Nutrition, Hygiene and Stimulation Education for Impoverished Mothers in Rural Uganda: Effect on Maternal Depression Symptoms and Their Associations to Child Development Outcomes

Abstract
:1. Introduction
2. Materials and Methods
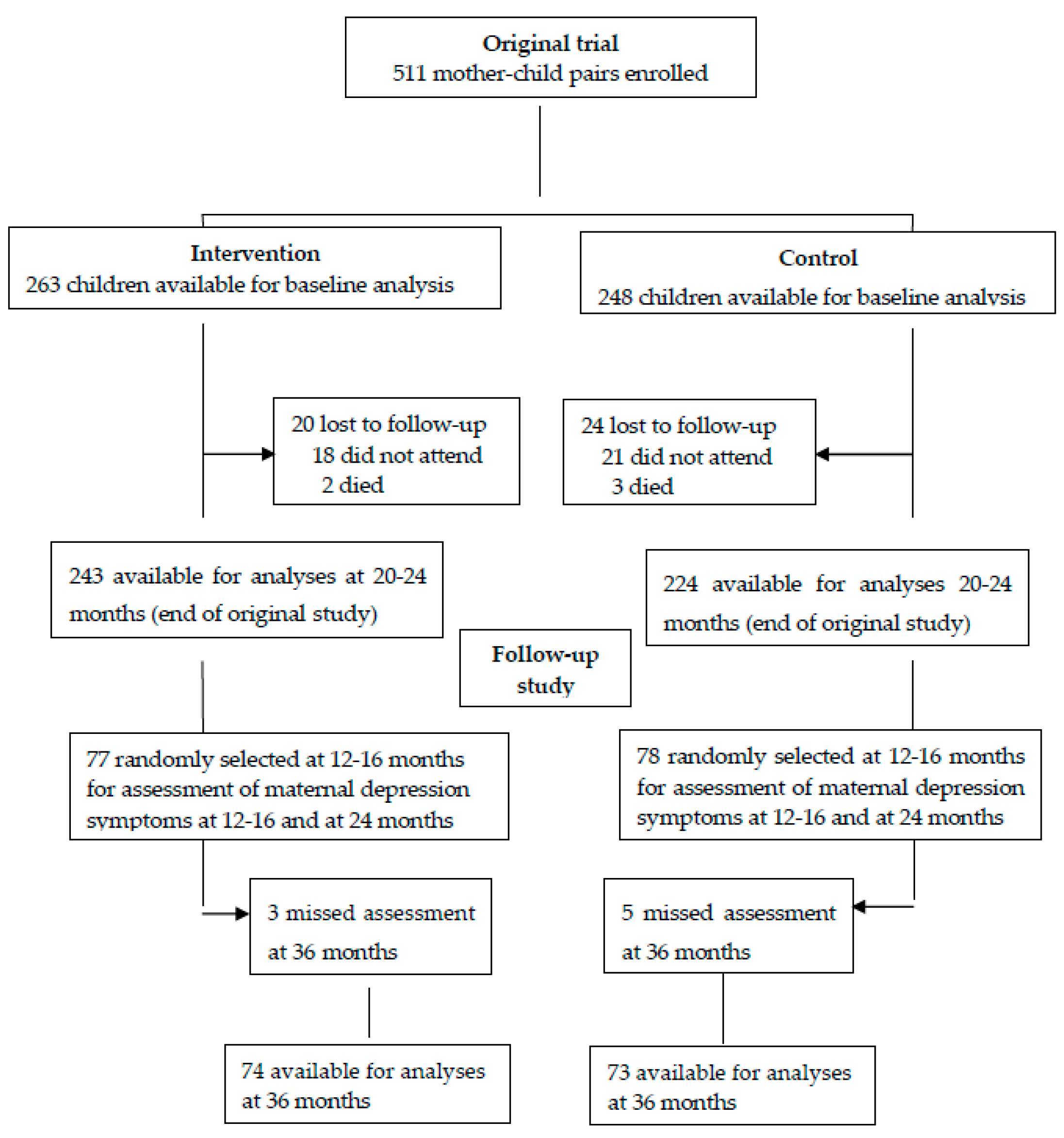
2.1. Participants and Approvals
2.2. Randomisation of the Parental and follow-up Participants
2.3. The Intervention in the Parental Trial
2.4. Outcomes
2.5. Statistical Analysis
3. Results
3.1. Characteristics of the Participants
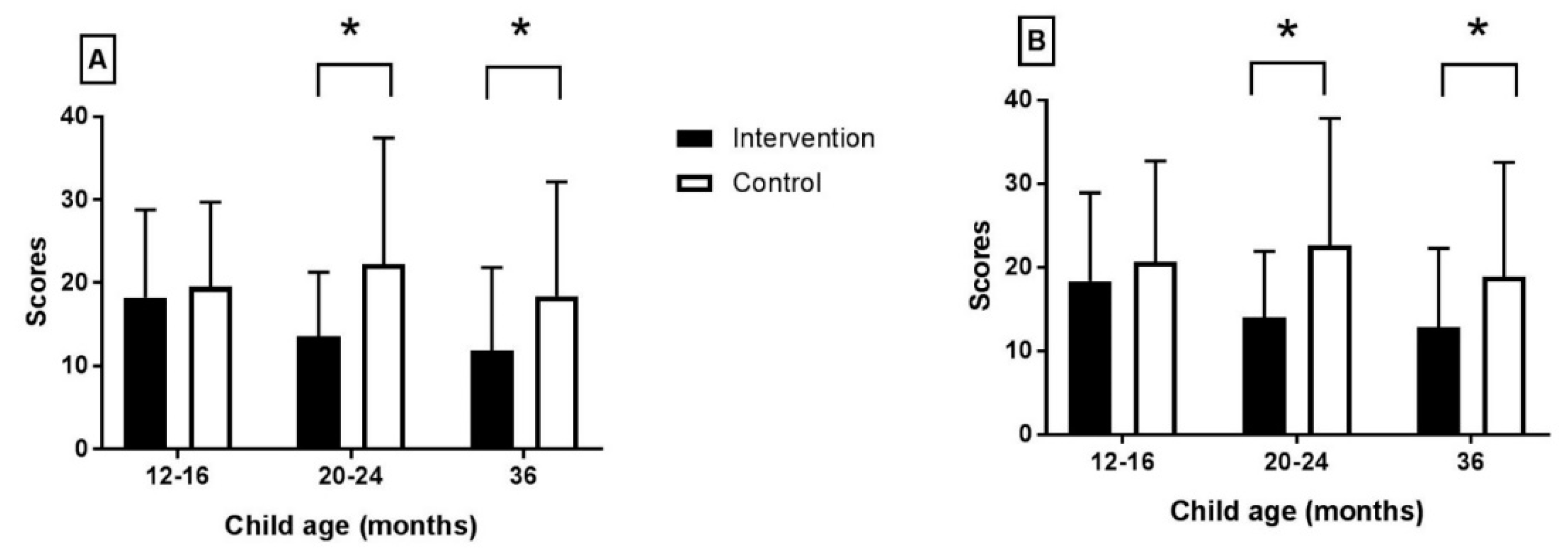
3.2. Effect of the Intervention on Maternal Depression Symptoms
3.3. Associations between Maternal Depression Symptoms and Child Development Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Perez-Escamilla, R.; Moran, V.H. The role of nutrition in integrated early child development in the 21st century: Contribution from the Maternal and Child Nutrition journal. Matern. Child Nutr. 2017, 13, 3–6. [Google Scholar] [CrossRef] [PubMed]
- PAHO/WHO. Guiding Priciples for Complementary Feeding of the Breastfed Child; Division of Health Promotion and Protection; World Health Organization: Washington, DC, USA, 2003. [Google Scholar]
- Vissers, K.M.; Feskens, E.J.M.; van Goudoever, J.B.; Janse, A.J. The timing of initiating complementary feeding in preterm infants and its effect on overweight: A systematic review. Ann. Nutr. Metab. 2018, 72, 307–315. [Google Scholar] [CrossRef] [PubMed]
- Smith Fawzi, M.C.; Andrews, K.G.; Fink, G.; Danaei, G.; McCoy, D.C.; Sudfeld, C.R.; Peet, E.D.; Cho, J.; Liu, Y.; Finlay, J.E.; et al. Lifetime economic impact of the burden of childhood stunting attributable to maternal psychosocial risk factors in 137 low/middle-income countries. BMJ Glob. Health 2019, 4, e001144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stellenberg, E.L.; Abrahams, J.M. Prevalence of and factors influencing postnatal depression in a rural community in South Africa. Afr. J. Prim. Health Care Fam. Med. 2015, 7, 874. [Google Scholar] [CrossRef] [PubMed]
- January, J.; Chimbari, M.J. Prevalence and factors associated with postnatal depression among women in two rural districts of Manicaland, Zimbabwe. South Jersey Psychol. 2018, 24, 1176. [Google Scholar] [CrossRef] [PubMed]
- Payne, J.L.; Maguire, J. Pathophysiological mechanisms implicated in postpartum depression. Front. Neuroendocrinol. 2019, 52, 165–180. [Google Scholar] [CrossRef]
- Garber, J.; Goodman, S.H.; Brunwasser, S.M.; Frankel, S.A.; Herrington, C.G. The effect of content and tone of maternal evaluative feedback on self-cognitions and affect in young children. J. Exp. Child Psychol. 2019, 182, 151–165. [Google Scholar] [CrossRef]
- Howard, L.M.; Challacombe, F. Effective treatment of postnatal depression is associated with normal child development. Lancet Psychol. 2018, 5, 95–97. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Dix, T. Mothers’ early depressive symptoms predict children’s low social competence in first grade: Mediation by children’s social cognition. J. Child Psychol. Psychiatry Allied Discip. 2015, 56, 183–192. [Google Scholar] [CrossRef]
- Nuttall, A.K.; Froyen, L.C.; Skibbe, L.E.; Bowles, R.P. Maternal and paternal depressive symptoms, home learning environment, and children’s early literacy. Child Psychiatry Hum. Dev. 2019, in press. [Google Scholar] [CrossRef]
- Conners-Burrow, N.A.; Bokony, P.; Whiteside-Mansell, L.; Jarrett, D.; Kraleti, S.; McKelvey, L.; Kayzer, A. Low-level depressive symptoms reduce maternal support for child cognitive development. J. Pediatr. Health Care 2014, 28, 404–412. [Google Scholar] [CrossRef] [PubMed]
- Patel, V.; Saxena, S.; Lund, C.; Thornicroft, G.; Baingana, F.; Bolton, P.; Chisholm, D.; Collins, P.Y.; Cooper, J.L.; Eaton, J.; et al. The Lancet Commission on global mental health and sustainable development. Lancet 2018, 392, 1553–1598. [Google Scholar] [CrossRef] [Green Version]
- Muhoozi, G.K.M.; Atukunda, P.; Diep, L.M.; Mwadime, R.; Kaaya, A.N.; Skaare, A.B.; Willumsen, T.; Westerberg, A.C.; Iversen, P.O. Nutrition, hygiene, and stimulation education to improve growth, cognitive, language, and motor development among infants in Uganda: A cluster-randomized trial. Matern. Child Nutr. 2018, 14, e12527. [Google Scholar] [CrossRef] [PubMed]
- Forsyth, D.R. Group Dynamics, 6th ed.; Wadsworth Publishing Cengage learning: Belmont, CA, USA, 2014. [Google Scholar]
- Paulus, P.B.; Poletes, G.; Camacho, L.M. Perception of performance in group brainstorming: The illusion of group productivity. Personal. Soc. Psychol. Bull. 1993, 19, 78–89. [Google Scholar]
- Atukunda, P.; Muhoozi, G.K.M.; van den Broek, T.J.; Kort, R.; Diep, L.M.; Kaaya, A.N.; Iversen, P.O.; Westerberg, A.C. Child development, growth and microbiota: Follow-up of a randomized education trial in Uganda. J. Glob. Health 2019, 9, 010431. [Google Scholar] [CrossRef] [PubMed]
- Bandura, A. Social cognitive theory: An agentic perspective. Ann. Rev. Psychol. 2001, 52, 1–26. [Google Scholar] [CrossRef] [PubMed]
- Ovuga, E.; Boardman, J.; Wasserman, D. Undergraduate student mental health at Makerere University, Uganda. World Psychiatry 2006, 5, 51–52. [Google Scholar] [PubMed]
- Lewinsohn, P.M.; Seeley, J.R.; Roberts, R.E.; Allen, N.B. Center for Epidemiologic Studies Depression Scale (CES-D) as a screening instrument for depression among community-residing older adults. Psychol. Aging 1997, 12, 277–287. [Google Scholar] [CrossRef]
- Ovuga, E.; Boardman, J.; Wasserman, D. The prevalence of depression in two districts of Uganda. Soc. Psychiatry Psychiatr. Epidemiol. 2005, 40, 439–445. [Google Scholar] [CrossRef]
- Natamba, B.K.; Achan, J.; Arbach, A.; Oyok, T.O.; Ghosh, S.; Mehta, S.; Stoltzfus, R.J.; Griffiths, J.K.; Young, S.L. Reliability and validity of the center for epidemiologic studies-depression scale in screening for depression among HIV-infected and -uninfected pregnant women attending antenatal services in northern Uganda: A cross-sectional study. BMC Psychiatry 2014, 14, 303. [Google Scholar] [CrossRef]
- Pietikainen, J.T.; Polo-Kantola, P.; Polkki, P.; Saarenpaa-Heikkila, O.; Paunio, T.; Paavonen, E.J. Sleeping problems during pregnancy-a risk factor for postnatal depressiveness. Arch. Womens Ment. Health 2019, 22, 327–337. [Google Scholar] [CrossRef] [PubMed]
- Singla, D.R.; Kumbakumba, E.; Aboud, F.E. Effects of a parenting intervention to address maternal psychological wellbeing and child development and growth in rural Uganda: A community-based, cluster randomised trial. Lancet Glob. Health 2015, 3, e458–e469. [Google Scholar] [CrossRef]
- Van der Heijden, I.; Abrahams, N.; Sinclair, D. Psychosocial group interventions to improve psychological well-being in adults living with HIV. Cochrane Database Syst. Rev. 2017, 3, Cd010806. [Google Scholar] [CrossRef] [PubMed]
- Campbell, M.J.; Donner, A.; Klar, N. Developments in cluster randomized trials and Statistics in Medicine. Stat. Med. 2007, 26, 2–19. [Google Scholar] [CrossRef] [PubMed]
- Arikpo, D.; Edet, E.S.; Chibuzor, M.T.; Odey, F.; Caldwell, D.M. Educational interventions for improving primary caregiver complementary feeding practices for children aged 24 months and under. Cochrane Database Syst. Rev. 2018, 18, CD011768. [Google Scholar] [CrossRef] [PubMed]
- Baker-Henningham, H.; Powell, C.; Walker, S.; Grantham-McGregor, S. The effect of early stimulation on maternal depression: A cluster randomised controlled trial. Arch. Dis. Child 2005, 90, 1230–1234. [Google Scholar] [CrossRef]
- Miklush, L.; Connelly, C.D. Maternal depression and infant development: Theory and current evidence. Am. J. Matern. Child Nurs. 2013, 38, 369–374. [Google Scholar] [CrossRef]
- Aoyagi, S.S.; Takei, N.; Nishimura, T.; Nomura, Y.; Tsuchiya, K.J. Association of late-onset postpartum depression of mothers with expressive language development during infancy and early childhood: The HBC study. PeerJ 2019, 7, e6566. [Google Scholar] [CrossRef]
- Milgrom, J.; Holt, C.J.; Bleker, L.S.; Holt, C.; Ross, J.; Ericksen, J.; Glover, V.; O’Donnell, K.J.; de Rooij, S.R.; Gemmill, A.W. Maternal antenatal mood and child development: An exploratory study of treatment effects on child outcomes up to 5 years. J. Dev. Orig. Health Dis. 2018, 10, 221–231. [Google Scholar] [CrossRef]
- Liu, Y.; Kaaya, S.; Chai, J.; McCoy, D.C.; Surkan, P.J.; Black, M.M.; Sutter-Dallay, A.L.; Verdoux, H.; Smith-Fawzi, M.C. Maternal depressive symptoms and early childhood cognitive development: A meta-analysis. Psychol. Med. 2017, 47, 680–689. [Google Scholar] [CrossRef]
- Ahun, M.N.; Cote, S.M. Maternal depressive symptoms and early childhood cognitive development: A review of putative environmental mediators. Arch. Womens Ment. Health 2019, 22, 15–24. [Google Scholar] [CrossRef] [PubMed]
- Ahun, M.N.; Geoffroy, M.C.; Herba, C.M.; Brendgen, M.; Seguin, J.R.; Sutter-Dallay, A.L.; Boivin, M.; Tremblay, R.E.; Côté, S.M. Timing and chronicity of maternal depression symptoms and children’s verbal abilities. J. Pediatr. 2017, 190, 251–257. [Google Scholar] [CrossRef] [PubMed]
- Letourneau, N.L.; Tramonte, L.; Willms, J.D. Maternal depression, family functioning and children’s longitudinal development. J. Pediatr. Nurs. 2013, 28, 223–234. [Google Scholar] [CrossRef] [PubMed]
- Goodman, S.H.; Rouse, M.H.; Connell, A.M.; Broth, M.R.; Hall, C.M.; Heyward, D. Maternal depression and child psychopathology: A meta-analytic review. Clin. Child Fam. Psychol. Rev. 2011, 14, 1–27. [Google Scholar] [CrossRef] [PubMed]
- Netsi, E.; Pearson, R.M.; Murray, L.; Cooper, P.; Craske, M.G.; Stein, A. Association of persistent and severe postnatal depression with child outcomes. JAMA Psychiatry 2018, 75, 247–253. [Google Scholar] [CrossRef] [PubMed]
- Mughal, M.K.; Giallo, R.; Arnold, P.D.; Kehler, H.; Bright, K.; Benzies, K.; Wajid, A.; Kingston, D. Trajectories of maternal distress and risk of child developmental delays: Findings from the All Our Families (AOF) pregnancy cohort. J. Affect. Disord. 2019, 248, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Cornish, A.M.; McMahon, C.A.; Ungerer, J.A.; Barnett, B.; Kowalenko, N.; Tennant, C. Postnatal depression and infant cognitive and motor development in the second postnatal year: The impact of depression chronicity and infant gender. Infant Behav. Dev. 2005, 28, 407–417. [Google Scholar] [CrossRef]
- World Health Organization. International Statistical Classification of Diseases and Related Health Problems (11th Revision). 2018. Available online: https://icd.who.int/browse11/l-m/en (accessed on 8 December 2018).
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 4th ed.; American Psychiatric Association: Arlington, VA, USA, 2000. [Google Scholar]



{kind=link}
{kind=link}
| Characteristics | Parental Trial (Data Obtained at Baseline) | Follow-up Study (Data Obtained at 12–16 Months) | ||
|---|---|---|---|---|
| Intervention (n = 263) | Control (n = 248) | Intervention (n = 77) | Control (n = 78) | |
| Children (n, %) | ||||
| Males | 139 (52.9) | 123 (49.6) | 44 (57.1) | 41 (52.6) |
| Females | 124 (47.1) | 125 (50.4) | 33 (42.9) | 37 (47.4) |
| Age at inclusion (months) | 7.4 (0.8) | 7.3 (0.9) | 21.4 (1.0) | 21.2 (1.0) |
| Child growth (n, %) | ||||
| Stunting * | 55 (20.9) | 70 (28.0) | 32 (41.6) | 46 (59.0) |
| Underweight * | 25 (9.5) | 36 (14.5) | 6 (7.8) | 8 (10.3) |
| Wasting * | 12 (4.6) | 12 (4.8) | 3 (3.9) | 2 (2.6) |
| BSID-III composite score | ||||
| Cognitive | 114.9 (21.3) | 99.3 (17.1) | 116.1 (15.6) | 105.9 (15.9) |
| Language | 98.3 (14.3) | 88.4 (9.1) | 106.5 (14.8) | 98.9 (12.8) |
| Motor | 113.6 (18.9) | 99.1 (14.3) | 122.3 (18.7) | 113.3 (19.9) |
| Maternal data | ||||
| Maternal education (years) | 4.9 (2.8) | 4.9 (2.8) | 5.5 (2.5) | 5.0 (2.6) |
| Maternal age (years) | 26.1 (5.8) | 26.8 (6.3) | 26.2 (6.1) | 27.4 (6.4) |
| Number of children per mother | 3.4 (2.2) | 3.3 (2.2) | 3.4 (2.2) | 3.3 (2.2) |
| Household data | ||||
| Household head age (years) | 31.3 (7.7) | 32.6 (19.4) | 30.2 (7.3) | 33.1 (10.9) |
| Household head education (years) | 6.4 (3.1) | 5.9 (3.1) | 6.6 (3.3) | 6.5 (3.4) |
| Household size (n) | 5.5 (2.1) | 5.5 (2.1) | 5.7 (2.2) | 5.8 (2.2) |
| Household poverty score | 47.8 (11.7) | 47.6 (11.4) | 49.0 (11.6) | 46.3 (12.3) |
| Sanitation composite score | 7.2 (1.9) | 7.3 (1.9) | 7.0 (1.8) | 7.1 (1.9) |
| Intervention * | Control * | Inter-Group Difference * | p-Value | Overall p-Value | |
|---|---|---|---|---|---|
| (n = 73–77) | (n = 74–78) | (n = 147–155) | |||
| Age of Child (months) | Beck Depression Inventory (BDI-II) | ||||
| 12–16 | 18.23 (10.55) | 19.50 (10.22) | −1.27 (−2.50 to −1.00) | 0.48 | 0.0001 |
| 20–24 | 13.58 (7.70) | 22.24 (15.20) | −8.26 (−11.49 to −1.13) | 0.0001 | |
| 36 | 11.87 (9.99) | 18.41 (13.75) | −6.54 (−8.69 to −2.99) | 0.004 | |
| Age of Child (months) | Center for Epidemiological Studies-Depression (CES-D) | ||||
| 12–16 | 18.36 (10.56) | 20.67 (12.06) | −2.31 (−4.99 to −1.31) | 0.32 | 0.002 |
| 20–24 | 14.06 (7.85) | 22.62 (15.18) | −8.56 (−10.82 to −2.72) | 0.0001 | |
| 36 | 12.81 (9.47) | 18.90 (13.66) | −6.09 (−9.21 to −3.09) | 0.002 | |
| Outcome | Child Age (months) | R * | 95% CI | p-Value ** | p-Value Interaction *** |
|---|---|---|---|---|---|
| BSID-III scores | |||||
| Cognitive development | 12–16 | −0.25 | −0.30 to 0.20 | 0.70 | 0.005 |
| 20–24 | −0.30 | −0.54 to −0.06 | 0.01 | ||
| 36 | −0.31 | −0.57 to −0.06 | 0.017 | ||
| Language development | 12–16 | −0.06 | −0.32 to 0.20 | 0.63 | 0.031 |
| 20–24 | −0.01 | −0.15 to 0.13 | 0.008 | ||
| 36 | −0.20 | −0.23 to 0.16 | 0.001 | ||
| Motor development | 12–16 | −0.02 | −0.25 to 0.02 | 0.82 | 0.031 |
| 20–24 | −0.11 | −0.33 to −0.11 | 0.34 | ||
| 36 | −0.29 | −0.57 to −0.003 | 0.043 |
| Outcome | Child Age (months) | R * | 95% CI | p-Value ** | p-Value Interaction *** |
|---|---|---|---|---|---|
| BSID-III scores | |||||
| Cognitive development | 12–16 | −0.04 | −0.29 to 0.21 | 0.73 | 0.026 |
| 20–24 | −0.30 | −0.04 to −0.001 | 0.03 | ||
| 36 | −0.28 | −0.53 to −0.04 | 0.023 | ||
| Language development | 12–16 | −0.05 | −0.32 to 0.30 | 0.52 | 0.032 |
| 20–24 | −0.01 | −0.15 to 0.14 | 0.006 | ||
| 36 | −0.20 | −0.23 to 0.16 | 0.001 | ||
| Motor development | 12–16 | −0.04 | −0.18 to 0.26 | 0.71 | 0.025 |
| 20–24 | −0.06 | −0.27 to 0.15 | 0.59 | ||
| 36 | −0.29 | −0.55 to 0.03 | 0.028 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Atukunda, P.; Muhoozi, G.K.M.; Westerberg, A.C.; Iversen, P.O. Nutrition, Hygiene and Stimulation Education for Impoverished Mothers in Rural Uganda: Effect on Maternal Depression Symptoms and Their Associations to Child Development Outcomes. Nutrients 2019, 11, 1561. https://doi.org/10.3390/nu11071561
Atukunda P, Muhoozi GKM, Westerberg AC, Iversen PO. Nutrition, Hygiene and Stimulation Education for Impoverished Mothers in Rural Uganda: Effect on Maternal Depression Symptoms and Their Associations to Child Development Outcomes. Nutrients. 2019; 11(7):1561. https://doi.org/10.3390/nu11071561
Chicago/Turabian StyleAtukunda, Prudence, Grace K. M. Muhoozi, Ane C. Westerberg, and Per O. Iversen. 2019. "Nutrition, Hygiene and Stimulation Education for Impoverished Mothers in Rural Uganda: Effect on Maternal Depression Symptoms and Their Associations to Child Development Outcomes" Nutrients 11, no. 7: 1561. https://doi.org/10.3390/nu11071561