Do Aspects of Protein Intake Vary Across the Week in Healthy Community-Dwelling Older Adults?—An enable Study

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Assessment of Paticipants’ Characteristics
2.3. Aspects of Protein Intake
2.4. Data Analysis and Statistics
3. Results
3.1. Characteristics of the Study Participants
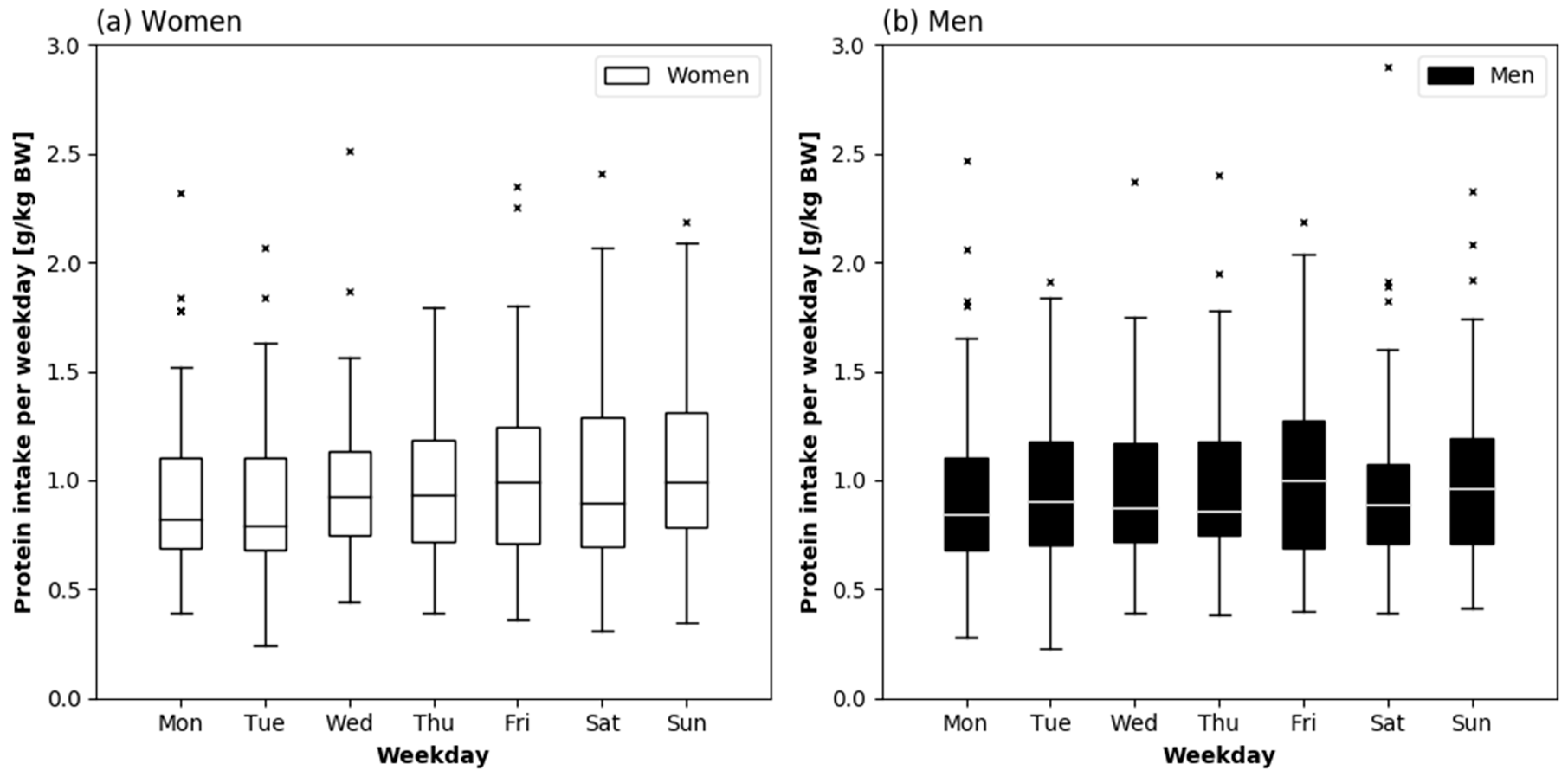
3.2. Daily Protein Intake Across the Week
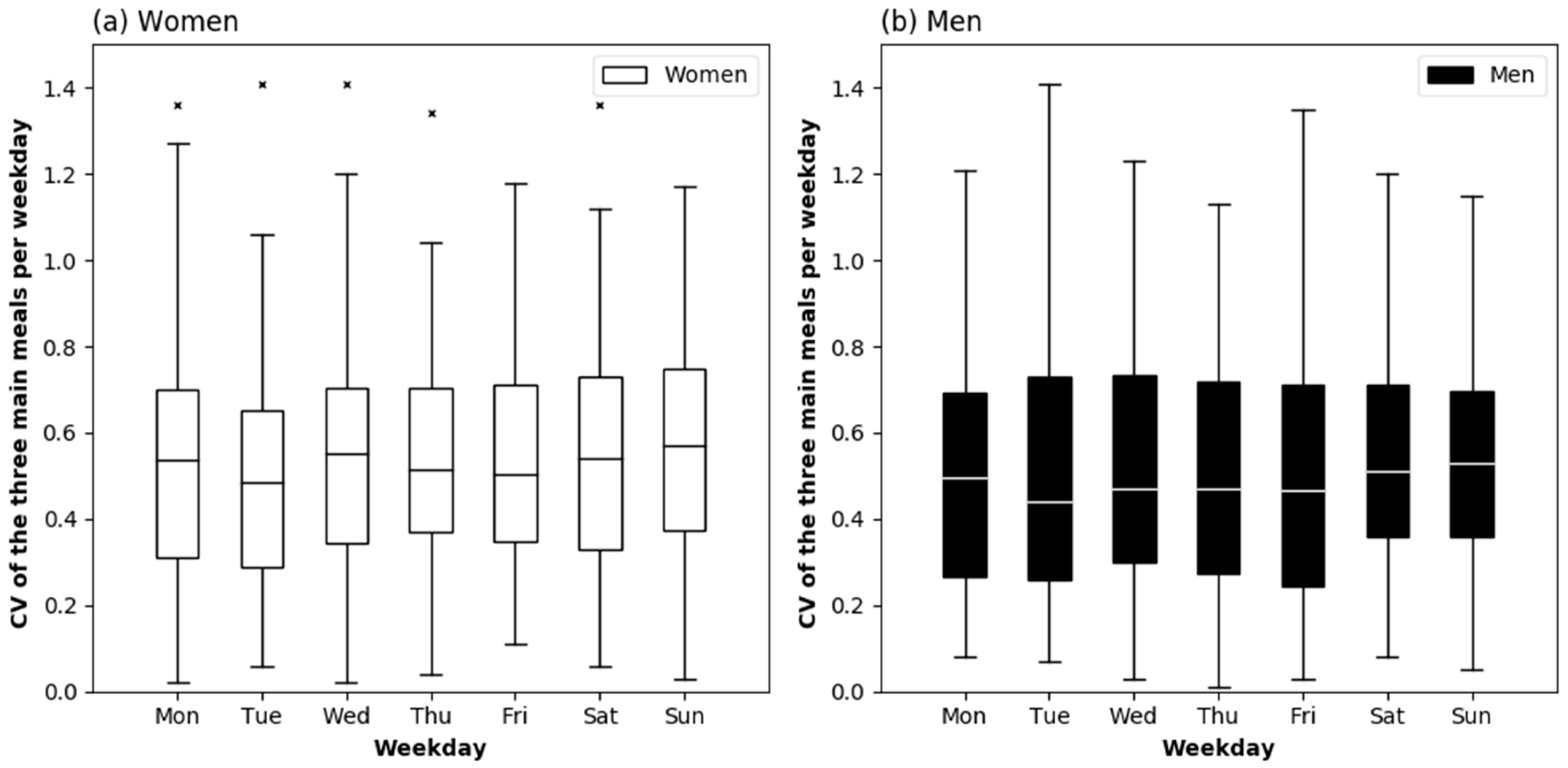
3.3. Distribution of Protein Intake between the Three Main Meals across the Week
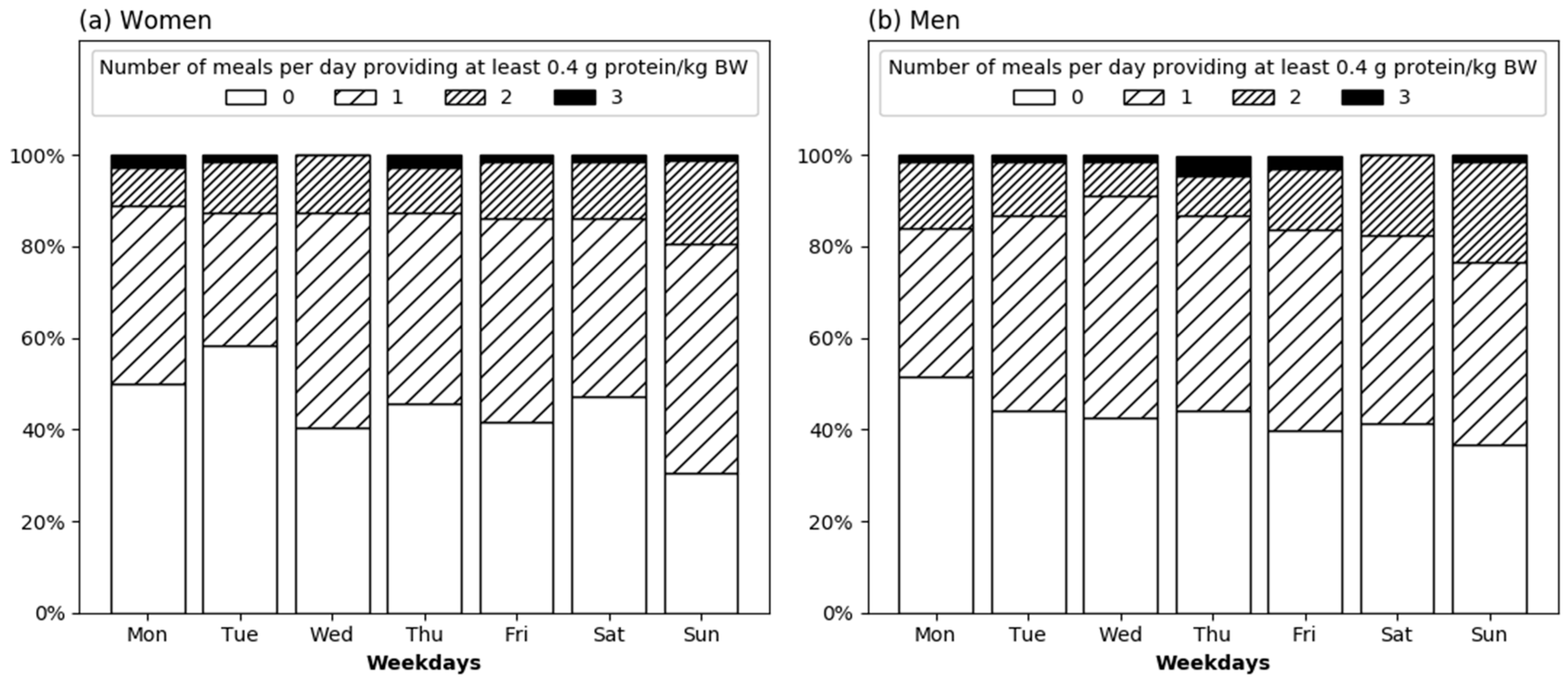
3.4. Number of Meals Providing Adequate Protein across the Week
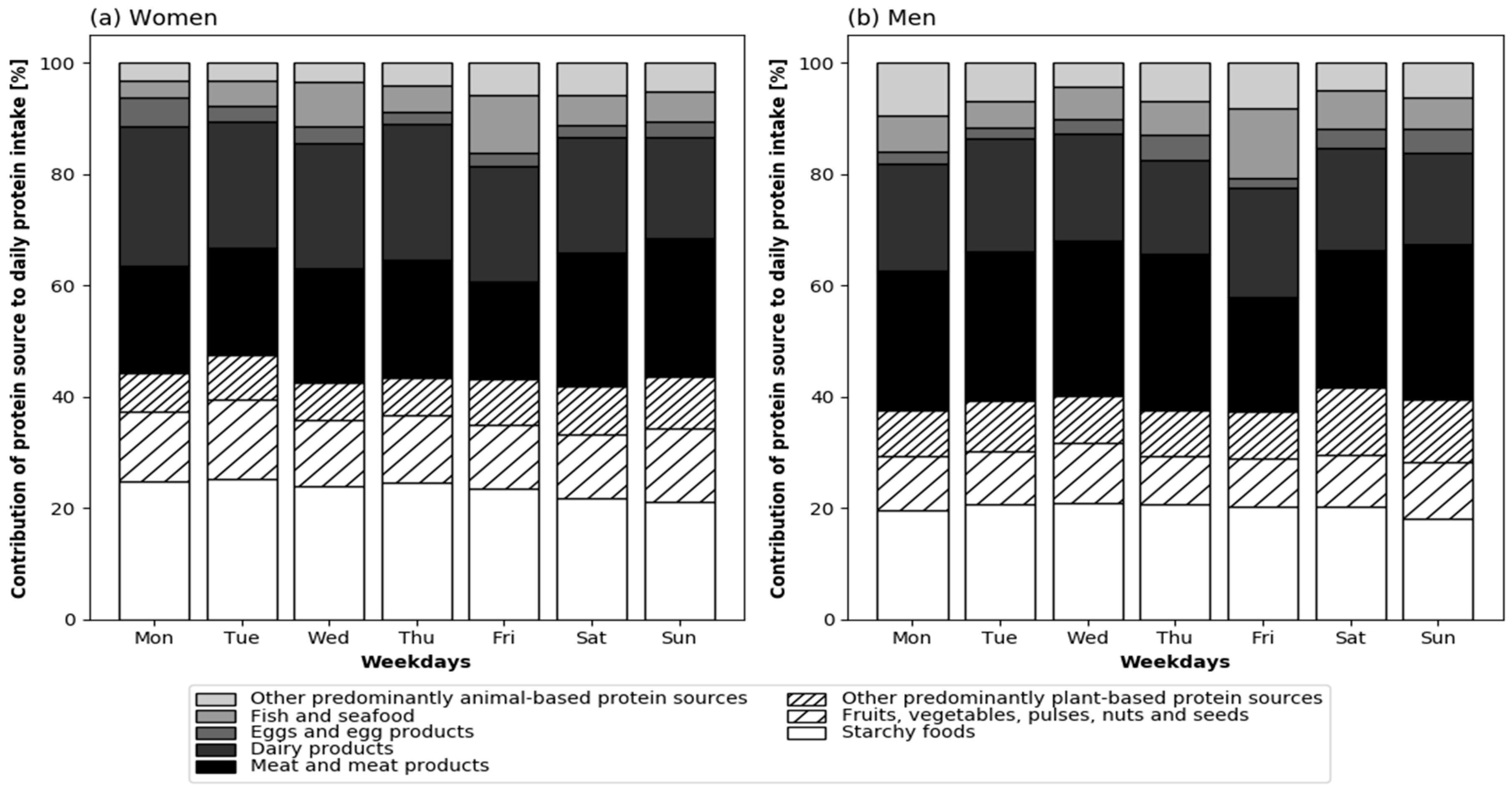
3.5. Protein Sources across the Week
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Deutz, N.E.; Bauer, J.M.; Barazzoni, R.; Biolo, G.; Boirie, Y.; Bosy-Westphal, A.; Cederholm, T.; Cruz-Jentoft, A.; Krznaric, Z.; Nair, K.S.; et al. Protein intake and exercise for optimal muscle function with aging: Recommendations from the ESPEN Expert Group. Clin. Nutr. 2014, 33, 929–936. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bauer, J.; Biolo, G.; Cederholm, T.; Cesari, M.; Cruz-Jentoft, A.J.; Morley, J.E.; Phillips, S.; Sieber, C.; Stehle, P.; Teta, D.; et al. Evidence-based recommendations for optimal dietary protein intake in older people: A position paper from the PROT-AGE Study Group. J. Am. Med. Dir. Assoc. 2013, 14, 542–559. [Google Scholar] [CrossRef] [PubMed]
- Paddon-Jones, D.; Campbell, W.W.; Jacques, P.F.; Kritchevsky, S.B.; Moore, L.L.; Rodriguez, N.R.; van Loon, L.J. Protein and healthy aging. Am. J. Clin. Nutr. 2015. [Google Scholar] [CrossRef] [PubMed]
- Murphy, C.H.; Oikawa, S.Y.; Phillips, S.M. Dietary Protein to Maintain Muscle Mass in Aging: A Case for Per-meal Protein Recommendations. J. Frailty Aging 2016, 5, 49–58. [Google Scholar] [PubMed]
- Breen, L.; Phillips, S.M. Skeletal muscle protein metabolism in the elderly: Interventions to counteract the ‘anabolic resistance’ of ageing. Nutr. Metab. 2011, 8, 68. [Google Scholar] [CrossRef] [PubMed]
- Gorissen, S.H.M.; Witard, O.C. Characterising the muscle anabolic potential of dairy, meat and plant-based protein sources in older adults. Proc. Nutr. Soc. 2017, 77, 20–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haines, P.S.; Hama, M.Y.; Guilkey, D.K.; Popkin, B.M. Weekend eating in the United States is linked with greater energy, fat, and alcohol intake. Obes. Res. 2003, 11, 945–949. [Google Scholar] [CrossRef] [PubMed]
- De Castro, J.M. Age-related changes in the social, psychological, and temporal influences on food intake in free-living, healthy, adult humans. J. Gerontol. A Biol. Sci. Med. Sci. 2002, 57, M368–M377. [Google Scholar] [CrossRef] [PubMed]
- Yang, P.H.; Black, J.L.; Barr, S.I.; Vatanparast, H. Examining differences in nutrient intake and dietary quality on weekdays versus weekend days in Canada. Appl. Physiol. Nutr. Metab. 2014, 39, 1413–1417. [Google Scholar] [CrossRef] [PubMed]
- McCarthy, S. Weekly patterns, diet quality and energy balance. Physiol. Behav. 2014, 134, 55–59. [Google Scholar] [CrossRef] [PubMed]
- An, R. Weekend-weekday differences in diet among U.S. adults, 2003–2012. Ann. Epidemiol. 2016, 26, 57–65. [Google Scholar] [CrossRef] [PubMed]
- Orsama, A.L.; Mattila, E.; Ermes, M.; van Gils, M.; Wansink, B.; Korhonen, I. Weight rhythms: Weight increases during weekends and decreases during weekdays. Obes. Facts 2014, 7, 36–47. [Google Scholar] [CrossRef] [PubMed]
- Farsijani, S.; Morais, J.A.; Payette, H.; Gaudreau, P.; Shatenstein, B.; Gray-Donald, K.; Chevalier, S. Relation between mealtime distribution of protein intake and lean mass loss in free-living older adults of the NuAge study. Am. J. Clin. Nutr. 2016, 104, 694–703. [Google Scholar] [CrossRef] [PubMed]
- Farsijani, S.; Payette, H.; Morais, J.A.; Shatenstein, B.; Gaudreau, P.; Chevalier, S. Even mealtime distribution of protein intake is associated with greater muscle strength, but not with 3-y physical function decline, in free-living older adults: The Quebec longitudinal study on Nutrition as a Determinant of Successful Aging (NuAge study). Am. J. Clin. Nutr. 2017, 106, 113–124. [Google Scholar] [CrossRef] [PubMed]
- Lord, C.; Chaput, J.P.; Aubertin-Leheudre, M.; Labonte, M.; Dionne, I.J. Dietary animal protein intake: Association with muscle mass index in older women. J. Nutr. Health Aging 2007, 11, 383–387. [Google Scholar] [PubMed]
- Kobayashi, S.; Asakura, K.; Suga, H.; Sasaki, S. High protein intake is associated with low prevalence of frailty among old Japanese women: A multicenter cross-sectional study. Nutr. J. 2013, 12, 164. [Google Scholar] [CrossRef] [PubMed]
- Loenneke, J.P.; Loprinzi, P.D.; Murphy, C.H.; Phillips, S.M. Per meal dose and frequency of protein consumption is associated with lean mass and muscle performance. Clin. Nutr. 2016, 35, 1506–1511. [Google Scholar] [CrossRef] [PubMed]
- Mishra, S.; Goldman, J.D.; Sahyoun, N.R.; Moshfegh, A.J. Association between dietary protein intake and grip strength among adults aged 51 years and over: What We Eat in America, National Health and Nutrition Examination Survey 2011–2014. PLoS ONE 2018, 13, e0191368. [Google Scholar] [CrossRef] [PubMed]
- Rahi, B.; Colombet, Z.; Gonzalez-Colaco Harmand, M.; Dartigues, J.F.; Boirie, Y.; Letenneur, L.; Feart, C. Higher Protein but Not Energy Intake Is Associated with a Lower Prevalence of Frailty Among Community-Dwelling Older Adults in the French Three-City Cohort. J. Am. Med. Dir. Assoc. 2016, 17, 672.e7–672.e11. [Google Scholar] [CrossRef] [PubMed]
- Granic, A.; Mendonca, N.; Sayer, A.A.; Hill, T.R.; Davies, K.; Adamson, A.; Siervo, M.; Mathers, J.C.; Jagger, C. Low protein intake, muscle strength and physical performance in the very old: The Newcastle 85+ Study. Clin. Nutr. 2017. [Google Scholar] [CrossRef] [PubMed]
- Isanejad, M.; Mursu, J.; Sirola, J.; Kroger, H.; Rikkonen, T.; Tuppurainen, M.; Erkkila, A.T. Dietary protein intake is associated with better physical function and muscle strength among elderly women. Br. J. Nutr. 2016, 115, 1281–1291. [Google Scholar] [CrossRef] [PubMed]
- Gingrich, A.; Spiegel, A.; Kob, R.; Schoene, D.; Skurk, T.; Hauner, H.; Sieber, C.C.; Volkert, D.; Kiesswetter, E. Amount, Distribution, and Quality of Protein Intake Are Not Associated with Muscle Mass, Strength, and Power in Healthy Older Adults without Functional Limitations-An enable Study. Nutrients 2017, 9. [Google Scholar] [CrossRef] [PubMed]
- D’Ath, P.; Katona, P.; Mullan, E.; Evans, S.; Katona, C. Screening, detection and management of depression in elderly primary care attenders. I: The acceptability and performance of the 15 item Geriatric Depression Scale (GDS15) and the development of short versions. Fam. Pract. 1994, 11, 260–266. [Google Scholar] [CrossRef] [PubMed]
- Cwikel, J.; Ritchie, K. Screening for depression among the elderly in Israel: An assessment of the Short Geriatric Depression Scale (S-GDS). Isr. J. Med. Sci. 1989, 25, 131–137. [Google Scholar] [PubMed]
- Folstein, M.F.; Robins, L.N.; Helzer, J.E. The Mini-Mental State Examination. Arch. Gen. Psychiatry 1983, 40, 812. [Google Scholar] [CrossRef] [PubMed]
- Guigoz, Y.; Vellas, B.; Garry, P.J. Assessing the nutritional status of the elderly: The Mini Nutritional Assessment as part of the geriatric evaluation. Nutr. Rev. 1996, 54, S59–S65. [Google Scholar] [CrossRef]
- Guralnik, J.M.; Ferrucci, L.; Pieper, C.F.; Leveille, S.G.; Markides, K.S.; Ostir, G.V.; Studenski, S.; Berkman, L.F.; Wallace, R.B. Lower extremity function and subsequent disability: Consistency across studies, predictive models, and value of gait speed alone compared with the short physical performance battery. J. Gerontol. A Biol. Sci. Med. Sci. 2000, 55, M221–M231. [Google Scholar] [CrossRef] [PubMed]
- Janssen, I.; Heymsfield, S.B.; Baumgartner, R.N.; Ross, R. Estimation of skeletal muscle mass by bioelectrical impedance analysis. J Appl. Physiol. 2000, 89, 465–471. [Google Scholar] [CrossRef] [PubMed]
- Dehne, L.I.; Klemm, C.; Henseler, G.; Hermann-Kunz, E. The German Food Code and Nutrient Data Base (BLS II.2). Eur. J. Epidemiol. 1999, 15, 355–359. [Google Scholar] [CrossRef] [PubMed]
- Bollwein, J.; Diekmann, R.; Kaiser, M.J.; Bauer, J.M.; Uter, W.; Sieber, C.C.; Volkert, D. Distribution but not amount of protein intake is associated with frailty: A cross-sectional investigation in the region of Nurnberg. Nutr. J. 2013, 12, 109. [Google Scholar] [CrossRef] [PubMed]
- Beasley, J.M.; Wertheim, B.C.; LaCroix, A.Z.; Prentice, R.L.; Neuhouser, M.L.; Tinker, L.F.; Kritchevsky, S.; Shikany, J.M.; Eaton, C.; Chen, Z.; et al. Biomarker-calibrated protein intake and physical function in the Women’s Health Initiative. J. Am. Geriatr. Soc. 2013, 61, 1863–1871. [Google Scholar] [CrossRef] [PubMed]
- Deutsche Gesellschaft für Ernährung: Wie viel Protein Brauchen wir? Available online: https://www.dge.de/wissenschaft/referenzwerte/protein/ (accessed on 26 July 2018).
- Cardon-Thomas, D.K.; Riviere, T.; Tieges, Z.; Greig, C.A. Dietary Protein in Older Adults: Adequate Daily Intake but Potential for Improved Distribution. Nutrients 2017, 9. [Google Scholar] [CrossRef] [PubMed]
- Gorissen, S.H.; Horstman, A.M.; Franssen, R.; Kouw, I.W.; Wall, B.T.; Burd, N.A.; de Groot, L.C.; van Loon, L.J. Habituation to low or high protein intake does not modulate basal or postprandial muscle protein synthesis rates: A randomized trial. Am. J. Clin. Nutr. 2017, 105, 332–342. [Google Scholar] [CrossRef] [PubMed]
- McNamara, D.J. The Fifty Year Rehabilitation of the Egg. Nutrients 2015, 7, 8716–8722. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robinson, S.M.; Jameson, K.A.; Batelaan, S.F.; Martin, H.J.; Syddall, H.E.; Dennison, E.M.; Cooper, C.; Sayer, A.A. Diet and its relationship with grip strength in community-dwelling older men and women: The Hertfordshire cohort study. J. Am. Geriatr. Soc. 2008, 56, 84–90. [Google Scholar] [CrossRef] [PubMed]
- Tieland, M.; Borgonjen-Van den Berg, K.J.; Van Loon, L.J.; de Groot, L.C. Dietary Protein Intake in Dutch Elderly People: A Focus on Protein Sources. Nutrients 2015, 7, 9697–9706. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rousset, S.; Patureau Mirand, P.; Brandolini, M.; Martin, J.F.; Boirie, Y. Daily protein intakes and eating patterns in young and elderly French. Br. J. Nutr. 2003, 90, 1107–1115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Livingstone, M.B.; Black, A.E. Markers of the validity of reported energy intake. J. Nutr. 2003, 133, 895S–920S. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All | Women | Men | p * | |
|---|---|---|---|---|
| n = 140 | n = 72 | n = 68 | ||
| Age [years] | 77.0 [76.0–80.0] | 77.0 [76.0–80.0] | 78.0 [76.0–80.0] | 0.559 |
| GDS [points] | 1.0 [0.0–2.0] | 1.0 [0.0–2.0] | 1.0 [0.0–1.8] | 0.809 |
| MMSE [points] | 29.0 [29.0–30.0] | 29.0 [29.0–30.0] | 29.0 [29.0–30.0] | 0.799 |
| MNA [points] | 27.5 [25.6–28.5] | 27.5 [25.5–28.5] | 27.5 [26.0–28.5] | 0.666 |
| SPPB [points] | 12.0 [11.0–12.0] | 12.0 [11.0–12.0] | 12.0 [11.0–12.0] | 0.223 |
| BMI [kg/m2] a | 26.7 [23.5–29.2] | 25.7 [23.0–28.7] | 27.6 [24.7–29.3] | 0.074 |
| Body weight [kg] a | 74.0 [63.5–82.9] | 65.8 [59.8–75.4] | 81.6 [72.4–89.2] | <0.001 |
| Fat free mass [kg] | 46.1 [38.4–55.6] | 38.6 [34.1–41.5] | 55.9 [51.6–59.9] | <0.001 |
| Skeletal muscle mass [kg] | 19.8 [15.6–26.1] | 15.7 [14.2–17.2] | 26.2 [24.7–28.2] | <0.001 |
| Skeletal muscle index [kg/m2] | 7.3 [6.0–8.8] | 6.1 [5.6–6.6] | 8.8 [8.3–9.2] | <0.001 |
| Living alone [%] | 55.7 | 73.6 | 36.8 | <0.001 |
| Main meal usually alone [%] | 55.7 | 70.8 | 39.7 | <0.001 |
| Appetite very good/good [%] | 87.9 | 84.7 | 91.2 | 0.243 |
| Energy intake [kcal] | 1892 [1598–2184] | 1678 [1524–1928] | 2111 [1820–2327] | <0.001 |
| Carbohydrate intake [g/day] | 190.4 [161.4–236.9] | 175.2 [153.8–211.2] | 211.6 [177.8–257.4] | <0.001 |
| Fat intake [g/day] | 78.5 [68.2–95.0] | 74.4 [67.6–89.3] | 86.7 [73.7–97.5] | 0.008 |
| Protein intake [g/day] | 68.1 [57.0–81.9] | 63.0 [53.1–73.0] | 73.6 [63.2–89.8] | <0.001 |
| Alcohol intake [g/day] | 6.6 [1.2–16.9] | 3.5 [0.7–8.2] | 11.5 [3.5–27.1] | <0.001 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gingrich, A.; Rennekamp, R.; Brandl, B.; Skurk, T.; Hauner, H.; Sieber, C.C.; Volkert, D.; Kiesswetter, E. Do Aspects of Protein Intake Vary Across the Week in Healthy Community-Dwelling Older Adults?—An enable Study. Nutrients 2018, 10, 1217. https://doi.org/10.3390/nu10091217
Gingrich A, Rennekamp R, Brandl B, Skurk T, Hauner H, Sieber CC, Volkert D, Kiesswetter E. Do Aspects of Protein Intake Vary Across the Week in Healthy Community-Dwelling Older Adults?—An enable Study. Nutrients. 2018; 10(9):1217. https://doi.org/10.3390/nu10091217
Chicago/Turabian StyleGingrich, Anne, Rachel Rennekamp, Beate Brandl, Thomas Skurk, Hans Hauner, Cornel C. Sieber, Dorothee Volkert, and Eva Kiesswetter. 2018. "Do Aspects of Protein Intake Vary Across the Week in Healthy Community-Dwelling Older Adults?—An enable Study" Nutrients 10, no. 9: 1217. https://doi.org/10.3390/nu10091217