
| Hypertensive | 286 (64.1) a | 306 (54.2) b | 43 (60.6) abc | 1198 (24.9) d | <0.01 |
| Smoking status, n (%) | |||||
| Never smoker | 227 (52.0) a | 299 (53.4) b | 44 (62.9) c | 2863 (60.3) c | <0.01 |
| Former smoker | 165 (37.8) | 200 (35.7) | 18 (25.7) | 1353 (28.5) | |
| Current smoker | 45 (10.3) | 61 (10.9) | 8 (11.4) | 533 (11.2) | |
| Physical activity, n (%) | |||||
| Sedentary | 73 (16.4) | 97 (17.2) | 15 (21.1) | 733 (15.3) | 0.675 |
| Insufficient | 133 (29.9) | 172 (30.5) | 23 (32.4) | 1474 (30.7) | |
| Sufficient | 239 (53.7) | 295 (50.3) | 33 (46.5) | 2596 (54.1) | |
| Energy intake, kJ/day | |||||
| 7430.70 (2483.87) a | 7838.61 (2548.32) b | 7351.24 (2618.71) b | 8018.08 (2735.2) c | 0.01 | |
| Saturated fat as proportion energy intake, % (SD) | |||||
| 12.60 (3.23) a | 13.75 (3.41) ab | 13.07 (3.30) ab | 14.48 (3.44) c | <0.01 | |
| LLT Users (n = 446) | Commenced LLT (n = 565) | Ceased LLT (n = 71) | Non LLT Users (n = 4813) | p Value | |
|---|---|---|---|---|---|
| Proportion meeting guidelines at baseline, n (%) | |||||
| All food groups | 2 (0.45) | 1 (0.18) | 0 (0.00) | 7 (0.15) | 0.506 |
| Vegetables | 13 (2.91) | 15 (2.65) | 2 (2.82) | 115 (2.39) | 0.894 |
| Fruit | 126 (28.25) | 160 (28.32) | 19 (26.76) | 1249 (25.95) | 0.501 |
| Cereal | 109 (24.44) | 117 (20.71) | 14 (19.72) | 902 (18.74) | 0.027 |
| Protein | 365 (81.84) a | 474 (83.89) ab | 63 (88.73) ab | 4221 (87.70) b | 0.001 |
| Dairy | 90 (20.18) | 109 (19.29) | 14 (19.72) | 1009 (20.96) | 0.802 |
| Proportion meeting guidelines at year 5, n (%) | |||||
| All food groups | 1 (0.23) | 0 (0.00) | 0 (0.00) | 3 (0.06) | 0.560 |
| Vegetable | 6 (1.36) | 10 (1.79) | 1 (1.45) | 95 (2.00) | 0.797 |
| Fruit | 116 (26.30) | 148 (26.48) | 20 (28.99) | 1354 (28.49) | 0.613 |
| Cereal | 75 (17.01) | 74 (13.24) | 6 (8.70) | 668 (14.05) | 0.166 |
| Protein | 360 (81.63) a | 468 (83.72) ab | 61 (88.41) ab | 4161 (87.54) b | 0.001 |
| Dairy | 85 (19.27) | 103 (18.43) | 12 (17.39) | 949 (19.97) | 0.786 |
| Food Group | LLT Users (n = 446) | Commenced LLT (n = 565) | Ceased LLT (n = 71) | Non LLT Users (n = 4813) |
|---|---|---|---|---|
| Vegetable | 2.21 (2.11, 2.31) | 2.27 (2.20, 2.35) | 2.16 (2.03, 2.30) | 2.27 (2.24, 2.30) |
| Fruit | 1.38 (1.31, 1.45) | 1.35 (1.28, 1.42) | 1.48 (1.34, 1.62) | 1.43 (1.41, 1.46) |
| Cereal | 2.77 (2.63, 2.91) | 2.85 (2.74, 2.96) | 3.01 (2.77, 3.26) | 2.90 (2.86, 2.95) |
| Protein | 1.98 (1.88, 2.08) | 2.02 (1.93, 2.11) | 2.19 (1.96, 2.42) | 2.08 (2.04, 2.11) |
| Dairy | 1.38 (1.31, 1.46) | 1.39 (1.33, 1.44) | 1.44 (1.27, 1.60) | 1.42 (1.40, 1.44) |
| Food Group | LLT Users (n = 446) | Non-Users (Ref.) | Commenced LLT (n = 565) | Non-Users (Ref.) |
|---|---|---|---|---|
| Vegetable | −0.09 (−0.20, 0.02) | −0.0001 (−0.08, 0.08) | ||
| Fruit | −0.04 (−0.12, 0.04) | −0.07 (−0.14, 0.001) | ||
| Cereal | −0.13 (−0.28, 0.02) | −0.07 (−0.19, 0.05) | ||
| Protein | −0.09 (−0.21, 0.03) | −0.06 (−0.15, 0.04) | ||
| Dairy | −0.03 (−0.11, 0.04) | −0.03 (−0.09, 0.03) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gadowski, A.M.; Nanayakkara, N.; Heritier, S.; Magliano, D.J.; Shaw, J.E.; Curtis, A.J.; Zoungas, S.; Owen, A.J. Association between Dietary Intake and Lipid-Lowering Therapy: Prospective Analysis of Data from Australian Diabetes, Obesity, and Lifestyle Study (AusDiab) Using a Quantile Regression Approach. Nutrients 2019, 11, 1858. https://doi.org/10.3390/nu11081858
Gadowski AM, Nanayakkara N, Heritier S, Magliano DJ, Shaw JE, Curtis AJ, Zoungas S, Owen AJ. Association between Dietary Intake and Lipid-Lowering Therapy: Prospective Analysis of Data from Australian Diabetes, Obesity, and Lifestyle Study (AusDiab) Using a Quantile Regression Approach. Nutrients. 2019; 11(8):1858. https://doi.org/10.3390/nu11081858
Chicago/Turabian StyleGadowski, Adelle M., Natalie Nanayakkara, Stephane Heritier, Dianna J. Magliano, Jonathan E. Shaw, Andrea J. Curtis, Sophia Zoungas, and Alice J. Owen. 2019. "Association between Dietary Intake and Lipid-Lowering Therapy: Prospective Analysis of Data from Australian Diabetes, Obesity, and Lifestyle Study (AusDiab) Using a Quantile Regression Approach" Nutrients 11, no. 8: 1858. https://doi.org/10.3390/nu11081858