Differing Water Intake and Hydration Status in Three European Countries—A Day-to-Day Analysis

 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Protocol
2.2. Study Procedure
2.3. Data Processing and Statistical Analysis
3. Results
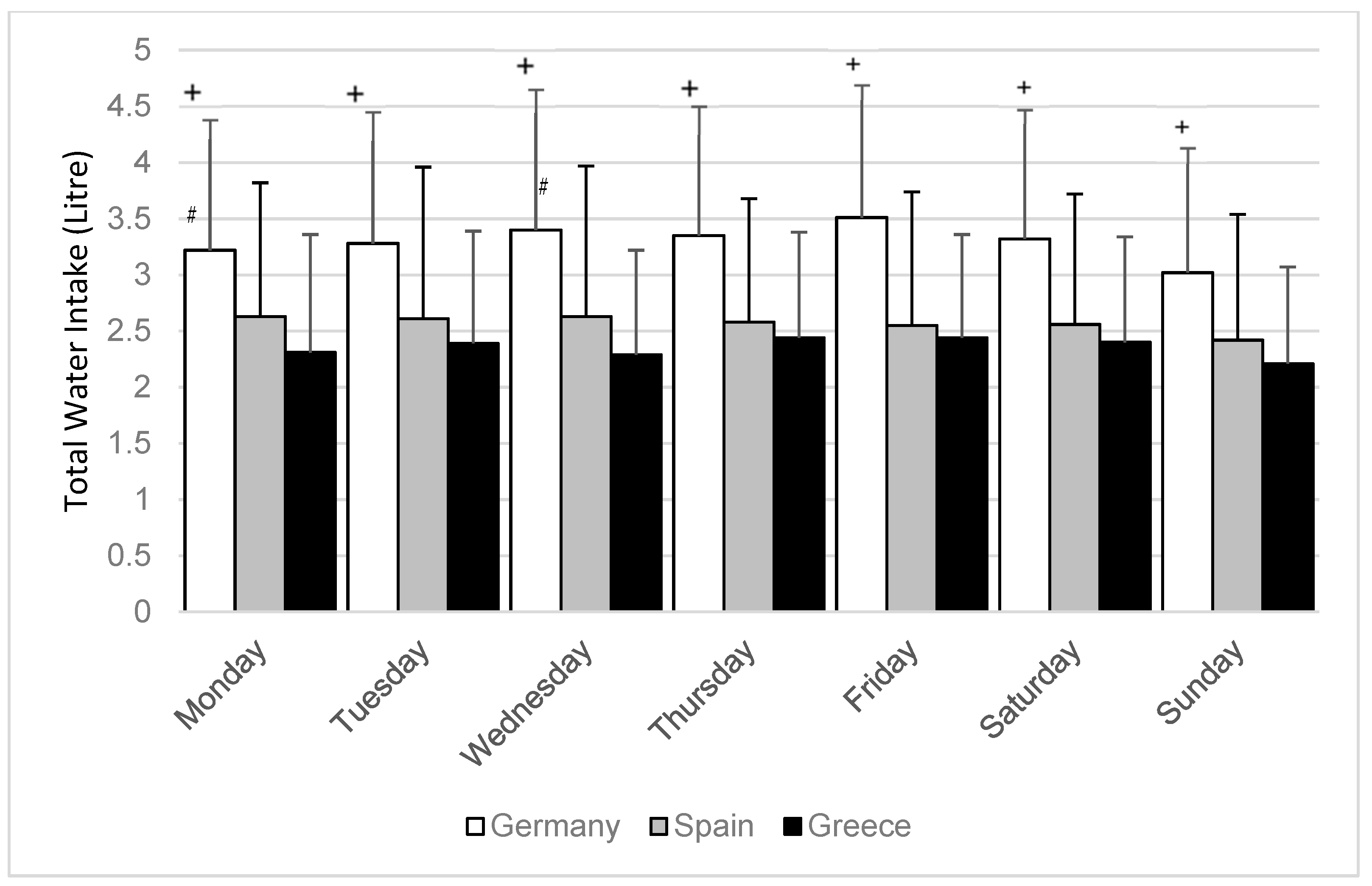
3.1. Total Water Intake
3.2. Urine Osmolality
3.3. Urine Volume
4. Discussion
4.1. Total Water Intake
4.2. Urine Osmolality
4.3. Urine Volume
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- EFSA. Scientific opinion on dietary reference values for water. EFSA J. 2010, 8, 1459–1507. [Google Scholar]
- Thomas, D.R.; Cote, T.R.; Lawhorne, L.; Levenson, S.A.; Rubenstein, L.Z.; Smith, D.A.; Morley, J.E. Understanding clinical dehydration and its treatment. J. Am. Med. Dir. Assoc. 2008, 9, 292–301. [Google Scholar] [CrossRef] [PubMed]
- Benelam, B.; Wyness, L. Hydration and health: A review. Nutr. Bull. 2010, 35, 3–25. [Google Scholar] [CrossRef]
- Cheuvront, S.N.; Kenefick, R.W.; Charkoudian, N.; Sawka, M.N. Physiologic basis for understanding quantitative dehydration assessment. Am. J. Clin. Nutr. 2013, 97, 455–462. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suhayda, R.; Walton, J.C. Preventing and managing dehydration. Medsurg. Nurs. 2002, 11, 267–278. [Google Scholar]
- El-Sharkawy, A.M.; Sahota, O.; Lobo, D.N. Acute and chronic effects of hydration status on health. Nutr. Rev. 2015, 73 (Suppl. 2), 97–109. [Google Scholar] [CrossRef] [Green Version]
- D’Aanci, K.E.; Mahoney, C.R.; Vibhhakar, A.; Kanter, J.H.; Taylor, H.A. Voluntary dehydration and cognitive performance in trained college athletes. Percept. Mot. Skills 2009, 109, 251–269. [Google Scholar] [CrossRef]
- Shirreffs, S.M.; Merson, S.J.; Fraser, S.M.; Archer, D.T. The effects of fluid restriction on hydration status and subjective feelings in man. Br. J. Nutr. 2004, 91, 951–958. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Armstrong, L.E.; Ganio, M.S.; Casa, D.J.; Lee, E.C.; McDermott, B.P.; Klau, J.F.; Jimenez, L.; Le Bellego, L.; Chevillotte, E.; Lieberman, H.R. Mild dehydration affects mood in healthy young women. J. Nutr. 2012, 142, 382–388. [Google Scholar] [CrossRef]
- Cian, C.; Barraud, P.A.; Melin, B.; Raphel, C. Effects of fluid ingestion on cognitive function after heat stress or exercise-induced dehydration. Int. J. Psychophysiol. 2001, 42, 243–251. [Google Scholar] [CrossRef]
- Ganio, M.S.; Armstrong, L.E.; Casa, D.J.; McDermott, B.P.; Lee, E.C.; Yamamoto, L.M.; Lieberman, H.R. Mild dehydration impairs cognitive performance and mood of men. Br. J. Nutr. 2011, 106, 1535–1543. [Google Scholar] [CrossRef] [Green Version]
- Pross, N.; Demazières, A.; Girard, N.; Barnouin, R.; Santoro, F.; Chevillotte, E.; Le Bellego, L. Influence of progressive fluid restriction on mood and physiological markers of dehydration in women. Br. J. Nutr. 2013, 109, 313–321. [Google Scholar] [CrossRef]
- Armstrong, L.E.; Johnson, E.C.; Munoz, C.X.; Swokla, B.; Le Bellego, L.; Jimenez, L.; Maresh, C.M. Hydration biomarkers and dietary fluid consumption of women. J. Acad. Nutr. Diet. 2012, 112, 1056–1061. [Google Scholar] [CrossRef] [PubMed]
- Gopinathan, P.M.; Pichan, G.; Sharma, V.M. Role of dehydration in heat stress-induced variations in mental performance. Arch. Environ. Health 1988, 43, 15–17. [Google Scholar] [CrossRef] [PubMed]
- Suhr, J.A.; Hall, J.; Patterson, S.M.; Niinistö, R.T. The relation of hydration status to cognitive performance in healthy older adults. Int. J. Psychophysiol. 2004, 53, 121–125. [Google Scholar] [CrossRef]
- Sharma, V.M.; Sridharan, K.; Pichan, G.; Panwar, M.R. Influence of heat-stress induced dehydration on mental functions. Ergonomics 1986, 29, 791–799. [Google Scholar] [CrossRef]
- Elmadfa, I.; Meyer, A.L. Patterns of drinking and eating across the European Union: Implications for hydration status. Nutr. Rev. 2015, 73 (Suppl. 2), 141–147. [Google Scholar] [CrossRef] [PubMed]
- Gibson, S.; Gunn, P.; Maughan, R.J. Hydration, water intake and beverage consumption habits among adults. Nutr. Bull. 2012, 37, 182–192. [Google Scholar] [CrossRef]
- Gibson, S.; Shirreffs, S.M. Beverage consumption habits “24/7” among British adults: Association with total water intake and energy intake. Nutr. J. 2013, 12, 9. [Google Scholar] [CrossRef] [PubMed]
- Malisova, O.; Athanasatou, A.; Pepa, A.; Husemann, M.; Domnik, K.; Braun, H.; Mora-Rodriguez, R.; Ortega, J.F.; Fernandez-Elias, V.E.; Kapsokefalou, M. Water Intake and Hydration Indices in Healthy European Adults: The European Hydration Research Study (EHRS). Nutrients 2016, 8, 204. [Google Scholar] [CrossRef]
- Mora-Rodriguez, R.; Ortega, J.F.; Fernandez-Elias, V.E.; Kapsokefalou, M.; Malisova, O.; Athanasatou, A.; Husemann, M.; Domnik, K.; Braun, H. Influence of Physical Activity and Ambient Temperature on Hydration: The European Hydration Research Study (EHRS). Nutrients 2016, 8, 252. [Google Scholar] [CrossRef]
- Perrier, E.T.; Buendia-Jimenez, I.; Vecchio, M.; Armstrong, L.E.; Tack, I.; Klein, A. Twenty-Four-Hour Urine Osmolality as a Physiological Index of Adequate Water Intake. Dis. Markers 2015, 2015, 231063. [Google Scholar] [CrossRef]
- Armstrong, L.E.; Johnson, E.C.; McKenzie, A.L.; Muñoz, C.X. An empirical method to determine inadequacy of dietary water. Nutrition 2016, 32, 79–82. [Google Scholar] [CrossRef]
- Perrier, E.; Rondeau, P.; Poupin, M.; Le Bellego, L.; Armstrong, L.E.; Lang, F.; Stookey, J.; Tack, I.; Vergne, S.; Klein, A. Relation between urinary hydration biomarkers and total fluid intake in healthy adults. Eur. J. Clin. Nutr. 2013, 67, 939–943. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Armstrong, L.E.; Johnson, E.C.; McKenzie, A.L.; Muñoz, C.X. Interpreting common hydration biomarkers on the basis of solute and water excretion. Eur. J. Clin. Nutr. 2013, 67, 249–253. [Google Scholar] [CrossRef] [PubMed]
- Manz, F.; Wentz, A. 24-h Hydration status: Parameters, epidemiology and recommendations. Eur. J. Clin. Nutr. 2003, 57 (Suppl. 2), S10–S18. [Google Scholar] [CrossRef] [PubMed]
- Cheuvront, S.N.; Ely, B.R.; Kenefick, R.W.; Sawka, M.N. Biological variation and diagnostic accuracy of dehydration assessment markers. Am. J. Clin. Nutr. 2010, 92, 565–573. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clark, W.F.; Sontrop, J.M.; Macnab, J.J.; Suri, R.S.; Moist, L.; Salvadori, M.; Garg, A.X. Urine volume and change in estimated GFR in a community-based cohort study. Clin. J. Am. Soc. Nephrol. 2011, 6, 2634–2641. [Google Scholar] [CrossRef]
- Strippoli, G.F.; Craig, J.C.; Rochtchina, E.; Flood, V.M.; Wang, J.J.; Mitchell, P. Fluid and nutrient intake and risk of chronic kidney disease. Nephrology 2011, 16, 326–334. [Google Scholar] [CrossRef]
- Sontrop, J.M.; Dixon, S.N.; Garg, A.X.; Buendia-Jimenez, I.; Dohein, O.; Huang, S.H.; Clark, W.F. Association between water intake, chronic kidney disease, and cardiovascular disease: A cross-sectional analysis of NHANES data. Am. J. Nephrol. 2013, 37, 434–442. [Google Scholar] [CrossRef]
- Perrier, E.; Vergne, S.; Klein, A.; Poupin, M.; Rondeau, P.; Le Bellego, L.; Armstrong, L.E.; Lang, F.; Stookey, J.; Tack, I. Hydration biomarkers in free-living adults with different levels of habitual fluid consumption. Br. J. Nutr. 2013, 109, 1678–1687. [Google Scholar] [CrossRef] [PubMed]
- Feehally, J.; Khosravi, M. Effects of acute and chronic hypohydration on kidney health and function. Nutr. Rev. 2015, 73 (Suppl. 2), 110–119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benton, D.; Young, H.A. Do small differences in hydration status affect mood and mental performance? Nutr. Rev. 2015, 73 (Suppl. 2), 83–96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Watson, P.; Whale, A.; Mears, S.A.; Reyner, L.A.; Maughan, R.J. Mild hypohydration increases the frequency of driver errors during a prolonged, monotonous driving task. Physiol. Behav. 2015, 147, 313–318. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Institute of Medicine (IoM). Dietary Reference Intakes for Water Potassium, Sodium, Chloride, and Sulfate; National Academies Press: Washington, DC, USA, 2004. [Google Scholar]
- Shirreffs, S.M.; Maughan, R.J. Urine osmolality and conductivity as indices of hydration status in athletes in the heat. Med. Sci. Sports Exerc. 1998, 30, 1598–1602. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Weekday | Total Water Intake (Mean ± SD in L/day) | TWI < EFSA (in %) | |||||
|---|---|---|---|---|---|---|---|
| All | Men | Women | p-Value * | All | Men # | Women # | |
| Monday | 2.74 ± 1.2 | 2.92 ± 1.26 | 2.55 ± 1.08 | =0.001 | 35 | 41 | 30 |
| Tuesday | 2.78 ± 1.2 | 2.94 ± 1.41 | 2.62 ± 1.04 | =0.012 | 32 | 38 | 25 |
| Wednesday | 2.80 ± 1.3 | 3.00 ± 1.38 | 2.59 ± 1.13 | <0.001 | 35 | 39 | 30 |
| Thursday | 2.80 ± 1.1 | 2.97 ± 1.21 | 2.64 ± 1.03 | =0.002 | 32 | 38 | 25 |
| Friday | 2.85 ± 1.2 | 3.02 ± 1.32 | 2.69 ± 1.08 | =0.004 | 35 | 41 | 28 |
| Saturday | 2.78 ± 1.2 | 2.98 ± 1.29 | 2.59 ± 0.99 | =0.001 | 35 | 41 | 28 |
| Sunday | 2.57 ± 1.1 | 2.76 ± 1.19 | 2.38 ± 0.98 | <0.001 | 37 | 41 | 36 |
| All days | 2.76 ± 1.2 | 2.94 ± 1.10 | 2.57 ± 0.89 | <0.001 | 35 | 40 | 29 |
| Weekday | 24 h Urine Osmolality (Mean ± SD in mOsmol/kg) | |||
|---|---|---|---|---|
| All | Men | Women | p-Value * | |
| Monday | 642 ± 252 | 680 ± 238 | 605 ± 259 | <0.001 |
| Tuesday | 639 ± 256 | 687 ± 238 | 593 ± 265 | <0.001 |
| Wednesday | 620 ± 255 | 670 ± 242 | 568 ± 257 | <0.001 |
| Thursday | 639 ± 265 | 685 ± 250 | 590 ± 270 | <0.001 |
| Friday | 634 ± 254 | 669 ± 234 | 595 ± 267 | <0.001 |
| Saturday | 637 ± 250 | 686 ± 239 | 588 ± 252 | <0.001 |
| Sunday | 656 ± 241 | 687 ± 216 | 624 ± 260 | =0.002 |
| All 24 h samples | 638 ± 254 | 681 ± 237 | 595 ± 261 | <0.001 |
| Weekday | <500 mOsmol/kg (%) | 500–799 mOsmol/kg (%) | ≥800 mOsmol/kg (%) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| All | Men | Women | All | Men | Women | All | Men | Women | |
| Monday | 34 | 27 | 41 | 36 | 39 | 33 | 30 | 34 | 26 |
| Tuesday | 33 | 23 | 43 | 38 | 42 | 34 | 29 | 35 | 23 |
| Wednesday | 38 | 29 | 47 | 36 | 39 | 33 | 26 | 32 | 20 |
| Thursday | 35 | 25 | 45 | 36 | 41 | 32 | 29 | 34 | 23 |
| Friday | 36 | 28 | 46 | 35 | 40 | 30 | 28 | 32 | 24 |
| Saturday | 35 | 26 | 45 | 39 | 43 | 34 | 26 | 31 | 21 |
| Sunday | 30 | 22 | 39 | 40 | 47 | 32 | 30 | 31 | 29 |
| All 24 h samples | 34 | 26 | 44 | 37 | 42 | 33 | 28 | 32 | 24 |
| Weekday | 24 h Urine Volume (Mean ± SD in L/day) | Urine Volume <1 L/day (%) | |||||
|---|---|---|---|---|---|---|---|
| All | Men | Women | p-Value * | All | Men | Women | |
| Monday | 1.69 ± 0.87 | 1.69 ± 0.83 | 1.69 ± 0.91 | =0.615 | 21 | 18 | 24 |
| Tuesday | 1.66 ± 0.86 | 1.64 ± 0.80 | 1.69 ± 0.91 | =0.907 | 24 | 24 | 24 |
| Wednesday | 1.70 ± 0.89 | 1.68 ± 0.86 | 1.73 ± 0.91 | =0.683 | 22 | 22 | 22 |
| Thursday | 1.66 ± 0.80 | 1.68 ± 0.78 | 1.66 ± 0.83 | =0.418 | 22 | 17 | 26 |
| Friday | 1.70 ± 0.88 | 1.69 ± 0.81 | 1.73 ± 0.95 | =0.785 | 20 | 17 | 23 |
| Saturday | 1.68 ± 0.85 | 1.65 ± 0.79 | 1.71 ± 0.92 | =0.911 | 21 | 19 | 23 |
| Sunday | 1.65 ± 0.82 | 1.68 ± 0.79 | 1.63 ± 0.85 | =0.198 | 22 | 17 | 26 |
| All 24 h samples | 1.68 ± 0.85 | 1.67 ± 0.81 | 1.69 ± 0.90 | =0.881 | 22 | 19 | 24 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Braun, H.; von Andrian-Werburg, J.; Malisova, O.; Athanasatou, A.; Kapsokefalou, M.; Ortega, J.F.; Mora-Rodriguez, R.; Thevis, M. Differing Water Intake and Hydration Status in Three European Countries—A Day-to-Day Analysis. Nutrients 2019, 11, 773. https://doi.org/10.3390/nu11040773
Braun H, von Andrian-Werburg J, Malisova O, Athanasatou A, Kapsokefalou M, Ortega JF, Mora-Rodriguez R, Thevis M. Differing Water Intake and Hydration Status in Three European Countries—A Day-to-Day Analysis. Nutrients. 2019; 11(4):773. https://doi.org/10.3390/nu11040773
Chicago/Turabian StyleBraun, Hans, Judith von Andrian-Werburg, Olga Malisova, Adelais Athanasatou, Maria Kapsokefalou, Juan F. Ortega, Ricardo Mora-Rodriguez, and Mario Thevis. 2019. "Differing Water Intake and Hydration Status in Three European Countries—A Day-to-Day Analysis" Nutrients 11, no. 4: 773. https://doi.org/10.3390/nu11040773