Growth, Protein and Energy Intake in Children with PKU Taking a Weaning Protein Substitute in the First Two Years of Life: A Case-Control Study

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Anthropometry
2.2. Dietary Records
2.3. Study Product (PKU Subjects)
2.4. Introduction of Weaning Protein Substitute (PKU Subjects)
2.5. Ethical Approval
2.6. Statistics
3. Results
3.1. Subjects
3.1.1. PKU Group
3.1.2. Control Group
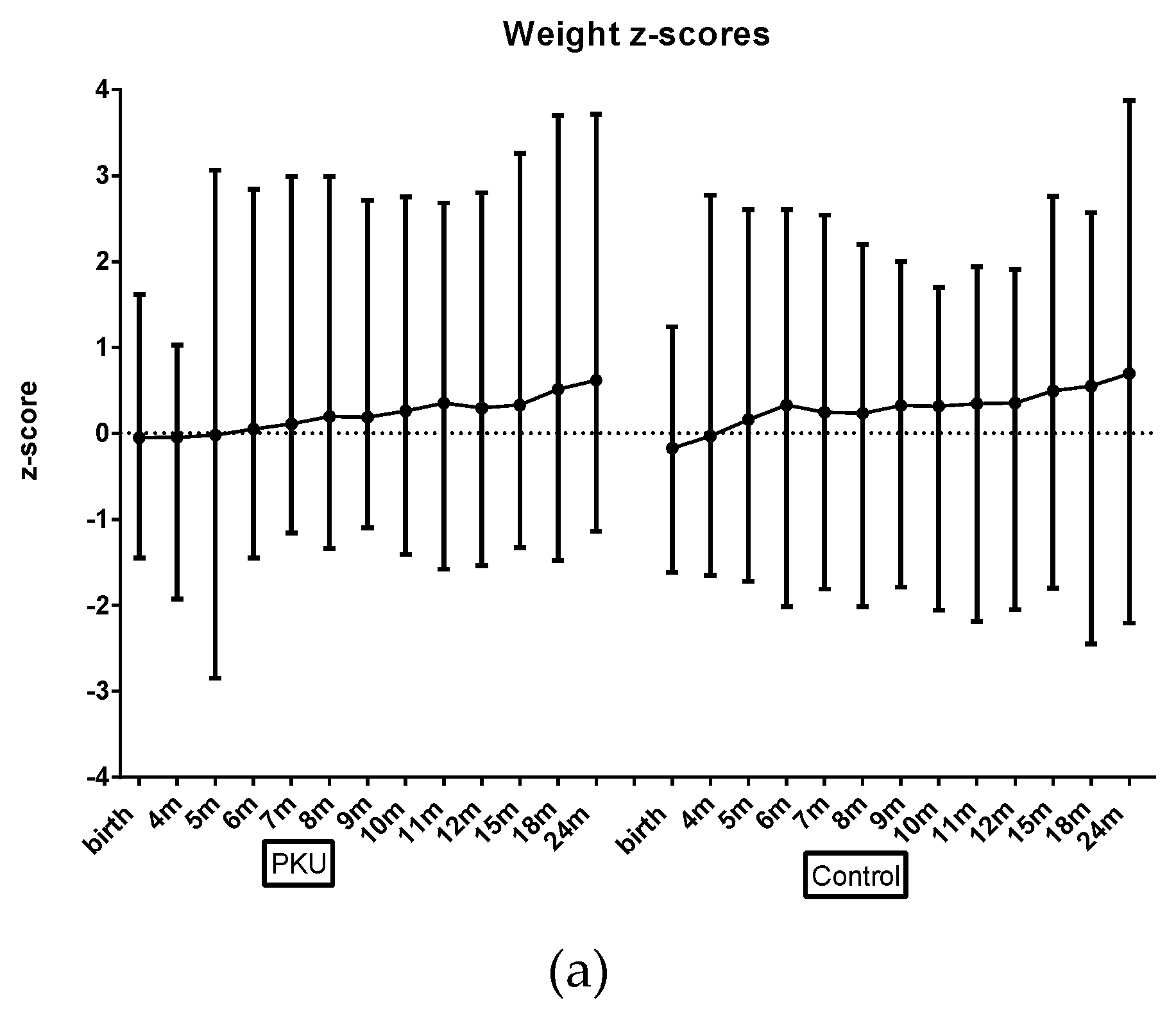
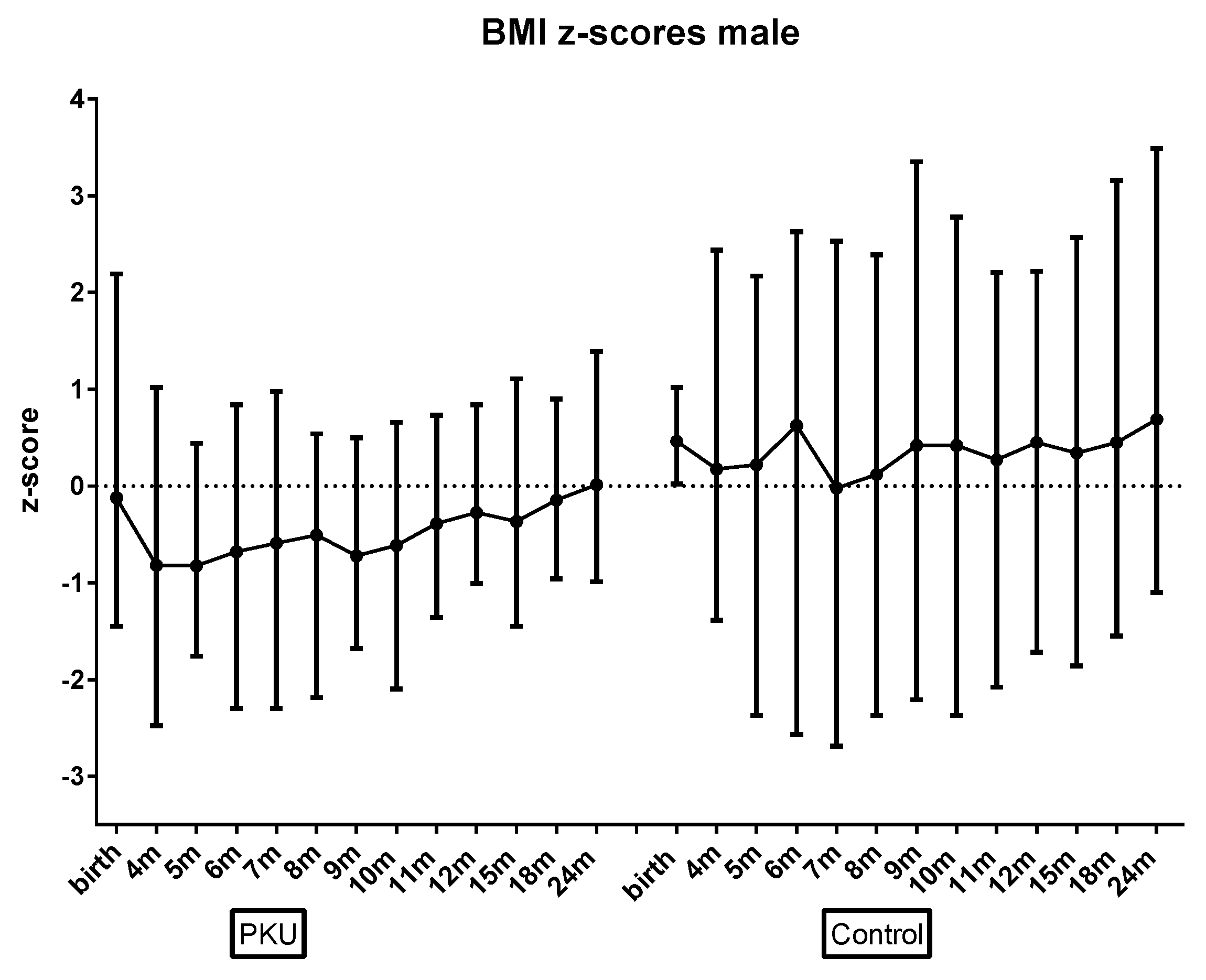
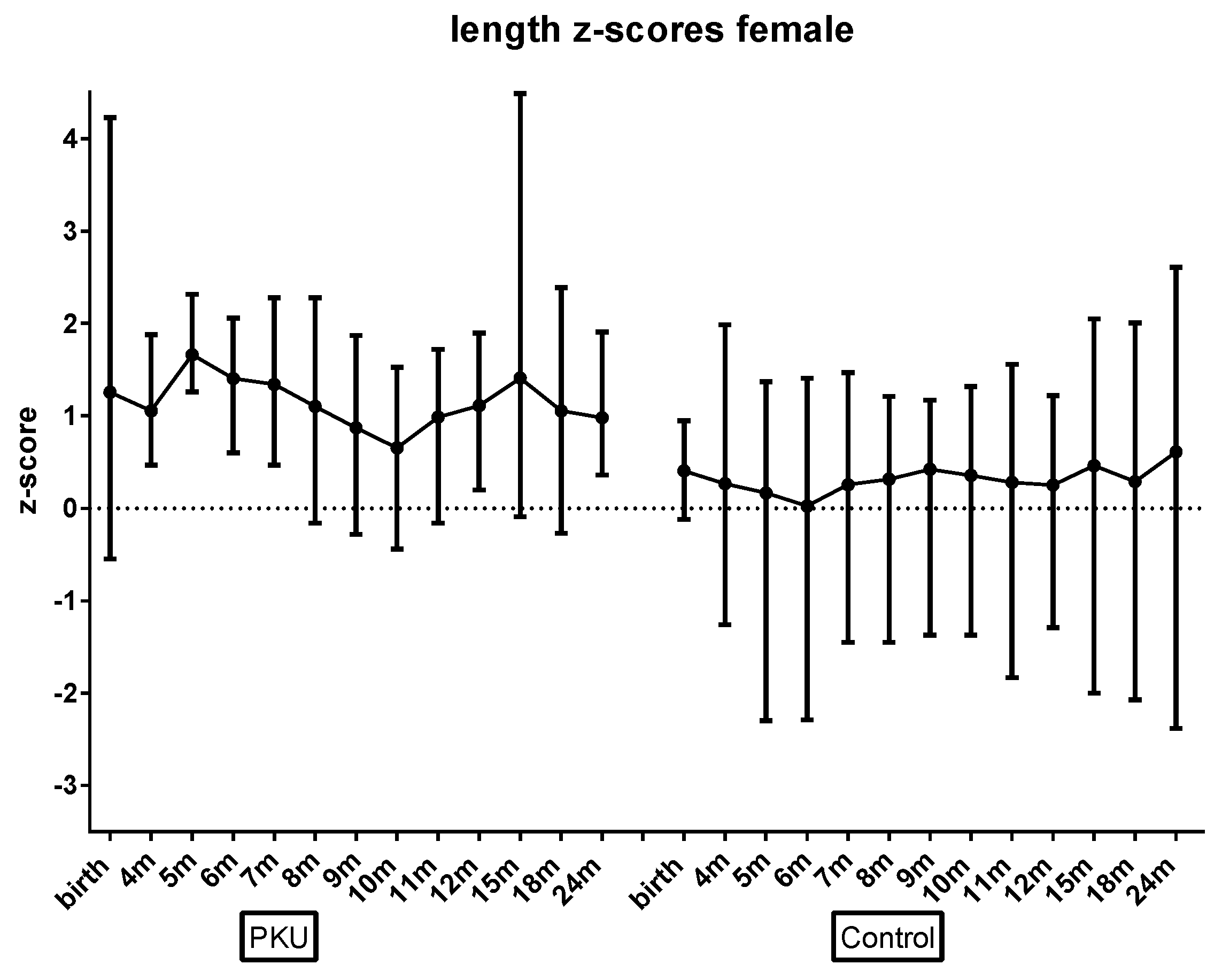
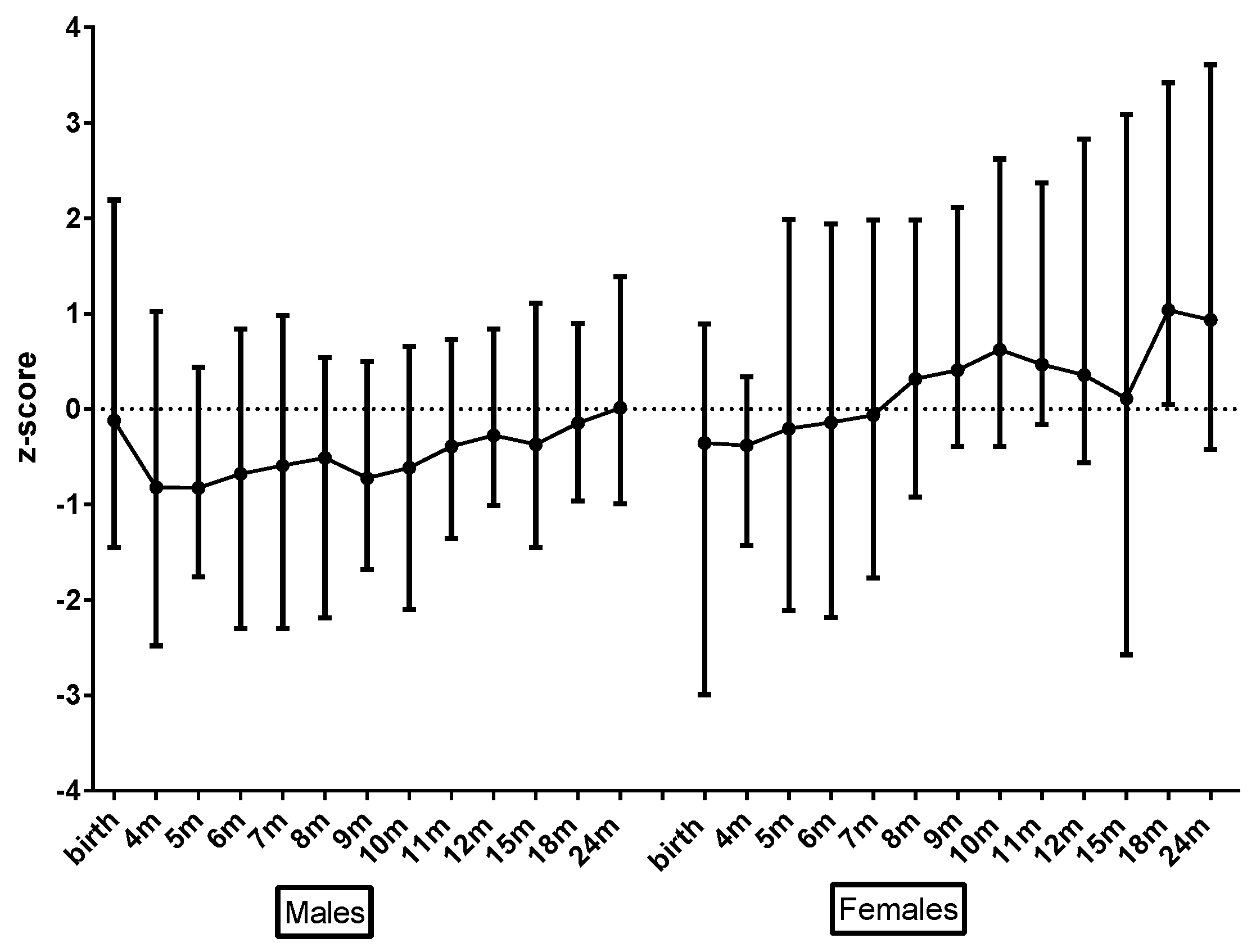
3.2. Growth
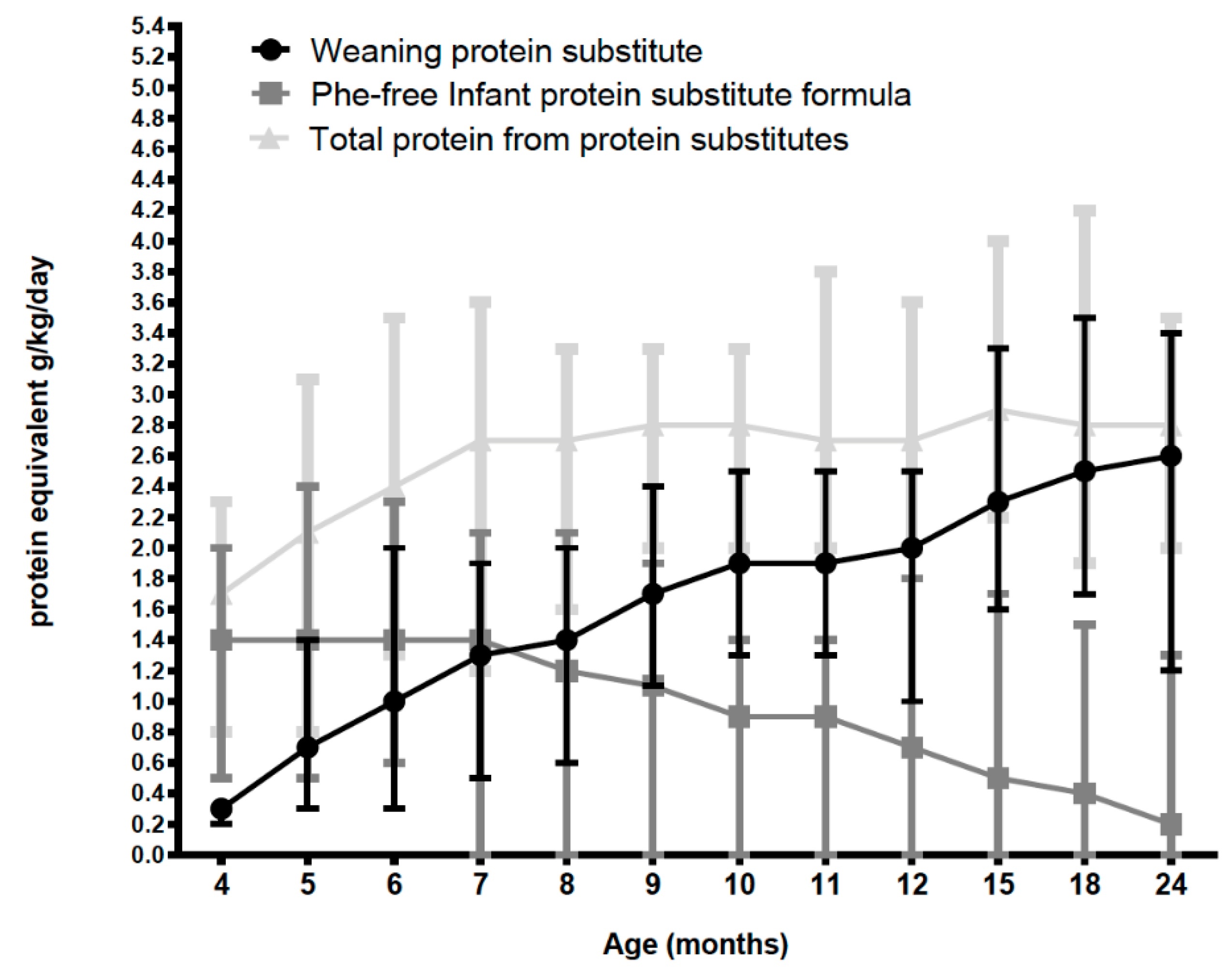
3.3. Protein Intake from Protein Substitutes (PKU Group Only) (Excluding Natural Protein Intake)
3.4. Total Protein Intake PKU vs. Control (Includes Natural Protein Intake)
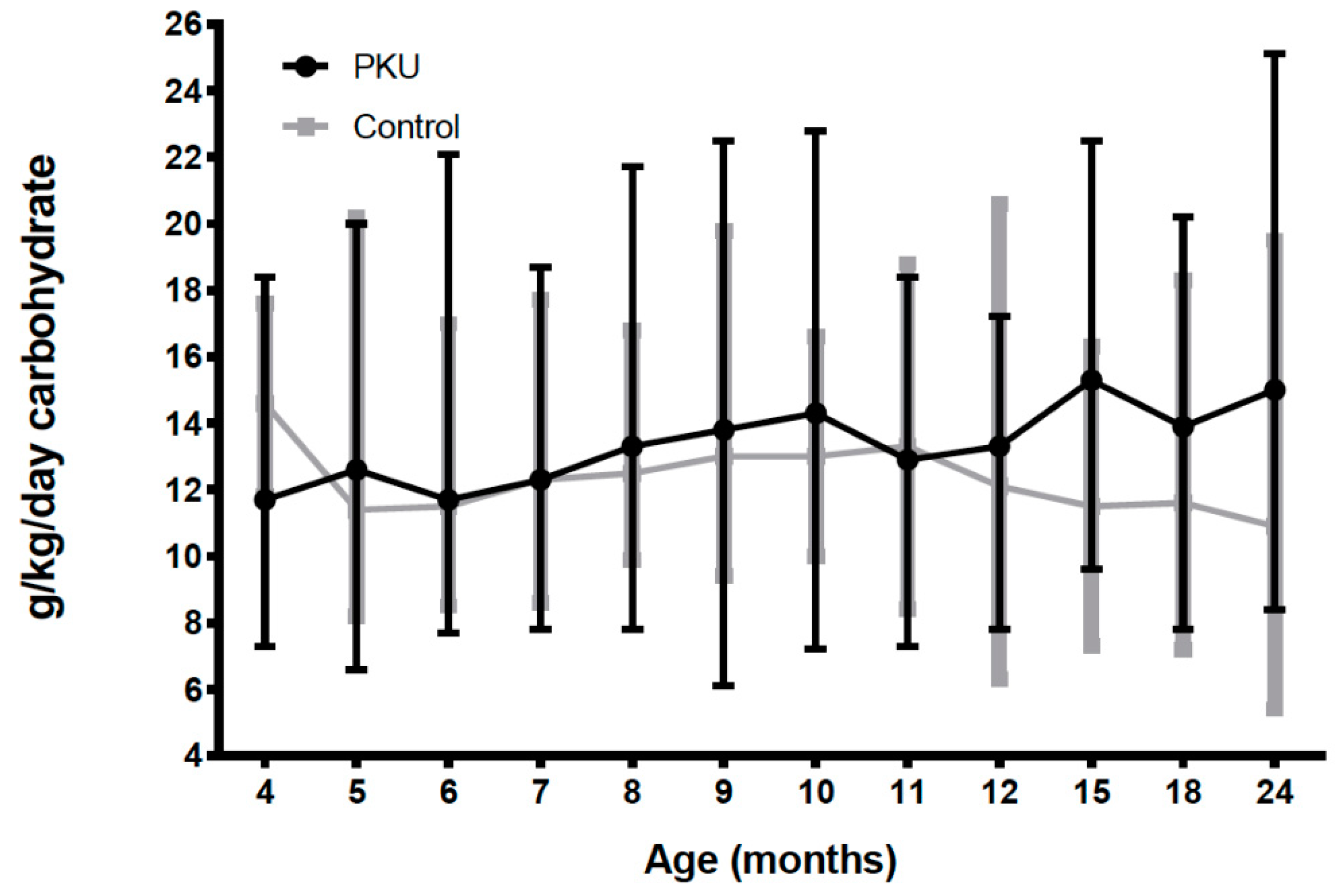
3.5. Total Carbohydrate and Fat Intake PKU vs. Control
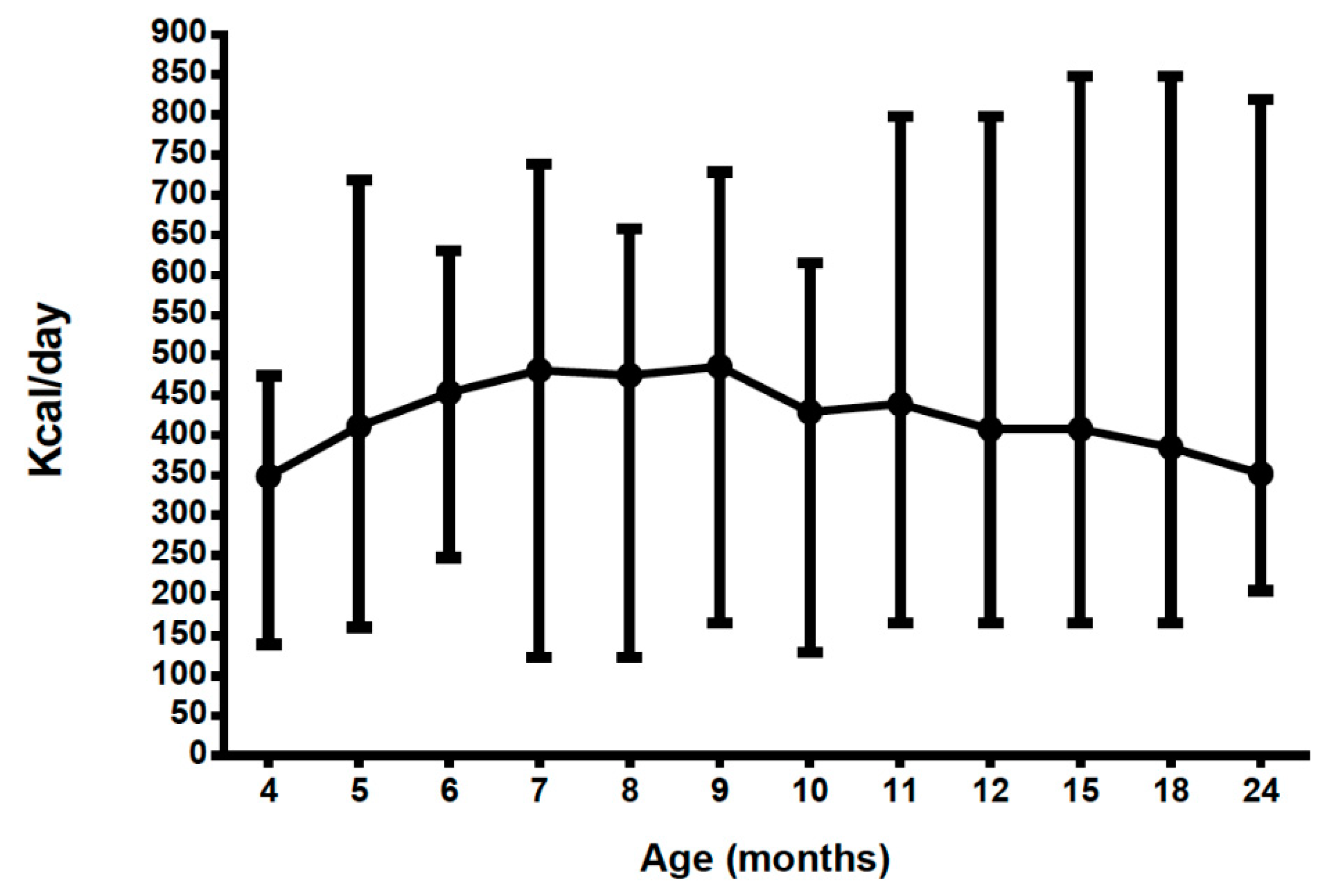
3.6. Energy Intake from Protein Substitutes (PKU Group Only) (Excludes Energy Contribution from Food)
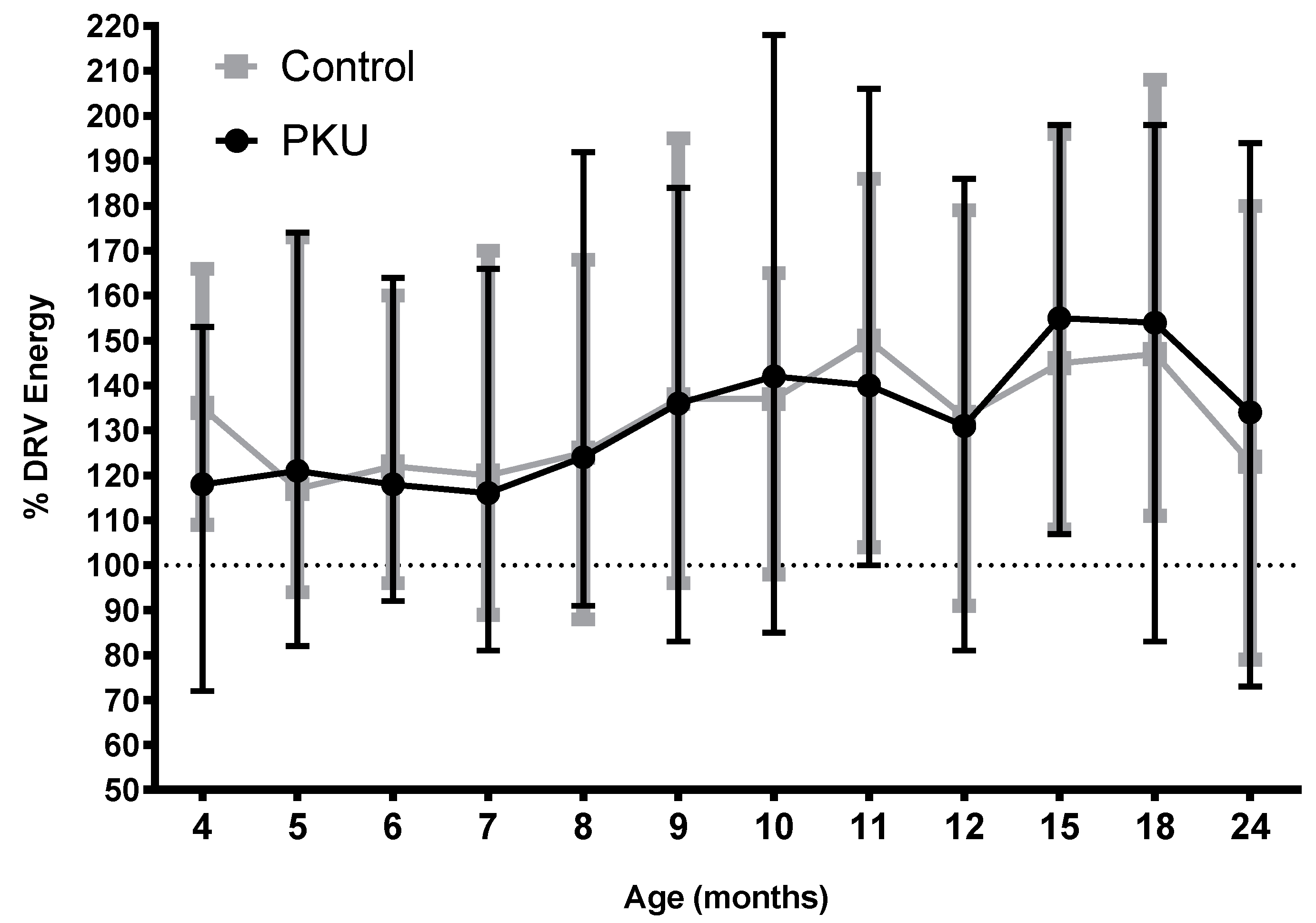
3.7. Total Energy Intake PKU vs. Control (Includes Energy Intake from Food)
3.8. Percentage of Energy from Carbohydrate, Fat and Protein PKU vs. Control (Includes Energy Intake from Food)
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Van Spronsen, F.J.; Van Wegberg, A.M.J.; Ahring, K.; Bélanger-Quintana, A.; Blau, N.; Bosch, A.M.; Burlina, A.; Campistol, J.; Feillet, F.; Gizewska, M.; et al. Key European guidelines for the diagnosis and management of patients with phenylketonuria. Lancet Diabetes Endocrinol. 2017, 5, 743–756. [Google Scholar] [CrossRef] [Green Version]
- Medical Research Council. Recommendations on the dietary management of phenylketonuria. Report of Medical Research Council Working Party on Phenylketonuria. Arch Dis. Child 1993, 68, 426–427. [Google Scholar] [CrossRef]
- Bickel, H.; Gerrard, J.; Hickmans, E.M. The Influence of Phenylalanine Intake on the Chemistry and Behaviour of a Phenylketonuria Child. Acta Paediatrica. 1954, 43, 64–77. [Google Scholar] [CrossRef] [PubMed]
- Schaefer, F.; Burgard, P.; Batzler, U.; Rupp, A.; Schmidt, H.; Gilli, G.; Bickel, H.; Bremer, H.J. Growth and skeletal maturation in children with phenylketonuria. Acta Paediatrica. 1994, 83, 534–541. [Google Scholar] [CrossRef] [PubMed]
- Arnold, G.L.; Vladutiu, C.J.; Kirby, R.S.; Blakely, E.M.; DeLuca, J.M. Protein insufficiency and linear growth restriction in phenylketonuria. J. Pediatrics. 2002, 141, 243–246. [Google Scholar] [CrossRef] [PubMed]
- Zaffanello, M.; Zamboni, G.; Tato, L. Growth parameters in newborns with hyperphenylalaninaemia. Paediat. Perinat. Epidemiol. 2002, 16, 274–277. [Google Scholar] [CrossRef]
- Dobbelaere, D.; Michaud, L.; Debrabander, A.; Vanderbecken, S.; Gottrand, F.; Turck, D.; Farriaux, J.P. Evaluation of nutritional status and pathophysiology of growth retardation in patients with phenylketonuria. J. Inherit. Metab Dis. 2003, 26, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Hoeksma, M.; Van Rijn, M.; Verkerk, P.H.; Bosch, A.M.; Mulder, M.F.; De Klerk, J.B.; De Koning, T.J.; Rubio-Gozalbo, E.; De Vries, M.; Sauer, P.J.; van Spronsen, F.J. The intake of total protein, natural protein and protein substitute and growth of height and head circumference in Dutch infants with phenylketonuria. J. Inherit. Metab. Dis. 2005, 28, 845–854. [Google Scholar] [CrossRef] [PubMed]
- Enns, G.M.; Koch, R.; Brumm, V.; Blakely, E.; Suter, R.E. Suboptimal outcomes in patients with PKU treated early with diet alone: Revisiting the evidence. Mol. Genet. Metab. 2010, 101, 99–109. [Google Scholar] [CrossRef] [PubMed]
- Aldamiz-Echevarria, L.; Bueno, M.A.; Couce, M.L.; Lage, S.; Dalmau, J.; Vitoria, I.; Andrade, F.; Blasco, J.; Alcalde, C.; Gil, D.; et al. Anthropometric characteristics and nutrition in a cohort of PAH-deficient patients. Clin. Nutr. (Edinburgh, Scotland). 2014, 33, 702–717. [Google Scholar] [CrossRef] [PubMed]
- Thiele, A.G.; Gausche, R.; Lindenberg, C.; Beger, C.; Arelin, M.; Rohde, C.; Mutze, U.; Weigel, J.F.; Mohnike, K.; Baerwald, C.; et al. Growth and Final Height Among Children with Phenylketonuria. Pediatrics 2017, 140, e20170015. [Google Scholar] [CrossRef] [PubMed]
- Belanger, A.; Martínez-Pardo, M. Physical development in patients with phenylketonuria on dietary treatment: A retrospective study. Mol. Genet. Metab. 2011, 104, 480–484. [Google Scholar] [CrossRef] [PubMed]
- Evans, M.; Truby, H.; Boneh, A. The relationship between dietary intake, growth and body composition in Phenylketonuria. Mol. Genet. Metab. 2017, 122, 36–42. [Google Scholar] [CrossRef] [PubMed]
- Matic, J.; Zeltner, N.A.J. Normal Growth in PKU Patients Under Low-Protein Diet in a Single-Center Cross-Sectional Study. JIMD Rep. 2018, 43, 1–6. [Google Scholar] [PubMed]
- Couce, M.L.; Guler, I.; Anca-Couce, A.; Lojo, M.; Miras, A.; Leis, R.; Perez-Munuzuri, A.; Fraga, J.M.; Gude, F. New insights in growth of phenylketonuric patients. Eur. J. Pediatr. 2015, 174, 651–659. [Google Scholar] [CrossRef] [PubMed]
- Rocha, J.C.; Van Spronsen, F.J.; Almeida, M.F.; Ramos, E.; Guimarães, J.T.; Borges, N. Early dietary treated patients with phenylketonuria can achieve normal growth and body composition. Mol. Genet. Metab. 2013, 110, S40–S43. [Google Scholar] [CrossRef] [PubMed]
- Huemer, M.; Huemer, C.; Möslinger, D.; Huter, D.; Stöckler-Ipsiroglu, S. Growth and body composition in children with classical phenylketonuria: Results in 34 patients and review of the literature. J. Inherited Metabol. Dis. 2007, 30, 694. [Google Scholar] [CrossRef] [PubMed]
- Scowen, P. “Weaning and the weaning diet”: A summary of the department of health report. Professional care of mother and child. 1995, 5, 39–40. [Google Scholar] [PubMed]
- Department of Health and Social Security. Weaning and the Weaning Diet. Report of the Working Group on the Weaning Diet of the Committee on Medical Aspects of Food Policy; HMSO: London, UK, 1994; pp. 10–16.
- Portnoi, P.; MacDonald, A.; Watling, R.; Clarke, B.J.; Barnes, J.; Robertson, L.; White, F.; Jarvis, C.; Laing, S.; Weetch, E.; et al. A survey of feeding practices in infants with phenylketonuria. J. Hum. Nutr. Diet. 1999, 12, 287–292. [Google Scholar] [CrossRef]
- Evans, S.; Daly, A.; MacDonald, J.; Pinto, A.; MacDonald, A. Fifteen years of using a second stage protein substitute for weaning in phenylketonuria: a retrospective study. J. Hum. Nutr. Diet. 2017, 31, 349–356. [Google Scholar] [CrossRef] [PubMed]
- MacDonald, A.; Rylance, G.W.; Asplin, D.A.; Hall, K.; Harris, G.; Booth, I.W. Feeding problems in young PKU children. Acta Paediatr Suppl. 1994, 407, 73–74. [Google Scholar] [CrossRef] [PubMed]
- WHO. Global Database on Child Growth and Malnutrition; WHO: Geneva, Switzerland, 1997. [Google Scholar]
- WHO/FAO/UNU. Protein and Amino acid Requirements in Human Nutrition; Report of a joint WHO/FAO/UNU Expert Consultation; WHO/FAO/UNU: Geneva, Switzerland, 2007. [Google Scholar]
- SACN. Dietary Reference Values for Energy, 1st ed.; Stationery Office: London, UK, 2011.
- Vail, B.; Prentice, P.; Dunger, D.B.; Hughes, I.A.; Acerini, C.L.; Ong, K.K. Age at Weaning and Infant Growth: Primary Analysis and Systematic Review. J. Pediatr. 2015, 167, 317–324. [Google Scholar] [CrossRef] [PubMed]
- Weglage, J.; Bramswig, J.H.; Koch, H.G.; Karassalidou, S.; Ullrich, K. Growth in patients with phenylketonuria. Eur. J. Pediatr. 1994, 153, 537–538. [Google Scholar] [CrossRef] [PubMed]
- Dhondt, J.L.; Largillière, C.; Moreno, L.; Farriaux, J.P. Physical growth in patients with phenylketonuria. J. Inherited Metabol. Dis. 1995, 18, 135–137. [Google Scholar] [CrossRef]
- Verkerk, P.H.; Van Spronsen, F.J.; Smit, G.P.; Sengers, R.C. Impaired prenatal and postnatal growth in Dutch patients with phenylketonuria. The National PKU Steering Committee. Arch. Dis. Child. 1994, 71, 114. [Google Scholar] [CrossRef] [PubMed]
- Allen, J.R.; Baur, L.A.; Waters, D.L.; Humphries, I.R.; Allen, B.J.; Roberts, D.C.; Gaskin, K.J. Body protein in prepubertal children with phenylketonuria. Eur. J. Clin. Nutr. 1996, 50, 178–186. [Google Scholar] [PubMed]
- Van Spronsen, F.J.; Verkerk, P.H.; Van Houten, M.; Smit, G.P.; Van Der Meer, S.B.; Bakker, H.D.; Sengers, R.C. Does impaired growth of PKU patients correlate with the strictness of dietary treatment? National Dutch PKU Steering Committee. Acta Paediatrica (Oslo Norway 1992) 1997, 86, 816–818. [Google Scholar] [CrossRef]
- Jani, R.; Coakley, K.; Douglas, T.; Singh, R. Protein intake and physical activity are associated with body composition in individuals with phenylalanine hydroxylase deficiency. Mol. Genet. Metab. 2017, 121, 104–110. [Google Scholar] [CrossRef] [PubMed]
- Rose, H.J.; White, F.; MacDonald, A.; Rutherford, P.J.; Favre, E. Fat intakes of children with PKU on low phenylalanine diets. J. Human Nutr. Dietetics. 2005, 18, 395–400. [Google Scholar] [CrossRef] [PubMed]
- Rocha, J.C.; MacDonald, A.; Trefz, F. Is overweight an issue in phenylketonuria? Mol. Genet. Metab. 2013, 110, S18–S24. [Google Scholar] [CrossRef] [PubMed]
- Pena, M.J.; Almeida, M.F.; Van Dam, E.; Ahring, K.; Belanger-Quintana, A.; Dokoupil, K.; Gokmen-Ozel, H.; Lammardo, A.M.; MacDonald, A.; Robert, M.; Rocha, J.C. Special low protein foods for phenylketonuria: Availability in Europe and an examination of their nutritional profile. Orphanet. J. Rare Dis. 2015, 10, 162. [Google Scholar] [CrossRef] [PubMed]
- Stephen, A.; Alles, M.; De Graaf, C.; Fleith, M.; Hadjilucas, E.; Isaacs, E.; Maffeis, C.; Zeinstra, G.; Matthys, C.; Gil, A. The role and requirements of digestible dietary carbohydrates in infants and toddlers. Eur. J. Clin. Nutr. 2012, 66, 765–779. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Acosta, P.B.; Yannicelli, S.; Singh, R.; Mofidi, S.; Steiner, R.; DeVincentis, E.; Jurecki, E.; Bernstein, L.; Gleason, S.; Chetty, M.; et al. Nutrient intakes and physical growth of children with phenylketonuria undergoing nutrition therapy. J. Am. Diet. Assoc. 2003, 103, 1167–1173. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age Number Subjects | % from Weaning Protein Substitute (WPS) | % from Phe-Free Infant Formula | % from Food | Total kcal/day |
|---|---|---|---|---|
| 4 months n = 10 | 3 (2–4) | 49 (31–62) | 48 (35–65) | 653 (395–831) |
| 5 months n = 20 | 6 (2–11) | 52 (30–74) | 43 (18–67) | 709 (482–1082) |
| 6 months n = 19 | 9 (3–19) | 55 (25–75) | 37 (16–60) | 716 (529–1020) |
| 7 months n = 20 | 11 (5–19) | 49 (0–69) | 40 (17–85) | 802 (583–1187) |
| 8 months n = 20 | 13 (5–22) | 44 (0–68) | 44 (21–86) | 864 (643–1375) |
| 9 months n = 19 | 14 (7–25) | 39 (0–69) | 47 (21–82) | 939 (592–1320) |
| 10 months n = 18 | 16 (7–24) | 30 (0–61) | 55 (26–84) | 983 (610–1558) |
| 11 months n = 17 | 17 (10–26) | 29 (0–50) | 54 (27–84) | 970 (703–1478) |
| 12 months n = 19 | 18 (7–29) | 23 (0–49) | 59 (35–83) | 978 (621–1420) |
| 15 months n = 19 | 18 (14–28) | 17 (0–55) | 65 (27–85) | 1160 (768–1509) |
| 18 months n = 20 | 21 (14–40) | 11 (0–44) | 67 (42–85) | 1155 (595–1511) |
| 24 months n = 19 | 22 (8–38) | 5 (0–32) | 73 (55–84) | 1320 (682–1910) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Evans, S.; Daly, A.; Wildgoose, J.; Cochrane, B.; Chahal, S.; Ashmore, C.; Loveridge, N.; MacDonald, A. Growth, Protein and Energy Intake in Children with PKU Taking a Weaning Protein Substitute in the First Two Years of Life: A Case-Control Study. Nutrients 2019, 11, 552. https://doi.org/10.3390/nu11030552
Evans S, Daly A, Wildgoose J, Cochrane B, Chahal S, Ashmore C, Loveridge N, MacDonald A. Growth, Protein and Energy Intake in Children with PKU Taking a Weaning Protein Substitute in the First Two Years of Life: A Case-Control Study. Nutrients. 2019; 11(3):552. https://doi.org/10.3390/nu11030552
Chicago/Turabian StyleEvans, Sharon, Anne Daly, Jo Wildgoose, Barbara Cochrane, Satnam Chahal, Catherine Ashmore, Nik Loveridge, and Anita MacDonald. 2019. "Growth, Protein and Energy Intake in Children with PKU Taking a Weaning Protein Substitute in the First Two Years of Life: A Case-Control Study" Nutrients 11, no. 3: 552. https://doi.org/10.3390/nu11030552